The Impact of Preoperative Inflammatory Markers on the Prognosis of Patients Undergoing Surgical Resection of Pulmonary Oligometastases

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Inflammation Markers
2.3. Statistical Analysis
3. Results
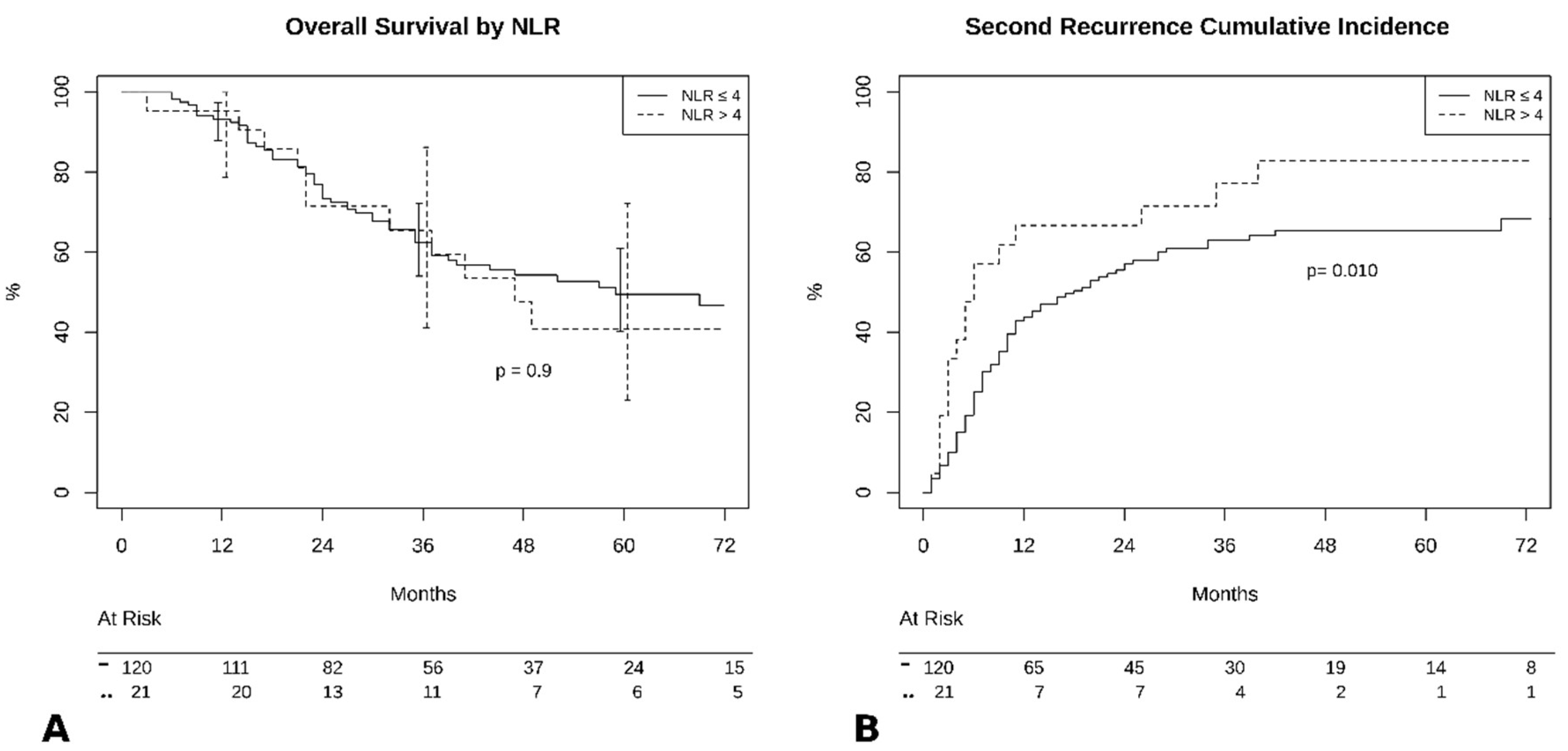
3.1. NLR
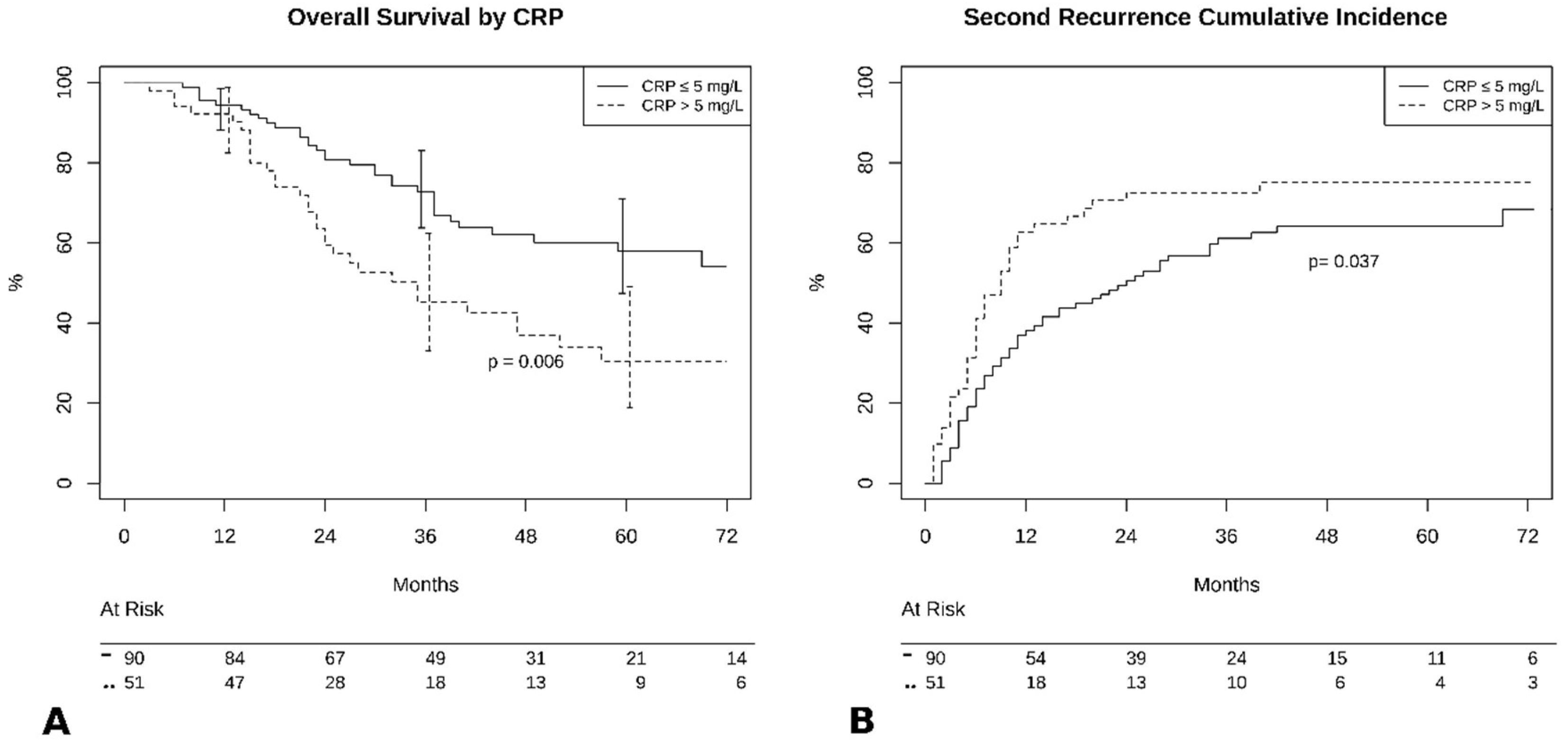
3.2. CRP
3.3. Predictors of Outcome
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Hellman, S.; Weichselbaum, R.R. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Rusch, V.W. Pulmonary Metastasectomy. Chest 1995, 107, 322S–331S. [Google Scholar] [CrossRef] [PubMed]
- Pastorino, U.; Buyse, M.; Friedel, G.; Ginsberg, R.J.; Girard, P.; Goldstraw, P.; Johnston, M.; McCormack, P.; Pass, H.; Putnam, J.B., Jr. Long-term results of lung metastasectomy: Prognostic analyses based on 5206 cases. J. Thorac. Cardiovasc. Surg. 1997, 113, 37–49. [Google Scholar] [CrossRef] [Green Version]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Cools-Lartigue, J.; Spicer, J.; Najmeh, S.; Ferri, L. Neutrophil extracellular traps in cancer progression. Cell Mol. Life Sci. 2014, 71, 4179–4194. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Nat. Cancer Instit. 2014, 106, dju124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanim, B.; Schweiger, T.; Jedamzik, J.; Glueck, O.; Glogner, C.; Lang, G.; Klepetko, W.; Hoetzenecker, K. Elevated inflammatory parameters and inflammation scores are associated with poor prognosis in patients undergoing pulmonary metastasectomy for colorectal cancer. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 616–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renaud, S.; Seitlinger, J.; St-Pierre, D.; Garfinkle, R.; Al Lawati, Y.; Guerrera, F.; Ruffini, E.; Falcoz, P.E.; Massard, G.; Ferri, L.; et al. Prognostic value of neutrophil to lymphocyte ratio in lung metastasectomy for colorectal cancer. Eur. J. Cardiothorac. Surg. 2019, 55, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Allin, K.H.; Nordestgaard, B.G. Elevated C-reactive protein in the diagnosis, prognosis, and cause of cancer. Crit. Rev. Clin. Lab. Sci. 2011, 48, 155–170. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [Green Version]
