Positron Emission Tomography Can Support the Diagnosis of Dialysis-Related Amyloidosis

 , , ,
, , , 
Abstract
:1. Background
2. Materials and Methods
2.1. Settings and Patients
- -
- each dialysis year = 1 point; each year of kidney transplantation = 0.2 point; each year of CKD stages 4-5 = 0.2 point; carpal tunnel or evidence of DRA = 5 points per site up to a maximum of 4 sites
- -
- each dialysis year = 1 point; each year of kidney transplantation = 0.2 point; carpal tunnel = 5 points per site
- -
- each dialysis year = 1 point; carpal tunnel or evidence of DRA = 5 points per site up to a maximum of 4 sites
2.2. Selection Criteria: Patients
2.3. Selection Criteria: Controls
2.4. PET Scan
2.5. Statistical Analysis
2.6. Ethical Issues
3. Results
3.1. Baseline Data
3.2. Indications for PET Scans
3.3. Correlation between PET Scans and Clinical Features
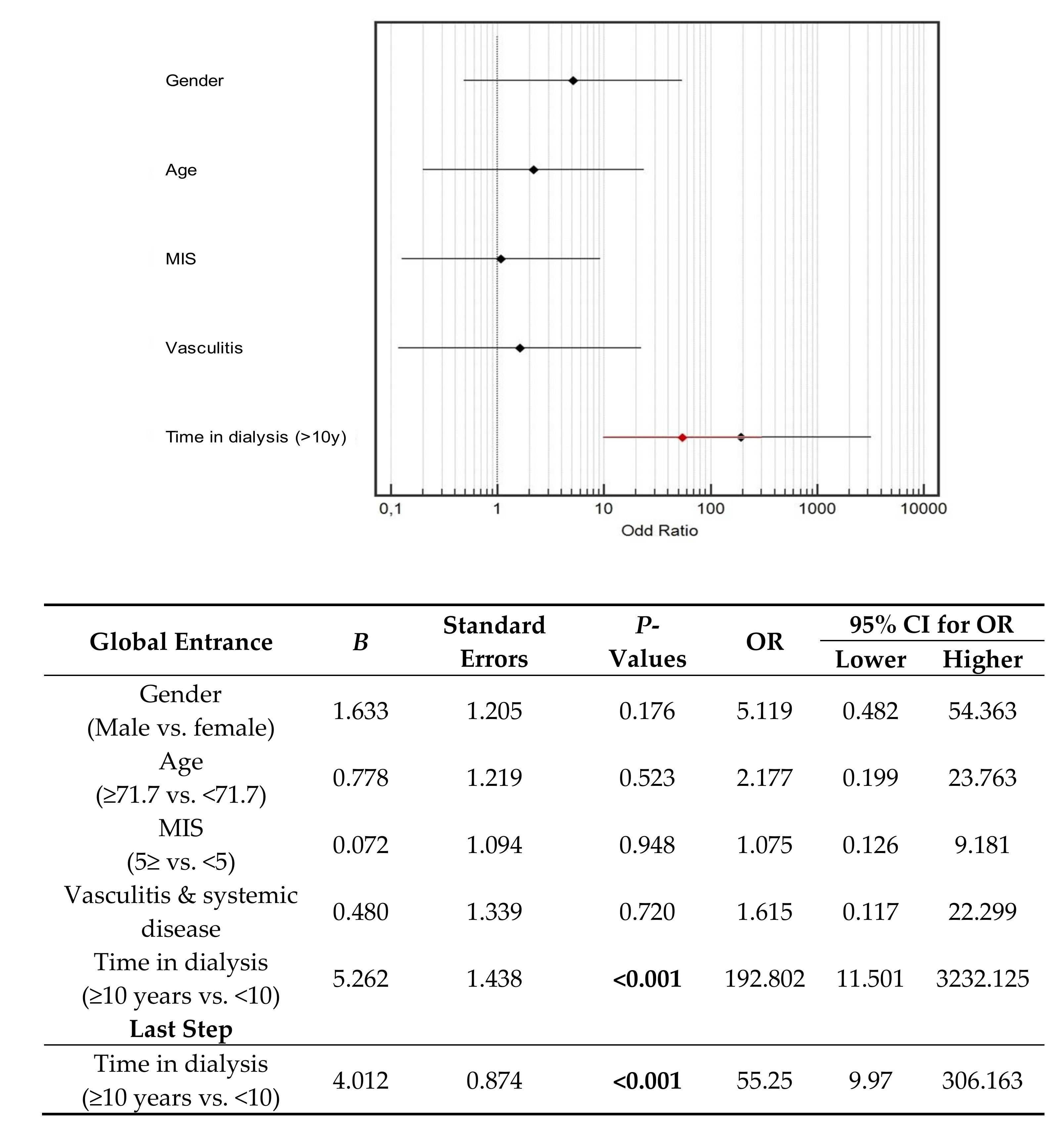
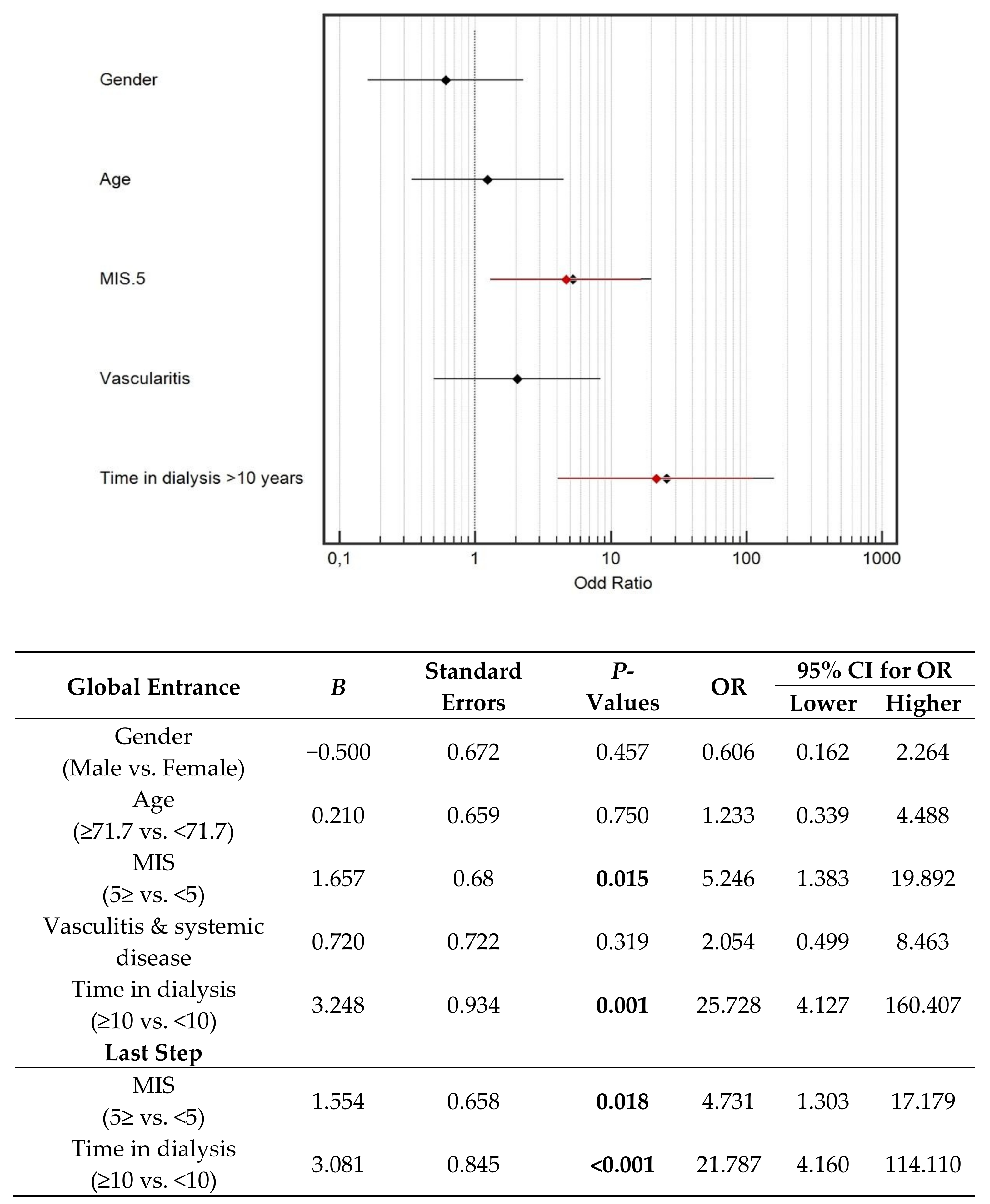
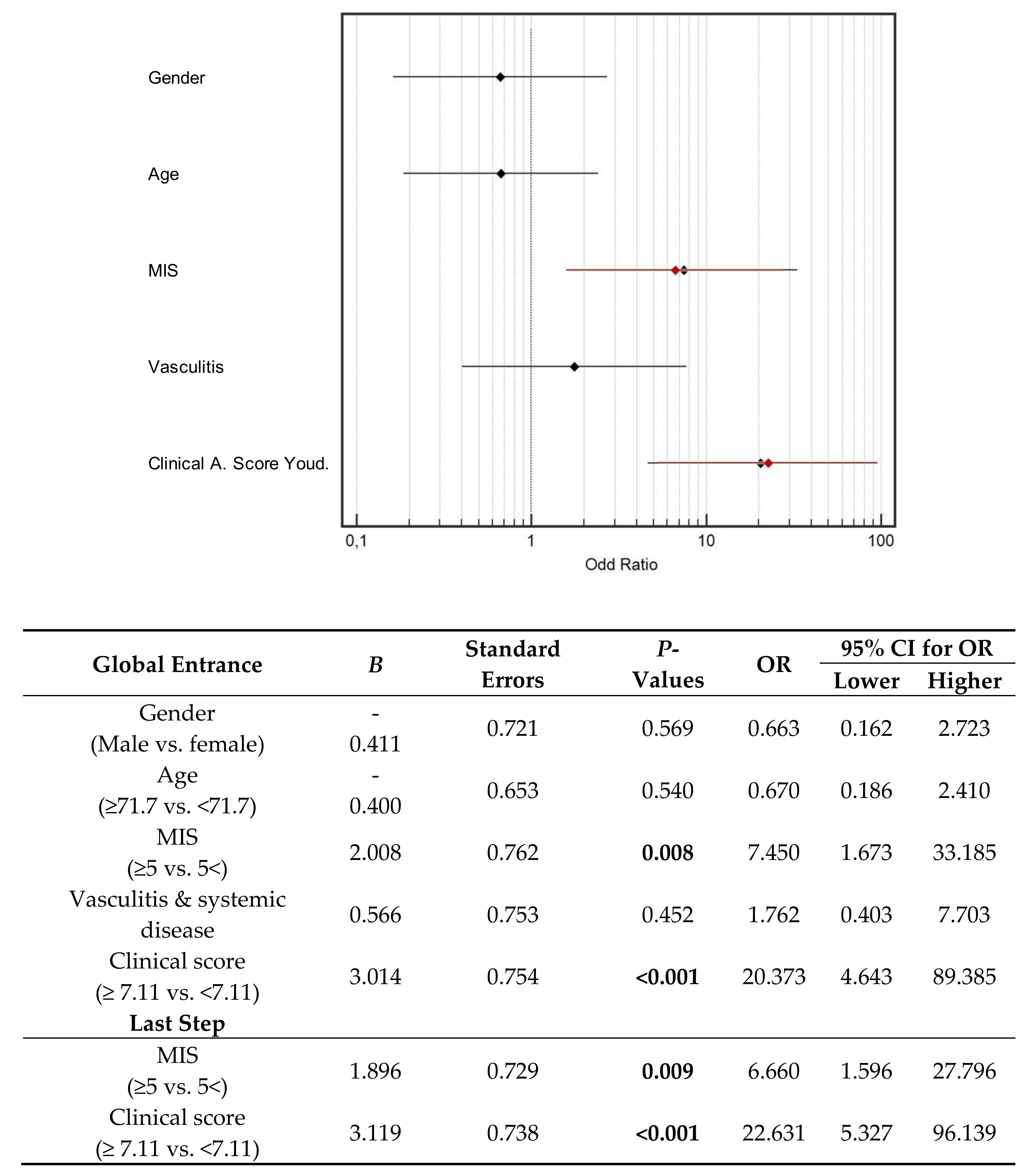
3.4. Multivariate Analysis
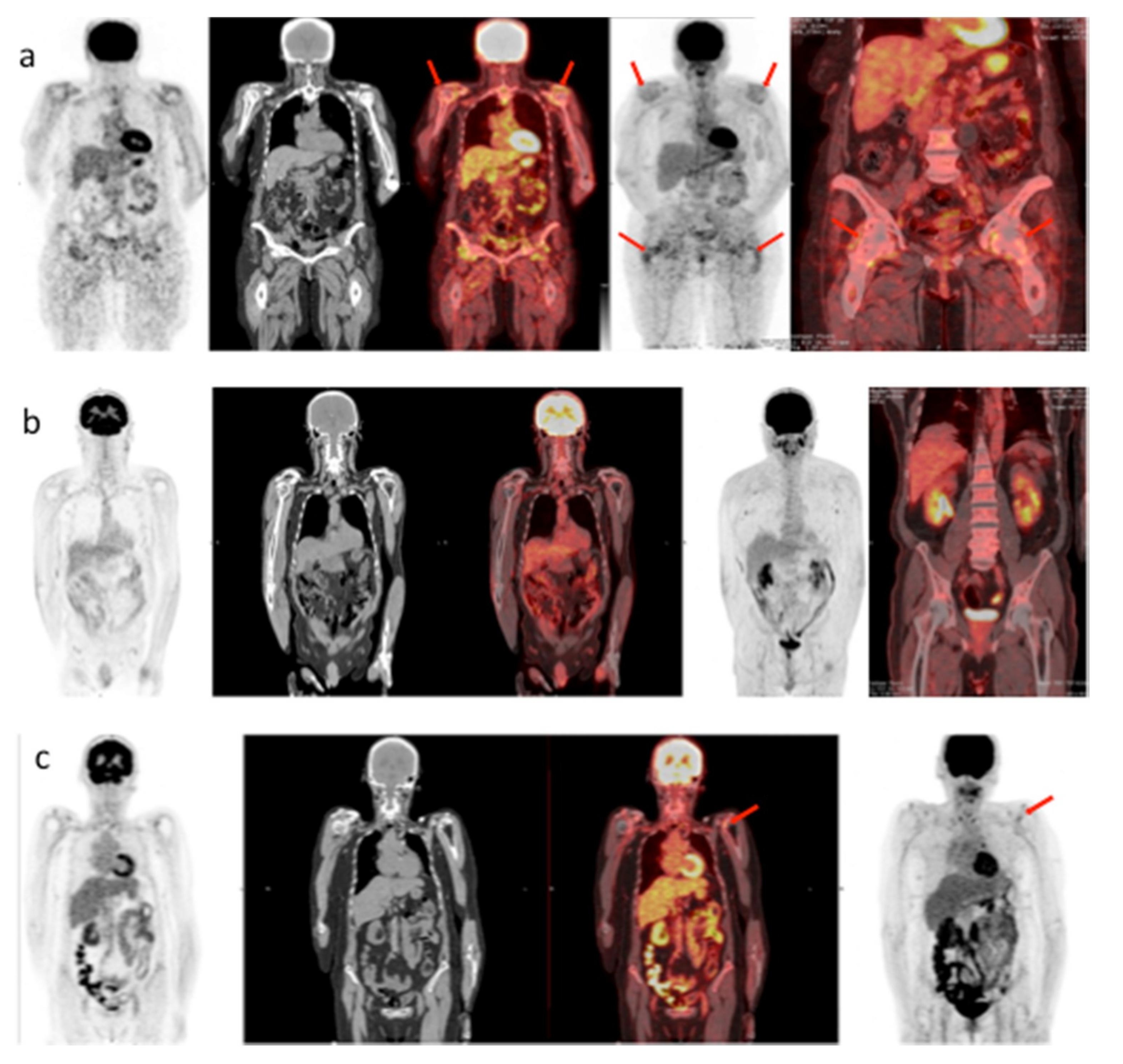
3.4.1. Outcomes: Carpal Tunnel and Positive PET Scan
3.4.2. ROC Curves and Sensitivity Analysis.
3.5. Prediction Model of “Dialysis-Related” PET Positivity.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Owen, W.F.; Madore, F.; Brenner, B.M. An observational study of cardiovascular characteristics of long-term end-stage renal disease survivors. Am. J. Kidney Dis. 1996, 28, 931–936. [Google Scholar] [CrossRef]
- Bazzi, C.; Arrigo, G.; Luciani, L.; Casazza, F.; Saviotti, M.; Malaspina, D.; Bonucci, E.; Ballanti, P.; Amaducci, S.; Lattuada, P.; et al. Clinical features of 24 patients on regular hemodialysis treatment (RDT) for 16–23 years in a single unit. Clin. Nephrol. 1995, 44, 96–107. [Google Scholar] [PubMed]
- Harris, S.A.C.; Brown, A. Patients surviving more than 10 years on hemodialysis. The natural history of the complications of treatment. Nephrol. Dial. Tranplant. 1998, 13, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Otsubo, S.; Otsubo, K.; Sugimoto, H.; Ueda, S.; Otsubo, Y.; Otsubo, O.; Yajima, A.; Yagi, S.; Kataoka, H.; Iwasaki, T.; et al. Characteristics of patients on hemodialysis therapy for more than 30 years. Ther. Apher. Dial. 2007, 11, 274–279. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Mezza, E.; Anania, P.; Iadarola, A.M.; Vischi, M.; Torazza, M.C.; Fop, F.; Guarena, C.; Martina, G.; Messina, M.; et al. Patients on renal replacement therapy for 20 or more years: A clinical profile. Nephrol. Dial. Transplant. 2002, 17, 1440–1449. [Google Scholar] [CrossRef] [PubMed]
- Davison, A.M. Editorial: Complications arising in patients on long-term hemodialysis. Kidney Int. 1993, 43 (Suppl. 41), S40–S41. [Google Scholar]
- Levey, A.S.; Eknoyan, G. Cardiovascular disease in chronic renal disease. Nephrol. Dial. Transplant. 1999, 4, 828–833. [Google Scholar] [CrossRef]
- Warren, D.J.; Otieno, L.S. Carpal tunnel syndrome in patients on intermittent haemodialysis. Postgrad. Med. J. 1975, 51, 450–452. [Google Scholar] [CrossRef] [Green Version]
