An Intraoral OCT Probe to Enhanced Detection of Approximal Carious Lesions and Assessment of Restorations


 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
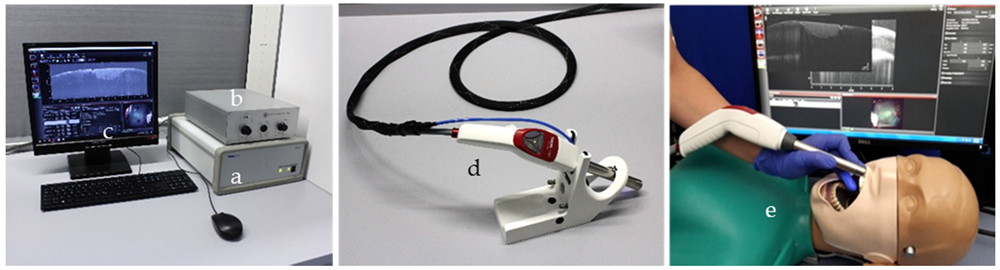
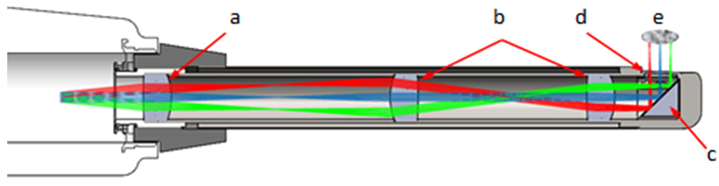
2.1. SD-OCT System and Hand-Held Probe
2.2. In-Vitro Study
2.3. In-Vivo Study Caries Diagnosis
2.3.1. Visual-Tactile Probing/FOTI/Radiography/Intraoral OCT
2.3.2. Calibration of Examiners and Image Analysis
2.3.3. Scoring and Statistical Analysis
- -
- Visual inspection: ICDAS, sound (0, ICDAS, code 0) or carious lesion (1, ICDAS, code 1–4)
- -
- Fiber optic transillumination: no shadow (0), shadow representing a carious lesion (1)
- -
- Bitewing radiography: no radiolucency (0) or radiolucency (1)
- -
- OCT: B scans, no signal representing a carious lesion (0) or signal present (1)
2.4. In-Vivo Study-Assessment of Tooth-Colored Restorations
3. Results
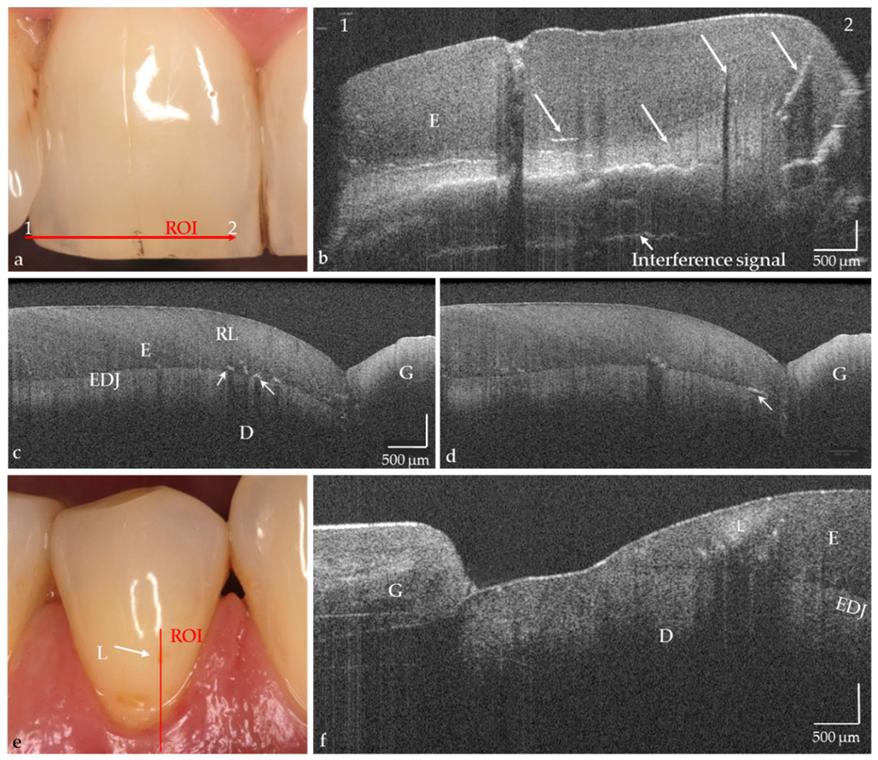
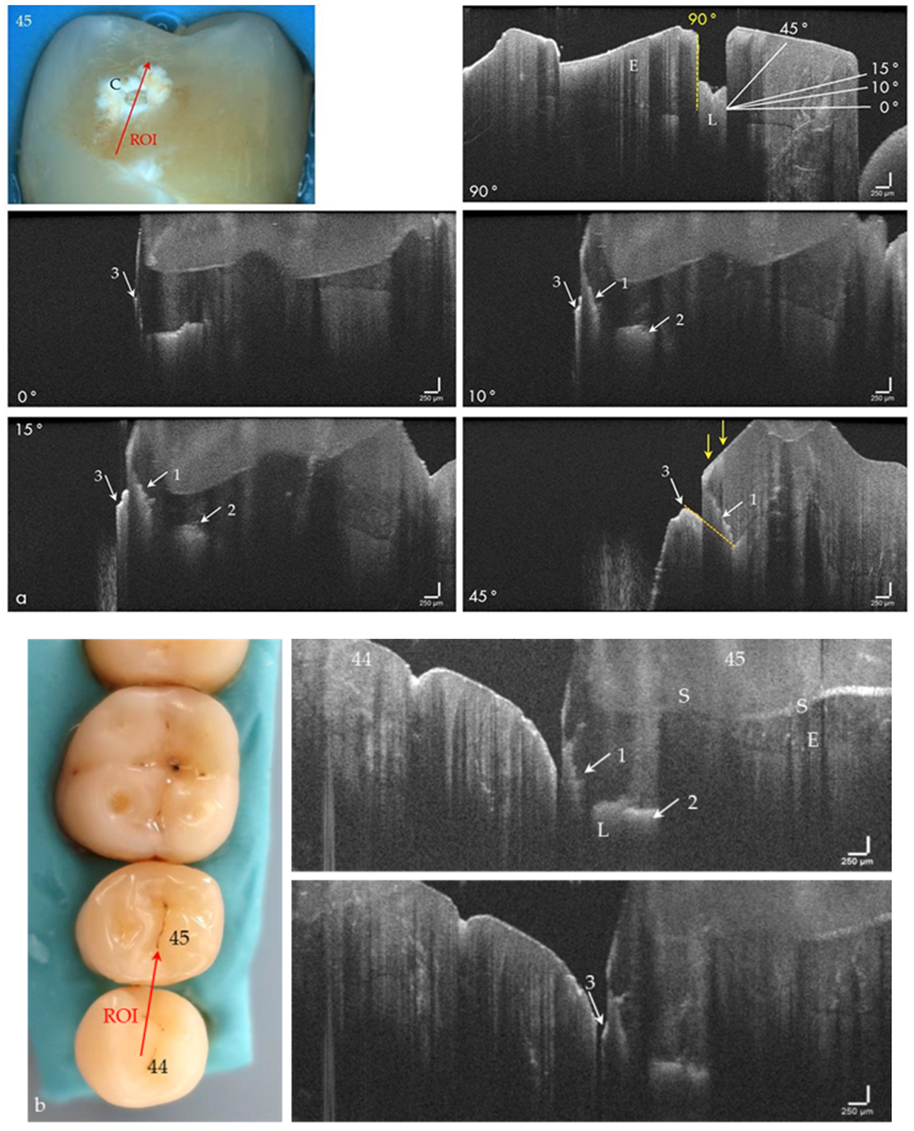
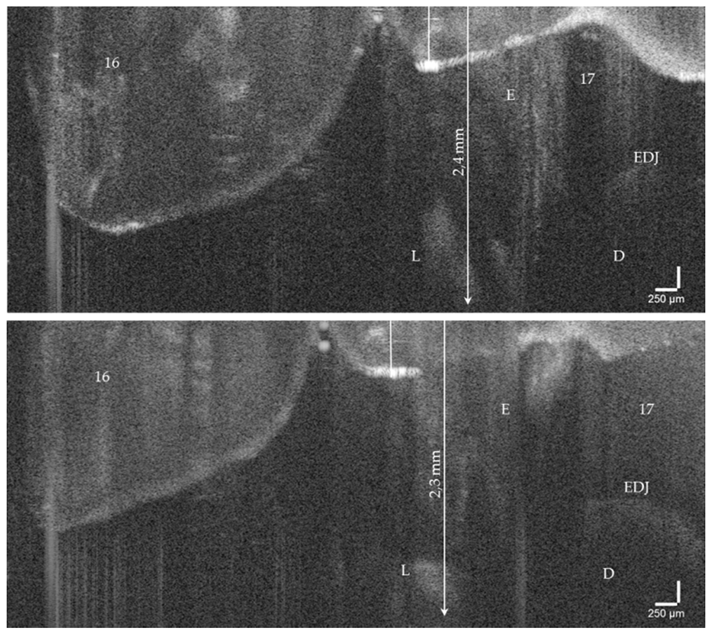
3.1. OCT Imaging of Human Teeth In Vitro and Intraorally
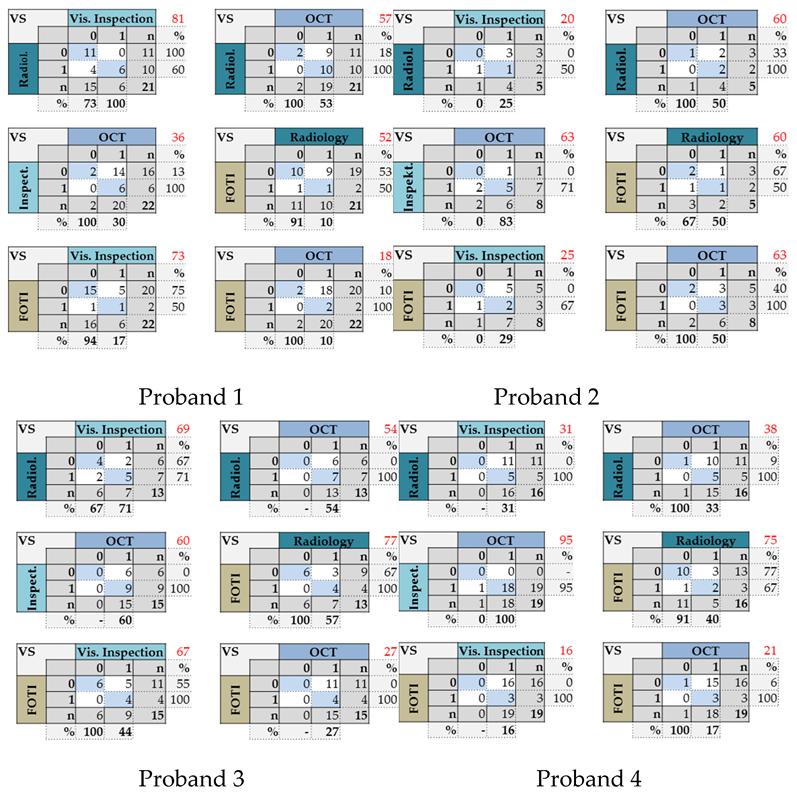
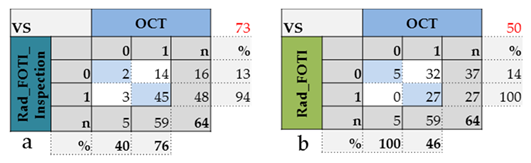
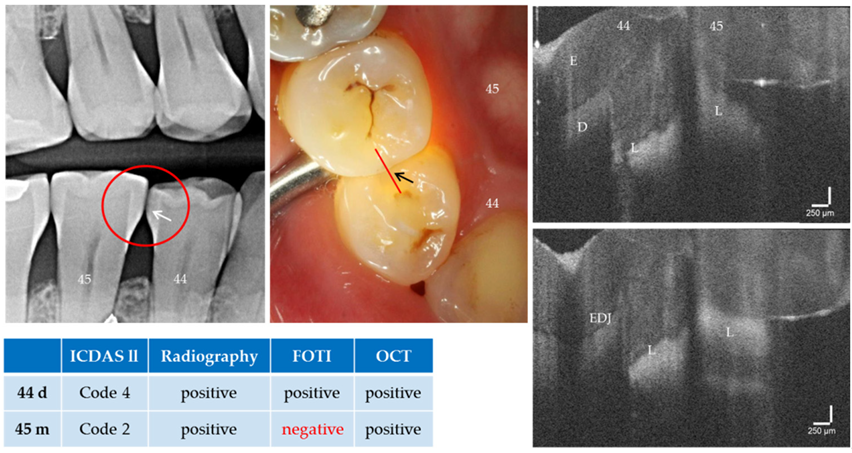
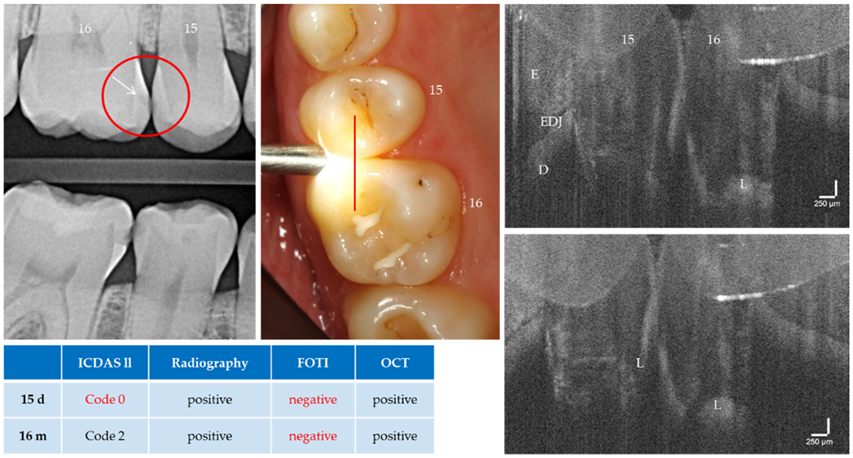
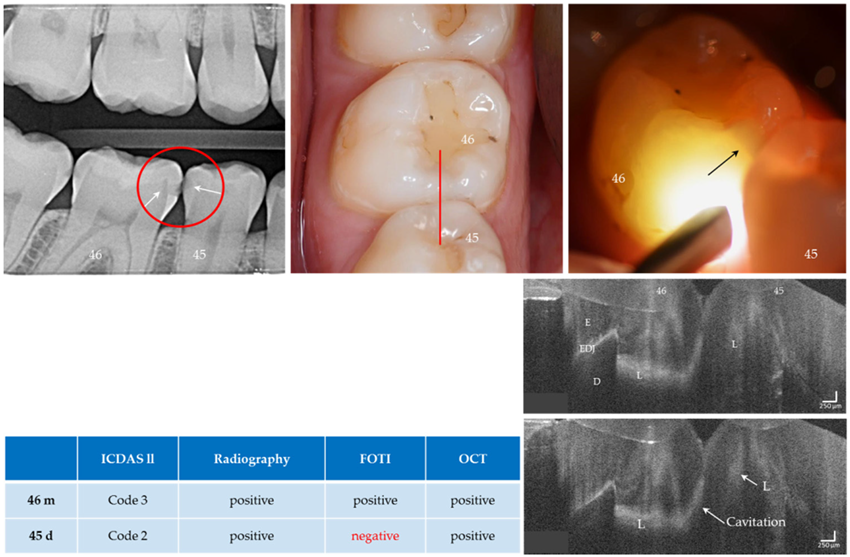
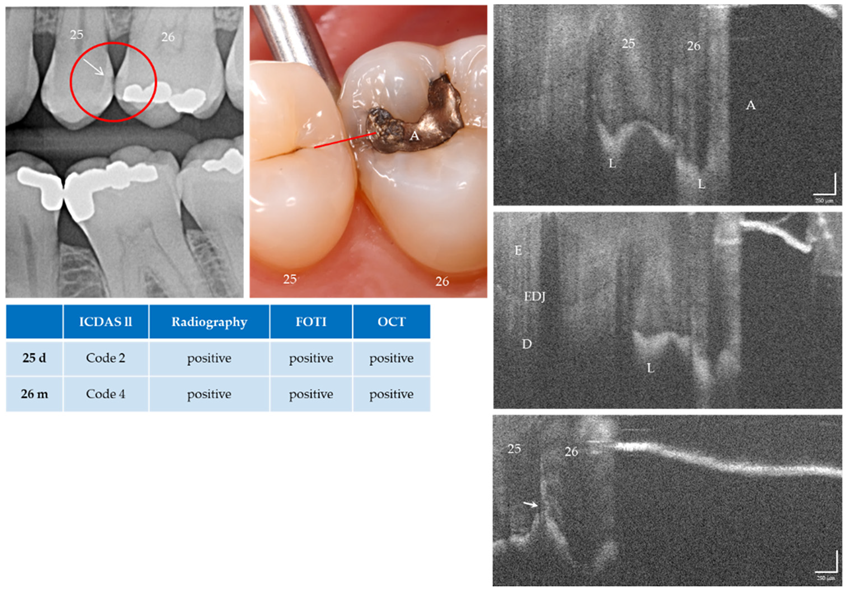
3.2. Approximal Caries Diagnosis
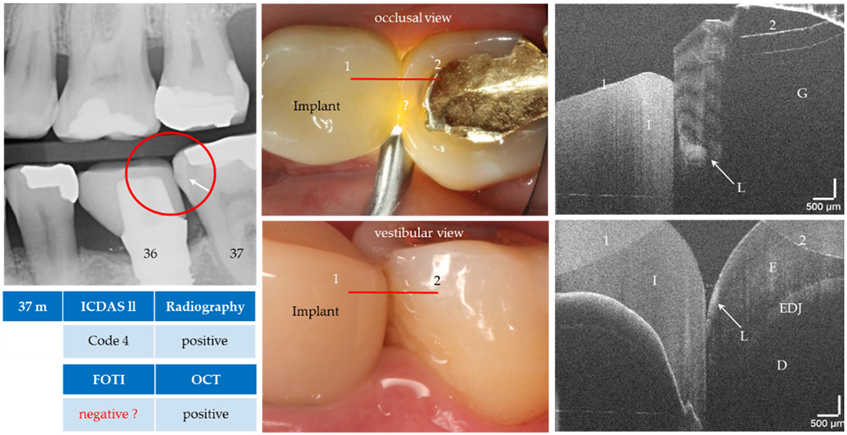
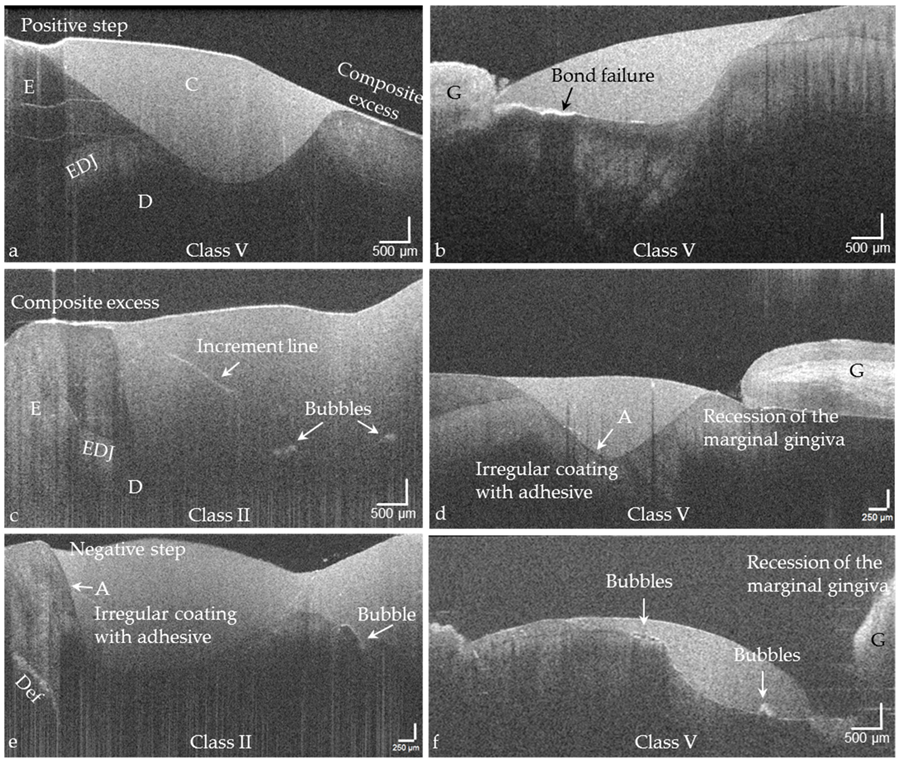
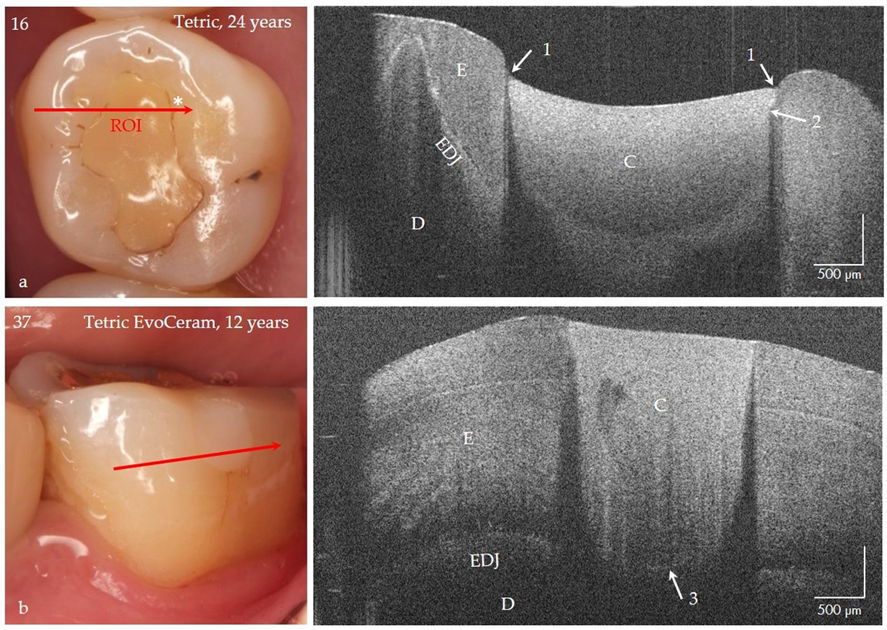
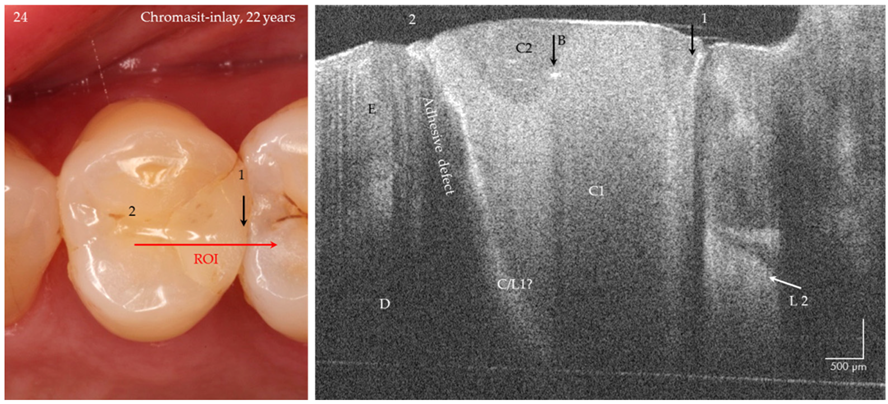
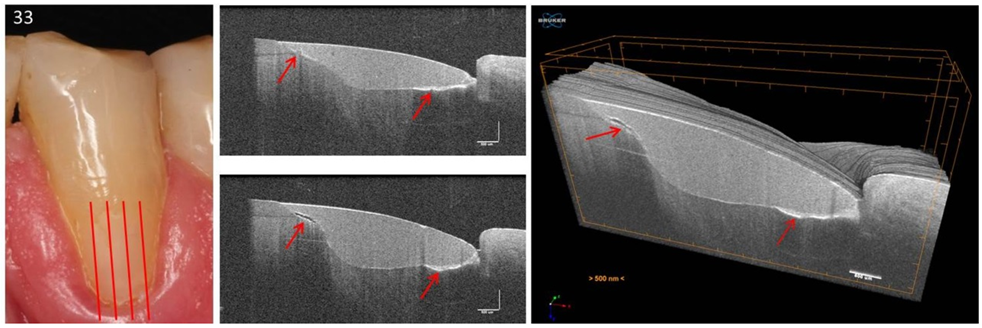
3.3. Tooth-Colored Restorations—Intraoral Imaging and Evaluation
4. Discussion
4.1. Diagnosis of Proximal Carious Lesions
4.2. Tooth-Colored Restorations
4.3. Methodological Criticism/Limitations of the Intraoral OCT Probe
