Evidence for Gender-Specific Bone Loss Mechanisms in Periprosthetic Osteolysis

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Ethical Statement
2.2. Patient Demographics
2.3. Osteocyte and Osteoclast Histomorphometric Analysis of Human Bone Biopsies
2.4. Statistical Analysis
3. Results
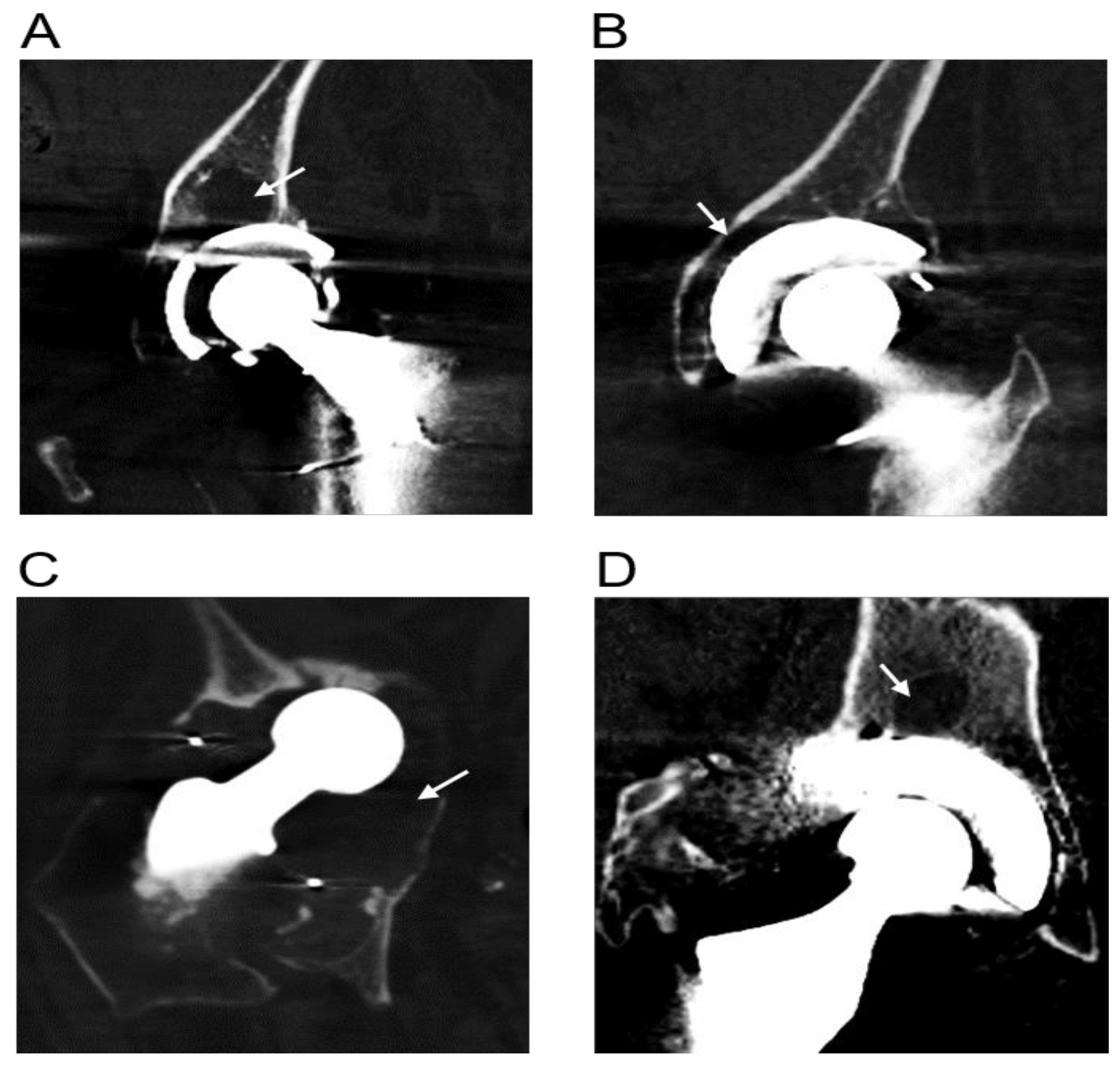
3.1. Radiographic Evidence of Osteolysis in Patients Undergoing Revision THR
3.2. Analysis of Human Bone Biopsies from Patients Undergoing Primary THR and Revision THR Surgery