- Koch, K.M. Dialysis-related amyloidosis. Kidney Int. 1992, 41, 1416–1429. [Google Scholar] [CrossRef] [Green Version]
- Danesh, F.; Ho, L.T. Dialysis-related amyloidosis: History and clinical manifestations. Semin. Dial. 2001, 14, 80–85. [Google Scholar] [CrossRef]
- Bardin, T.; Zingraff, J.; Kuntz, D.; Drüeke, T. Dialysis-related amyloidosis. Nephrol. Dial. Transplant. 1986, 1, 151–154. [Google Scholar] [PubMed]
- Dember, L.M.; Jaber, B.L. Dialysis-related amyloidosis: Late finding or hidden epidemic? Semin. Dial. 2006, 19, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Scarpioni, R.; Ricardi, M.; Albertazzi, V.; De Amicis, S.; Rastelli, F.; Zerbini, L. Dialysis-related amyloidosis: Challenges and solutions. Int. J. Nephrol. Renovasc. Dis. 2016, 9, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Otsubo, S.; Kimata, N.; Okutsu, I.; Oshikawa, K.; Ueda, S.; Sugimoto, H.; Mitobe, M.; Uchida, K.; Otsubo, K.; Nitta, K.; et al. Characteristics of dialysis-related amyloidosis in patients on haemodialysis therapy for more than 30 years. Nephrol. Dial. Transplant. 2009, 24, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Fenves, A.Z.; Emmett, M.; White, M.G.; Greenway, G.; Michaels, D.B. Carpal tunnel syndrome with cystic bone lesions secondary to amyloidosis in chronic hemodialysis patients. Am. J. Kidney Dis. 1986, 7, 130–134. [Google Scholar] [CrossRef]
- Nakazawa, R.; Hamaguchi, K.; Hosaka, E.; Shishido, H.; Yokoyama, T. Synovial amyloidosis of beta 2-microglobulin type in patients undergoing long-term hemodialysis. Nephron 1986, 44, 379–380. [Google Scholar] [CrossRef] [PubMed]
- Gejyo, F.; Homma, N.; Suzuki, Y.; Arakawa, M. Serum levels of beta 2-microglobulin as a new form of amyloid protein in patients undergoing long-term hemodialysis. N. Engl. J. Med. 1986, 314, 585–586. [Google Scholar]
- Zingraff, J.J.; Noel, L.H.; Bardin, T.; Atienza, C.; Zins, B.; Drueke, T.B.; Kuntz, D. Beta 2 microglobulin amyloidosis in chronic renal failure. N. Engl. J. Med. 1990, 323, 1070–1071. [Google Scholar]
- Drüeke, T.B. Beta2-microglobulin and amyloidosis. Nephrol. Dial. Transplant. 2000, 15 (Suppl. 1), 17–24. [Google Scholar] [CrossRef]
- Drüeke, T.B.; Massy, Z.A. Beta2-microglobulin. Semin. Dial. 2009, 22, 378–380. [Google Scholar] [CrossRef]
- Jadoul, M.; Drüeke, T.B. β2 microglobulin amyloidosis: An update 30 years later. Nephrol. Dial. Transplant. 2016, 31, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Gorevic, P.D.; Casey, T.T.; Stone, W.J.; DiRaimondo, C.R.; Prelli, F.C.; Frangione, B. Beta-2 microglobulin is an amyloidogenic protein in man. J. Clin. Investig. 1985, 76, 2425–2429. [Google Scholar] [CrossRef] [PubMed]
- Shirahama, T.; Skinner, M.; Cohen, A.S.; Gejyo, F.; Arakawa, M.; Suzuki, M.; Hirasawa, Y. Histochemical and immunohistochemical characterization of amyloid associated with chronic hemodialysis as beta 2-microglobulin. Lab. Investig. 1985, 53, 705–709. [Google Scholar] [PubMed]