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kassebaum, N.; Smith, A.G.; Bernabé, E.; Fleming, T.; Reynolds, A.; Vos, T.; Murray, C.; Marcenes, W.; Abyu, G. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral health1, Oral deseases: A global public heatth challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Watt, R.G.; Daly, B.; Allison, P.; MacPherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreño, C.C.; Celeste, R.K.; et al. Ending the neglect of global oral health: Time for radical action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]
- Gomez, J. Detection and diagnosis of the early caries lesion. BMC Oral Health 2015, 15, S3. [Google Scholar] [CrossRef] [Green Version]
- Abdullah, Z.; John, J. Minimally Invasive Treatment of White Spot Lesions—A Systematic Review. Oral Health Prev. Dent. 2016, 14, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diniz, M.B.; Rodrigues, J.A.; Hug, I.; Cordeiro, R.D.C.L.; Lussi, A. Reproducibility and accuracy of the ICDAS-II for occlusal caries detection. Community Dent. Oral Epidemiol. 2009, 37, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Gimenez, T.; Piovesan, C.; Braga, M.; Raggio, D.; Deery, C.; Ricketts, D.; Ekstrand, K.; Mendes, F. Visual Inspection for Caries Detection. J. Dent. Res. 2015, 94, 895–904. [Google Scholar] [CrossRef]
- Karlsson, L. Caries Detection Methods Based on Changes in Optical Properties between Healthy and Carious Tissue. Int. J. Dent. 2010, 2010, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Abogazalah, N.; Ando, M. Alternative methods to visual and radiographic examinations for approximal caries detection. J. Oral Sci. 2017, 59, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Pretty, I.A. Caries detection and diagnosis: Novel technologies. J. Dent. 2006, 34, 727–739. [Google Scholar] [CrossRef] [PubMed]
