Prevalence of Non-Affective Psychoses in Individuals with Autism Spectrum Disorders: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
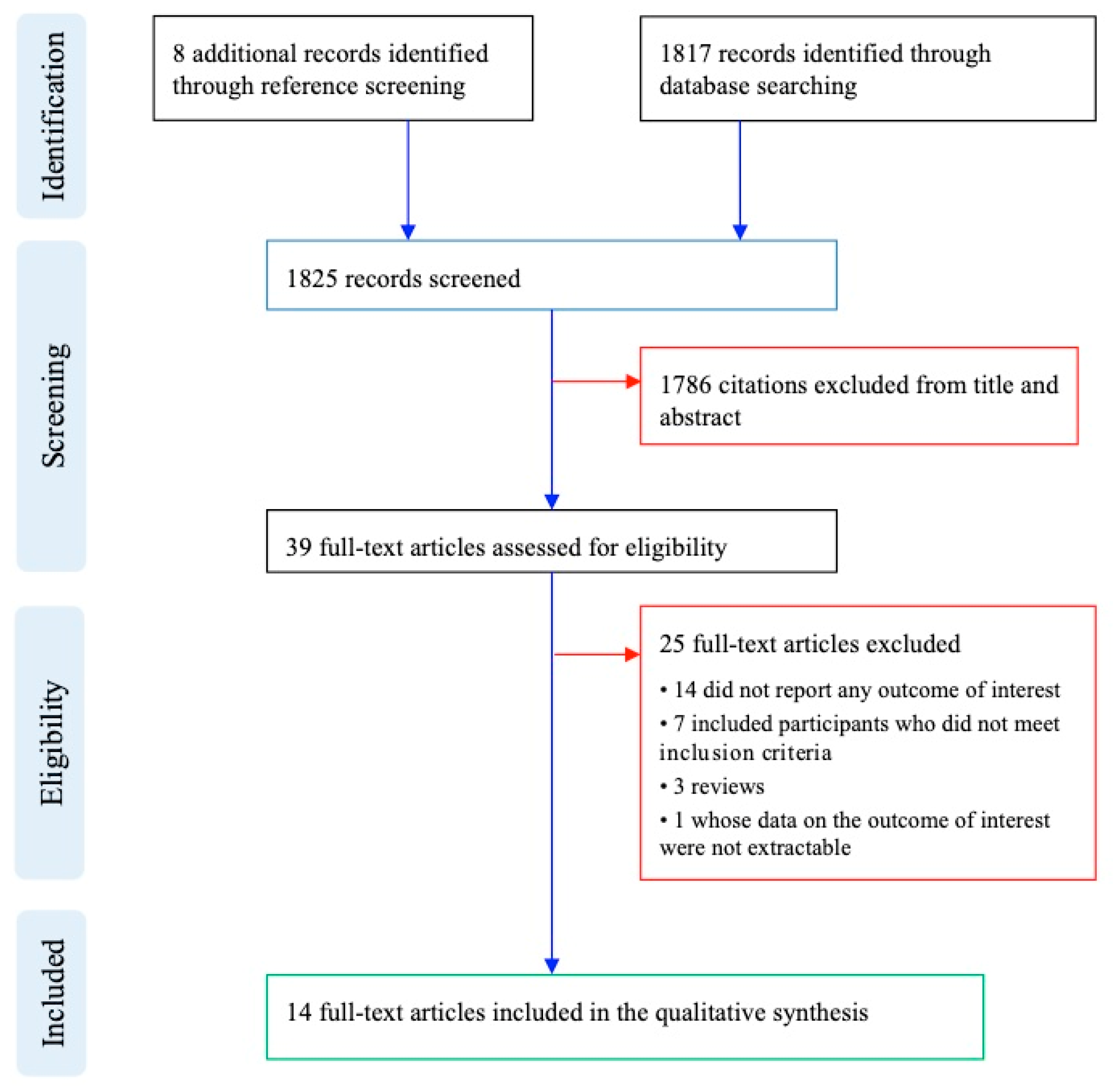
2. Methods
3. Results
3.1. Low Prevalence of Psychotic Symptoms/Schizophrenia in ASD (<20%)
3.2. High Prevalence of Psychotic Symptoms/Schizophrenia in ASD (≥20%)
3.3. Subgroup Analyses
4. Discussion
4.1. Limitations
4.2. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Bleuler, E. Dementia praecox or the group of schizophrenias. Vertex 2010, 21, 394–400. [Google Scholar] [PubMed]
- Bender, L. Childhood schizophrenia: Clinical study on one hundred schizophrenic children. Am. J. Orthopsychiatry 1947, 17, 40–56. [Google Scholar] [CrossRef]
- Kanner, L. Autistic disturbances of affective contact. Acta Paedopsychiatr. 1968, 35, 100–136. [Google Scholar]
- Rutter, M. Childhood schizophrenia reconsidered. J. Autism Child. Schizophr. 1972, 2, 315–337. [Google Scholar] [CrossRef] [PubMed]
- Kolvin, I. Studies in the Childhood Psychoses I. Diagnostic Criteria and Classification. Br. J. Psychiatry 1971, 118, 381–384. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Insel, T.R. Rethinking schizophrenia. Nature 2010, 468, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Cardno, A.G.; Gottesman, I.I. Twin studies of schizophrenia: From bow-and-arrow concordances to star wars Mx and functional genomics. Am. J. Med. Genet. 2000, 97, 12–17. [Google Scholar] [CrossRef]
- Freitag, C.M. The genetics of autistic disorders and its clinical relevance: A review of the literature. Mol. Psychiatry 2007, 12, 2–22. [Google Scholar] [CrossRef]
- Sandin, S.; Lichtenstein, P.; Kuja-Halkola, R.; Larsson, H.; Hultman, C.M.; Reichenberg, A. The familial risk of autism. JAMA 2014, 311, 1770–1777. [Google Scholar] [CrossRef]
- Daniels, J.L.; Forssen, U.; Hultman, C.M.; Cnattingius, S.; Savitz, D.A.; Feychting, M.; Sparen, P. Parental Psychiatric Disorders Associated with Autism Spectrum Disorders in the Offspring. Pediatrics 2008, 121, e1357–e1362. [Google Scholar] [CrossRef]
- Larsson, H.J.; Eaton, W.W.; Madsen, K.M.; Vestergaard, M.; Olesen, A.V.; Agerbo, E.; Schendel, D.; Thorsen, P.; Mortensen, P.B. Risk factors for autism: Perinatal factors, parental psychiatric history, and socioeconomic status. Am. J. Epidemiol. 2005, 161, 916–925. [Google Scholar] [CrossRef]
- Sporn, A.L.; Addington, A.M.; Gogtay, N.; Ordoñez, A.E.; Gornick, M.; Clasen, L.; Greenstein, D.; Tossell, J.W.; Gochman, P.; Lenane, M.; et al. Pervasive developmental disorder and childhood-onset schizophrenia: Comorbid disorder or a phenotypic variant of a very early onset illness? Biol. Psychiatry 2004, 55, 989–994. [Google Scholar] [CrossRef]
