25-Hydroxy Vitamin D Detection Using Different Analytic Methods in Patients with Migraine

 ,
, 
 ,
, 


Abstract
:1. Introduction
2. Methods
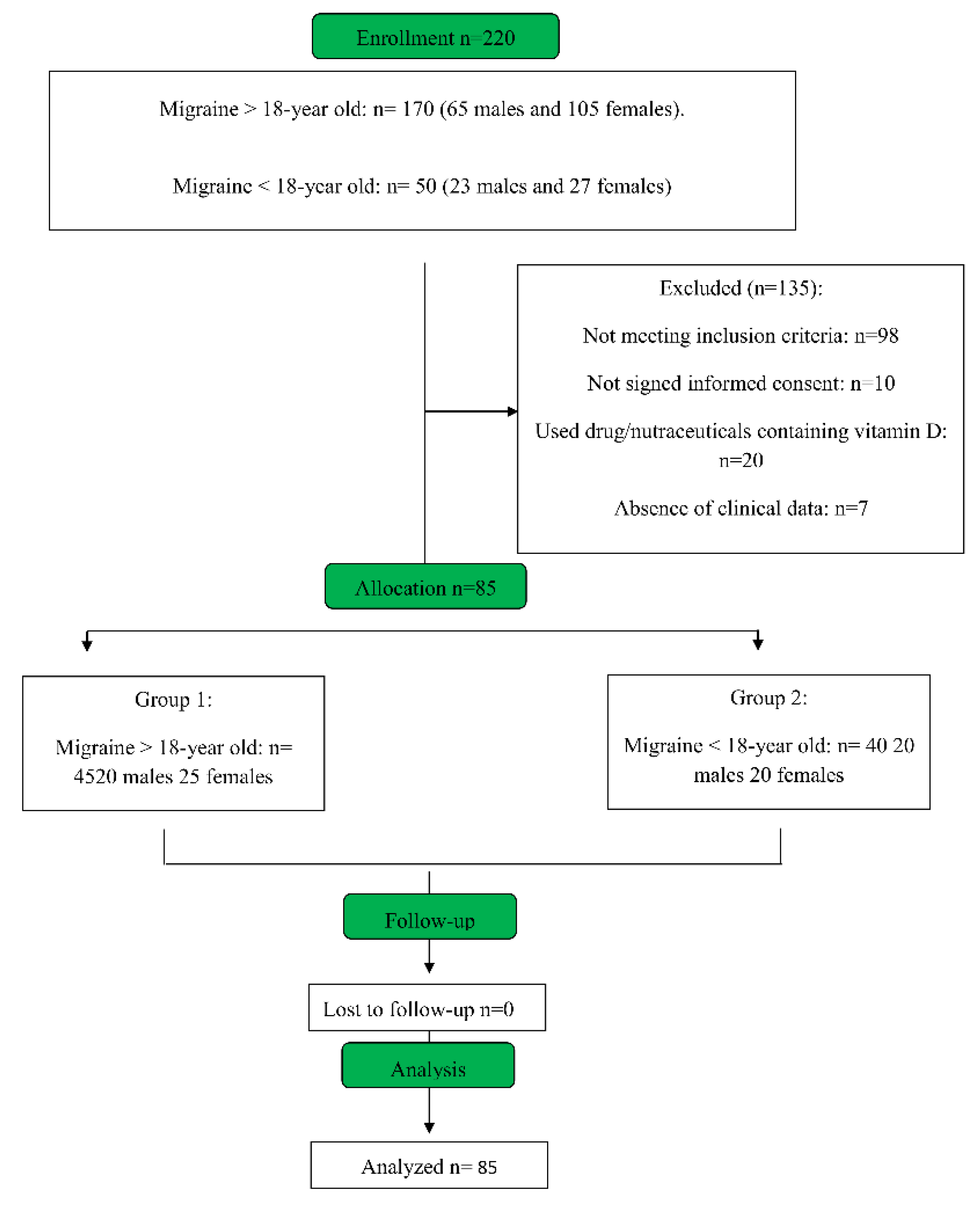
2.1. Study
2.2. Samples
2.3. Inclusion and Exclusion Criteria
2.4. Endpoints
2.5. Experimental Protocol
2.5.1. Blood Collection and Storage
2.5.2. Vitamin D Detection
2.5.3. LC-MS/MS Analysis
2.5.4. HPLC Analysis
2.5.5. Enzyme-Linked Immunosorbent Assay (EIA)
2.5.6. Chemiluminescence Immune Assays (CLIA)
2.6. Statistical Analysis
3. Results
3.1. Samples Collection
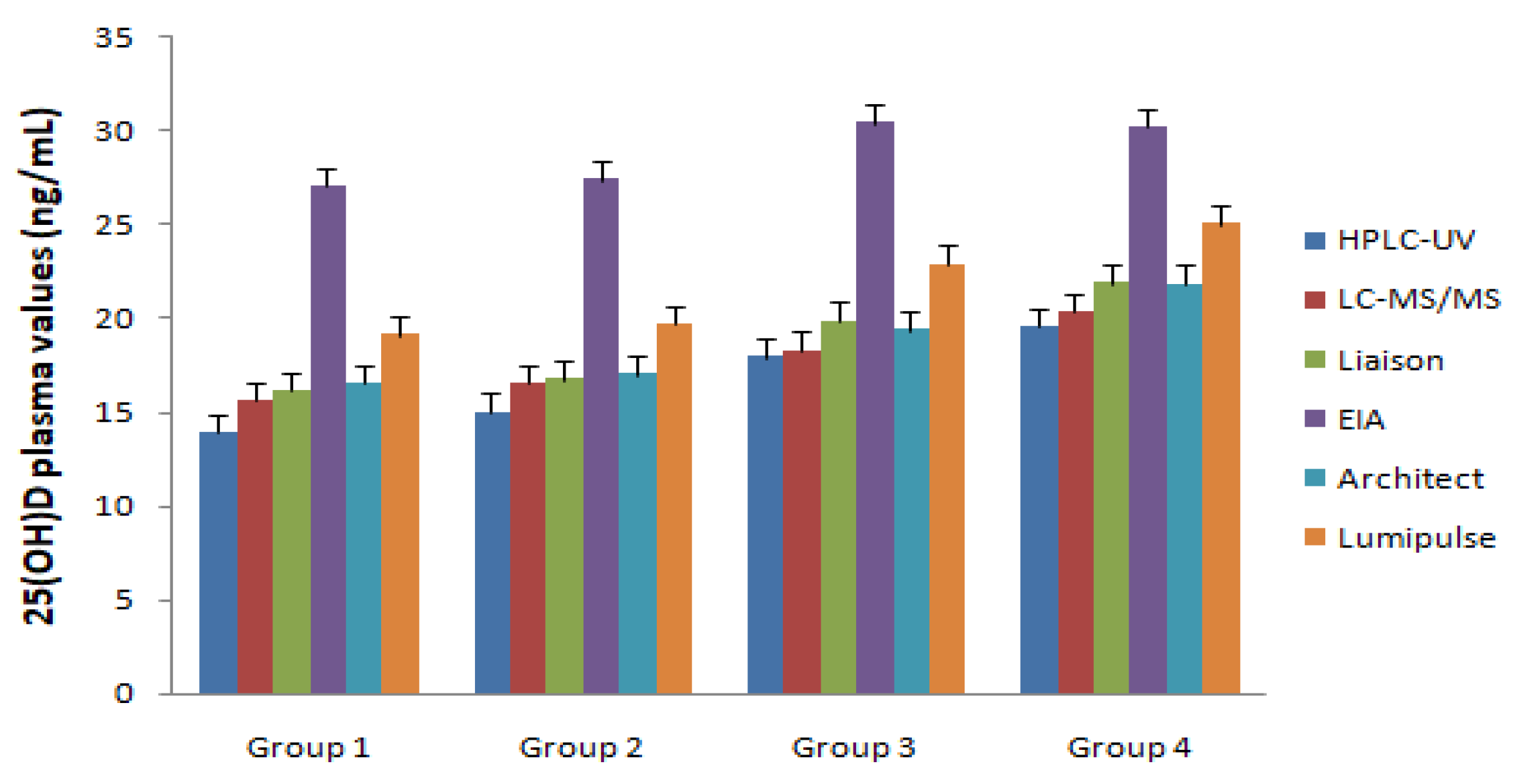
3.2. Vitamin 25(OH)D Evaluation
3.3. Vitamin 25(OH)D Differences in Methodological Approaches
3.4. Vitamin 25(OH)D Differences in Collection Tubes Used
3.5. Vitamin 25(OH)D Supplementation
4. Discussion
Author Contributions
Conflicts of Interest
References
- Holick, M.F.; Chen, T.C.; Lu, Z.; Sauter, E. Vitamin D and skin physiology: A D-lightful story. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2007, 22 (Suppl. 2), 28–33. [Google Scholar] [CrossRef]
- Houghton, L.A.; Vieth, R. The case against ergocalciferol (vitamin D2) as a vitamin supplement. Am. J. Clin. Nutr. 2006, 84, 694–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollis, B.W. Comparison of equilibrium and disequilibrium assay conditions for ergocalciferol, cholecalciferol, and their major metabolites. J. Steroid Biochem. 1984, 21, 81–86. [Google Scholar] [CrossRef]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 Dietary Reference Intakes for Calcium and Vitamin D: What dietetics practitioners need to know. J. Am. Diet. Assoc. 2011, 111, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P. Serum 25-hydroxyvitamin D is a reliable indicator of vitamin D status. Am. J. Clin. Nutr. 2011, 94, 619–620. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, H.L.; Wu, J. Is headache related with vitamin D insufficiency? J. Headache Pain 2010, 11, 369. