Lung Metastases in Patients with Stage IV Pancreatic Cancer: Prevalence, Risk Factors, and Survival Impact

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Selection
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cancer Stat Facts: Pancreatic Cancer. Available online: https://seer.cancer.gov/statfacts/html/pancreas.html (accessed on 20 July 2019).
- Health Registry Annual Report 2016. Republic of China. Republic of China: Republic of China: Bureau of Health Promotion, Department of Health, Executive Yuan. 2018. Available online: http://www.hpa.gov.tw/BHPNet/Web/Stat/Statistics.aspx (accessed on 20 July 2019).
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. Folfirinox versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.A.; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef] [PubMed]
- Oweira, H.; Petrausch, U.; Helbling, D.; Schmidt, J.; Mannhart, M.; Mehrabi, A.; Schob, O.; Giryes, A.; Decker, M.; Abdel-Rahman, O. Prognostic value of site-specific metastases in pancreatic adenocarcinoma: A Surveillance Epidemiology and End Results database analysis. World J. Gastroenterol. 2017, 23, 1872–1880. [Google Scholar] [CrossRef] [PubMed]
- Downs-Canner, S.; Zenati, M.; Boone, B.A.; Varley, P.R.; Steve, J.; Hogg, M.E.; Zureikat, A.; Zeh, H.J.; Lee, K.K.W. The indolent nature of pulmonary metastases from ductal adenocarcinoma of the pancreas. J. Surg. Oncol. 2015, 112, 80–85. [Google Scholar] [CrossRef] [Green Version]
- Arnaoutakis, G.J.; Rangachari, D.; Laheru, D.A.; Iacobuzio-Donahue, C.A.; Hruban, R.H.; Herman, J.M.; Edil, B.H.; Pawlik, T.M.; Schulick, R.D.; Cameron, J.L.; et al. Pulmonary resection for isolated pancreatic adenocarcinoma metastasis: An analysis of outcomes and survival. J. Gastrointest. Surg. 2011, 15, 1611–1617. [Google Scholar] [CrossRef]
- Kruger, S.; Haas, M.; Burger, P.J.; Ormanns, S.; Modest, D.P.; Westphalen, C.B.; Michl, M.; Kleespies, A.; Angele, M.K.; Hartwig, W.; et al. Isolated pulmonary metastases define a favorable subgroup in metastatic pancreatic cancer. Pancreatology 2016, 16, 593–598. [Google Scholar] [CrossRef]
- Decoster, C.; Gilabert, M.; Autret, A.; Turrini, O.; Oziel-Taieb, S.; Poizat, F.; Giovannini, M.; Viens, P.; Iovanna, J.; Raoul, J.L. Heterogeneity of metastatic pancreatic adenocarcinoma: Lung metastasis show better prognosis than liver metastasis—A case control study. Oncotarget 2016, 7, 45649–45655. [Google Scholar] [CrossRef]
- Lovecek, M.; Skalicky, P.; Chudacek, J.; Szkorupa, M.; Svebisova, H.; Lemstrova, R.; Ehrmann, J.; Melichar, B.; Yogeswara, T.; Klos, D.; et al. Different clinical presentations of metachronous pulmonary metastases after resection of pancreatic ductal adenocarcinoma: Retrospective study and review of the literature. World J. Gastroenterol. 2017, 23, 6420–6428. [Google Scholar] [CrossRef]