- Mialhe, F.L.; Pereira, A.C.; Pardi, V.; Meneghim, M.D.C. Comparison of three methods for detection of carious lesions in proximal surfaces versus direct visual examination after tooth separation. J. Clin. Pediatric Dent. 2003, 28, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, G.; Pitchika, V.; Litzenburger, F.; Hickel, R.; Kühnisch, J. Evaluation of occlusal caries detection and assessment by visual inspection, digital bitewing radiography and near-infrared light transillumination. Clin. Oral Investig. 2018, 22, 2431–2438. [Google Scholar] [CrossRef] [PubMed]
- Alammari, M.R.; Smith, P.W.; De Jong, E.D.J.; Higham, S.M. Quantitative light-induced fluorescence (QLF): A tool for early occlusal dental caries detection and supporting decision making in vivo. J. Dent. 2013, 41, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.S.; Huynh, G.D.; Jones, G.C.; Fried, D. Near-infrared transillumination at 1310-nm for the imaging of early dental decay. Opt. Express 2003, 11, 2259–2265. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, F.; Askar, H.; Paris, S.; Schwendicke, F. Detecting Secondary Caries Lesions. J. Dent. Res. 2015, 95, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Machiulskiene, V.; Campus, G.; Carvalho, J.C.; Dige, I.; Ekstrand, K.R.; Jablonski-Momeni, A.; Maltz, M.; Manton, D.J.; Martignon, S.; Martinez-Mier, E.A.; et al. Terminology of Dental Caries and Dental Caries Management: Consensus Report of a Workshop Organized by ORCA and Cariology Research Group of IADR. Caries Res. 2020, 54, 7–14. [Google Scholar] [CrossRef]
- Nedeljkovic, I.; Teughels, W.; De Munck, J.; Van Meerbeek, B.; Van Landuyt, K.L. Is secondary caries with composites a material-based problem? Dent. Mater. 2015, 31, e247–e277. [Google Scholar] [CrossRef]