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Mehta, N.C.; Dabhi, A.S.; Lakhani, O.; Khilari, M.; Shah, N.D. The prevalence of headache may be related with the latitude: A possible role of Vitamin D insufficiency? J. Headache Pain 2010, 11, 301–307. [Google Scholar] [CrossRef]
- Freeman, J.; Wilson, K.; Spears, R.; Shalhoub, V.; Sibley, P. Performance evaluation of four 25-hydroxyvitamin D assays to measure 25-hydroxyvitamin D2. Clin. Biochem. 2015, 48, 1097–1104. [Google Scholar] [CrossRef] [Green Version]
- Simpson, C.A.; Cusano, A.M.; Bihuniak, J.; Walker, J.; Insogna, K.L. Effect of 25(OH) vitamin D reference method procedure (RMP) alignment on clinical measurements obtained with the IDS-iSYS chemiluminescent-based automated analyzer. J. Steroid Biochem. Mol. Biol. 2015, 148, 41–46. [Google Scholar] [CrossRef]
- Botros, R.M.; AbdElsalam Besibes, M.M.; Bahaaeldin, A.M.; Abo Elyazed, S. Vitamin D Status in Hospitalized Chronically Ill Subjects. J. Am. Coll. Nutr. 2018, 37, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Kumar, M.; Belani, P.; Susvirkar, A.; Ahuja, S. Interrelationships between chronic tension-type headache, musculoskeletal pain, and vitamin D deficiency: Is osteomalacia responsible for both headache and musculoskeletal pain? Ann. Indian Acad. Neurol. 2013, 16, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Shah, N.D. Chronic tension-type headache with vitamin D deficiency: Casual or causal association? Headache 2009, 49, 1214–1222. [Google Scholar] [CrossRef]
- Prakash, S.; Makwana, P.; Rathore, C. Vitamin D deficiency mimicking chronic tension-type headache in children. BMJ Case Rep. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Rathore, C.; Makwana, P.; Dave, A.; Joshi, H.; Parekh, H. Vitamin D Deficiency in Subjects With Chronic Tension-Type Headache: A Case-Control Study. Headache 2017, 57, 1096–1108. [Google Scholar] [CrossRef] [PubMed]