- Jimenez, R.E.; Price, D.A.; Pinkus, G.S.; Owen, W.F., Jr.; Lazarus, J.M.; Kay, J.; Turner, J.R. Development of gastrointestinal beta2-microglobulin amyloidosis correlates with time on dialysis. Am. J. Surg. Pathol. 1998, 22, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Gal, R.; Korzets, A.; Schwartz, A.; Rath-Wolfson, L.; Gafter, U. Systemic distribution of beta 2-microglobulin-derived amyloidosis in patients who undergo long-term hemodialysis. Report of seven cases and review of the literature. Arch. Pathol. Lab. Med. 1994, 118, 718–721. [Google Scholar] [PubMed]
- Kuntz, D.; Naveau, B.; Bardin, T.; Drueke, T.; Treves, R.; Dryll, A. Destructive spondylarthropathy in hemodialyzed patients. A new syndrome. Arthritis Rheum. 1984, 27, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Floege, J.; Schäffer, J.; Koch, K.M.; Shaldon, S. Dialysis related amyloidosis: A disease of chronic retention and inflammation? Kidney Int. Suppl. 1992, 38, S78–S85. [Google Scholar] [PubMed]
- Canaud, B.; Morena, M.; Cristol, J.P.; Krieter, D. Beta2-microglobulin, a uremic toxin with a double meaning. Kidney Int. 2006, 69, 1297–1299. [Google Scholar] [CrossRef]
- Bommer, J.; Jaber, B.L. Ultrapure dialysate: Facts and myths. Semin. Dial. 2006, 19, 115. [Google Scholar] [CrossRef]
- Di Iorio, B.; Di Micco, L.; Bruzzese, D.; Nardone, L.; Russo, L.; Formisano, P.; D’Esposito, V.; Russo, D. Ultrapure dialysis water obtained with additional ultrafilter may reduce inflammation in patients on hemodialysis. J. Nephrol. 2017, 30, 795–801. [Google Scholar] [CrossRef]
- Labriola, L.; Jadoul, M. Dialysis-related Amyloidosis: Is It Gone or Should It Be? Semin. Dial. 2017, 30, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Argiles, A.; Mourad, G.; Berta, P.; Polito, C.; Canaud, B.; Robinet-Levy, M.; Mion, C. Dialysis-associated amyloidosis in a patient on long-term post-dilutional hemofiltration. Nephron 1987, 46, 96–97. [Google Scholar] [CrossRef] [PubMed]
- Kay, J. Beta 2-microglobulin amyloidosis in renal failure: Understanding this recently recognized condition. Cleve Clin. J. Med. 1999, 66, 145–147. [Google Scholar] [PubMed]
- Canaud, B.; Assounga, A.; Flavier, J.L.; Slingeneyer, A.; Aznar, R.; Robinet-Levy, M.; Mion, C. Beta-2 microglobulin serum levels in maintenance dialysis. What does it mean? ASAIO Trans. 1988, 34, 923–929. [Google Scholar] [PubMed]
- Hauglustaine, D.; Waer, M.; Michielsen, P.; Goebels, J.; Vandeputte, M. Haemodialysis membranes, serum beta 2-microglobulin, and dialysis amyloidosis. Lancet 1986, 24, 1211–1212. [Google Scholar] [CrossRef]
- Kaneko, S.; Yamagata, K. Hemodialysis-related amyloidosis: Is it still relevant? Semin. Dial. 2018, 31, 612–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldreich, T.; Nowak, C.; Fall, T.; Carlsson, A.C.; Carrero, J.J.; Ripsweden, J.; Qureshi, A.R.; Heimbürger, O.; Barany, P.; Stenvinkel, P.; et al. Circulating proteins as predictors of cardiovascular mortality in end-stage renal disease. J. Nephrol. 2019, 32, 111–119. [Google Scholar] [CrossRef] [PubMed]