- Wangjam, T.; Zhang, Z.; Zhou, X.C.; Lyer, L.; Faisal, F.; Soares, K.C.; Fishman, E.; Hruban, R.H.; Herman, J.M.; Laheru, D.; et al. Resected pancreatic ductal adenocarcinomas with recurrence limited in lung have a significantly better prognosis than those with other recurrence patterns. Oncotarget 2015, 6, 36903–36910. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, K.; Miyamoto, A.; Hama, N.; Asaoka, T.; Maeda, S.; Omiya, H.; Takami, K.; Doki, Y.; Mori, M.; Nakamori, S. Survival impact of pulmonary metastasis as recurrence of pancreatic ductal adenocarcinoma. Dig. Surg. 2015, 32, 464–471. [Google Scholar] [CrossRef] [PubMed]
- UICC TNM. Classification of Malignant Tumours, 7th ed.; Wiley & Liss: New York, NY, USA, 2009. [Google Scholar]
- Lee, S.H.; Chang, P.H.; Chen, P.T.; Lu, C.H.; Hung, Y.S.; Tsang, N.M.; Hung, C.Y.; Chen, J.S.; Hsu, H.C.; Chen, Y.Y.; et al. Association of time interval between cancer diagnosis and initiation of palliative chemotherapy with overall survival in patients with unresectable pancreatic cancer. Cancer Med. 2019, 8, 3471–3478. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.L.; Chen, Y.Y.; Lu, C.H.; Hung, C.Y.; Kuo, Y.C.; Chen, J.S.; Hsu, H.C.; Chen, P.T.; Chang, P.H.; Hung, Y.S.; et al. Effect of S-1 on survival outcomes in 838 patients with advanced pancreatic cancer: A 7-year multicenter observational cohort study in Taiwan. Cancer Med. 2019, 8, 2085–2094. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.C.; Chen, Y.Y.; Hung, C.Y.; Chen, J.S.; Lu, C.H.; Chang, P.H. Evolution of the chemotherapeutic landscape and survival outcome in patients with metastatic pancreatic cancer: A four-institute cohort study in Taiwan, 2010–2016. Cancer Manag. Res. 2019, 11, 2119–2127. [Google Scholar] [CrossRef] [PubMed]
- Pappas, S.G.; Christians, K.K.; Tolat, P.P.; Mautz, A.P.; Lal, A.; McElroy, L.; Gamblin, T.C.; Turaga, K.K.; Tsai, S.; Erickson, B.; et al. Staging chest computed tomography and positron emission tomography in patients with pancreatic adenocarcinoma: Utility or futility? HPB (Oxf.) 2014, 16, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Mehtsun, W.T.; Chipidza, F.E.; Fernández-Del Castillo, C.; Hemingway, K.; Fong, Z.V.; Chang, D.C.; Pandharipande, P.; Clark, J.W.; Allen, J.; Hong, T.S.; et al. Are staging computed tomography (CT) scans of the chest necessary in pancreatic adenocarcinoma? Ann. Surg. Oncol. 2018, 25, 3936–3942. [Google Scholar] [CrossRef] [PubMed]
