Belching in Gastroesophageal Reflux Disease: Literature Review


Abstract
:1. Introduction
2. Two Types of Belching: Gastric Belching and Supragastric Belching
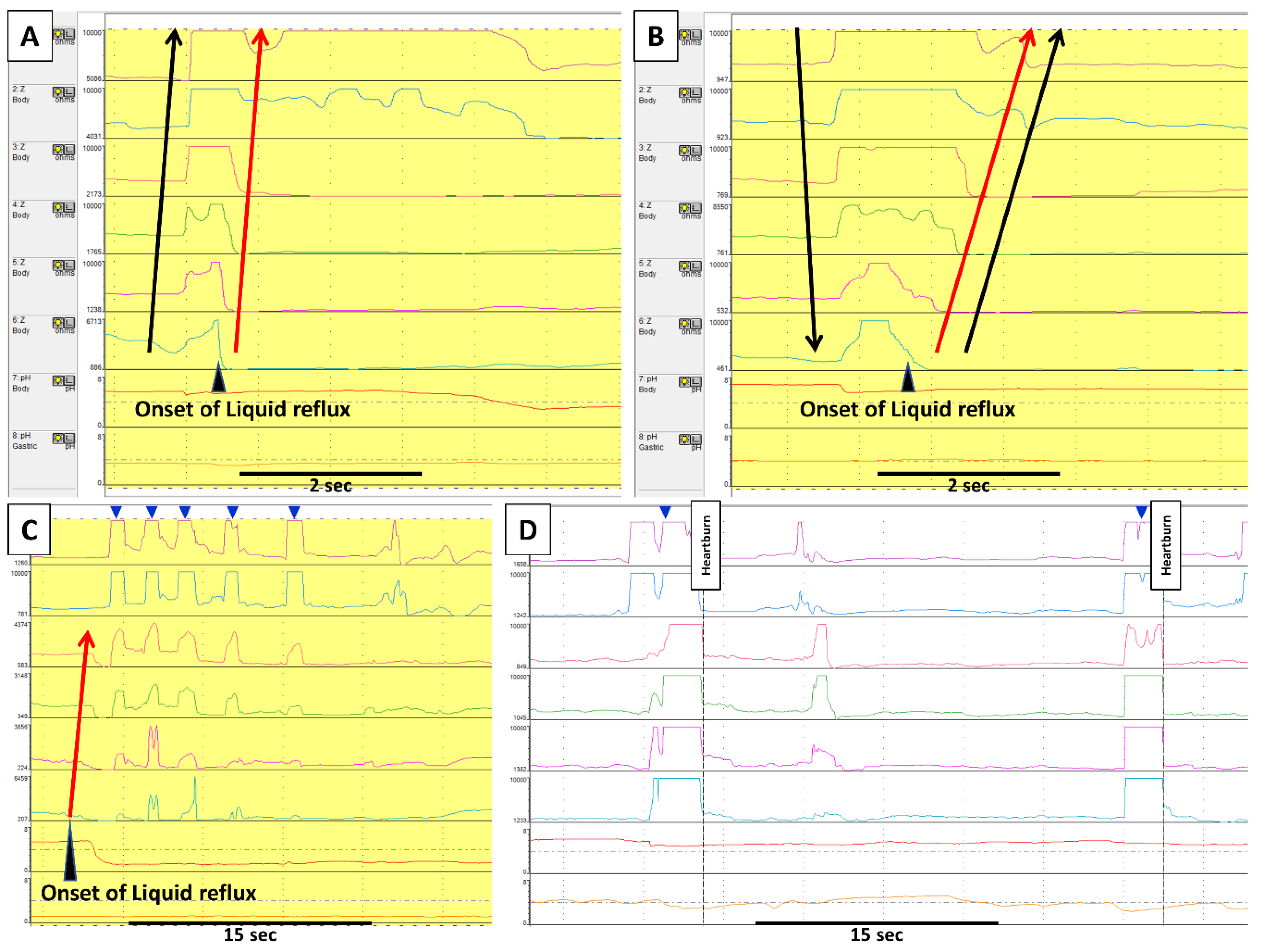
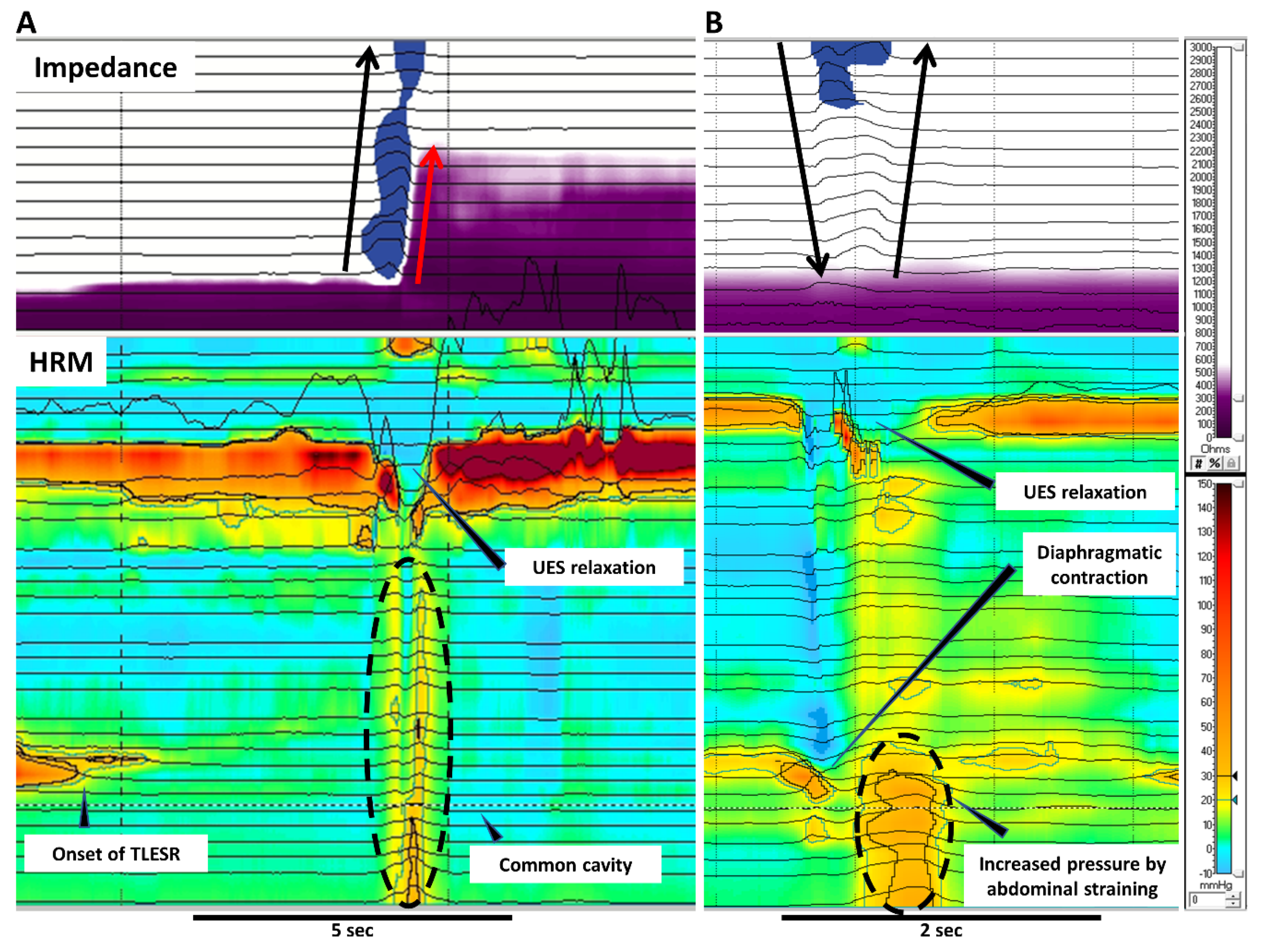
2.1. Gastric Belching (GB)
2.2. Supragastric Belching (SGB)
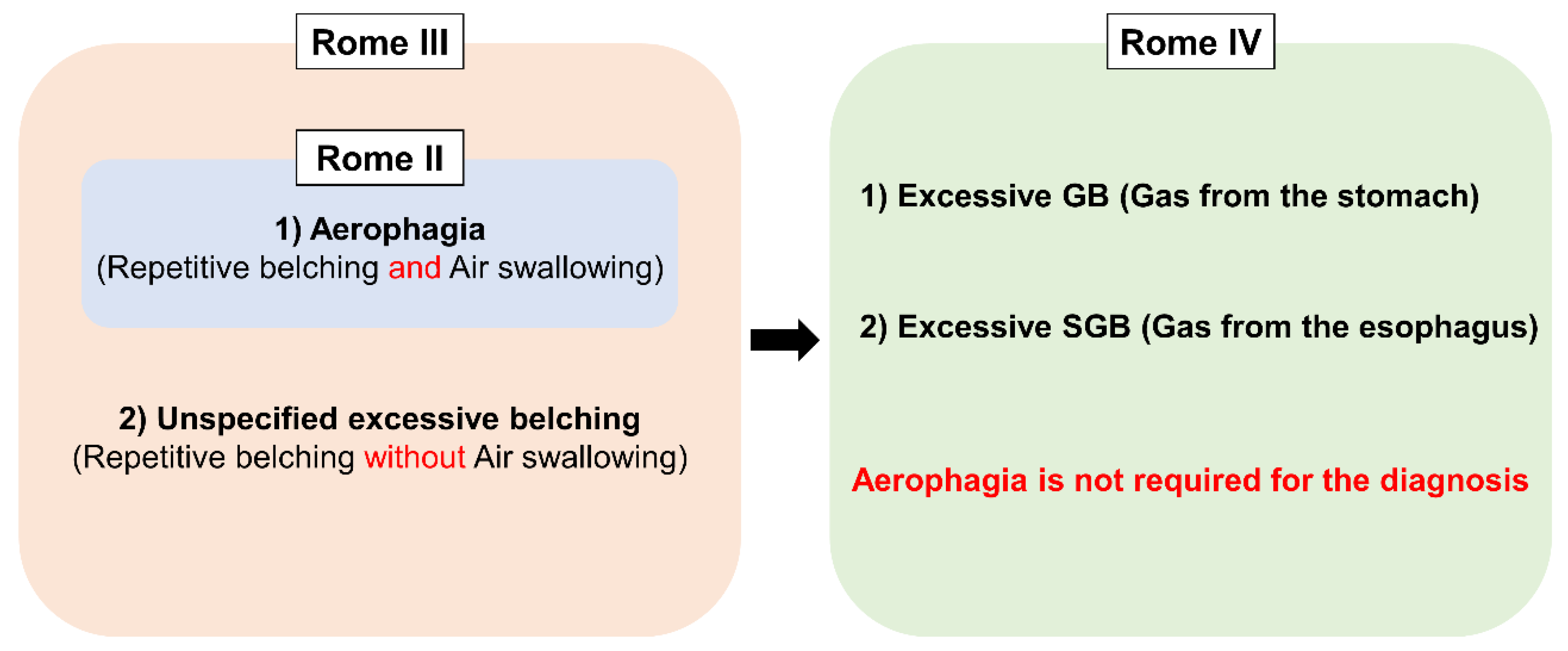
3. Conceptual Change of Belching Disorders and Aerophagia in Rome Diagnostic Criteria
4. Epidemiology
5. Belching and Gastroesophageal Reflux Disease
5.1. Gastric Belching (GB)
5.2. Supragastric Belching (SGB)
5.3. Impact of Supragastric Belching (SGB) on PPI-Refractory GERD
5.4. Belching after Anti-Reflux Surgery
5.4.1. Laparoscopic Fundoplication
5.4.2. Magnetic Sphincter Augmentation Device (LINX Reflux Management System)
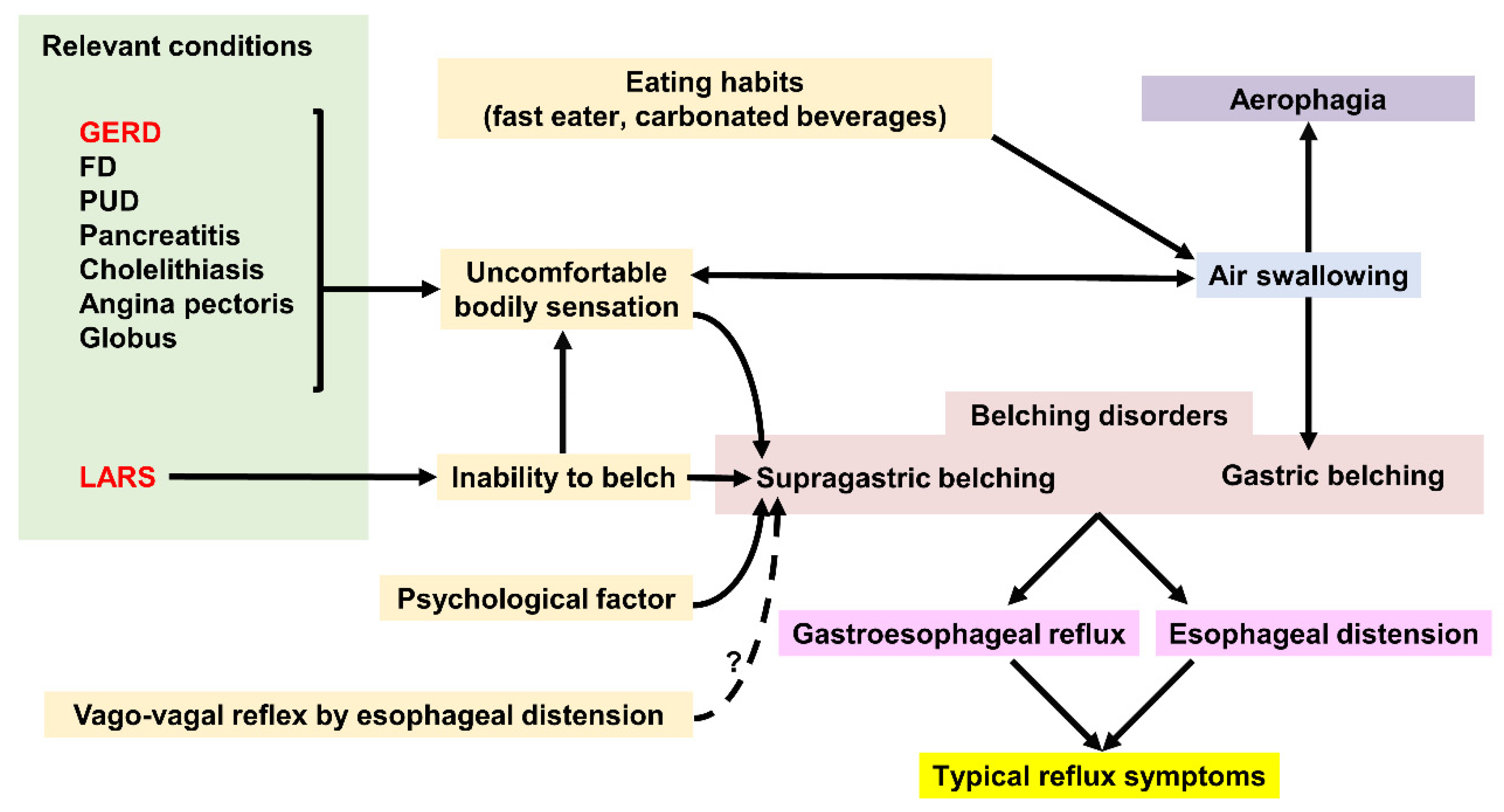
6. Belching and Other Relevant Conditions
6.1. Functional Dyspepsia
6.2. Globus
6.3. Bariatric Surgery (Sleeve Gastrectomy)
6.4. Miscellaneous Conditions
7. Clinical Approach and Treatment for Belching
7.1. Clinical Approach to Excessive Belching
7.2. Clinical Approach to Hidden SGB in PPI-Refractory GERD
7.3. Treatment for Gastric Belching
7.4. Treatment for Supragastric Belching
7.5. Treatment Implication for SGB With PPI-Refractory GERD
7.5.1. Excessive SGB with Severe Erosive Esophagitis or NERD
7.5.2. Excessive SGB with RH
7.5.3. Excessive SGB with FH
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Stanghellini, V.; Chan, F.K.; Hasler, W.L.; Malagelada, J.R.; Suzuki, H.; Tack, J.; Talley, N.J. Gastroduodenal Disorders. Gastroenterology 2016, 150, 1380–1392. [Google Scholar] [CrossRef] [PubMed]
- Sawada, A.; Guzman, M.; Nikaki, K.; Sonmez, S.; Yazaki, E.; Aziz, Q.; Woodland, P.; Rogers, B.; Gyawali, C.P.; Sifrim, D. Identification of Different Phenotypes of Esophageal Reflux Hypersensitivity and Implications for Treatment. Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Glasinovic, E.; Wynter, E.; Arguero, J.; Ooi, J.; Nakagawa, K.; Yazaki, E.; Hajek, P.; Psych, C.C.; Woodland, P.; Sifrim, D. Treatment of supragastric belching with cognitive behavioral therapy improves quality of life and reduces acid gastroesophageal reflux. Am. J. Gastroenterol. 2018, 113, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Bravi, I.; Woodland, P.; Gill, R.S.; Al-Zinaty, M.; Bredenoord, A.J.; Sifrim, D. Increased prandial air swallowing and postprandial gas-liquid reflux among patients refractory to proton pump inhibitor therapy. Clin. Gastroenterol. Hepatol. 2013, 11, 784–789. [Google Scholar] [CrossRef]
- Yadlapati, R.; Tye, M.; Roman, S.; Kahrilas, P.J.; Ritter, K.; Pandolfino, J.E. Postprandial High-Resolution Impedance Manometry Identifies Mechanisms of Nonresponse to Proton Pump Inhibitors. Clin. Gastroenterol. Hepatol. 2018, 16, 211–218. [Google Scholar] [CrossRef]
- Hemmink, G.J.; Bredenoord, A.J.; Weusten, B.L.; Timmer, R.; Smout, A.J. Supragastric belching in patients with reflux symptoms. Am. J. Gastroenterol. 2009, 104, 1992–1997. [Google Scholar] [CrossRef]