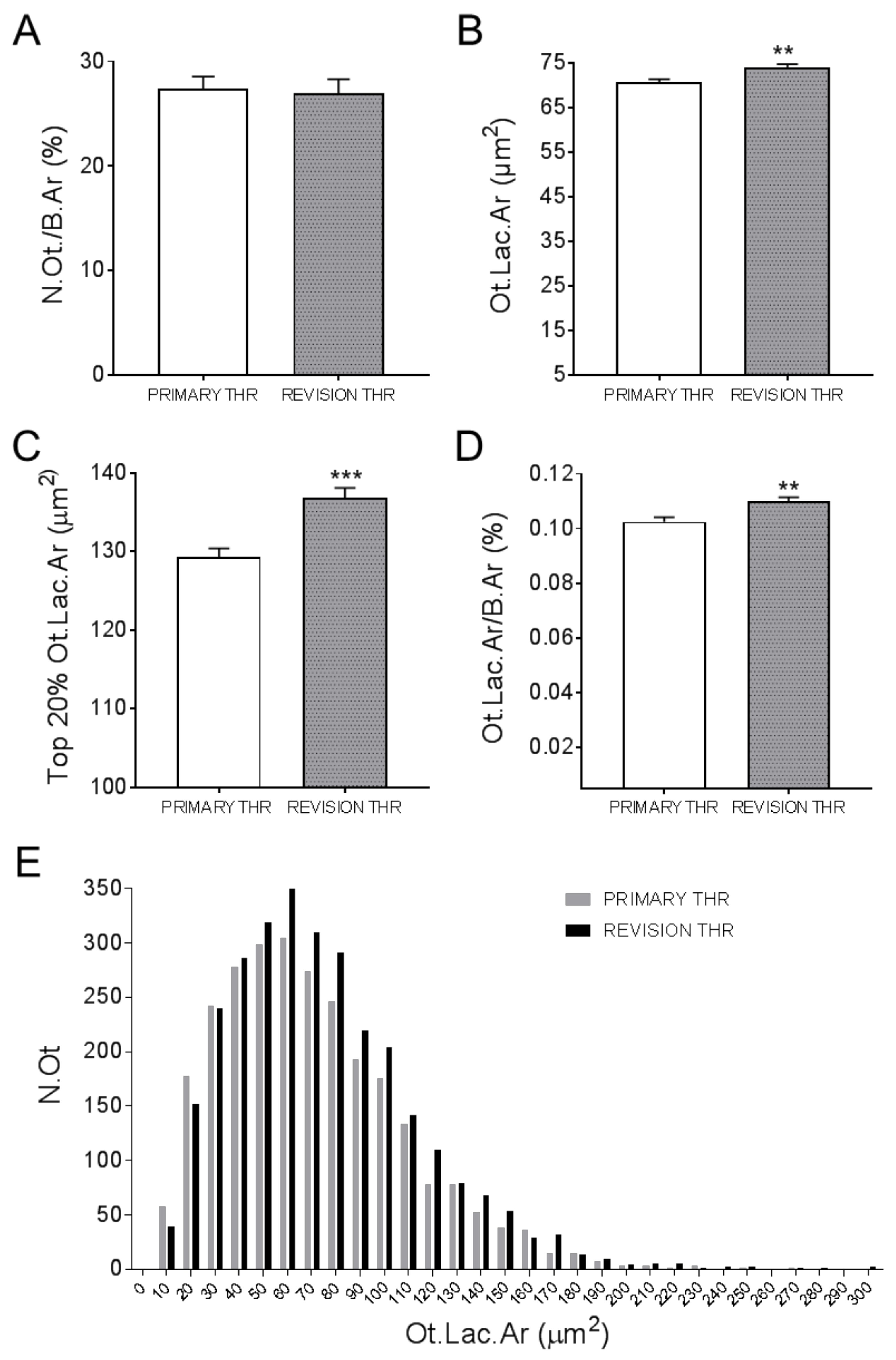
3.3. Osteocyte Characteristics of Primary and Revision THR Ccohorts
3.4. Osteocyte Characteristics of Female THR and Male THR Bone Biopsies
3.5. Osteoclast Analysis of Primary and Revision THR Bone Biopsies
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Australian Orthopaedic Association National Joint Replacement Registry Annual Report 2017. Available online: https://aoanjrr.sahmri.com/annual-reports-2017 (accessed on 30 June 2019).