- De Mauri, A.; Vidali, M.; Chiarinotti, D.; Bellomo, G.; Rolla, R. Lipoprotein-associated phospholipase A2 predicts cardiovascular events in dialyzed patients. J. Nephrol. 2019, 32, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Massy, Z.A.; Liabeuf, S. Middle-Molecule Uremic Toxins and Outcomes in Chronic Kidney Disease. Contrib. Nephrol. 2017, 191, 8–17. [Google Scholar] [PubMed]
- Vanholder, R.; Van Laecke, S.; Glorieux, G. The middle-molecule hypothesis 30 years after: Lost and rediscovered in the universe of uremic toxicity? J. Nephrol. 2008, 21, 146–160. [Google Scholar] [PubMed]
- Vanholder, R.; Eloot, S.; Van Biesen, W. Do we need new indicators of dialysis adequacy based on middle-molecule removal? Nat. Clin. Pract. Nephrol. 2008, 4, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Brunati, C.C.M.; Gervasi, F.; Cabibbe, M.; Ravera, F.; Menegotto, A.; Querques, M.; Colussi, G. Single Session and Weekly Beta 2-Microglobulin Removal with Different Dialytic Procedures: Comparison between High-Flux Standard Bicarbonate Hemodialysis, Post-Dilution Hemodiafiltration, Short Frequent Hemodialysis with NxStage Technology and Automated Peritoneal Dialysis. Blood Purif. 2019, 48, 86–96. [Google Scholar] [PubMed]
- Roumelioti, M.E.; Trietley, G.; Nolin, T.D.; Ng, Y.H.; Xu, Z.; Alaini, A.; Figueroa, R.; Unruh, M.L.; Argyropoulos, C.P. Beta-2 microglobulin clearance in high-flux dialysis and convective dialysis modalities: A meta-analysis of published studies. Nephrol. Dial. Transplant. 2018, 33, 1025–1039. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, J.; Yamagata, K.; Nishi, S.; Nakai, S.; Masakane, I.; Iseki, K.; Tsubakihara, Y. Significance of the decreased risk of dialysis-related amyloidosis now proven by results from Japanese nationwide surveys in 1998 and 2010. Nephrol. Dial. Transplant. 2016, 31, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Bataille, S.; Fernandez, C.; Zink, J.V.; Brunet, P.; Berland, Y.; Burtey, S. The Case|A hip fracture in a hemodialysis patient. Pathologic right-hip fracture from β2-microglobulin amyloidosis. Kidney Int. 2013, 83, 1211–1212. [Google Scholar] [CrossRef]
- Kazama, J.J.; Yamamoto, S.; Wakasugi, M.; Narita, I. A hip fracture in a dialysis patient with Aβ2M amyloidosis. Kidney Int. 2014, 85, 214–215. [Google Scholar] [CrossRef]
- Hoshino, J.; Yamagata, K.; Nishi, S.; Nakai, S.; Masakane, I.; Iseki, K.; Tsubakihara, Y. Carpal tunnel surgery as proxy for dialysis-related amyloidosis: Results from the Japanese society for dialysis therapy. Am. J. Nephrol. 2014, 39, 449–458. [Google Scholar] [CrossRef]
- Hoshino, J.; Kawada, M.; Imafuku, A.; Mise, K.; Sumida, K.; Hiramatsu, R.; Hasegawa, E.; Hayami, N.; Yamanouchi, M.; Suwabe, T.; et al. A clinical staging score to measure the severity of dialysis-related amyloidosis. Clin. Exp. Nephrol. 2016, 21, 300–306. [Google Scholar] [CrossRef]
- Ketteler, M.; Koch, K.M.; Floege, J. Imaging techniques in the diagnosis of dialysis-related amyloidosis. Semin. Dial. 2001, 14, 90–93. [Google Scholar] [CrossRef]