- Martin, C.J.; Patrikios, J.; Dent, J. Abolition of gas reflux and transient lower esophageal sphincter relaxation by vagal blockade in the dog. Gastroenterology 1986, 91, 890–896. [Google Scholar] [CrossRef]
- Mittal, R.K.; Balaban, D.H. The esophagogastric junction. N. Engl. J. Med. 1997, 336, 924–932. [Google Scholar] [CrossRef]
- Mittal, R.K. Regulation and dysregulation of esophageal peristalsis by the integrated function of circular and longitudinal muscle layers in health and disease. Am. J. Phys. Gastrointest. Liver Physiol. 2016, 311, G431–G443. [Google Scholar] [CrossRef] [Green Version]
- Kessing, B.F.; Bredenoord, A.J.; Smout, A.J. Mechanisms of gastric and supragastric belching: A study using concurrent high-resolution manometry and impedance monitoring. Neurogastroenterol. Motil. 2012, 24, 573–579. [Google Scholar] [CrossRef]
- Koukias, N.; Woodland, P.; Yazaki, E.; Sifrim, D. Supragastric Belching: Prevalence and Association With Gastroesophageal Reflux Disease and Esophageal Hypomotility. J. Neurogastroenterol. Motil. 2015, 21, 398–403. [Google Scholar] [CrossRef] [Green Version]
- Sawada, A.; Itami, H.; Nakagawa, K.; Hirano, S.; Kitamura, H.; Nakata, R.; Takashima, S.; Abe, Y.; Saito, M.; Yazaki, E.; et al. Supragastric belching in Japan: Lower prevalence and relevance for management of gastroesophageal reflux disease compared to United Kingdom. J. Gastroenterol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bredenoord, A.J.; Smout, A.J. Impaired health-related quality of life in patients with excessive supragastric belching. Eur. J. Gastroenterol. Hepatol. 2010, 22, 1420–1423. [Google Scholar] [CrossRef] [PubMed]
- Kessing, B.F.; Bredenoord, A.J.; Velosa, M.; Smout, A.J. Supragastric belches are the main determinants of troublesome belching symptoms in patients with gastro-oesophageal reflux disease. Aliment. Pharmacol. Ther. 2012, 35, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.M.; Medda, B.K.; Shaker, R. Characterization and mechanisms of the supragastric belch in the cat. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 313, G220–G229. [Google Scholar] [CrossRef]
- Bredenoord, A.J.; Weusten, B.L.; Timmer, R.; Smout, A.J. Psychological factors affect the frequency of belching in patients with aerophagia. Am. J. Gastroenterol. 2006, 101, 2777–2781. [Google Scholar] [CrossRef] [PubMed]
- Karamanolis, G.; Triantafyllou, K.; Tsiamoulos, Z.; Polymeros, D.; Kalli, T.; Misailidis, N.; Liakakos, T.; Ladas, S.D. Effect of sleep on excessive belching: A 24-hour impedance-pH study. J. Clin. Gastroenterol. 2010, 44, 332–334. [Google Scholar] [CrossRef]
- Talley, N.J.; Stanghellini, V.; Heading, R.C.; Koch, K.L.; Malagelada, J.R.; Tytgat, G.N. Functional gastroduodenal disorders. Gut 1999, 45, 37–42. [Google Scholar] [CrossRef]