- Sullivan, P.F.; Magnusson, C.; Reichenberg, A.; Boman, M.; Dalman, C.; Davidson, M.; Fruchter, E.; Hultman, C.M.; Lundberg, M.; Långström, N.; et al. Family history of schizophrenia and bipolar disorder as risk factors for autism. Arch. Gen. Psychiatry 2012, 69, 1099–1103. [Google Scholar] [CrossRef]
- Lionel, A.C.; Vaags, A.K.; Sato, D.; Gazzellone, M.J.; Mitchell, E.B.; Chen, H.Y.; Costain, G.; Walker, S.; Egger, G.; Thiruvahindrapuram, B.; et al. Rare exonic deletions implicate the synaptic organizer Gephyrin (GPHN) in risk for autism, schizophrenia and seizures. Hum. Mol. Genet. 2013, 22, 2055–2066. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, S.E.; Makarov, V.; Kirov, G.; Addington, A.M.; McClellan, J.; Yoon, S.; Perkins, D.O.; Dickel, D.E.; Kusenda, M.; Krastoshevsky, O.; et al. Microduplications of 16p11.2 are associated with schizophrenia. Nat. Genet. 2009, 41, 1223–1227. [Google Scholar] [CrossRef]
- Moreno-De-Luca, D.; SGENE Consortium; Mulle, J.G.; Simons Simplex Collection Genetics Consortium; Kaminsky, E.B.; Sanders, S.J.; Gene, S.T.A.R.; Myers, S.M.; Adam, M.P.; Pakula, A.T.; et al. Deletion 17q12 Is a Recurrent Copy Number Variant that Confers High Risk of Autism and Schizophrenia. Am. J. Hum. Genet. 2010, 87, 618–630. [Google Scholar] [Green Version]
- Weiss, L.A.; Shen, Y.; Korn, J.M.; Arking, D.E.; Miller, D.T.; Fossdal, R.; Saemundsen, E.; Stefansson, H.; Ferreira, M.A.R.; Green, T.; et al. Association between microdeletion and microduplication at 16p11.2 and autism. N. Engl. J. Med. 2008, 358, 667–675. [Google Scholar] [CrossRef]
- Chisholm, K.; Lin, A.; Armando, M. Schizophrenia Spectrum Disorder and Autism Spectrum Disorder. In Psychiatric Symptoms and Comorbidities in Autism Spectrum Disorder; Springer International Publishing: Berlin/Heidelberg, Germany, 2016; pp. 51–66. [Google Scholar] [CrossRef]
- Raja, M.; Azzoni, A. Autistic spectrum disorders and schizophrenia in the adult psychiatric setting: Diagnosis and comorbidity. Psychiatr. Danub. 2010, 22, 514–521. [Google Scholar]
- De Crescenzo, F.; Postorino, V.; Siracusano, M.; Riccioni, A.; Armando, M.; Curatolo, P.; Mazzone, L. Autistic Symptoms in Schizophrenia Spectrum Disorders: A Systematic Review and Meta-Analysis. Front. Psychiatry 2019, 10, 78. [Google Scholar] [CrossRef] [Green Version]
- Brugha, T.S.; McManus, S.; Bankart, J.; Scott, F.; Purdon, S.; Smith, J.; Bebbington, P.; Jenkins, R.; Meltzer, H. Epidemiology of autism spectrum disorders in adults in the community in England. Arch. Gen. Psychiatry 2011, 68, 459–465. [Google Scholar] [CrossRef]
- Kendler, K.S.; Gallagher, T.J.; Abelson, J.M.; Kessler, R.C. Lifetime prevalence, demographic risk factors, and diagnostic validity of nonaffective psychosis as assessed in a US community sample. The National Comorbidity Survey. Arch. Gen. Psychiatry 1996, 53, 1022–1031. [Google Scholar] [CrossRef]
- Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators; Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders—Autism and Developmental Disabilities Monitoring Network, 14 sites, United States, 2008. MMWR Surveill. Summ. 2012, 61, 1–19. [Google Scholar]
- Van Os, J.; Hanssen, M.; Bijl, R.V.; Vollebergh, W. Prevalence of psychotic disorder and community level of psychotic symptoms: An urban-rural comparison. Arch. Gen. Psychiatry 2001, 58, 663–668. [Google Scholar] [CrossRef]
- Eaves, L.C.; Ho, H.H. Young adult outcome of autism spectrum disorders. J. Autism Dev. Disord. 2008, 38, 739–747. [Google Scholar] [CrossRef]
- Hutton, J.; Goode, S.; Murphy, M.; Le Couteur, A.; Rutter, M. New-onset psychiatric disorders in individuals with autism. Autism 2008, 12, 373–390. [Google Scholar] [CrossRef]
- Volkmar, F.R.; Cohen, D.J. Comorbid association of autism and schizophrenia. Am. J. Psychiatry 1991, 148, 1705–1707. [Google Scholar]
- Abdallah, M.W.; Greaves-Lord, K.; Grove, J.; Nørgaard-Pedersen, B.; Hougaard, D.M.; Mortensen, E.L. Psychiatric comorbidities in autism spectrum disorders: Findings from a Danish Historic Birth Cohort. Eur. Child Adolesc. Psychiatry 2011, 20, 599–601. [Google Scholar] [CrossRef]
- Stahlberg, O.; Soderstrom, H.; Rastam, M.; Gillberg, C. Bipolar disorder, schizophrenia, and other psychotic disorders in adults with childhood onset AD/HD and/or autism spectrum disorders. J. Neural Transm. 2004, 111, 891–902. [Google Scholar] [CrossRef]
- Billstedt, E.; Gillberg, C.; Gillberg, C. Autism after adolescence: Population-based 13- to 22-year follow-up study of 120 individuals with autism diagnosed in childhood. J. Autism Dev. Disord. 2005, 35, 351–360. [Google Scholar] [CrossRef]
- Hofvander, B.; Delorme, R.; Chaste, P.; Nydén, A.; Wentz, E.; Ståhlberg, O.; Herbrecht, E.; Stopin, A.; Anckarsäter, H.; Gillberg, C.; et al. Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry 2009, 9, 35. [Google Scholar] [CrossRef]
- Lugnegård, T.; Hallerbäck, M.U.; Gillberg, C. Psychiatric comorbidity in young adults with a clinical diagnosis of Asperger syndrome. Res. Dev. Disabil. 2011, 32, 1910–1917. [Google Scholar] [CrossRef]
- Mouridsen, S.E.; Rich, B.; Isager, T. Epilepsy and other neurological diseases in the parents of children with infantile autism. A case control study. Child Psychiatry Hum. Dev. 2008, 39, 1–8. [Google Scholar] [CrossRef]
- Guinchat, V.; Cravero, C.; Diaz, L.; Périsse, D.; Xavier, J.; Amiet, C.; Gourfinkel-An, I.; Bodeau, N.; Wachtel, L.; Cohen, D.; et al. Acute behavioral crises in psychiatric inpatients with autism spectrum disorder (ASD): Recognition of concomitant medical or non-ASD psychiatric conditions predicts enhanced improvement. Res. Dev. Disabil. 2015, 38, 242–255. [Google Scholar] [CrossRef]