- Leitch, E.F.; Chakrabarti, M.; Crozier, J.E.; McKee, R.F.; Anderson, J.H.; Horgan, P.G.; McMillan, D.C. Comparison of the prognostic value of selected markers of the systemic inflammatory response in patients with colorectal cancer. Br. J. Cancer 2007, 97, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Demers, M.; Krause, D.S.; Schatzberg, D.; Martinod, K.; Voorhees, J.R.; Fuchs, T.A.; Scadden, D.T.; Wagner, D.D. Cancers predispose neutrophils to release extracellular DNA traps that contribute to cancer-associated thrombosis. Proc. Natl. Acad. Sci. USA 2012, 109, 13076–13081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acuff, H.B.; Carter, K.J.; Fingleton, B.; Gorden, D.L.; Matrisian, L.M. Matrix metalloproteinase-9 from bone marrow-derived cells contributes to survival but not growth of tumor cells in the lung microenvironment. Cancer Res. 2006, 66, 259–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, T.J.; Nannuru, K.C.; Futakuchi, M.; Singh, R.K. Cathepsin G-mediated enhanced TGF-beta signaling promotes angiogenesis via upregulation of VEGF and MCP-1. Cancer Lett. 2010, 288, 162–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, T.; Takahashi, S.; Mizumoto, T.; Harao, M.; Akizuki, M.; Takasugi, M.; Fukutomi, T.; Yamashita, J.-I. Neutrophil elastase and cancer. Surg. Oncol. 2006, 15, 217–222. [Google Scholar] [CrossRef]
- Pine, J.K.; Morris, E.; Hutchins, G.G.; West, N.P.; Jayne, D.G.; Quirke, P.; Prasad, K.R. Systemic neutrophil-to-lymphocyte ratio in colorectal cancer: The relationship to patient survival, tumour biology and local lymphocytic response to tumour. Br. J. Cancer 2015, 113, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Chua, W.; Charles, K.A.; Baracos, V.E.; Clarke, S.J. Neutrophil/lymphocyte ratio predicts chemotherapy outcomes in patients with advanced colorectal cancer. Br. J. Cancer 2011, 104, 1288–1295. [Google Scholar] [CrossRef] [Green Version]