- Schaeffer, J.; Floege, J.; Koch, K.M. Diagnostic aspects of beta 2-microglobulin amyloidosis. Nephrol. Dial. Transplant. 1996, 11 (Suppl. 2), 144–146. [Google Scholar] [CrossRef]
- Floege, J.; Schäffer, J.; Koch, K.M. Scintigraphic methods to detect beta 2-microglobulin associated amyloidosis (Abeta2-microglobulin amyloidosis). Nephrol. Dial. Transplant. 2001, 16 (Suppl. 4), 12–16. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Baillod, R.; Brown, E.; Farrington, K.; Soper, C.; Percy, M.; Clutterbuck, E.; Madhoo, S.; Pepys, M.B.; Hawkins, P.N. Clinical, radiological and serum amyloid P component scintigraphic features of beta 2-microglobulin amyloidosis associated with continuous ambulatory peritoneal dialysis. Nephrol Dial. Transplant. 1999, 14, 1467. [Google Scholar] [CrossRef]
- Yen, T.C.; Tzen, K.Y.; Chen, K.S.; Tsai, C.J. The value of gallium-67 and thallium-201 whole-body and single-photon emission tomography images in dialysis-related beta 2-microglobulin amyloid. Eur. J. Nucl. Med. 2000, 27, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Schäffer, J.; Burchert, W.; Floege, J.; Gielow, P.; Kionka, C.; Linke, R.P.; Weiss, E.H.; Shaldon, S.; Koch, K.M. Recombinant versus natural human 111In-beta 2-microglobulin for scintigraphic detection of A beta 2-amyloid in dialysis patients. Kidney Int. 2000, 58, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Kiss, E.; Keusch, G.; Zanetti, M.; Jung, T.; Schwarz, A.; Schocke, M.; Jaschke, W.; Czermak, B.V. Dialysis-related amyloidosis revisited. Am. J. Roentgenol. 2005, 185, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Kecler-Pietrzyk, A.; Kok, H.K.; Lyburn, I.D.; Torreggiani, W.C. Dialysis related amyloidarthropathy on FDG PET-CT. Ulster Med. J. 2014, 83, 117–118. [Google Scholar] [PubMed]
- Piccoli, G.B.; Hachemi, M.; Molfino, I.; Coindre, J.P.; Boursot, C. Doxycycline treatment in dialysis related amyloidosis: Discrepancy between antalgic effect and inflammation, studied with FDG-positron emission tomography: A case report. BMC Nephrol. 2017, 18, 28. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cabiddu, G.; Moio, M.R.; Fois, A.; Cao, R.; Molfino, I.; Kaniassi, A.; Lippi, F.; Froger, L.; Pani, A.; et al. Efficiency and nutritional parameters in an elderly high risk population on hemodialysis and hemodiafiltration in Italy and France: Different treatments with similar names? BMC Nephrol. 2018, 19, 171. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Nielsen, L.; Gendrot, L.; Fois, A.; Cataldo, E.; Cabiddu, G. Prescribing Hemodialysis or Hemodiafiltration: When One Size Does Not Fit All the Proposal of a Personalized Approach Based on Comorbidity and Nutritional Status. J. Clin. Med. 2018, 7, 331. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Enia, G.; Sicuso, C.; Alati, G.; Zoccali, C. Subjective global assessment of nutrition in dialysis patients. Nephrol. Dial. Transplant. 1993, 8, 1094–1098. [Google Scholar] [PubMed]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef] [PubMed]