- Bakken, T.L.; Helverschou, S.B.; Eilertsen, D.E.; Heggelund, T.; Myrbakk, E.; Martinsen, H. Psychiatric disorders in adolescents and adults with autism and intellectual disability: A representative study in one county in Norway. Res. Dev. Disabil. 2010, 31, 1669–1677. [Google Scholar] [CrossRef]
- Joshi, G.; Petty, C.; Wozniak, J.; Henin, A.; Fried, R.; Galdo, M.; Kotarski, M.; Walls, S.; Biederman, J. The heavy burden of psychiatric comorbidity in youth with autism spectrum disorders: A large comparative study of a psychiatrically referred population. J. Autism Dev. Disord. 2010, 40, 1361–1370. [Google Scholar] [CrossRef]
- Mouridsen, S.E.; Rich, B.; Isager, T. Psychiatric disorders in adults diagnosed as children with atypical autism. A case control study. J. Neural Transm. 2008, 115, 135–138. [Google Scholar] [CrossRef]
- Lai, M.-C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism spectrum disorder. Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef]
- Solomon, M.; Olsen, E.; Niendam, T.; Ragland, J.D.; Yoon, J.; Minzenberg, M.; Carter, C.S. From lumping to splitting and back again: Atypical social and language development in individuals with clinical-high-risk for psychosis, first episode schizophrenia, and autism spectrum disorders. Schizophr. Res. 2011, 131, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Chisholm, K.; Lin, A.; Abu-Akel, A.; Wood, S.J. The association between autism and schizophrenia spectrum disorders: A review of eight alternate models of co-occurrence. Neurosci. Biobehav. Rev. 2015, 55, 173–183. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study, Year | Country | Diagnosis, n | ASD Severity | Age (Mean/Median, SD/Range) | % Female | IQ/Intellectual Disability | Setting | % Psychotic | Scale |
|---|---|---|---|---|---|---|---|---|---|
| Bakken, 2010 | Norway | AD and Intellectual Disability (ICD-10), n = 62 | NR | 24.3 (14–57) | 27% | IQ < 34, n = 30 | Specialist outpatient | 25.10% | PAC—psychosis subscale * |
| IQ 35–70, n = 32 | |||||||||
| Billstedt, 2005 | Sweden | AD (DSM-III-R), n = 73 | AD: GAF = 22.2 (SD 16.8); Atypical autism: GAF = 18.5 (SD 15.2) | NR | 30% | IQ < 50, n = 56; | Specialist outpatient | 7% (AD); 9% (Atypical autism) | Psychiatrist assessment |
| Atypical autism (DSM-III-R), n = 35 | IQ 50–70, n = 42, IQ 71–85, n = 17; IQ > 85, n = 5 | ||||||||
| Eaves, 2008 | Canada | ASD (DSM-IV), n = 48 | CARS = 31.0 (5.9) | 24 (19–31) | 22.90% | Verbal IQ < 34, n = 7; IQ 35–49, n = 16; IQ 50–69, n = 15; IQ > 70, n = 8 | Specialist outpatient | 0% | NR |
| Hofvander, 2009 | Sweden, France | ASD (DSM-IV), n = 122 | NR | 29 (16–60) | 33% | Normal IQ | Specialist outpatient | 12% | NR |
| Joshi, 2010 | US | ASD (DSM-III-R), n = 217 | NR | 9.7 (3.6) Range = 3–17 | 13% | NR | Specialist outpatient | 20% | K-SADS-E |