- Cetin, B.; Berk, V.; Kaplan, M.A.; Afsar, B.; Tufan, G.; Ozkan, M.; Isikdogan, A.; Benekli, M.; Coskun, U.; Buyukberber, S. Is the pretreatment neutrophil to lymphocyte ratio an important prognostic parameter in patients with metastatic renal cell carcinoma? Clin. Genitourin. Cancer 2013, 11, 141–148. [Google Scholar] [CrossRef]
- Ding, P.-R.; An, X.; Zhang, R.-X.; Fang, Y.-J.; Li, L.-R.; Chen, G.; Wu, X.-J.; Lu, Z.-H.; Lin, J.-Z.; Kong, L.-H.; et al. Elevated preoperative neutrophil to lymphocyte ratio predicts risk of recurrence following curative resection for stage IIA colon cancer. Int. J. Colorectal Dis. 2010, 25, 1427–1433. [Google Scholar] [CrossRef]
- Pastorino, U.; Morelli, D.; Leuzzi, G.; Rolli, L.; Suatoni, P.; Taverna, F.; Bertocchi, E.; Boeri, M.; Sozzi, G.; Cantarutti, A.; et al. Baseline and Postoperative C-reactive Protein Levels Predict Long-Term Survival After Lung Metastasectomy. Ann. Surg. Oncol. 2019, 26, 869–875. [Google Scholar] [CrossRef]
- Marnell, L.; Mold, C.; Du Clos, T.W. C-reactive protein: Ligands, receptors and role in inflammation. Clin. Immunol. 2005, 117, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Pathak, A.; Agrawal, A. Evolution of C-Reactive Protein. Front. Immunol. 2019, 10, 943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Potempa, L.A.; El Kebir, D.; Filep, J.G. C-reactive protein and inflammation: Conformational changes affect function. Biol. Chem. 2015, 396, 1181–1197. [Google Scholar] [CrossRef]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef]
- Køstner, A.H.; Kersten, C.; Löwenmark, T.; Ydsten, K.A.; Peltonen, R.; Isoniemi, H.; Haglund, C.; Gunnarsson, U.; Isaksson, B. The prognostic role of systemic inflammation in patients undergoing resection of colorectal liver metastases: C-reactive protein (CRP) is a strong negative prognostic biomarker. J. Surg. Oncol. 2016, 114, 895–899. [Google Scholar] [CrossRef]