- Abu-Amer, Y.; Darwech, I.; Clohisy, J.C. Aseptic loosening of total joint replacements: Mechanisms underlying osteolysis and potential therapies. Arthritis Res. Ther. 2007, 9 (Suppl. 1), S6. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, J.J.; Roebuck, K.A.; Archibeck, M.; Hallab, N.J.; Glant, T.T. Osteolysis: Basic science. Clin. Orthop. Relat. Res. 2001, 393, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Purdue, P.E.; Koulouvaris, P.; Nestor, B.J.; Sculco, T.P. The central role of wear debris in periprosthetic osteolysis. HSS J. 2006, 2, 102–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkins, G.J.; Haynes, D.R.; Howie, D.W.; Findlay, D.M. Role of polyethylene particles in peri-prosthetic osteolysis: A review. World J. Orthop. 2011, 2, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Athanasou, N.A. The pathobiology and pathology of aseptic implant failure. Bone Jt. Res. 2016, 5, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Howie, D.W.; Neale, S.D.; Haynes, D.R.; Holubowycz, O.T.; McGee, M.A.; Solomon, L.B.; Callary, S.A.; Atkins, G.J.; Findlay, D.M. Periprosthetic osteolysis after total hip replacement: Molecular pathology and clinical management. Inflammopharmacology 2013, 21, 389–396. [Google Scholar] [CrossRef] [Green Version]
- Dattani, R. Femoral osteolysis following total hip replacement. Postgrad Med. J. 2007, 83, 312–316. [Google Scholar] [CrossRef]
- Goodman, S.B.; Huie, P.; Song, Y.; Schurman, D.; Maloney, W.; Woolson, S.; Sibley, R. Cellular profile and cytokine production at prosthetic interfaces-study of tissues retrieved from revised hip and knee replacements. J. Bone Jt. Surg. Br. Vol. 1998, 80b, 531–539. [Google Scholar] [CrossRef]
- Magone, K.; Luckenbill, D.; Goswami, T. Metal ions as inflammatory initiators of osteolysis. Arch. Orthop. Trauma Surg. 2015, 135, 683–695. [Google Scholar] [CrossRef]
- Chang, J.D.; Lee, S.S.; Hur, M.; Seo, E.M.; Chung, Y.K.; Lee, C.J. Revision total hip arthroplasty in hip joints with metallosis: A single-center experience with 31 cases. J. Arthroplast. 2005, 20, 568–573. [Google Scholar] [CrossRef]
- Grosse, S.; Haugland, H.K.; Lilleng, P.; Ellison, P.; Hallan, G.; Hol, P.J. Wear particles and ions from cemented and uncemented titanium-based hip prostheses-a histological and chemical analysis of retrieval material. J. Biomed. Mater. Res. Part B Appl. Biomater. 2015, 103, 709–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haynes, D.R.; Boyle, S.J.; Rogers, S.D.; Howie, D.W.; Vernon-Roberts, B. Variation in cytokines induced by particles from different prosthetic materials. Clin. Orthop. Relat. Res. 1998, 352, 223–230. [Google Scholar] [CrossRef]
- Goodman, S.B.; Davidson, J.A.; Song, Y.; Martial, N.; Fornasier, V.L. Histomorphological reaction of bone to different concentrations of phagocytosable particles of high-density polyethylene and ti-6al-4v alloy in vivo. Biomaterials 1996, 17, 1943–1947. [Google Scholar] [CrossRef]
- Chiu, R.; Ma, T.; Smith, R.L.; Goodman, S.B. Ultrahigh molecular weight polyethylene wear debris inhibits osteoprogenitor proliferation and differentiation in vitro. J. Biomed. Mater. Res. Part A 2008. [Google Scholar] [CrossRef] [PubMed]