| Lugnegård, 2011 | Sweden | Asperger syndrome, n = 54 | NR | 27 (3.9) | 51.85% | Mean IQ = 102 (SD 12) | Specialist outpatient | 3.70% | NR |
| Guinchat, 2015 | France | ASD (ICD-10), n = 58 | GAF = 17.66 (9.05); | 15.66 (4.07) | 24.13% | Severe/profound ID, n = 40 (71.00%) | Specialist inpatient | 9% | NR |
| CARS = 40.18 (4.76) | Range = 10.9–37 | ||||||||
| Abdallah, 2011 | Denmark | ASD (ICD-8/ICD 10), n = 414 | NR | 16.28 (4.55) | 19.08% | ICD-8/ICD-10 diagnosis n = 88 (21.3%) | NR | SCZ (ICD-8/ICD-10) 2.9% | NR |
| Raja, | Italy | ASD (DSM-IV-TR), n = 26 | NR | 30.2 (9.8) | 3.85% | IQ mean 83.5 (SD 18.2) | Specialist PICU | SCZ (DSM-IV-TR) 61.54% | NR |
| 2010 | |||||||||
| Hutton, 2008 | UK | ASD (ICD-10), n = 135 | NR | 34.9 (21–57) | 22.96% | IQ > 30 in all patients | Specialist outpatient | 0% | NR |
| Mouridsen, 2008a | Denmark | Atypical autism (ICD-10), n = 89 | NR | 45.3 (7.2) | 34.83% | IQ < 50, n = 20, | Specialist inpatient | 34.80% | NR |
| IQ > 50, n = 68 | |||||||||
| Mouridsen, 2008b | Denmark | Infantile autism (ICD-9), n = 118 | NR | 5.4 (2.5), Range = 2–15 | 26% | IQ < 50, n = 48 | Specialist inpatient | 6.60% | NR |
| IQ 50–69, n = 30 IQ > 69, n = 32 | |||||||||
| Stahlberg, 2004 | Sweden | ASD (ICD-10/DSM-IV), n = 129 | GAF = 45.8 (10.8) | 30.6 (9.7) | 38.75% | IQ mean 86.2 | Specialist outpatient | SCZ 2.94%; | NR |
| (SD 21.3) | SCZ or other psychotic disorders (non-bipolar) 7.8% | ||||||||
| Volkmar, 1991 | US | ASD (DSM-III-R), n = 163 | NR | 24.1 (5.58) | 14.72% | NR | Specialist outpatient | SCZ (DSM-II-R) 0.61% | NR |
| Range = 15–41 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Giorgi, R.; De Crescenzo, F.; D’Alò, G.L.; Rizzo Pesci, N.; Di Franco, V.; Sandini, C.; Armando, M. Prevalence of Non-Affective Psychoses in Individuals with Autism Spectrum Disorders: A Systematic Review. J. Clin. Med. 2019, 8, 1304. https://doi.org/10.3390/jcm8091304
De Giorgi R, De Crescenzo F, D’Alò GL, Rizzo Pesci N, Di Franco V, Sandini C, Armando M. Prevalence of Non-Affective Psychoses in Individuals with Autism Spectrum Disorders: A Systematic Review. Journal of Clinical Medicine. 2019; 8(9):1304. https://doi.org/10.3390/jcm8091304
Chicago/Turabian StyleDe Giorgi, Riccardo, Franco De Crescenzo, Gian Loreto D’Alò, Nicola Rizzo Pesci, Valeria Di Franco, Corrado Sandini, and Marco Armando. 2019. "Prevalence of Non-Affective Psychoses in Individuals with Autism Spectrum Disorders: A Systematic Review" Journal of Clinical Medicine 8, no. 9: 1304. https://doi.org/10.3390/jcm8091304
APA StyleDe Giorgi, R., De Crescenzo, F., D’Alò, G. L., Rizzo Pesci, N., Di Franco, V., Sandini, C., & Armando, M. (2019). Prevalence of Non-Affective Psychoses in Individuals with Autism Spectrum Disorders: A Systematic Review. Journal of Clinical Medicine, 8(9), 1304. https://doi.org/10.3390/jcm8091304