- Su, B.; Liu, T.; Fan, H.; Chen, F.; Ding, H.; Wu, Z.; Wang, H.; Hou, S. Inflammatory Markers and the Risk of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0150586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, S.; Zhou, C.; Kalionis, B.; Shuang, X.; Ge, H.; Gao, W. Combined Antioxidant, Anti-inflammaging and Mesenchymal Stem Cell Treatment: A Possible Therapeutic Direction in Elderly Patients with Chronic Obstructive Pulmonary Disease. Aging Dis. 2020, 11, 129–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaitkus, M.; Lavinskiene, S.; Barkauskiene, D.; Bieksiene, K.; Jeroch, J.; Sakalauskas, R. Reactive oxygen species in peripheral blood and sputum neutrophils during bacterial and nonbacterial acute exacerbation of chronic obstructive pulmonary disease. Inflammation 2013, 36, 1485–1493. [Google Scholar] [CrossRef]
- Hou, Z.; Zhang, H.; Gui, L.; Wang, W.; Zhao, S. Video-assisted thoracoscopic surgery versus open resection of lung metastases from colorectal cancer. Int. J. Clin. Exp. Med. 2015, 8, 13571–13577. [Google Scholar]
- Kim, J.Y.; Park, I.J.; Kim, H.R.; Kim, D.K.; Lee, J.L.; Yoon, Y.S.; Kim, C.W.; Lim, S.-B.; Lee, J.B.; Yu, C.S.; et al. Post-pulmonary metastasectomy prognosis after curative resection for colorectal cancer. Oncotarget 2017, 8, 36566–36577. [Google Scholar] [CrossRef]
- Robert, J.H.; Ambrogi, V.; Mermillod, B.; Dahabreh, D.; Goldstraw, P. Factors influencing long-term survival after lung metastasectomy. Ann. Thorac. Surg. 1997, 63, 777–784. [Google Scholar] [CrossRef]
- Veronesi, G.; Petrella, F.; Leo, F.; Solli, P.; Maissoneuve, P.; Galetta, D.; Gasparri, R.; Pelosi, G.; De Pas, T.; Spaggiari, L. Prognostic role of lymph node involvement in lung metastasectomy. J. Thorac. Cardiovasc. Surg. 2007, 133, 967–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Population | All 141 (100) | NLR < 4 121 (85.8) | NLR ≥ 4 20 (14.2) | p | CRP < 5 90 (63.8) | CRP ≥ 5 51 (36.2) | p |
|---|---|---|---|---|---|---|---|
| Gender: Male | 80 (56.7) | 68 (56.2) | 12 (60) | 0.81 | 42 (46.7) | 38 (74.5) | 0.002 |
| Age at Surgery | 66 (IQR 59–71) | 67 (IQR 59–70) | 64.5 (IQR 59–73) | >0.99 | 67 (IQR 59–72) | 64 (IQR 59–69) | 0.26 |
| ASA: | |||||||