- Fass, J.; Silny, J.; Braun, J.; Heindrichs, U.; Dreuw, B.; Schumpelick, V.; Rau, G. Measuring esophageal motility with a new intraluminal impedance device. First clinical results in reflux patients. Scand. J. Gastroenterol. 1994, 29, 693–702. [Google Scholar] [CrossRef]
- Sifrim, D.; Silny, J.; Holloway, R.H.; Janssens, J.J. Patterns of gas and liquid reflux during transient lower oesophageal sphincter relaxation: A study using intraluminal electrical impedance. Gut 1999, 44, 47–54. [Google Scholar] [CrossRef]
- Bredenoord, A.J.; Weusten, B.L.; Sifrim, D.; Timmer, R.; Smout, A.J. Aerophagia, gastric, and supragastric belching: A study using intraluminal electrical impedance monitoring. Gut 2004, 53, 1561–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tack, J.; Talley, N.J.; Camilleri, M.; Holtmann, G.; Hu, P.; Malagelada, J.R.; Stanghellini, V. Functional gastroduodenal disorders. Gastroenterology 2006, 130, 1466–1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bredenoord, A.J. Excessive belching and aerophagia: Two different disorders. Dis. Esophagus 2010, 23, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Hemmink, G.J.; Weusten, B.L.; Bredenoord, A.J.; Timmer, R.; Smout, A.J. Aerophagia: Excessive air swallowing demonstrated by esophageal impedance monitoring. Clin. Gastroenterol. Hepatol. 2009, 7, 1127–1129. [Google Scholar] [CrossRef] [PubMed]
- Westbrook, J.I.; Talley, N.J. Empiric clustering of dyspepsia into symptom subgroups: A population-based study. Scand. J. Gastroenterol. 2002, 37, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Bor, S.; Mandiracioglu, A.; Kitapcioglu, G.; Caymaz-Bor, C.; Gilbert, R.J. Gastroesophageal reflux disease in a low-income region in Turkey. Am. J. Gastroenterol. 2005, 100, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Rey, E.; Elola-Olaso, C.M.; Rodríguez-Artalejo, F.; Locke, G.R.; Díaz-Rubio, M. Prevalence of atypical symptoms and their association with typical symptoms of gastroesophageal reflux in Spain. Eur. J. Gastroenterol. Hepatol. 2006, 18, 969–975. [Google Scholar] [CrossRef]
- Li, Y.M.; Du, J.; Zhang, H.; Yu, C.H. Epidemiological investigation in outpatients with symptomatic gastroesophageal reflux from the Department of Medicine in Zhejiang Province, east China. J. Gastroenterol. Hepatol. 2008, 23, 283–289. [Google Scholar] [CrossRef]
- Klauser, A.G.; Schindlbeck, N.E.; Müller-Lissner, S.A. Symptoms in gastro-oesophageal reflux disease. Lancet 1990, 335, 205–208. [Google Scholar] [CrossRef]
- Dore, M.P.; Pedroni, A.; Pes, G.M.; Maragkoudakis, E.; Tadeu, V.; Pirina, P.; Realdi, G.; Delitala, G.; Malaty, H.M. Effect of antisecretory therapy on atypical symptoms in gastroesophageal reflux disease. Dig. Dis. Sci. 2007, 52, 463–468. [Google Scholar] [CrossRef]
- Yarandi, S.S.; Nasseri-Moghaddam, S.; Mostajabi, P.; Malekzadeh, R. Overlapping gastroesophageal reflux disease and irritable bowel syndrome: Increased dysfunctional symptoms. World J. Gastroenterol. 2010, 16, 1232–1238. [Google Scholar] [CrossRef]
