Raman Spectroscopy Analysis for Optical Diagnosis of Oral Cancer Detection

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Pre-Processing and Data Analysis
2.3. Raman Spectroscopy (RS)
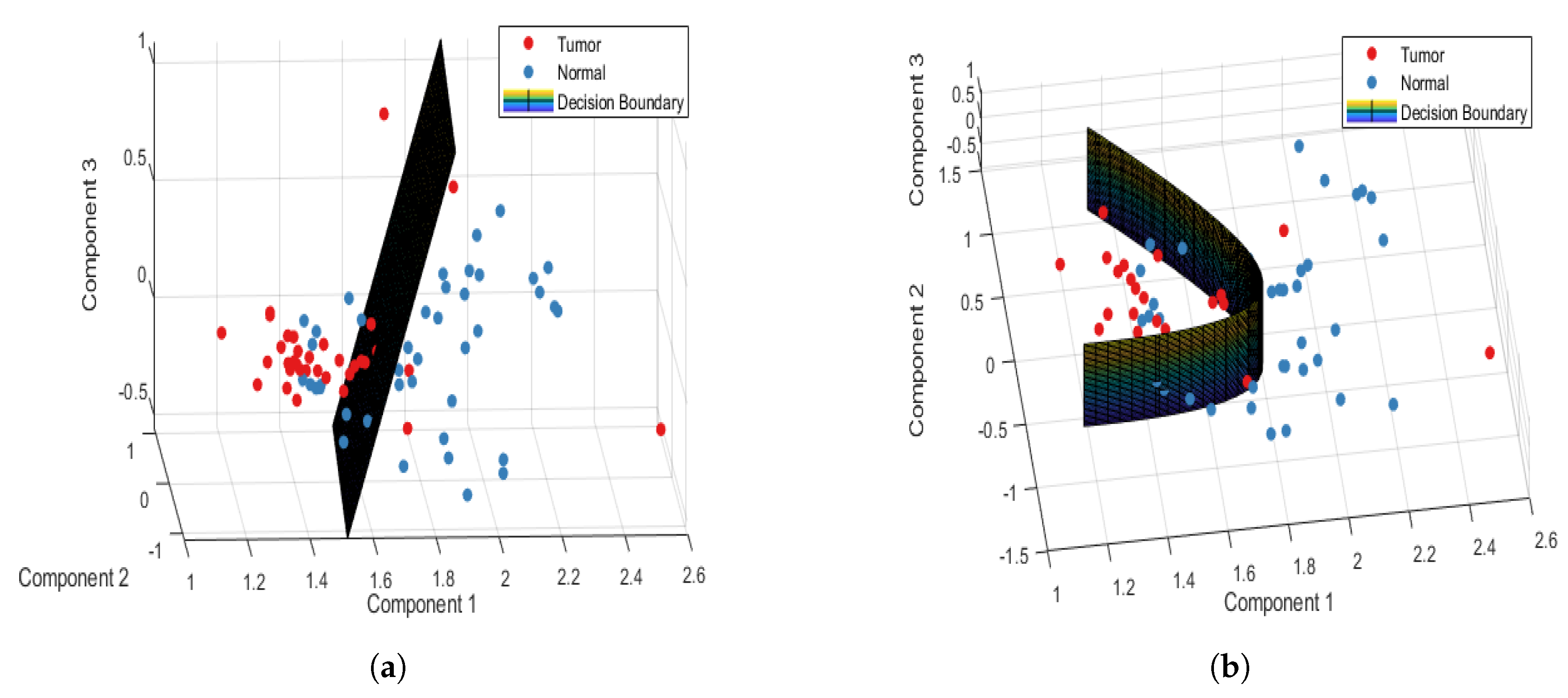
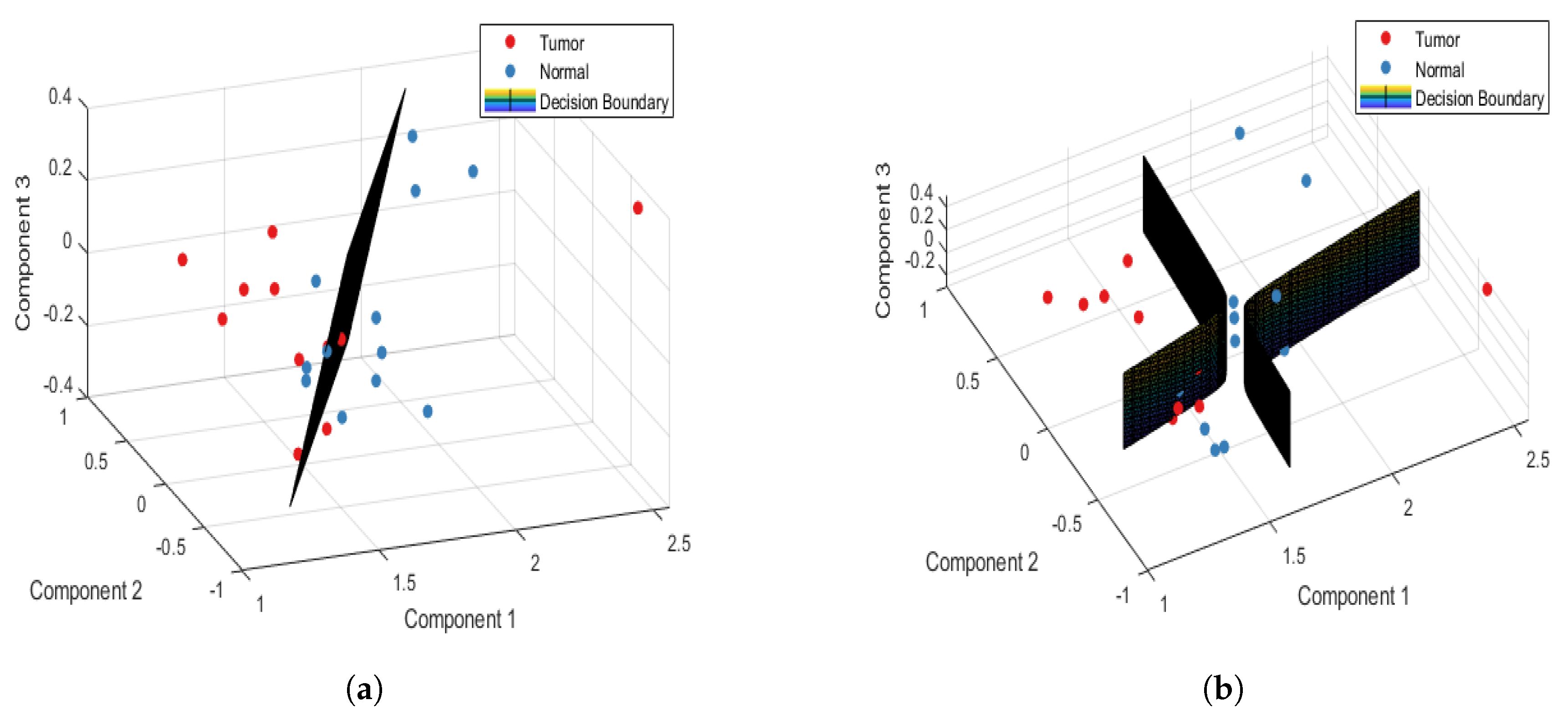
2.4. Multivariate Analysis
3. Results and Discussion