| 2 | 94 (66.7) | 82 (67.8) | 12 (60) | 0.60 | 61 (67.8) | 33 (64.7) | 0.71 |
| 3 | 47 (32.9) | 39 (32.2) | 8 (40) | 29 (32.2) | 18 (35.3) | ||
| Comorbidities | |||||||
| Coronaropathy | 9 (6.3) | 8 (6.6) | 1 (5) | >0.99 | 6 (6.7) | 3 (5.9) | >0.99 |
| Arrhythmia | 8 (5.7) | 7 (5.8) | 1 (5) | >0.99 | 3 (3.3) | 5 (9.8) | 0.14 |
| Hypertension | 52 (36.9) | 43 (35.5) | 9 (45) | 0.45 | 29 (32.2) | 23 (45.1) | 0.15 |
| Previous Cancer | 34 (24.1) | 28 (23.1) | 6 (30) | 0.57 | 17 (18.9) | 17 (33.3) | 0.07 |
| Lung Disease | 17 (12.1) | 15 (12.4) | 2 (10) | >0.99 | 10 (11.1) | 7 (13.7) | 0.78 |
| Diabetes | 14 (9.9) | 11 (9.1) | 3 (15) | 0.42 | 6 (6.7) | 8 (15.7) | 0.14 |
| Chronic Renal Failure | 3 (2.1) | 2 (1.6) | 1 (5) | 0.37 | 2 (2.2) | 1 (2) | >0.99 |
| Liver Disease | 6 (4.3) | 6 (4.9) | 0 | 0.59 | 4 (4.4) | 2 (3.9) | >0.99 |
| Other | 31 (22.0) | 27 (22) | 4 (20) | >0.99 | 20 (22.2) | 11 (21.6) | >0.99 |
| Primary tumor | |||||||
| Colon-Rectum | 57 (40.4) | 51 (42.5) | 6 (30) | 0.33 | 36 (40) | 21 (41.2) | >0.99 |
| Melanoma | 12 (8.5) | 12 (9.9) | 0 | 0.21 | 6 (6.7) | 6 (11.8) | 0.35 |
| Uterus | 4 (2.8) | 3 (2.5) | 1 (5) | 0.46 | 4 (4.4) | 0 | 0.30 |
| Breast | 6 (4.3) | 4 (3.3) | 2 (10) | 0.20 | 5 (5.6) | 1 (2) | 0.41 |
| Head-Neck | 6 (4.3) | 6 (4.9) | 0 | 0.59 | 4 (4.4) | 2 (3.9) | >0.99 |
| NSCLC | 12 (8.5) | 9 (7.4) | 3 (15) | 0.37 | 5 (5.6) | 7 (13.7) | 0.12 |
| Kidney | 16 (11.3) | 14 (11.6) | 2 (10) | >0.99 | 11 (12.2) | 5 (9.8) | 0.78 |
| Sarcoma | 14 (9.9) | 10 (8.3) | 4 (20) | 0.11 | 10 (11.1) | 4 (7.8) | 0.77 |
| Other | 14 (9.9) | 12 (9.9) | 2 (10) | >0.99 | 9 (10) | 5 (9.8) | >0.99 |
| RT/CHT | |||||||
| Neoadjuvant | 21 (14.9) | 20 (16.5) | 1 (5) | 0.30 | 13 (14.4) | 8 (15.7) | >0.99 |
| Adjuvant | 88 (62.4) | 77 (63.6) | 11 (55) | 0.47 | 62 (68.9) | 26 (51) | 0.05 |
| Metastases | |||||||
| Synchronous | 14 (9.9) | 14 (11.6) | 0 | 0.22 | 11 (12.2) | 3 (5.9) | 0.38 |
| Size (mm) | 14 (IQR 10–25) | 13 (IQR 10–25) | 16 (IQR 10–30) | 0.24 | 13 (IQR 10–25) | 16 (IQR 10–30) | 0.24 |
| Number of Lesions | |||||||