- Hickel, R.; Roulet, J.-F.; Bayne, S.; Heintze, S.D.; Mjör, I.A.; Peters, M.; Rousson, V.; Randall, R.; Schmalz, G.; Tyas, M.; et al. Recommendations for conducting controlled clinical studies of dental restorative materials. Clin. Oral Investig. 2007, 11, 5–33. [Google Scholar] [CrossRef]
- Schneider, H.; Steigerwald-Otremba, A.; Häfer, M.; Krause, F.; Scholz, M.; Haak, R. Is Optical Coherence Tomography a Potential Tool to Evaluate Marginal Adaptation of Class III/IV Composite Restorations In Vivo? Oper. Dent. 2019, 44, 242–253. [Google Scholar] [CrossRef]
- Katkar, R.A.; Tadinada, S.A.; Amaechi, B.T.; Fried, D. Optical Coherence Tomography. Dent. Clin. N. Am. 2018, 62, 421–434. [Google Scholar] [CrossRef]
- Machoy, M.; Seeliger, J.; Szyszka-Sommerfeld, L.; Koprowski, R.; Gedrange, T.; Woźniak, K. The Use of Optical Coherence Tomography in Dental Diagnostics: A State-of-the-Art Review. J. Heal. Eng. 2017, 2017, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Schneider, H.; Park, K.-J.; Häfer, M.; Rüger, C.; Schmalz, G.; Krause, F.; Schmidt, J.; Ziebolz, D.; Haak, R. Dental Applications of Optical Coherence Tomography (OCT) in Cariology. Appl. Sci. 2017, 7, 472. [Google Scholar] [CrossRef] [Green Version]
- Haak, R.; Schmidt, P.; Park, K.-J.; Häfer, M.; Krause, F.; Ziebolz, D.; Schneider, H. OCT for early quality evaluation of tooth–composite bond in clinical trials. J. Dent. 2018, 76, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Haak, R.; Hähnel, M.; Schneider, H.; Rosolowski, M.; Park, K.-J.; Ziebolz, D.; Häfer, M. Clinical and OCT outcomes of a universal adhesive in a randomized clinical trial after 12 months. J. Dent. 2019, 90, 103200. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.-T.; Wang, Y.-L.; Yeh, T.-W.; Lee, H.-C.; Chen, W.-J.; Ke, J.-L.; Lee, Y. Early detection of enamel demineralization by optical coherence tomography. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sahyoun, C.C.; Subhash, H.M.; Peru, D.; Ellwood, R.P.; Pierce, M.C. An Experimental Review of Optical Coherence Tomography Systems for Noninvasive Assessment of Hard Dental Tissues. Caries Res. 2020, 54, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [Green Version]
- Wylęgała, A.; Teper, S.; Dobrowolski, D.; Wylęgała, E. Optical coherence angiography: A review. Medicine 2016, 95, e4907. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.M.; Lo, S.; Scolyer, R.; Meekings, A.; Carlos, G.; Guitera, P. Accuracy of optical coherence tomography for the diagnosis of superficial basal cell carcinoma—A prospective, consecutive, cohort study of 168 cases. Br. J. Dermatol. 2016, 175, 1290–1300. [Google Scholar] [CrossRef]
- Vignali, L.; Solinas, E.; Emanuele, E. Research and Clinical Applications of Optical Coherence Tomography in Invasive Cardiology: A Review. Curr. Cardiol. Rev. 2014, 10, 369–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colston, B.; Sathyam, U.S.; DaSilva, L.; Everett, M.; Otis, L.; Stroeve, P. Dental OCT. Opt. Express 1998, 3, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Shimada, Y.; Nakagawa, H.; Sadr, A.; Wada, I.; Nakajima, M.; Nikaido, T.; Otsuki, M.; Tagami, J.; Sumi, Y. Noninvasive cross-sectional imaging of proximal caries using swept-source optical coherence tomography (SS-OCT) in vivo. J. Biophotonics 2014, 7, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Wada, I.; Shimada, Y.; Ikeda, M.; Sadr, A.; Nakashima, S.; Tagami, J.; Sumi, Y.; Ikumi, W.; Yasushi, S.; Alireza, S.; et al. Clinical assessment of non carious cervical lesion using swept-source optical coherence tomography. J. Biophotonics 2015, 8, 846–854. [Google Scholar] [CrossRef]