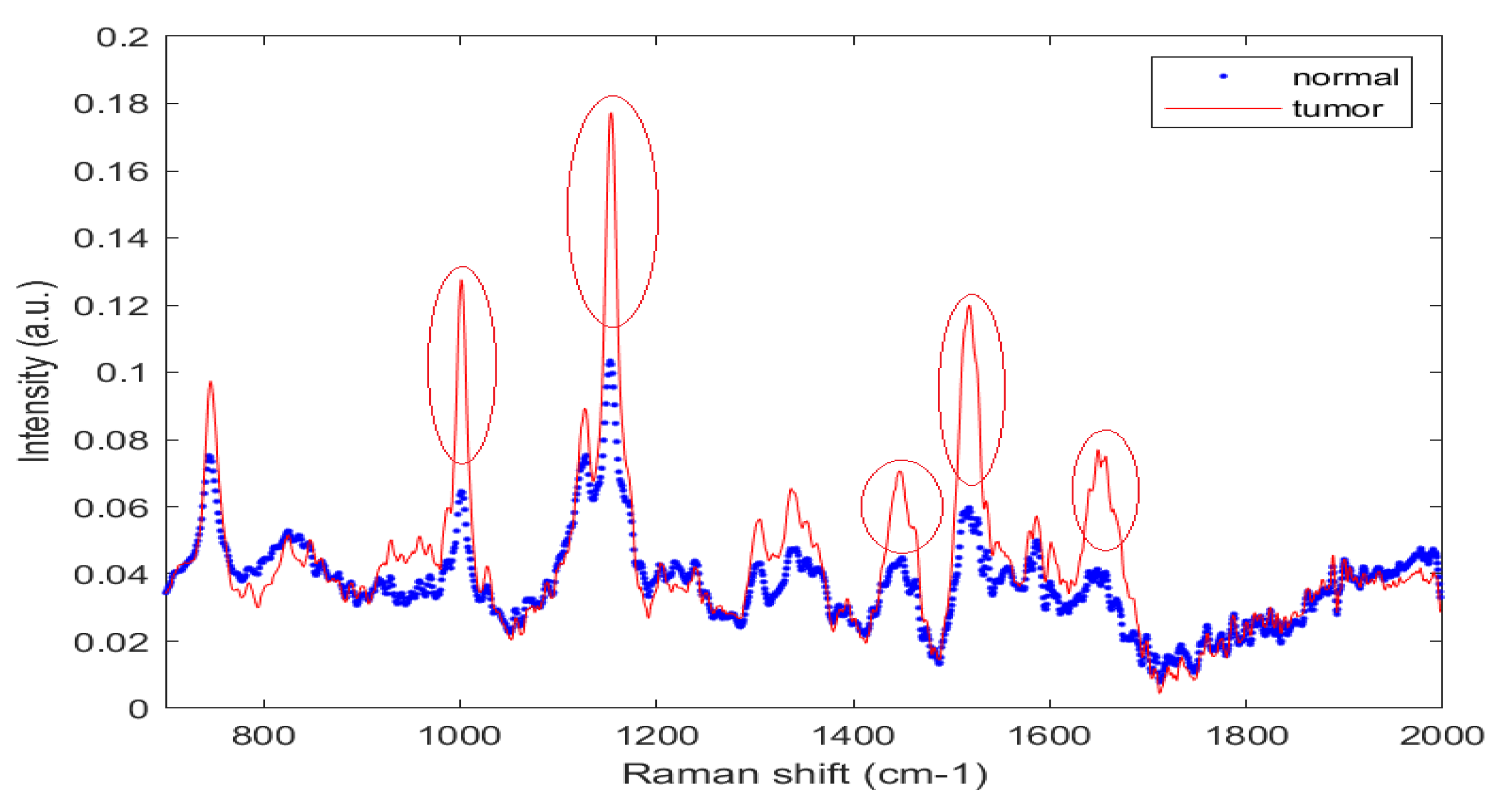
3.1. Finger Print Region
3.2. Analysis of Normal and Tumor Sample Data
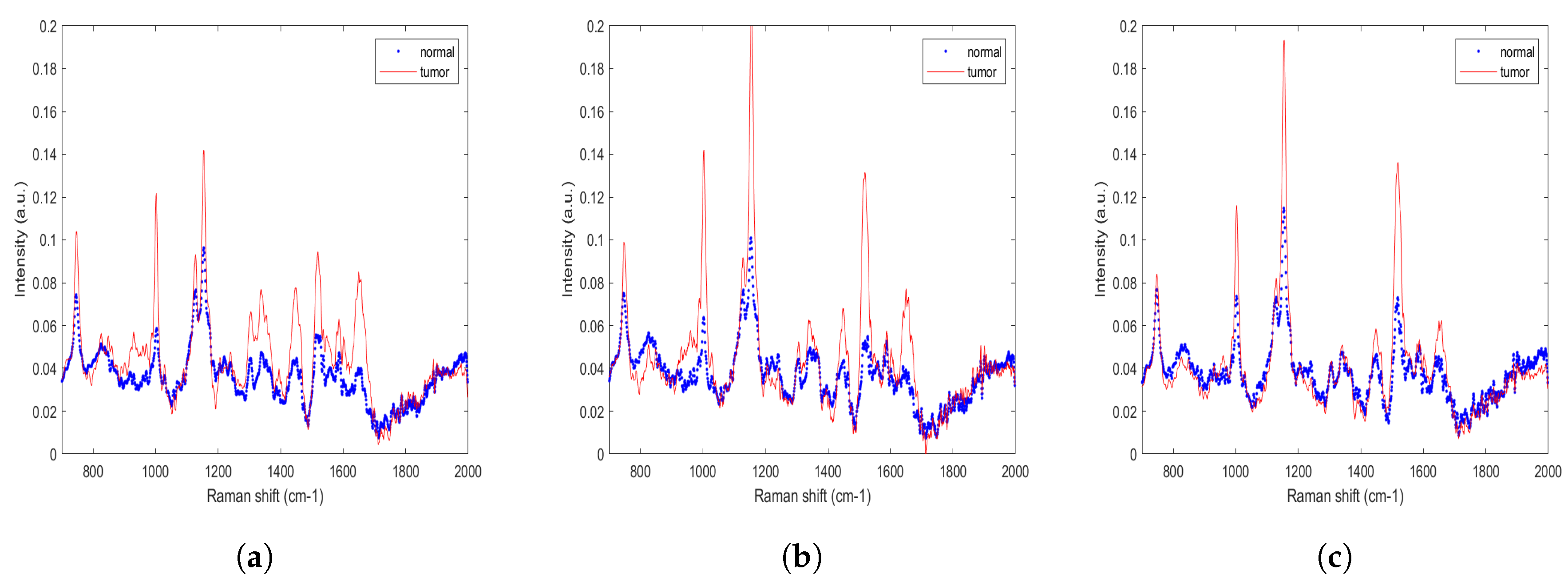
3.3. Analysis of Data from Normal and Tumor Samples from Tongue, Buccal Mucosa, and Gingiva Sub-Sites
4. Validation Methods
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Reddy, S.S.; Sharma, S.; Mysorekar, V. Expression of Epstein–barr virus among oral potentially malignant disorders and oral squamous cell carcinomas in the South Indian tobacco-chewing population. J. Oral Pathol. Med. 2017, 46, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Samal, S.K.; Routray, S.; Dash, R.; Dixit, A. Identification of oral cancer related candidate genes by integrating protein-protein interactions, gene ontology, pathway analysis and immunohistochemistry. Sci. Rep. 2017, 7, 2472. [Google Scholar] [CrossRef] [PubMed]
- Stewart, B.; Wild, C.P. World Cancer Report 2014. Available online: https://www.drugsandalcohol.ie/28525/1/World%20Cancer%20Report.pdf (accessed on 23 August 2019).