- Lohmann, C.H.; Schwartz, Z.; Koster, G.; Jahn, U.; Buchhorn, G.H.; MacDougall, M.J.; Casasola, D.; Liu, Y.; Sylvia, V.L.; Dean, D.D.; et al. Phagocytosis of wear debris by osteoblasts affects differentiation and local factor production in a manner dependent on particle composition. Biomaterials 2000, 21, 551–561. [Google Scholar] [CrossRef]
- Busse, B.; Hahn, M.; Niecke, M.; Jobke, B.; Puschel, K.; Delling, G.; Katzer, A. Allocation of nonbirefringent wear debris: Darkfield illumination associated with pixe microanalysis reveals cobalt deposition in mineralized bone matrix adjacent to cocr implants. J. Biomed. Mater. Res. Part A 2008, 87, 536–545. [Google Scholar] [CrossRef] [PubMed]
- Atkins, G.J.; Welldon, K.J.; Holding, C.A.; Haynes, D.R.; Howie, D.W.; Findlay, D.M. The induction of a catabolic phenotype in human primary osteoblasts and osteocytes by polyethylene particles. Biomaterials 2009, 30, 3672–3681. [Google Scholar] [CrossRef]
- Ormsby, R.T.; Cantley, M.; Kogawa, M.; Solomon, L.B.; Haynes, D.R.; Findlay, D.M.; Atkins, G.J. Evidence that osteocyte perilacunar remodelling contributes to polyethylene wear particle induced osteolysis. Acta Biomater. 2016, 33, 242–251. [Google Scholar] [CrossRef]
- Prideaux, M.; Findlay, D.M.; Atkins, G.J. Osteocytes: The master cells in bone remodelling. Curr. Opin. Pharmacol. 2016, 28, 24–30. [Google Scholar] [CrossRef]
- Bonewald, L.F. The amazing osteocyte. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2011, 26, 229–238. [Google Scholar] [CrossRef]
- Qing, H.; Ardeshirpour, L.; Pajevic, P.D.; Dusevich, V.; Jahn, K.; Kato, S.; Wysolmerski, J.; Bonewald, L.F. Demonstration of osteocytic perilacunar/canalicular remodeling in mice during lactation. J. Bone Miner. Res. 2012, 27, 1018–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, S.Y.; Herber, R.P.; Ho, S.P.; Alliston, T. Matrix metalloproteinase-13 is required for osteocytic perilacunar remodeling and maintains bone fracture resistance. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2012, 27, 1936–1950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogawa, M.; Wijenayaka, A.R.; Ormsby, R.T.; Thomas, G.P.; Anderson, P.H.; Bonewald, L.F.; Findlay, D.M.; Atkins, G.J. Sclerostin regulates release of bone mineral by osteocytes by induction of carbonic anhydrase 2. J. Bone Miner. Res. 2013, 28, 2436–2448. [Google Scholar] [CrossRef] [PubMed]
- Qing, H.; Bonewald, L.F. Osteocyte remodeling of the perilacunar and pericanalicular matrix. Int. J. Oral Sci. 2009, 1, 59–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, M.V.; Russell, P.K.; Findlay, D.M.; Sastra, S.; Anderson, P.H.; Skinner, J.P.; Atkins, G.J.; Zajac, J.D.; Davey, R.A. A role for the calcitonin receptor to limit bone loss during lactation in female mice by inhibiting osteocytic osteolysis. Endocrinology 2015, 156, 3203–3214. [Google Scholar] [CrossRef] [Green Version]
- Ormsby, R.T.; Solomon, L.B.; Yang, D.; Crotti, T.N.; Haynes, D.R.; Findlay, D.M.; Atkins, G.J. Osteocytes respond to particles of clinically-relevant conventional and cross-linked polyethylene and metal alloys by up-regulation of resorptive and inflammatory pathways. Acta Biomater. 2019, 87, 296–306. [Google Scholar] [CrossRef]