| 1 | 105 (74.5) | 69 (76.7) | 36 (70.6) | 0.65 | 69 (76.7) | 36 (70.6) | 0.65 |
| 2 | 24 (17) | 12 (13.3) | 12 (23.5) | 12 (13.3) | 12 (23.5) | ||
| ≥3 | 12 (8.5) | 9 (10) | 3 (5.9) | 9 (10) | 3 (5.9) | ||
| Bilateral Nodules | 16 (11.3) | 11 (9.1) | 5 (25) | 0.053 | 11 (12.2) | 5 (9.8) | 0.79 |
| DFI (Months) | 30 (IQR 17–56) | 29 (IQR 16–49) | 46 (IQR 22–121) | 0.07 | 32.5 (IQR 18–61) | 23 (IQR 14–49) | 0.24 |
| Population | All 141 (100) | NLR < 4 121 (85.8) | NLR ≥ 4 20 (14.2) | p | CRP < 5 90 (63.8) | CRP ≥ 5 51 (36.2) | p |
|---|---|---|---|---|---|---|---|
| Resection | |||||||
| Tumorectomy | 3 (2.1) | 3 (2.5) | 0 | >0.99 | 1 (1.1) | 2 (3.9) | 0.29 |
| Wedge Resection | 88 (62.4) | 76 (62.8) | 12 (60) | 0.46 | 65 (72.2) | 28 (54.9) | 0.04 |
| Segmentectomy | 10 (7.1) | 9 (7.4) | 1 (5) | >0.99 | 6 (6.7) | 4 (7.8) | >0.99 |
| Lobectomy/bilobectomy | 40 (28.4) | 33 (27.3) | 7 (35) | 0.79 | 20 (22.2) | 20 (39.2) | 0.03 |
| Approach | |||||||
| VATS | 78 (55.3) | 72 (59.5) | 6 (30) | 0.016 | 57 (63.3) | 21 (41.2) | 0.01 |
| Time of Surgery (min) | 125 (IQR 85–190) | 120 (IQR 80–190) | 142 (IQR 117.5–182.5) | 0.20 | 120 (IQR 80–170) | 140 (IQR 95–205) | 0.21 |
| Post-Resection Status | |||||||
| R0 | 135 (95.7) | 115 (95.1) | 20 (100) | 0.59 | 86 (95.6) | 49 (96.1) | >0.99 |
| Population | All 141 (100) | NLR < 4 121 (85.8) | NLR ≥ 4 20 (14.2) | p | CRP < 5 90 (63.8) | CRP ≥ 5 51 (36.2) | p |
|---|---|---|---|---|---|---|---|
| Length of Stay (days) | 5 (IQR 3–7) | 5 (IQR 3–7) | 5.5 (IQR 4–8) | 0.19 | 5 (IQR 3–8) | 5 (IQR 4–7) | 0.57 |
| Complications | |||||||
| Total | 17 (12.6) | 13 (10.7) | 4 (20) | 0.26 | 9 (10) | 8 (15.7) | 0.42 |
| Hemorrhage | 2 (1.4) | 2 (1.6) | 0 | >0.99 | 2 (2.2) | 0 | 0.53 |
| Persistent Air-Leak | 6 (4.3) | 5 (4.1) | 1 (5) | >0.99 | 4 (4.4) | 2 (3.9) | >0.99 |
| Arrhythmia | 3 (2.1) | 1 (0.8) | 2 (10) | 0.053 | 2 (2.2) | 1 (2) | >0.99 |
| ARDS | 1 (0.7) | 0 | 1 (5) | 0.14 | 0 | 1 (2) | 0.36 |
| Pneumonia | 4 (2.8) | 3 (2.5) | 1 (5) | 0.46 | 2 (2.2) | 2 (3.9) | 0.62 |
| Other | 7 (4.9) | 6 (5) | 1 (5) | >0.99 | 3 (3.3) | 4 (7.8) | 0.25 |