- Ribolsi, M.; Cicala, M.; Zentilin, P.; Neri, M.; Mauro, A.; Efthymakis, K.; Petitti, T.; Savarino, V.; Penagini, R. Prevalence and clinical characteristics of refractoriness to optimal proton pump inhibitor therapy in non-erosive reflux disease. Aliment. Pharmacol. Ther. 2018, 48, 1074–1081. [Google Scholar] [CrossRef]
- Lin, M.; Triadafilopoulos, G. Belching: Dyspepsia or gastroesophageal reflux disease? Am. J. Gastroenterol. 2003, 98, 2139–2145. [Google Scholar] [CrossRef] [PubMed]
- Bredenoord, A.J.; Weusten, B.L.; Timmer, R.; Smout, A.J. Air swallowing, belching, and reflux in patients with gastroesophageal reflux disease. Am. J. Gastroenterol. 2006, 101, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Bredenoord, A.J.; Weusten, B.L.; Timmer, R.; Akkermans, L.M.; Smout, A.J. Relationships between air swallowing, intragastric air, belching and gastro-oesophageal reflux. Neurogastroenterol. Motil. 2005, 17, 341–347. [Google Scholar] [CrossRef]
- Sifrim, D.; Holloway, R.; Silny, J.; Tack, J.; Lerut, A.; Janssens, J. Composition of the postprandial refluxate in patients with gastroesophageal reflux disease. Am. J. Gastroenterol. 2001, 96, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Paterson, W.G.; Rattan, S.; Goyal, R.K. Experimental induction of isolated lower esophageal sphincter relaxation in anesthetized opossums. J. Clin. Investig. 1986, 77, 1187–1193. [Google Scholar] [CrossRef] [Green Version]
- Nikaki, K.; Sawada, A.; Ustaoglu, A.; Sifrim, D. Neuronal Control of Esophageal Peristalsis and Its Role in Esophageal Disease. Curr. Gastroenterol. Rep. 2019, 21, 59. [Google Scholar] [CrossRef] [Green Version]
- Pandolfino, J.E.; Ghosh, S.K.; Zhang, Q.; Han, A.; Kahrilas, P.J. Upper sphincter function during transient lower oesophageal sphincter relaxation (tLOSR); it is mainly about microburps. Neurogastroenterol. Motil. 2007, 19, 203–210. [Google Scholar] [CrossRef]
- Takeda, T.; Nabae, T.; Kassab, G.; Liu, J.; Mittal, R.K. Oesophageal wall stretch: The stimulus for distension induced oesophageal sensation. Neurogastroenterol. Motil. 2004, 16, 721–728. [Google Scholar] [CrossRef]
- Broeders, J.A.; Mauritz, F.A.; Ahmed Ali, U.; Draaisma, W.A.; Ruurda, J.P.; Gooszen, H.G.; Smout, A.J.; Broeders, I.A.; Hazebroek, E.J. Systematic review and meta-analysis of laparoscopic Nissen (posterior total) versus Toupet (posterior partial) fundoplication for gastro-oesophageal reflux disease. Br. J. Surg. 2010, 97, 1318–1330. [Google Scholar] [CrossRef] [PubMed]
- Catarci, M.; Gentileschi, P.; Papi, C.; Carrara, A.; Marrese, R.; Gaspari, A.L.; Grassi, G.B. Evidence-based appraisal of antireflux fundoplication. Ann. Surg. 2004, 239, 325–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varin, O.; Velstra, B.; De Sutter, S.; Ceelen, W. Total vs partial fundoplication in the treatment of gastroesophageal reflux disease: A meta-analysis. Arch. Surg. 2009, 144, 273–278. [Google Scholar] [CrossRef]