- Lane, N.E.; Yao, W.; Balooch, M.; Nalla, R.K.; Balooch, G.; Habelitz, S.; Kinney, J.H.; Bonewald, L.F. Glucocorticoid-treated mice have localized changes in trabecular bone material properties and osteocyte lacunar size that are not observed in placebo-treated or estrogen-deficient mice. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2006, 21, 466–476. [Google Scholar] [CrossRef] [Green Version]
- Bitar, D.; Parvizi, J. Biological response to prosthetic debris. World J. Orthop. 2015, 6, 172–189. [Google Scholar] [CrossRef]
- Rokkum, M.; Brandt, M.; Bye, K.; Hetland, K.R.; Waage, S.; Reigstad, A. Polyethylene wear, osteolysis and acetabular loosening with an ha-coated hip prosthesis. A follow-up of 94 consecutive arthroplasties. J. Bone Jt. Surg. Br. Vol. 1999, 81, 582–589. [Google Scholar] [CrossRef]
- Beck, R.T.; Illingworth, K.D.; Saleh, K.J. Review of periprosthetic osteolysis in total joint arthroplasty: An emphasis on host factors and future directions. J. Orthopaed Res. 2012, 30, 541–546. [Google Scholar] [CrossRef]
- Schmalzried, T.P.; Shepherd, E.F.; Dorey, F.J.; Jackson, W.O.; dela Rosa, M.; Fa’vae, F.; McKellop, H.A.; McClung, C.D.; Martell, J.; Moreland, J.R.; et al. The john charnley award. Wear is a function of use, not time. Clin. Orthop. Relat. Res. 2000, i7, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Wysolmerski, J.J. Osteocytes remove and replace perilacunar mineral during reproductive cycles. Bone 2013, 54, 230–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salari, P.; Abdollahi, M. The influence of pregnancy and lactation on maternal bone health: A systematic review. J. Fam. Reprod Health 2014, 8, 135–148. [Google Scholar]
- Sanz-Salvador, L.; Garcia-Perez, M.A.; Tarin, J.J.; Cano, A. Bone metabolic changes during pregnancy: A period of vulnerability to osteoporosis and fracture. Eur. J. Endocrinol. 2015, 172, R53–R65. [Google Scholar] [CrossRef]
- Sowers, M.R.; Greendale, G.A.; Bondarenko, I.; Finkelstein, J.S.; Cauley, J.A.; Neer, R.M.; Ettinger, B. Endogenous hormones and bone turnover markers in pre- and perimenopausal women: Swan. Osteoporos. Int. 2003, 14, 191–197. [Google Scholar] [CrossRef]
- Nicks, K.M.; Fowler, T.W.; Gaddy, D. Reproductive hormones and bone. Curr. Osteoporos Rep. 2010, 8, 60–67. [Google Scholar] [CrossRef]
- Yang, D.; Wijenayaka, A.R.; Solomon, L.B.; Pederson, S.M.; Findlay, D.M.; Kidd, S.P.; Atkins, G.J. Novel insights into staphylococcus aureus deep bone infections: The involvement of osteocytes. MBio 2018, 9, e00415-18. [Google Scholar] [CrossRef] [Green Version]
- Sundararaghavan, V.; Mazur, M.M.; Evans, B.; Liu, J.; Ebraheim, N.A. Diabetes and bone health: Latest evidence and clinical implications. Ther. Adv. Musculoskelet Dis. 2017, 9, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Al-Bashaireh, A.M.; Haddad, L.G.; Weaver, M.; Kelly, D.L.; Chengguo, X.; Yoon, S. The effect of tobacco smoking on musculoskeletal health: A systematic review. J. Environ. Public Health 2018, 2018, 4184190. [Google Scholar] [CrossRef]