- Nordback, I.; Saaristo, R.; Piironen, A.; Sand, J. Chest computed tomography in the staging of pancreatic and periampullary carcinoma. Scand. J. Gastroenterol. 2004, 39, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Poruk, K.E.; Kim, Y.; Cameron, J.L.; He, J.; Eckhauser, F.E.; Rezaee, N.; Herman, J.; Laheru, D.; Zheng, L.; Fishman, E.K.; et al. What is the significance of indeterminate pulmonary nodules in patients undergoing resection for pancreatic adenocarcinoma? J. Gastrointest. Surg. 2015, 19, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.T.; Nguyen, D.C.; Raptis, C.; Menias, C.O.; Zhou, G.; Wang-Gillam, A.; Linehan, D.C.; Hawkins, W.G.; Strasberg, S.M.; Fields, R.C. Natural history of preoperative subcentimeter pulmonary nodules in patients with resectable pancreatic adenocarcinoma: A retrospective cohort study. Ann. Surg. 2015, 261, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.S.; Hung, C.Y.; Chang, H.; Liu, C.T.; Chen, Y.Y.; Lu, C.H.; Chang, P.H.; Hung, Y.S.; Chou, W.C. Venous thromboembolism in asian patients with pancreatic cancer following palliative chemotherapy: Low incidence but a negative prognosticator for those with early onset. Cancers (Basel) 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Hohla, F.; Hopfinger, G.; Romeder, F.; Rinnerthaler, G.; Bezan, A.; Stättner, S.; Hauser-Kronberger, C.; Ulmer, H.; Greil, R. Female gender may predict response to FOLFIRINOX in patients with unresectable pancreatic cancer: A single institution retrospective review. Int. J. Oncol. 2014, 44, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.; Mukherjee, A.; Karanam, B.; Davis, M.; Jaynes, J.; Reams, R.R.; Dean-Colomb, W.; Yates, C. African Americans with pancreatic ductal adenocarcinoma exhibit gender differences in Kaiso expression. Cancer Lett. 2016, 380, 513–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Median age, year (range) | 62 (25–88) |
| Sex | |
| male | 393 (60.1) |
| female | 261 (39.9) |
| Body mass index, Kg/m2, median (range) | 22.4 (13.0–36.2) |
| Active or ever smoker | 249 (38.1) |
| ECOG performance scale | |
| 0 or 1 | 450 (68.8) |
| 2 | 174 (26.6) |
| 3 | 30 (4.6) |
| Charlson comorbidity index | |
| 0 | 177 (27.1) |
| 1 | 227 (34.7) |
| 2 | 148 (22.6) |
| 3 | 79 (12.1) |
| 4 | 18 (2.8) |
| 5 | 5 (0.8) |
| Body weight loss, %, median (range) | 5 (0–33) |
| Primary tumor site + | |
| head | 224 (34.3) |
| body | 121 (18.5) |
| tail | 162 (24.8) |
| overlapping | 147 (22.5) |
| Tumor size, cm, median (range) + | 4.5 (1.4–14.0) |
| Previous pancreatectomy | |
| yes | 23 (3.5) |
| no | 631 (96.5) |
| T-classification, 7th AJCC + | |