- Allen, C.T.; Law, J.H.; Dunn, G.P.; Uppaluri, R. Emerging insights into head and neck cancer metastasis. Head Neck 2013, 35, 1669–1678. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, H.; Baharvand, M.; Mehdipour, M. Oral potentially malignant disorders: An overview of more than 20 entities. J. Dent. Res. Dent. Clin. Dent. Prospect. 2014, 8, 6. [Google Scholar] [CrossRef]
- Liu, D.; Zhao, X.; Zeng, X.; Dan, H.; Chen, Q. Non-invasive techniques for detection and diagnosis of oral potentially malignant disorders. Tohoku J. Exp. Med. 2016, 238, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Cordero, E.; Latka, I.; Matthäus, C.; Schie, I.W.; Popp, J. In-vivo Raman spectroscopy: From basics to applications. J. Biomed. Opt. 2018, 23, 071210. [Google Scholar] [CrossRef] [PubMed]
- Vašková, H. A powerful tool for material identification: Raman spectroscopy. Int. J. Math. Model. Methods Appl. Sci. 2011, 5, 1205–1212. [Google Scholar]
- Pence, I.; Mahadevan-Jansen, A. Clinical instrumentation and applications of Raman spectroscopy. Chem. Soc. Rev. 2016, 45, 1958–1979. [Google Scholar] [CrossRef] [Green Version]
- Cui, S.; Zhang, S.; Yue, S. Raman Spectroscopy and Imaging for Cancer Diagnosis. J. Healthc. Eng. 2018, 2018. [Google Scholar] [CrossRef]
- Notingher, I. Raman spectroscopy cell-based biosensors. Sensors 2007, 7, 1343–1358. [Google Scholar] [CrossRef]
- Bakker Schut, T.; Witjes, M.; Sterenborg, H.; Speelman, O.; Roodenburg, J.; Marple, E.; Bruining, H.; Puppels, G. In vivo detection of dysplastic tissue by Raman spectroscopy. Anal. Chem. 2000, 72, 6010–6018. [Google Scholar] [CrossRef]
- Sunder, N.S.; Rao, N.N.; Kartha, V.; Ullas, G.; Kurien, J. Laser Raman spectroscopy: A novel diagnostic tool for oral cancer. J. Orofac. Sci. 2011, 3, 15–19. [Google Scholar]
- Malini, R.; Venkatakrishna, K.; Kurien, J.M.; Pai, K.; Rao, L.; Kartha, V.; Krishna, C.M. Discrimination of normal, inflammatory, premalignant, and malignant oral tissue: A Raman spectroscopy study. Biopolym. Orig. Res. Biomol. 2006, 81, 179–193. [Google Scholar] [CrossRef]
- Singh, S.; Deshmukh, A.; Chaturvedi, P.; Krishna, C.M. In vivo Raman spectroscopic identification of premalignant lesions in oral buccal mucosa. J. Biomed. Opt. 2012, 17, 105002. [Google Scholar] [CrossRef]
- Dai, W.Y.; Lee, S.; Hsu, Y.C. Discrimination between oral cancer and healthy cells based on the adenine signature detected by using Raman spectroscopy. J. Raman Spectrosc. 2018, 49, 336–342. [Google Scholar] [CrossRef]
- Chen, P.H.; Shimada, R.; Yabumoto, S.; Okajima, H.; Ando, M.; Chang, C.T.; Lee, L.T.; Wong, Y.K.; Chiou, A.; Hamaguchi, H.O. Automatic and objective oral cancer diagnosis by Raman spectroscopic detection of keratin with multivariate curve resolution analysis. Sci. Rep. 2016, 6, 20097. [Google Scholar] [CrossRef] [Green Version]
- Cals, F.L.; Bakker Schut, T.C.; Koljenović, S.; Puppels, G.J.; de Jong, R.J.B. Method development: Raman spectroscopy-based histopathology of oral mucosa. J. Raman Spectrosc. 2013, 44, 963–972. [Google Scholar] [CrossRef]