- Savvidis, C.; Tournis, S.; Dede, A.D. Obesity and bone metabolism. Horm. (Athens) 2018, 17, 205–217. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Range | Mean Age | Number Per Group | |
|---|---|---|---|
| Primary THR | 69–89 | 74 | 20 (M 10, F 10) |
| Revision THR | 69–91 | 80 | 21 (M 10, F 11) |
| Male Primary THR | 70–83 | 75 | 10 |
| Male Revision THR | 69–87 | 79 | 10 |
| Female Primary THR | 69–89 | 75 | 10 |
| Female Revision THR | 69–91 | 80 | 11 |
| Patient | Sex | Age | Acetabular Cup Name | Cup Material | Liner | Stem Name | Stem Material | Particle Type |
|---|---|---|---|---|---|---|---|---|
| 1 | F | 69 | Trilogy | Titanium | UHMWPE | CPT© | Co-Cr Alloy | Metal |
| 2 | F | 74 | PCA | Vitallium | UHMWPE | PCA | Vitallium | Not detected |
| 3 | F | 76 | HGP | Titanium | UHMWPE | Zimmer Anatomic II | Titanium | Both |
| 4 | F | 79 | Exeter | Steel | UHMWPE | Exeter | Steel | Metal |
| 5 | F | 82 | HGP | Titanium | UHMWPE | HGP | Titanium | Both |
| 6 | F | 82 | Unknown | Unknown | UHMWPE | Unknown | Unknown | Both |
| 7 | F | 83 | Exeter | All-Poly Cup | UHMWPE | Exeter polished monoblock | Stainless Steel | PE |
| 8 | F | 84 | None | None | None | Exeter Hemiarthroplasty | Stainless Steel | Metal |
| 9 | F | 86 | Trilogy | Titanium | XLPE | MULLER | Stainless steel and Titanium | Both |
| 10 | F | 89 | MULLER | All-Poly Cup | UHMWPE | MULLER | Co-Cr-Mo-Ni | Both |
| 11 | F | 91 | Unknown | Unknown | Unknown | Unknown | Unknown | Not detected |
| 12 | M | 69 | Howmedica All-Poly Cup | All-Poly Cup | UHMWPE | Howmedica Osteonics ODC | Co-Cr Alloy | Metal |
| 13 | M | 71 | Charnley | All-Poly Cup | UHMWPE | Unknown | Unknown | Not detected |
| 14 | M | 73 | PCA | Vitallium | UHMWPE | PCA | Vitallium | Both |
| 15 | M | 76 | Biomet | Titanium | UHMWPE | Unknown | Unknown | PE |
| 16 | M | 77 | PCA | Vitallium | UHMWPE | PCA | Vitallium | Both |
| 17 | M | 81 | Charnley | All-Poly Cup | UHMWPE | Charnley | Stainless Steel | PE |
| 18 | M | 83 | Trilogy | Unknown | UHMWPE | CPT | Co-Cr Alloy | Not detected |
| 19 | M | 84 | CLS | Titanium | UHMWPE | CLS | Titanium | PE |
| 20 | M | 87 | Meridian | Vitallium | UHMWPE | Vitaloc | Vitallium | PE |
| 21 | M | 87 | Unknown | Unknown | Unknown | Unknown | Unknown | PE |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ormsby, R.T.; Solomon, L.B.; Stamenkov, R.; Findlay, D.M.; Atkins, G.J. Evidence for Gender-Specific Bone Loss Mechanisms in Periprosthetic Osteolysis. J. Clin. Med. 2020, 9, 53. https://doi.org/10.3390/jcm9010053
Ormsby RT, Solomon LB, Stamenkov R, Findlay DM, Atkins GJ. Evidence for Gender-Specific Bone Loss Mechanisms in Periprosthetic Osteolysis. Journal of Clinical Medicine. 2020; 9(1):53. https://doi.org/10.3390/jcm9010053
Chicago/Turabian StyleOrmsby, Renee T., Lucian B. Solomon, Roumen Stamenkov, David M. Findlay, and Gerald J. Atkins. 2020. "Evidence for Gender-Specific Bone Loss Mechanisms in Periprosthetic Osteolysis" Journal of Clinical Medicine 9, no. 1: 53. https://doi.org/10.3390/jcm9010053
APA StyleOrmsby, R. T., Solomon, L. B., Stamenkov, R., Findlay, D. M., & Atkins, G. J. (2020). Evidence for Gender-Specific Bone Loss Mechanisms in Periprosthetic Osteolysis. Journal of Clinical Medicine, 9(1), 53. https://doi.org/10.3390/jcm9010053