- Nakajima, Y.; Shimada, Y.; Sadr, A.; Wada, I.; Miyashin, M.; Takagi, Y.; Tagami, J.; Sumi, Y. Detection of occlusal caries in primary teeth using swept source optical coherence tomography. J. Biomed. Opt. 2014, 19, 016020. [Google Scholar] [CrossRef] [PubMed]
- Ibusuki, T.; Kitasako, Y.; Sadr, A.; Shimada, Y.; Sumi, Y.; Tagami, J. Obser vation of white spot lesions using swept source optical coherence tomography (SS-OCT): In vitro and in vivo study. Dent. Mater. J. 2015, 34, 545–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haak, R.; Ahrens, M.; Schneider, H.; Strumpski, M.; Rueger, C.; Haefer, M.; Hüttmann, G.; Theisen-Kunde, D.; Schulz-Hildebrandt, H. Handheld OCT probe for intraoral diagnosis on teeth. In Proceedings of the Clinical and Preclinical Optical Diagnostics II. Preclinical and Clinical Optical Diagnostics, Munich, Germany, 23–27 June 2019; Brown, J.Q., Van Leeuwen, T.G., Eds.; SPIE: Bellingham, WA, USA, 2019; p. 31. [Google Scholar]
- Walther, J.; Schnabel, C.; Tetschke, F.; Rosenauer, T.; Golde, J.; Ebert, N.; Baumann, M.; Hannig, C.; Koch, E. In vivo imaging in the oral cavity by endoscopic optical coherence tomography. J. Biomed. Opt. 2018, 23, 071207. [Google Scholar] [CrossRef] [Green Version]
- Park, K.-J.; Schneider, H.; Haak, R. Assessment of interfacial defects at composite restorations by swept source optical coherence tomography. J. Biomed. Opt. 2013, 18, 076018. [Google Scholar] [CrossRef] [Green Version]
- Park, K.-J.; Schneider, H.; Haak, R. Assessment of defects at tooth/self-adhering flowable composite interface using swept-source optical coherence tomography (SS-OCT). Dent. Mater. 2015, 31, 534–541. [Google Scholar] [CrossRef]
- Park, K.-J.; Haak, R.; Ziebolz, D.; Krause, F.; Schneider, H.; Hartmut, S. OCT assessment of non-cavitated occlusal carious lesions by variation of incidence angle of probe light and refractive index matching. J. Dent. 2017, 62, 31–35. [Google Scholar] [CrossRef]