- Broeders, J.A.; Bredenoord, A.J.; Hazebroek, E.J.; Broeders, I.A.; Gooszen, H.G.; Smout, A.J. Effects of anti-reflux surgery on weakly acidic reflux and belching. Gut 2011, 60, 435–441. [Google Scholar] [CrossRef] [Green Version]
- Broeders, J.A.; Bredenoord, A.J.; Hazebroek, E.J.; Broeders, I.A.; Gooszen, H.G.; Smout, A.J. Reflux and belching after 270 degree versus 360 degree laparoscopic posterior fundoplication. Ann. Surg. 2012, 255, 59–65. [Google Scholar] [CrossRef]
- Oor, J.E.; Broeders, J.A.; Roks, D.J.; Oors, J.M.; Weusten, B.L.; Bredenoord, A.J.; Hazebroek, E.J. Reflux and Belching after Laparoscopic 270 degree Posterior Versus 180 degree Anterior Partial Fundoplication. J. Gastrointest. Surg. 2018, 22, 1852–1860. [Google Scholar] [CrossRef]
- Skubleny, D.; Switzer, N.J.; Dang, J.; Gill, R.S.; Shi, X.; de Gara, C.; Birch, D.W.; Wong, C.; Hutter, M.M.; Karmali, S. LINX. Surg. Endosc. 2017, 31, 3078–3084. [Google Scholar] [CrossRef]
- Aiolfi, A.; Asti, E.; Bernardi, D.; Bonitta, G.; Rausa, E.; Siboni, S.; Bonavina, L. Early results of magnetic sphincter augmentation versus fundoplication for gastroesophageal reflux disease: Systematic review and meta-analysis. Int. J. Surg. 2018, 52, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Bonavina, L.; DeMeester, T.; Fockens, P.; Dunn, D.; Saino, G.; Bona, D.; Lipham, J.; Bemelman, W.; Ganz, R.A. Laparoscopic sphincter augmentation device eliminates reflux symptoms and normalizes esophageal acid exposure: One- and 2-year results of a feasibility trial. Ann. Surg. 2010, 252, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Ganz, R.A.; Edmundowicz, S.A.; Taiganides, P.A.; Lipham, J.C.; Smith, C.D.; DeVault, K.R.; Horgan, S.; Jacobsen, G.; Luketich, J.D.; Smith, C.C.; et al. Long-term Outcomes of Patients Receiving a Magnetic Sphincter Augmentation Device for Gastroesophageal Reflux. Clin. Gastroenterol. Hepatol. 2016, 14, 671–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonavina, L.; Saino, G.; Bona, D.; Sironi, A.; Lazzari, V. One hundred consecutive patients treated with magnetic sphincter augmentation for gastroesophageal reflux disease: 6 years of clinical experience from a single center. J. Am. Coll. Surg. 2013, 217, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Piessevaux, H.; De Winter, B.; Louis, E.; Muls, V.; De Looze, D.; Pelckmans, P.; Deltenre, M.; Urbain, D.; Tack, J. Dyspeptic symptoms in the general population: A factor and cluster analysis of symptom groupings. Neurogastroenterol. Motil. 