| Survival | Recurrence | ||||
|---|---|---|---|---|---|
| HR | CI | SHR | CI | ||
| Preop Neutrophils | 1.113 | 1.030–1.227 | Preop CRP | 1.015 | 1.008–1.022 |
| NLR | 1.893 | 0.846–4.327 | Age | 0.985 | 0.972–1.843 |
| Lung Comorbidity | 2.127 | 1.117–4.051 | Lung Comorbidity | 2.448 | 1.425–4.206 |
| Post-Op Pneumonia | 2.869 | 0.953–8.639 | N of Metastasis | 1.303 | 1.092–1.554 |
| Other Complications | 2.232 | 0.897–5.552 | Year of Surgery | 0.901 | 0.70–3.753 |
| Year of Surgery | 0.847 | 0.632–4.129 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Londero, F.; Grossi, W.; Parise, O.; Cinel, J.; Parise, G.; Masullo, G.; Tetta, C.; Micali, L.R.; Mauro, E.; Morelli, A.; et al. The Impact of Preoperative Inflammatory Markers on the Prognosis of Patients Undergoing Surgical Resection of Pulmonary Oligometastases. J. Clin. Med. 2020, 9, 3378. https://doi.org/10.3390/jcm9103378
Londero F, Grossi W, Parise O, Cinel J, Parise G, Masullo G, Tetta C, Micali LR, Mauro E, Morelli A, et al. The Impact of Preoperative Inflammatory Markers on the Prognosis of Patients Undergoing Surgical Resection of Pulmonary Oligometastases. Journal of Clinical Medicine. 2020; 9(10):3378. https://doi.org/10.3390/jcm9103378
Chicago/Turabian StyleLondero, Francesco, William Grossi, Orlando Parise, Jacqueline Cinel, Gianmarco Parise, Gianluca Masullo, Cecilia Tetta, Linda Renata Micali, Emanuela Mauro, Angelo Morelli, and et al. 2020. "The Impact of Preoperative Inflammatory Markers on the Prognosis of Patients Undergoing Surgical Resection of Pulmonary Oligometastases" Journal of Clinical Medicine 9, no. 10: 3378. https://doi.org/10.3390/jcm9103378
APA StyleLondero, F., Grossi, W., Parise, O., Cinel, J., Parise, G., Masullo, G., Tetta, C., Micali, L. R., Mauro, E., Morelli, A., Maessen, J. G., & Gelsomino, S. (2020). The Impact of Preoperative Inflammatory Markers on the Prognosis of Patients Undergoing Surgical Resection of Pulmonary Oligometastases. Journal of Clinical Medicine, 9(10), 3378. https://doi.org/10.3390/jcm9103378