- Guze, K.; Pawluk, H.C.; Short, M.; Zeng, H.; Lorch, J.; Norris, C.; Sonis, S. Pilot study: Raman spectroscopy in differentiating premalignant and malignant oral lesions from normal mucosa and benign lesions in humans. Head Neck 2015, 37, 511–517. [Google Scholar] [CrossRef]
- Knipfer, C.; Motz, J.; Adler, W.; Brunner, K.; Gebrekidan, M.T.; Hankel, R.; Agaimy, A.; Will, S.; Braeuer, A.; Neukam, F.W.; et al. Raman difference spectroscopy: A non-invasive method for identification of oral squamous cell carcinoma. Biomed. Opt. Express 2014, 5, 3252–3265. [Google Scholar] [CrossRef]
- Lau, D.P.; Huang, Z.; Lui, H.; Man, C.S.; Berean, K.; Morrison, M.D.; Zeng, H. Raman spectroscopy for optical diagnosis in normal and cancerous tissue of the nasopharynx—Preliminary findings. Lasers Surg. Med. 2003, 32, 210–214. [Google Scholar] [CrossRef]
- Lau, D.P.; Huang, Z.; Lui, H.; Anderson, D.W.; Berean, K.; Morrison, M.D.; Shen, L.; Zeng, H. Raman spectroscopy for optical diagnosis in the larynx: Preliminary findings. Lasers Surg. Med. Off. J. Am. Soc. Laser Med. Surg. 2005, 37, 192–200. [Google Scholar] [CrossRef]
- Sahu, A.; Tawde, S.; Pai, V.; Gera, P.; Chaturvedi, P.; Nair, S.; Krishna, C.M. Raman spectroscopy and cytopathology of oral exfoliated cells for oral cancer diagnosis. Anal. Methods 2015, 7, 7548–7559. [Google Scholar] [CrossRef]
- Sahu, A.; Sawant, S.; Mamgain, H.; Krishna, C.M. Raman spectroscopy of serum: An exploratory study for detection of oral cancers. Analyst 2013, 138, 4161–4174. [Google Scholar] [CrossRef]
- Sahu, A.; Sawant, S.; Talathi-Desai, S.; Murali Krishna, C. Raman spectroscopy of serum: A study on oral cancers. Biomed. Spectrosc. Imaging 2015, 4, 171–187. [Google Scholar]
- Barroso, E.; Smits, R.; Bakker Schut, T.; Ten Hove, I.; Hardillo, J.; Wolvius, E.; Baatenburg de Jong, R.; Koljenovic, S.; Puppels, G. Discrimination between oral cancer and healthy tissue based on water content determined by Raman spectroscopy. Anal. Chem. 2015, 87, 2419–2426. [Google Scholar] [CrossRef]
- Cals, F.L.; Schut, T.C.B.; Hardillo, J.A.; De Jong, R.J.B.; Koljenović, S.; Puppels, G.J. Investigation of the potential of Raman spectroscopy for oral cancer detection in surgical margins. Lab. Investig. 2015, 95, 1186–1196. [Google Scholar] [CrossRef] [Green Version]
- Cals, F.L.; Koljenović, S.; Hardillo, J.A.; de Jong, R.J.B.; Schut, T.C.B.; Puppels, G.J. Development and validation of Raman spectroscopic classification models to discriminate tongue squamous cell carcinoma from non-tumorous tissue. Oral Oncol. 2016, 60, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Kerr, L.T.; Byrne, H.J.; Hennelly, B.M. Optimal choice of sample substrate and laser wavelength for Raman spectroscopic analysis of biological specimen. Anal. Methods 2015, 7, 5041–5052. [Google Scholar] [CrossRef] [Green Version]
- Siqueira, L.F.; Júnior, R.F.A.; de Araújo, A.A.; Morais, C.L.; Lima, K.M. LDA vs. QDA for FT-MIR prostate cancer tissue classification. Chemom. Intell. Lab. Syst. 2017, 162, 123–129. [Google Scholar] [CrossRef]
- Xue, J.H.; Titterington, D.M. Do unbalanced data have a negative effect on LDA? Pattern Recog. 2008, 41, 1558–1571. [Google Scholar] [CrossRef] [Green Version]