2009, 21, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Tack, J.; Caenepeel, P.; Fischler, B.; Piessevaux, H.; Janssens, J. Symptoms associated with hypersensitivity to gastric distention in functional dyspepsia. Gastroenterology 2001, 121, 526–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tack, J.; Caenepeel, P.; Arts, J.; Lee, K.J.; Sifrim, D.; Janssens, J. Prevalence of acid reflux in functional dyspepsia and its association with symptom profile. Gut 2005, 54, 1370–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conchillo, J.M.; Selimah, M.; Bredenoord, A.J.; Samsom, M.; Smout, A.J. Air swallowing, belching, acid and non-acid reflux in patients with functional dyspepsia. Aliment. Pharmacol. Ther. 2007, 25, 965–971. [Google Scholar] [CrossRef]
- Aziz, Q.; Fass, R.; Gyawali, C.P.; Miwa, H.; Pandolfino, J.E.; Zerbib, F. Functional Esophageal Disorders. Gastroenterology 2016. [Google Scholar] [CrossRef]
- Nevalainen, P.; Walamies, M.; Kruuna, O.; Arkkila, P.; Aaltonen, L.M. Supragastric belch may be related to globus symptom—A prospective clinical study. Neurogastroenterol. Motil. 2016, 28, 680–686. [Google Scholar] [CrossRef]
- Sawada, A.; Anastasi, N.; Green, A.; Glasinovic, E.; Wynter, E.; Albusoda, A.; Hajek, P.; Sifrim, D. Management of supragastric belching with cognitive behavioural therapy: Factors determining success and follow-up outcomes at 6-12 months post-therapy. Aliment. Pharmacol. Ther. 2019, 50, 530–537. [Google Scholar] [CrossRef]
- Burgerhart, J.S.; van de Meeberg, P.C.; Mauritz, F.A.; Schoon, E.J.; Smulders, J.F.; Siersema, P.D.; Smout, A.J. Increased Belching After Sleeve Gastrectomy. Obes. Surg. 2016, 26, 132–137. [Google Scholar] [CrossRef]
- Burgerhart, J.S.; Schotborgh, C.A.; Schoon, E.J.; Smulders, J.F.; van de Meeberg, P.C.; Siersema, P.D.; Smout, A.J. Effect of sleeve gastrectomy on gastroesophageal reflux. Obes. Surg. 2014, 24, 1436–1441. [Google Scholar] [CrossRef]
- Bredenoord, A.J. Management of belching, hiccups, and aerophagia. Clin. Gastroenterol. Hepatol. 2013, 11, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xiao, Y.; Peng, S.; Lin, J.; Chen, M. Characteristics of belching, swallowing, and gastroesophageal reflux in belching patients based on Rome III criteria. J. Gastroenterol. Hepatol. 2013, 28, 1282–1287. [Google Scholar] [CrossRef] [PubMed]
- Kahrilas, P.J.; Miner, P.; Johanson, J.; Mao, L.; Jokubaitis, L.; Sloan, S. Efficacy of rabeprazole in the treatment of symptomatic gastroesophageal reflux disease. Dig. Dis. Sci. 2005, 50, 2009–2018. [Google Scholar] [CrossRef] [PubMed]
- Miner, P.; Orr, W.; Filippone, J.; Jokubaitis, L.; Sloan, S. Rabeprazole in nonerosive gastroesophageal reflux disease: A randomized placebo-controlled trial. Am. J. Gastroenterol. 2002, 97, 1332–1339. [Google Scholar] [CrossRef] [PubMed]