- Park, K.-J.; Schneider, H.; Ziebolz, D.; Krause, F.; Haak, R. Optical coherence tomography to evaluate variance in the extent of carious lesions in depth. Lasers Med. Sci. 2018, 33, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.; Ekstrand, K.R.; Foundation, T.I. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS) - Methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef]
- Schwendicke, F.; Frencken, J.E.; Bjørndal, L.; Maltz, M.; Manton, D.; Ricketts, D.; Van Landuyt, K.; Banerjee, A.; Campus, G.; Doméjean, S.; et al. Managing Carious Lesions. Adv. Dent. Res. 2016, 28, 58–67. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, H.; Sadr, A.; Shimada, Y.; Tagami, J.; Sumi, Y. Validation of swept source optical coherence tomography (SS-OCT) for the diagnosis of smooth surface caries in vitro. J. Dent. 2013, 41, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Shimada, Y.; Sadr, A.; Sumi, Y.; Tagami, J. Application of Optical Coherence Tomography (OCT) for Diagnosis of Caries, Cracks, and Defects of Restorations. Curr. Oral Health Rep. 2015, 2, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, J.C.; Darling, C.L.; Fried, D. Assessment of cavitation in artificial approximal dental lesions with near-IR imaging. In Proceedings of the SPIE BiOS, San Francisco, CA, USA, 28 January 2017; Rechmann, P., Fried, D., Eds.; SPIE: Bellingham, WA, USA, 2017; p. 1004407. [Google Scholar]
- De Munck, J.; Van Meerbeek, B.; Yoshida, Y.; Inoue, S.; Vargas, M.; Suzuki, K.; Lambrechts, P.; Vanherle, G. Four-year Water Degradation of Total-etch Adhesives Bonded to Dentin. J. Dent. Res. 2003, 82, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Schneider, H.; Park, K.-J.; Rüger, C.; Ziebolz, D.; Krause, F.; Haak, R. Imaging resin infiltration into non-cavitated carious lesions by optical coherence tomography. J. Dent. 2017, 60, 94–98. [Google Scholar] [CrossRef] [PubMed]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Central wavelength ± bandwidth | 1310 nm ± 107 nm |