- Eisenbeis, R.A. Pitfalls in the application of discriminant analysis in business, finance, and economics. J. Financ. 1977, 32, 875–900. [Google Scholar] [CrossRef]
- Parker, F.S. Applications of Infrared, Raman, and Resonance Raman Spectroscopy in Biochemistry; Springer Science & Business Media: Berlin, Germany, 1983. [Google Scholar]
- Movasaghi, Z.; Rehman, S.; Rehman, I.U. Raman spectroscopy of biological tissues. Appl. Spectrosc. Rev. 2007, 42, 493–541. [Google Scholar] [CrossRef]
- Huang, Z.; McWilliams, A.; Lui, H.; McLean, D.I.; Lam, S.; Zeng, H. Near-infrared Raman spectroscopy for optical diagnosis of lung cancer. Int. J. Cancer 2003, 107, 1047–1052. [Google Scholar] [CrossRef]
- Mahadevan-Jansen, A.; Richards-Kortum, R. Raman spectroscopy for cancer detection: A review. In Proceedings of the 19th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Magnificent Milestones and Emerging Opportunities in Medical Engineering (Cat. No. 97CH36136), Chicago, IL, USA, 30 October–2 November 1997; Volume 6, pp. 2722–2728. [Google Scholar]
- Ciano, J.; Beatty, B.L. Regional quantitative histological variations in human oral mucosa. Anat. Rec. 2015, 298, 562–578. [Google Scholar] [CrossRef]
- Carvalho, L.F.C.; Nogueira, M.S.; Bhattacharjee, T.; Neto, L.P.; Daun, L.; Mendes, T.O.; Rajasekaran, R.; Chagas, M.; Martin, A.A.; Soares, L.E.S. In vivo Raman spectroscopic characteristics of different sites of the oral mucosa in healthy volunteers. Clin. Oral Investig. 2018, 23, 3021–3031. [Google Scholar] [CrossRef]
- Liu, S.A.; Wang, C.C.; Jiang, R.S.; Lee, F.Y.; Lin, W.J.; Lin, J.C. Pathological features and their prognostic impacts on oral cavity cancer patients among different subsites–A singe institute’s experience in Taiwan. Sci. Rep. 2017, 7, 7451. [Google Scholar] [CrossRef]
- Freier, K.; Joos, S.; Flechtenmacher, C.; Devens, F.; Benner, A.; Bosch, F.X.; Lichter, P.; Hofele, C. Tissue microarray analysis reveals site-specific prevalence of oncogene amplifications in head and neck squamous cell carcinoma. Cancer Res. 2003, 63, 1179–1182. [Google Scholar]
- Sathyan, K.; Sailasree, R.; Jayasurya, R.; Lakshminarayanan, K.; Abraham, T.; Nalinakumari, K.; Abraham, E.K.; Kannan, S. Carcinoma of tongue and the buccal mucosa represent different biological subentities of the oral carcinoma. J. Cancer Res. Clin. Oncol. 2006, 132, 601–609. [Google Scholar] [CrossRef]
- Zhu, W.; Zeng, N.; Wang, N. Sensitivity, specificity, accuracy, associated confidence interval and ROC analysis with practical SAS implementations. NESUG Proc. Health Care Life Sci. Balt. Md. 2010, 19, 67. [Google Scholar]
- Cals, F.L.; Schut, T.B.; Caspers, P.; de Jong, R.B.; Koljenović, S.; Puppels, G.J. Raman spectroscopic analysis of the molecular composition of oral cavity squamous cell carcinoma and healthy tongue tissue. Analyst 2018, 143, 4090–4102. [Google Scholar] [CrossRef]
- Wang, H.; Zheng, H. Model Validation, Machine Learning. In Encyclopedia of Systems Biology; Dubitzky, W., Wolkenhauer, O., Cho, K.H., Yokota, H., Eds.; Springer: New York, NY, USA, 2013; pp. 1406–1407. [Google Scholar]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning; Springer: New York, NY, USA, 2013; Volume 112. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sub-Sites | Tongue | Buccal Mucosa | Gingiva | Total |