- Gerson, L.B.; Kahrilas, P.J.; Fass, R. Insights into gastroesophageal reflux disease-associated dyspeptic symptoms. Clin. Gastroenterol. Hepatol. 2011, 9, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Kriengkirakul, C.; Patcharatrakul, T.; Gonlachanvit, S. The Therapeutic and Diagnostic Value of 2-week High Dose Proton Pump Inhibitor Treatment in Overlapping Non-erosive Gastroesophageal Reflux Disease and Functional Dyspepsia Patients. J. Neurogastroenterol. Motil. 2012, 18, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Cossentino, M.J.; Mann, K.; Armbruster, S.P.; Lake, J.M.; Maydonovitch, C.; Wong, R.K. Randomised clinical trial: The effect of baclofen in patients with gastro-oesophageal reflux—A randomised prospective study. Aliment. Pharmacol. Ther. 2012, 35, 1036–1044. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Lehmann, A.; Rigda, R.; Dent, J.; Holloway, R.H. Control of transient lower oesophageal sphincter relaxations and reflux by the GABA(B) agonist baclofen in patients with gastro-oesophageal reflux disease. Gut 2002, 50, 19–24. [Google Scholar] [CrossRef]
- Boeckxstaens, G.E.; Rydholm, H.; Lei, A.; Adler, J.; Ruth, M. Effect of lesogaberan, a novel GABA(B)-receptor agonist, on transient lower oesophageal sphincter relaxations in male subjects. Aliment. Pharmacol. Ther. 2010, 31, 1208–1217. [Google Scholar] [CrossRef] [Green Version]
- Tan, V.P.; Liu, K.S.; Lam, F.Y.; Hung, I.F.; Yuen, M.F.; Leung, W.K. Randomised clinical trial: Rifaximin versus placebo for the treatment of functional dyspepsia. Aliment. Pharmacol. Ther. 2017, 45, 767–776. [Google Scholar] [CrossRef] [Green Version]
- Porika, S.K.; Veligandla, K.C.; Muni, S.K.; Acharya, S.; Mehta, S.C.; Sharma, A.D. Real-World, Non-Interventional, Observational Study to Evaluate Effectiveness and Tolerability of Acotiamide Hydrochloride Hydrate in Treatment of Functional Dyspepsia. Adv. Ther. 2018, 35, 1884–1893. [Google Scholar] [CrossRef]
- Amini, M.; Ghamar Chehreh, M.E.; Khedmat, H.; Valizadegan, G.; Babaei, M.; Darvishi, A.; Taheri, S. Famotidine in the treatment of functional dyspepsia: A randomized double-blind, placebo-controlled trial. J. Egypt. Public Health Assoc. 2012, 87, 29–33. [Google Scholar] [CrossRef] [Green Version]
- Miwa, H.; Osada, T.; Nagahara, A.; Ohkusa, T.; Hojo, M.; Tomita, T.; Hori, K.; Matsumoto, T.; Sato, N. Effect of a gastro-protective agent, rebamipide, on symptom improvement in patients with functional dyspepsia: A double-blind placebo-controlled study in Japan. J. Gastroenterol. Hepatol. 2006, 21, 1826–1831. [Google Scholar] [CrossRef] [PubMed]
- Ong, A.M.; Chua, L.T.; Khor, C.J.; Asokkumar, R.; S/O Namasivayam, V.; Wang, Y.T. Diaphragmatic Breathing Reduces Belching and Proton Pump Inhibitor Refractory Gastroesophageal Reflux Symptoms. Clin. Gastroenterol. Hepatol. 2018, 16, 407–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzka, D.A. Simple office-based behavioral approach to patients with chronic belching. Dis. Esophagus 2013, 26, 570–573. [Google Scholar] [CrossRef]
- Hemmink, G.J.; Ten Cate, L.; Bredenoord, A.J.; Timmer, R.; Weusten, B.L.; Smout, A.J. Speech therapy in patients with excessive supragastric belching—A pilot study. Neurogastroenterol. Motil. 2010, 22, 24-e3. [Google Scholar] [CrossRef]