- Spatola, L.; Finazzi, S.; Calvetta, A.; Reggiani, F.; Morenghi, E.; Santostasi, S.; Angelini, C.; Badalamenti, S.; Mugnai, G. Subjective Global Assessment-Dialysis Malnutrition Score and cardiovascular risk in hemodialysispatients: An observational cohort study. J. Nephrol. 2018, 31, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Molinaro, A.M.; Simon, R.; Pfeiffer, R.M. Prediction error estimation: A comparison of resampling methods. Bioinforma. Oxf. Engl. 2005, 21, 3301–3307. [Google Scholar] [CrossRef] [PubMed]
- Nishi, S.; Hoshino, J.; Yamamoto, S.; Goto, S.; Fujii, H.; Ubara, Y.; Motomiya, Y.; Morita, H.; Takaichi, K.; Yamagata, K.; et al. Multicentre cross-sectional study for bone-articular lesions associated with dialysis related amyloidosis in Japan. Nephrology 2018, 23, 640–645. [Google Scholar] [CrossRef]
- Tagami, A.; Tomita, M.; Adachi, S.; Tsuda, K.; Yamada, S.; Chiba, K.; Okazaki, N.; Yonekura, A.; Tsujimoto, R.; Kajiyama, S.; et al. Epidemiological survey and risk factor analysis of dialysis-related amyloidosis including destructive spondyloarthropathy, dialysis amyloid arthropathy, and carpal tunnel syndrome. J. Bone Miner. Metab. 2019, 14. [Google Scholar] [CrossRef]
- Yamamoto, S.; Kazama, J.J.; Maruyama, H.; Nishi, S.; Narita, I.; Gejyo, F. Patients undergoing dialysis therapy for 30 years or more survive with serious osteoarticular disorders. Clin. Nephrol. 2008, 70, 496–502. [Google Scholar] [CrossRef]
- Sigaux, J.; Abdelkefi, I.; Bardin, T.; Laredo, J.D.; Ea, H.K.; UreñaTorres, P.; Cohen-Solal, M. Tendon thickening in dialysis-related joint arthritis is due to amyloid deposits at the surface of the tendon. Jt. Bone Spine 2019, 86, 233–238. [Google Scholar] [CrossRef]
- Kuragano, T.; Kida, A.; Yahiro, M.; Nakanishi, T. Clinical Benefit of an Adsorptive Technique for Elderly Long-Term Hemodialysis Patients. Contrib. Nephrol. 2019, 198, 94–102. [Google Scholar]
- Giorgetti, S.; Raimondi, S.; Pagano, K.; Relini, A.; Bucciantini, M.; Corazza, A.; Fogolari, F.; Codutti, L.; Salmona, M.; Mangione, P.; et al. Effect of tetracyclines on the dynamics of formation and destructuration of beta 2-microglobulin amyloid fibrils. J. Biol. Chem. 2011, 286, 2121–2131. [Google Scholar] [CrossRef]
- Hiyama, E.; Hyodo, T.; Kondo, M.; Otsuka, K.; Honma, T.; Taira, T.; Yoshida, K.; Uchida, T.; Endo, T.; Sakai, T.; et al. Performance of the newer type (Lixelle Type S-15) on direct hemoperfusion beta 2-microglobulin adsorption column for dialysis-related amyloidosis. Nephron 2002, 92, 501–502. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Uchita, K.; Orita, H.; Kamimura, M.; Oda, M.; Hasegawa, H.; Kobata, H.; Fukunishi, M.; Shimazaki, M.; Abe, T.; et al. Effect of beta(2)-microglobulin adsorption column on dialysis-related amyloidosis. Kidney Int. 2003, 64, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Kuragano, T.; Inoue, T.; Yoh, K.; Shin, J.; Fujita, Y.; Yoshiya, K.; Kim, J.I.; Sakai, R.; Sekita, K.; Goto, T.; et al. Effectiveness of β(2)-microglobulin adsorption column in treating dialysis-related amyloidosis: A multicenter study. Blood Purif. 2011, 32, 317–322. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dialysis Patients (n = 46) | Controls (n = 218) | P | |