| 1 | 13 (2) |
| 2 | 82 (12.5) |
| 3 | 188 (28.7) |
| 4 | 371 (56.7) |
| N-classification, 7th AJCC + | |
| 0 | 134 (20.5) |
| 1 | 520 (79.5) |
| Number of metastatic organ + | |
| 1 | 391 (59.8) |
| 2 | 191 (29.2) |
| 3 | 53 (8.1) |
| ≥4 | 19 (2.9) |
| Organ of metastases *,+ | |
| liver | 438 (67.0) |
| peritoneum | 239 (36.5) |
| distant lymph nodes | 150 (22.9) |
| lung | 98 (15.0) |
| others | 51 (6.1) |
| CEA, ng/dL | |
| ≤5 | 290 (44.3) |
| >5 | 364 (55.7) |
| CA19-9, ng/dL | |
| ≤37 | 130 (19.9) |
| >37 | 524 (80.1) |
| First-line chemotherapeutic regimen | |
| Gemcitabine monotherapy | 208 (31.8) |
| Gemcitabine plus platinum or 5-fluorouracil/TS-1 | 398 (60.9) |
| 5-fluorouracil +/- oxaliplatin +/- irinotecan | 15 (2.3) |
| TS-1 monotherapy | 32 (4.9) |
| Variable | Category | No of Lung Metastases/No of Total Patients (%) | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | |||
| Overall | 98/654 (15.0) | |||||
| Sex | male | 46/393 (11.7) | 1 | 1 | ||
| female | 52/261 (19.9) | 1.88 (1.22–2.89) | 0.004 | 1.90 (1.23–2.95) | 0.004 | |
| Age, year | ≤65 | 39/309 (12.6) | 1 | 1 | ||
| >65 | 59/345 (17.1) | 1.43 (0.93–2.21) | 0.09 | 1.37 (0.88–2.14) | 0.17 | |
| ECOG performance | 0 or 1 | 65/450 (14.4) | 1 | |||
| 2 | 27/174 (15.5) | 1.09 (0.67–1.77) | 0.74 | |||
| 3 | 6/30 (20) | 1.48 (0.58–3.76) | 0.41 | |||
| CCI | 0 or 1 | 57/404 (14.1) | 1 | |||
| >1 | 41/250 (16.4) | 1.19 (0.77–1.85) | 0.43 | |||
| Active or ever smoking | no | 63/405 (15.6) | 1 | |||
| yes | 35/249 (14.1) | 0.89 (0.57–1.39) | 0.60 | |||
| CEA, ng/dL | ≤5 | 46/290 (15.9) | 1 | |||
| >5 | 52/364 (14.3) | 0.88 (0.58–1.36) | 0.58 | |||
| CA19-9, ng/dL | ≤37 | 22/130 (16.9) | 1 | |||
| >37 | 76/524 (14.5) | 0.83 (0.49–1.41) | 0.49 | |||
| Body weight loss | ≤5% | 40/286 (14.0) | 1 | |||
| >5% | 47/287 (16.4) | 1.20 (0.76–1.90) | 0.43 | |||
| Primary tumor site | head | 32/224 (14.3) | 1 | |||
| body | 20/121 (16.5) | 1.19 (0.65–2.18) | 0.58 | |||
| tail | 24/162 (14.8) | 1.04 (0.59–1.85) | 0.88 | |||
| overlapping | 22/147 (15.0) | 0.59–1.90 | 0.86 | |||
| Tumor grade | well to moderate | 3/63 (4.8) | 1 | 1 | ||
| poorly or undifferentiated | 95/591 (16.1) | 3.83 (1.18–12.5) | 0.026 | 4.08 (1.24–13.4) | 0.020 | |
| T-classification | 1 or 2 | 12/95 (12.6) | 1 | |||
| 3 | 29/188 (15.4) | 1.26 (0.61–2.60) | 0.53 | |||
| 4 | 57/371 (15.4) | 1.26 (0.64–2.45) | 0.50 | |||
| N-classification | 0 | 21/134 (15.7) | 1 | |||
| 1 | 77/520 (14.8) | 0.94 (0.55–1.58) | 0.80 | |||
| T-size | <8 cm | 86/609 (14.1) | 1 | 1 | ||
| ≥8 cm | 12/45 (26.7) | 2.21 (1.10–4.45) | 0.026 | 2.23 (1.09–4.54) | 0.027 | |