- Ten Cate, L.; Herregods, T.V.K.; Dejonckere, P.H.; Hemmink, G.J.M.; Smout, A.J.P.M.; Bredenoord, A.J. Speech Therapy as Treatment for Supragastric Belching. Dysphagia 2018, 33, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Kunte, H.; Kronenberg, G.; Fink, K.; Harms, L.; Hellweg, R. Successful treatment of excessive supragastric belching by combination of pregabalin and baclofen. Psychiatry Clin. Neurosci. 2015, 69, 124–125. [Google Scholar] [CrossRef] [Green Version]
- Blondeau, K.; Boecxstaens, V.; Rommel, N.; Farré, R.; Depeyper, S.; Holvoet, L.; Boeckxstaens, G.; Tack, J.F. Baclofen improves symptoms and reduces postprandial flow events in patients with rumination and supragastric belching. Clin. Gastroenterol. Hepatol. 2012, 10, 379–384. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Study Subjects | Number of People Surveyed (n) | Overall Prevalence of Belching | Prevalence of Belching Symptom without GERD | Prevalence of Belching Symptom with GERD | Definition of GERD |
|---|---|---|---|---|---|---|---|
| Westbrook et al. [25] | Australia | General population | 2300 | 6.7% | |||
| Bor et al. [26] | Turkey | General population | 630 | 15.9% | 11.5% (n = 393) | 23.2% (n = 237) | Heartburn and/or regurgitation |
| Rey et al. [27] | Spain | General population | 2500 | 20.5% | 12.6% (n = 1709) | 37.5% (n = 791) | Heartburn and/or regurgitation |
| Li et al. [28] | China | Outpatients | 15283 | 28.8% (n = 13282) | 26.3% (n = 12257) | 58.5% (n = 1025) | RDQ score > 12 |
| Kessing et al. [14] | Netherland | GERD | 90 | - | - | 75.6% | Reflux symptoms |
| Klauser et al. [29] | Germany | GERD | 304 | 44.7% | Esophageal symptom | ||
| Dore et al. [30] | Italy | GERD | 266 | - | - | 26.3% | Heartburn, regurgitation, dysphagia or odynophagia |
| Yarandi et al. [31] | Iran | GERD | 1522 | - | - | 4.1% | Heartburn, regurgitation and dysphagia |
| Ribolsi et al. [32] | Italy | GERD | 573 | - | - | 62.7% | Heartburn, regurgitation, or noncardiac chest pain |
| Lin et al. [33] | USA | GERD | 180 | 70% | Positive DeMeester score (>14.2), endoscopic esophagitis, or Barrett’s esophagus |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawada, A.; Fujiwara, Y.; Sifrim, D. Belching in Gastroesophageal Reflux Disease: Literature Review. J. Clin. Med. 2020, 9, 3360. https://doi.org/10.3390/jcm9103360
Sawada A, Fujiwara Y, Sifrim D. Belching in Gastroesophageal Reflux Disease: Literature Review. Journal of Clinical Medicine. 2020; 9(10):3360. https://doi.org/10.3390/jcm9103360
Chicago/Turabian StyleSawada, Akinari, Yasuhiro Fujiwara, and Daniel Sifrim. 2020. "Belching in Gastroesophageal Reflux Disease: Literature Review" Journal of Clinical Medicine 9, no. 10: 3360. https://doi.org/10.3390/jcm9103360
APA StyleSawada, A., Fujiwara, Y., & Sifrim, D. (2020). Belching in Gastroesophageal Reflux Disease: Literature Review. Journal of Clinical Medicine, 9(10), 3360. https://doi.org/10.3390/jcm9103360