|---|---|---|---|
| Age (years), median (min–max) | 71.7 (33.6–89.2) | 67.6 (34.8–89.3) | 0.0179 |
| Sex (% females) | 54.3% | 48.6% | 0.4813 |
| Serum creatinine (µmol/L), median (min-max) | Dialysis | 68 (39–106) | - |
| Positive “shoulder and hip pattern” at PET-FDG, n (%) ** | 20 (43.5%) | 11 (5.0%) | <0.0001 |
| All Patients (n = 46) | All PET Scans (n = 72) | ||
|---|---|---|---|
| Age (years), median (min–max) | 71.7 (33.6–89.2) | 71.1 (33.6–89.2) | |
| Sex, (% female) | 54.3% | 54.2% | |
| Cancer, n (%) | 21 (45.7%) | 39 (54.2%) | |
| Vasculitis, n (%) | 12 (26.1%) | 18 (25.0%) | |
| Dialysis vintage (years), median (min–max) | 3.7 (0.1–42.1) | 3.4 (0.1–42.1) | |
| Kidney transplant, n (%) | 6 (13.0%) | 11 (15.3%) | |
| Kt/V, mean (±SD) | 1.48 (±0.36) | 1.49 (±0.33) | |
| Albumin (g/L), mean (±SD) | 32.7 (±4.3) | 32.9 (±4.32) | |
| Beta-2 microglobulin, mean (±SD) | 27.5 (±9.1) | 27.0 (±8.3) | |
| Charlson Comorbidity Index, median (min-max) | 9 (3–12) | 9 (3–12) | |
| MIS, median (min–max) | 8 (3–19) | 7 (3–19) | |
| SGA | A, (%) | 63.0% | 66.7% |
| B, (%) | 30.4% | 26.4% | |
| C, (%) | 6.6% | 6.9% | |
| PET-FDG positive, n (%) | 20 (43.5%) | 31 (41.3%) | |
| Carpal Tunnel positive, n (%) | 7 (15.2%) | 15 (20.8%) | |
| Patients Considered | PET Scans Considered | ||||||
|---|---|---|---|---|---|---|---|
| C.T. Positive (n = 7) | C.T. Negative (n = 39) | P | C.T. Positive (n = 15) | C.T. Negative (n = 57) | P | ||
| Age (years), median (min-max) | 67.8 (57.6–82.6) | 72.0 (33.6–89.2) | 0.3510 | 67.6 (57.6–82.6) | 71.5 (33.6–89.2) | 0.0661 | |
| Sex, (% female) | 57.1% | 53.8% | 0.8733 | 60.0% | 52.6% | 0.6128 | |
| Cancer, n (%) | 3 (42.9%) | 18 (46.2%) | 0.8733 | 7 (46.7%) | 32 (56.1%) | 0.5153 | |
| Vasculitis, n (%) | 1 (14.3%) | 11 (28.2%) | 0.4450 | 2 (13.3%) | 16 (28.1%) | 0.2442 | |
| Dialysis vintage (years), median (min–max) | 13.2 (6.1–42.1) | 1.6 (0.1–21.2) | 0.0006 | 14.3 (6.1–42.1) | 2.3 (0.1–21.2) | <0.0001 | |
| Kidney transplant, n (%) | 3 (42.9%) | 3 (7.7%) | 0.0119 | 8 (53.3%) | 3 (5.3%) | <0.0001 | |
| Kt/V, mean (±SD) | 1.59 (±0.33) | 1.46 (±0.37) | 0.4110 | 1.60 (±0.27) | 1.46 (±0.34) | 0.1520 | |
| Albumin (g/L), mean (±SD) | 28.3 (±4.1) | 33.4 (±4.0) | 0.0070 | 31.5 (±5.2) | 33.2 (±4.1) | 0.1860 | |
| Beta-2 microglobulin, mean (±SD) | 26.6 (±10.5) | 27.6 (±9.0) | 0.7990 | 26.3 (±8.1) | 27.2 (±8.1) | 0.7260 | |
| Charlson, median (min–max) | 9 (3–12) | 9 (4–11) | 0.7805 | 9 (3–12) | 9 (4–11) | 0.2304 | |
| MIS, median (min-max) | 9 (5–19) | 7 (3–14) | 0.1319 | 9 (4–19) | 6 (3–14) | 0.1061 | |
| SGA | A, (%) | 57.1% | 64.1% | 0.0316 | 66.7% | 66.7% | 0.0012 |
| B, (%) | 14.3% | 33.3% | 6.7% | 31.6% | |||
| C, (%) | 28.6% | 2.6% | 26.7% | 1.8% | |||
| PET SCAN positive, n (%) | 7 (100%) | 13 (33.3%) | 0.0012 | 14 (93.3%) | 17 (29.8%) | <0.0001 | |