| Variable | Category | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | ||
| Sex | male | 1 | 1 | ||
| female | 0.84 (0.71–0.99) | 0.033 | 0.86 (0.72–1.01) | 0.86 | |
| Age, year | ≤65 | 1 | 1 | ||
| >65 | 1.30 (1.10–1.52) | 0.002 | 1.02 (0.86–1.22) | 0.80 | |
| ECOG performance | 0 or 1 | 1 | 1 | ||
| 2 | 2.50 (2.08–3.01) | <0.001 | 2.46 (2.02–2.99) | <0.001 | |
| 3 | 5.60 (3.75–8.36) | <0.001 | 5.79 (3.83–8.77) | <0.001 | |
| Body weight loss | ≤5% | 1 | |||
| >5% | 1.04 (0.87–1.23) | 0.67 | |||
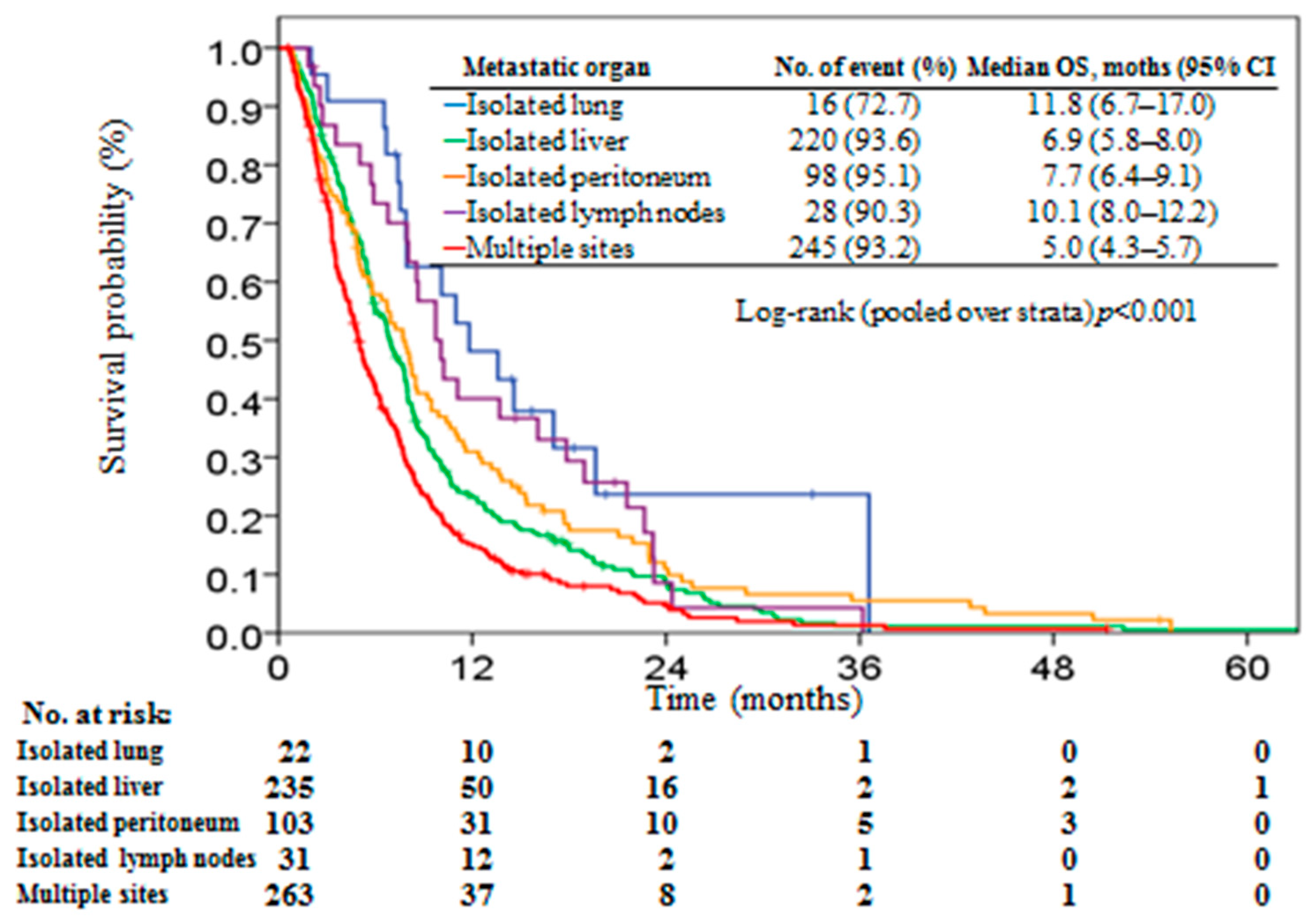
| Metastatic organ | isolated lung | 1 | 1 | ||
| isolated liver | 1.96 (1.18–3.25) | 0.010 | 1.92 (1.15–3.21) | 0.013 | |
| isolated peritoneum | 1.68 (0.99–2.85) | 0.055 | 1.54 (0.90–2.62) | 0.11 | |
| isolated lymph nodes | 1.38 (0.75–2.55) | 0.31 | 1.47 (0.79–2.74) | 0.22 | |
| multiple sites | 2.66 (1.60–4.42) | <0.001 | 2.60 (1.56–4.35) | <0.001 | |
| CCI | 0 to 1 | 1 | 1 | ||
| >1 | 1.34 (1.40–1.58) | <0.001 | 1.21 (1.02–1.44) | 0.027 | |
| Active or ever smoker | no | 1 | 1 | ||
| yes | 1.16 (0.98–1.36) | 0.080 | 1.22 (1.03–1.44) | 0.021 | |
| CEA, ng/dL | ≤5 | 1 | 1 | ||
| >5 | 1.17 (0.99–1.38) | 0.053 | 1.15 (0.98–1.36) | 0.090 | |
| CA19-9, ng/dL | ≤37 | 1 | |||
| >37 | 1.03 (0.84–1.25) | 0.81 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, K.-H.; Hung, C.-Y.; Hsueh, S.-W.; Chang, P.-H.; Chen, Y.-Y.; Lu, C.-H.; Chen, P.-T.; Yeh, K.-Y.; Huang, P.-W.; Tsang, N.-M.; et al. Lung Metastases in Patients with Stage IV Pancreatic Cancer: Prevalence, Risk Factors, and Survival Impact. J. Clin. Med. 2019, 8, 1402. https://doi.org/10.3390/jcm8091402
Liu K-H, Hung C-Y, Hsueh S-W, Chang P-H, Chen Y-Y, Lu C-H, Chen P-T, Yeh K-Y, Huang P-W, Tsang N-M, et al. Lung Metastases in Patients with Stage IV Pancreatic Cancer: Prevalence, Risk Factors, and Survival Impact. Journal of Clinical Medicine. 2019; 8(9):1402. https://doi.org/10.3390/jcm8091402
Chicago/Turabian StyleLiu, Keng-Hao, Chia-Yen Hung, Shu-Wen Hsueh, Pei-Hung Chang, Yen-Yang Chen, Chang-Hsien Lu, Ping-Tsung Chen, Kun-Yun Yeh, Pei-Wei Huang, Ngan-Ming Tsang, and et al. 2019. "Lung Metastases in Patients with Stage IV Pancreatic Cancer: Prevalence, Risk Factors, and Survival Impact" Journal of Clinical Medicine 8, no. 9: 1402. https://doi.org/10.3390/jcm8091402
APA StyleLiu, K. -H., Hung, C. -Y., Hsueh, S. -W., Chang, P. -H., Chen, Y. -Y., Lu, C. -H., Chen, P. -T., Yeh, K. -Y., Huang, P. -W., Tsang, N. -M., Hung, Y. -S., & Chou, W. -C. (2019). Lung Metastases in Patients with Stage IV Pancreatic Cancer: Prevalence, Risk Factors, and Survival Impact. Journal of Clinical Medicine, 8(9), 1402. https://doi.org/10.3390/jcm8091402