- Celikbilek, A.; Gocmen, A.Y.; Zararsiz, G.; Tanik, N.; Ak, H.; Borekci, E.; Delibas, N. Serum levels of vitamin D, vitamin D-binding protein and vitamin D receptor in migraine subjects from central Anatolia region. Int. J. Clin. Pract. 2014, 68, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- Siniscalchi, A.; De Sarro, G.; Michniewicz, A.; Gallelli, L. Conventional and New Antiepileptic Drugs on Vitamin D and Bone Health: What We Know to Date? Curr. Clin. Pharmacol. 2016, 11, 69–70. [Google Scholar] [CrossRef]
- Delavari, B.; Saboury, A.A.; Atri, M.S.; Ghasemi, A.; Bigdeli, B.; Khammari, A.; Maghami, P.; Moosavi-Movahedi, A.A.; Haertlé, T.; Goliaei, B. Alpha-lactalbumin: A new carrier for vitamin D3 food enrichment. Food Hydrocoll. 2015, 45, 124–131. [Google Scholar] [CrossRef]
- Li, T.-L.; Min, D.B. Stability and Photochemistry of Vitamin D2 in Model System. J. Food Sci. 1998, 63, 413–417. [Google Scholar] [CrossRef]
- Wielders, J.P.; Wijnberg, F.A. Preanalytical stability of 25(OH)-vitamin D3 in human blood or serum at room temperature: Solid as a rock. Clin. Chem. 2009, 55, 1584–1585. [Google Scholar] [CrossRef]
- Ocke, M.C.; Schrijver, J.; Obermann-de Boer, G.L.; Bloemberg, B.P.; Haenen, G.R.; Kromhout, D. Stability of blood (pro)vitamins during four years of storage at −20 degrees C: Consequences for epidemiologic research. J. Clin. Epidemiol. 1995, 48, 1077–1085. [Google Scholar] [CrossRef]
- Rossini, M.; Adami, S.; Bertoldo, F.; Diacinti, D.; Gatti, D.; Giannini, S.; Malavolta, N.; Minisola, S.; Osella, G.; Pedrazzoni, M.; et al. Guidelines for the diagnosis, prevention, and management of osteoporosis. Reumatismo 2016, 68, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Cesareo, R.; Attanasio, R.; Caputo, M.; Castello, R.; Chiodini, I.; Falchetti, A.; Guglielmi, R.; Papini, E.; Santonati, A.; Scillitani, A.; et al. Italian Association of Clinical Endocrinologists (AME) and Italian Chapter of the American Association of Clinical Endocrinologists (AACE) Position Statement: Clinical Management of Vitamin D Deficiency in Adults. Nutrients 2018, 10, 546. [Google Scholar] [CrossRef] [PubMed]