| Power on sample | 2.3 mW |
| Sensitivity | ≤106 dB |
| Imaging depth | 2.5 mm |
| Pixels per A-scan | 727 |
| NA | 0.011 |
| Axial resolution (water) | 5.5 µm |
| Lateral resolution (spot size) | 11.5 µm |
| A-scan | 28 kHz |
| B-scan | 10 Hz |
| FOV (maximal) | ≤8 mm × 8 mm |
| Angulation | 90° |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider, H.; Ahrens, M.; Strumpski, M.; Rüger, C.; Häfer, M.; Hüttmann, G.; Theisen-Kunde, D.; Schulz-Hildebrandt, H.; Haak, R. An Intraoral OCT Probe to Enhanced Detection of Approximal Carious Lesions and Assessment of Restorations. J. Clin. Med. 2020, 9, 3257. https://doi.org/10.3390/jcm9103257
Schneider H, Ahrens M, Strumpski M, Rüger C, Häfer M, Hüttmann G, Theisen-Kunde D, Schulz-Hildebrandt H, Haak R. An Intraoral OCT Probe to Enhanced Detection of Approximal Carious Lesions and Assessment of Restorations. Journal of Clinical Medicine. 2020; 9(10):3257. https://doi.org/10.3390/jcm9103257
Chicago/Turabian StyleSchneider, Hartmut, Martin Ahrens, Michaela Strumpski, Claudia Rüger, Matthias Häfer, Gereon Hüttmann, Dirk Theisen-Kunde, Hinnerk Schulz-Hildebrandt, and Rainer Haak. 2020. "An Intraoral OCT Probe to Enhanced Detection of Approximal Carious Lesions and Assessment of Restorations" Journal of Clinical Medicine 9, no. 10: 3257. https://doi.org/10.3390/jcm9103257
APA StyleSchneider, H., Ahrens, M., Strumpski, M., Rüger, C., Häfer, M., Hüttmann, G., Theisen-Kunde, D., Schulz-Hildebrandt, H., & Haak, R. (2020). An Intraoral OCT Probe to Enhanced Detection of Approximal Carious Lesions and Assessment of Restorations. Journal of Clinical Medicine, 9(10), 3257. https://doi.org/10.3390/jcm9103257