| Patients Considered | PET Scans Considered | ||||||
|---|---|---|---|---|---|---|---|
| Positive (n = 20) | Negative (n = 26) | P | Positive (n = 31) | Negative (n = 41) | P | ||
| Age (years), median (min-max) | 70.1 (37.8–86.7) | 71.9 (33.6–89.2) | 0.6103 | 67.7 (37.8–86.7) | 71.9 (33.6–89.2) | 0.0695 | |
| Sex, (% female) | 70.0% | 42.3% | 0.0645 | 67.7% | 43.9% | 0.0459 | |
| Cancer, n (%) | 10 (50.0%) | 11 (42.3%) | 0.6076 | 18 (58.1%) | 21 (51.2%) | 0.5665 | |
| Vasculitis, n (%) | 6 (30.0%) | 6 (23.1%) | 0.6001 | 8 (25.8%) | 10 (24.4%) | 0.8915 | |
| Dialysis vintage (years), median (min–max) | 7.2 (0.1–42.1) | 1.2 (0.1–13.0) | 0.0153 | 11.0 (0.1–42.1) | 1.6 (0.1–13.0) | <0.0001 | |
| Kidney transplant, n (%) | 4 (20.0%) | 2 (7.7%) | 0.3831 | 9 (29.0%) | 2 (4.9%) | 0.0071 | |
| Kt/V, mean (±SD) | 1.57 (±0.40) | 1.41 (±0.32) | 0.1480 | 1.59 (±0.35) | 1.41 (±0.29) | 0.0270 | |
| Albumin (g/L), mean (±SD) | 31.6 (±4.5) | 33.5 (±4.1) | 0.1450 | 32.6 (±4.6) | 33.1 (±4.2) | 0.6520 | |
| Beta 2 microglobulin, mean (±SD) | 27.9 (±9.7) | 27.2 (±8.8) | 0.8010 | 27.6 (±9.3) | 26.6 (±7.6) | 0.6210 | |
| Charlson Comorbidity Index, median (min–max) | 9 (3–12) | 9 (4–11) | 0.3634 | 9 (3–12) | 9 (4–11) | 0.0692 | |
| MIS, median (min–max) | 10 (5–19) | 6 (3–14) | 0.0034 | 9 (5–19) | 5 (3–14) | <0.0001 | |
| SGA | A, (%) | 60% | 65.4% | 0.7010 | 61.3% | 70.7% | 0.2202 |
| B, (%) | 30% | 30.8% | 25.8% | 26.8% | |||
| C, (%) | 10% | 3.8% | 12.9% | 2.4% | |||
| Carpal Tunnel positive, n (%) * | 7 (35.0%) | 0 (0.0%) | 0.0012 | 14 (45.2%) | 1 (2.4%) | <0.0001 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/Licenses/by/4.0/).
Share and Cite
Santagati, G.; Cataldo, E.; Columbano, V.; Chatrenet, A.; Penna, D.; Pelosi, E.; Hachemi, M.; Gendrot, L.; Nielsen, L.; Cinquantini, F.; et al. Positron Emission Tomography Can Support the Diagnosis of Dialysis-Related Amyloidosis. J. Clin. Med. 2019, 8, 1494. https://doi.org/10.3390/jcm8091494
Santagati G, Cataldo E, Columbano V, Chatrenet A, Penna D, Pelosi E, Hachemi M, Gendrot L, Nielsen L, Cinquantini F, et al. Positron Emission Tomography Can Support the Diagnosis of Dialysis-Related Amyloidosis. Journal of Clinical Medicine. 2019; 8(9):1494. https://doi.org/10.3390/jcm8091494
Chicago/Turabian StyleSantagati, Giulia, Emanuela Cataldo, Valeria Columbano, Antoine Chatrenet, Daniele Penna, Ettore Pelosi, Mammar Hachemi, Lurlinys Gendrot, Louise Nielsen, Francesco Cinquantini, and et al. 2019. "Positron Emission Tomography Can Support the Diagnosis of Dialysis-Related Amyloidosis" Journal of Clinical Medicine 8, no. 9: 1494. https://doi.org/10.3390/jcm8091494
APA StyleSantagati, G., Cataldo, E., Columbano, V., Chatrenet, A., Penna, D., Pelosi, E., Hachemi, M., Gendrot, L., Nielsen, L., Cinquantini, F., Saulnier, P., Arena, V., Boursot, C., & Piccoli, G. B. (2019). Positron Emission Tomography Can Support the Diagnosis of Dialysis-Related Amyloidosis. Journal of Clinical Medicine, 8(9), 1494. https://doi.org/10.3390/jcm8091494