- Poscia, A.; Cambieri, A.; Tucceri, C.; Ricciardi, W.; Volpe, M. Audit as a tool to assess and promote the quality of medical records and hospital appropriateness: Methodology and preliminary results. Ig. Sanita Pubbl. 2015, 71, 139–156. [Google Scholar] [PubMed]
- Albano, G.D.; Bertozzi, G.; Maglietta, F.; Montana, A.; Di Mizio, G.; Esposito, M.; Mazzeo, P.; D’Errico, S.; Salerno, M. Medical Records Quality as Prevention Tool for Healthcare-Associated Infections (HAIs) Related Litigation: A Case Series. Curr. Pharm. Biotechnol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Albolino, S.; Bellandi, T.; Cappelletti, S.; Di Paolo, M.; Fineschi, V.; Frati, P.; Offidani, C.; Tanzini, M.; Tartaglia, R.; Turillazzi, E. New rules on patient’s safety and professional liability for the Italian Health Service. Curr. Pharm. Biotechnol. 2019. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group1 | Group2 | Group3 | Group4 | |
|---|---|---|---|---|
| Male (n) | 20 | 20 | 45 | 16 |
| Female (n) | 25 | 20 | 45 | 14 |
| Age (n) | 40 ± 6.7 | 13.9 ± 2 | 54.2 ± 8.4 | 13.8 ± 2.3 |
| Body mass index | 28 ± 3 | 24 ± 3 | 29 ± 6 | 25 ± 4 |
| Smokers (n) | 23 | 1 | 38 | 0 |
| Blood pressure (mm/Hg) | 135/88 ± 7 | 115/70 ± 3 | 143/92 ± 5 | 115/68 ± 4 |
| Diabetes mellitus (n) | 8 | 3 | 2 | 2 |
| Hypertension (n) | 29 | 0 | 33 | 0 |
| Groups | Sex | HPLC-UV (ng/mL) | LC-MS/MS (ng/mL) | Liaison (ng/mL) | EIA (ng/mL) | Architect (ng/mL) | Lumipulse (ng/mL) |
|---|---|---|---|---|---|---|---|
| Group 1 | M | 13.7 ± 4.1 | 15.4 ± 4.3 | 16.0 ± 5.1 | 27.3 ± 6.1 | 16.3 ± 4.0 | 18.7 ± 5.3 |
| F | 14.1 ± 3.5 | 15.8 ± 3.7 | 16.3 ± 4.2 | 26.7 ± 6.2 | 16.7 ± 3.3 | 19.5 ± 5.5 | |