|---|---|---|---|---|
| Tumor | 13 | 19 | 12 | 44 |
| Normal | 11 | 14 | 11 | 36 |
| Dataset | Confusion Table | Performance Parameters | ||||
|---|---|---|---|---|---|---|
| PCA-LDA | Tumor | Normal | Total | Accuracy (%) | Sensitivity (%) | Specificity (%) |
| Tumor | 177 | 43 | 220 | 74.50 | 80.45 | 67.22 |
| Normal | 59 | 121 | 180 | |||
| PCA-QDA | Tumor | Normal | Total | Accuracy (%) | Sensitivity (%) | Specificity (%) |
| Tumor | 184 | 36 | 220 | 81.75 | 83.63 | 79.44 |
| Normal | 37 | 143 | 180 | |||
| Dataset | Confusion Table | Performance Parameters | ||||
|---|---|---|---|---|---|---|
| PCA-LDA | Tumor | Normal | Total | Accuracy (%) | Sensitivity (%) | Specificity (%) |
| Tumor | 34 | 10 | 44 | 81.25 | 77.27 | 86.11 |
| Normal | 5 | 31 | 36 | |||
| PCA-QDA | Tumor | Normal | Total | Accuracy (%) | Sensitivity (%) | Specificity (%) |
| Tumor | 40 | 4 | 44 | 87.50 | 90.90 | 83.33 |
| Normal | 6 | 30 | 36 | |||
| Patient-Wise: Tongue | Accuracy (%) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| PCA-LDA | 79.16 | 92.30 | 63.63 |
| PCA-QDA | 87.50 | 100.00 | 72.72 |
| Patient-Wise: Buccal | Accuracy (%) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| PCA-LDA | 84.84 | 78.94 | 92.85 |
| PCA-QDA | 87.87 | 84.21 | 92.85 |
| Patient-Wise: Gingiva | Accuracy (%) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| PCA-LDA | 91.30 | 91.66 | 90.90 |
| PCA-QDA | 87.12 | 75.00 | 100.00 |
| Error Rate | PCA-LDA (%) | PCA-QDA (%) | Validation: K-fold (%) | Validation: LOOCV (%) |
|---|---|---|---|---|
| Point-wise | 25.50 | 16.27 | 18.25 | 17.00 |
| Patient-wise | 18.75 | 12.50 | 16.25 | 11.25 |
| Error Rate | PCA-LDA (%) | PCA-QDA (%) | Validation: K-fold (%) | Validation: LOOCV (%) |
|---|---|---|---|---|
| Tongue | 20.83 | 12.50 | 16.67 | 16.67 |
| Buccal | 15.16 | 12.13 | 18.18 | 21.21 |
| Gingiva | 8.60 | 12.88 | 13.04 | 19.04 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeng, M.-J.; Sharma, M.; Sharma, L.; Chao, T.-Y.; Huang, S.-F.; Chang, L.-B.; Wu, S.-L.; Chow, L. Raman Spectroscopy Analysis for Optical Diagnosis of Oral Cancer Detection. J. Clin. Med. 2019, 8, 1313. https://doi.org/10.3390/jcm8091313
Jeng M-J, Sharma M, Sharma L, Chao T-Y, Huang S-F, Chang L-B, Wu S-L, Chow L. Raman Spectroscopy Analysis for Optical Diagnosis of Oral Cancer Detection. Journal of Clinical Medicine. 2019; 8(9):1313. https://doi.org/10.3390/jcm8091313
Chicago/Turabian StyleJeng, Ming-Jer, Mukta Sharma, Lokesh Sharma, Ting-Yu Chao, Shiang-Fu Huang, Liann-Be Chang, Shih-Lin Wu, and Lee Chow. 2019. "Raman Spectroscopy Analysis for Optical Diagnosis of Oral Cancer Detection" Journal of Clinical Medicine 8, no. 9: 1313. https://doi.org/10.3390/jcm8091313
APA StyleJeng, M. -J., Sharma, M., Sharma, L., Chao, T. -Y., Huang, S. -F., Chang, L. -B., Wu, S. -L., & Chow, L. (2019). Raman Spectroscopy Analysis for Optical Diagnosis of Oral Cancer Detection. Journal of Clinical Medicine, 8(9), 1313. https://doi.org/10.3390/jcm8091313