| Group 2 | M | 14.9 ± 4.7 | 16.6 ± 4.7 | 17.5 ± 5.9 | 25.8 ± 6.8 | 17.4 ± 4.4 | 20.0 ± 5.8 |
| F | 15.1 ± 5.7 | 16.4 ± 6.0 | 16.0 ± 6.8 | 28.9 ± 6.2 | 16.6 ± 5.6 | 19.3 ± 6.1 | |
| Group 3 | M | 17.3 ± 4.3 | 18.2 ± 3.2 | 19.8 ± 3.6 | 30.2 ± 6.2 | 19.6 ± 4.1 | 23.6 ± 5.2 |
| F | 18.5 ± 3.8 | 18.3 ± 3.6 | 19.9 ± 4.1 | 30.5 ± 5.9 | 19.1 ± 3.9 | 22.1 ± 4.8 | |
| Group 4 | M | 18.9 ± 4.2 | 19.1 ± 5.2 | 20.1 ± 4.8 | 30.7 ± 5.2 | 20.2 ± 4.5 | 23.1 ± 4.6 |
| F | 20.2 ± 4.5 | 21.5 ± 4.6 | 23.6 ± 4.5 | 29.6 ± 5.1 | 23.4 ± 3.7 | 26.9 ± 5.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallelli, L.; Michniewicz, A.; Cione, E.; Squillace, A.; Colosimo, M.; Pelaia, C.; Fazio, A.; Zampogna, S.; Peltrone, F.; Iannacchero, R.; et al. 25-Hydroxy Vitamin D Detection Using Different Analytic Methods in Patients with Migraine. J. Clin. Med. 2019, 8, 895. https://doi.org/10.3390/jcm8060895
Gallelli L, Michniewicz A, Cione E, Squillace A, Colosimo M, Pelaia C, Fazio A, Zampogna S, Peltrone F, Iannacchero R, et al. 25-Hydroxy Vitamin D Detection Using Different Analytic Methods in Patients with Migraine. Journal of Clinical Medicine. 2019; 8(6):895. https://doi.org/10.3390/jcm8060895
Chicago/Turabian StyleGallelli, Luca, Andzelika Michniewicz, Erika Cione, Aida Squillace, Manuela Colosimo, Corrado Pelaia, Alessia Fazio, Stefania Zampogna, Francesco Peltrone, Rosario Iannacchero, and et al. 2019. "25-Hydroxy Vitamin D Detection Using Different Analytic Methods in Patients with Migraine" Journal of Clinical Medicine 8, no. 6: 895. https://doi.org/10.3390/jcm8060895
APA StyleGallelli, L., Michniewicz, A., Cione, E., Squillace, A., Colosimo, M., Pelaia, C., Fazio, A., Zampogna, S., Peltrone, F., Iannacchero, R., Sarro, G. D., G&SP Working Group, Salerno, M., & Di Mizio, G. (2019). 25-Hydroxy Vitamin D Detection Using Different Analytic Methods in Patients with Migraine. Journal of Clinical Medicine, 8(6), 895. https://doi.org/10.3390/jcm8060895