Chorioretinal Side Effects of Therapeutic Ocular Irradiation: A Multimodal Imaging Approach




Abstract
:1. Introduction
1.1. Uveal Melanoma and Radiotherapy
1.2. Main Imaging Tools in Ocular Oncology
2. Materials and Methods
3. Results
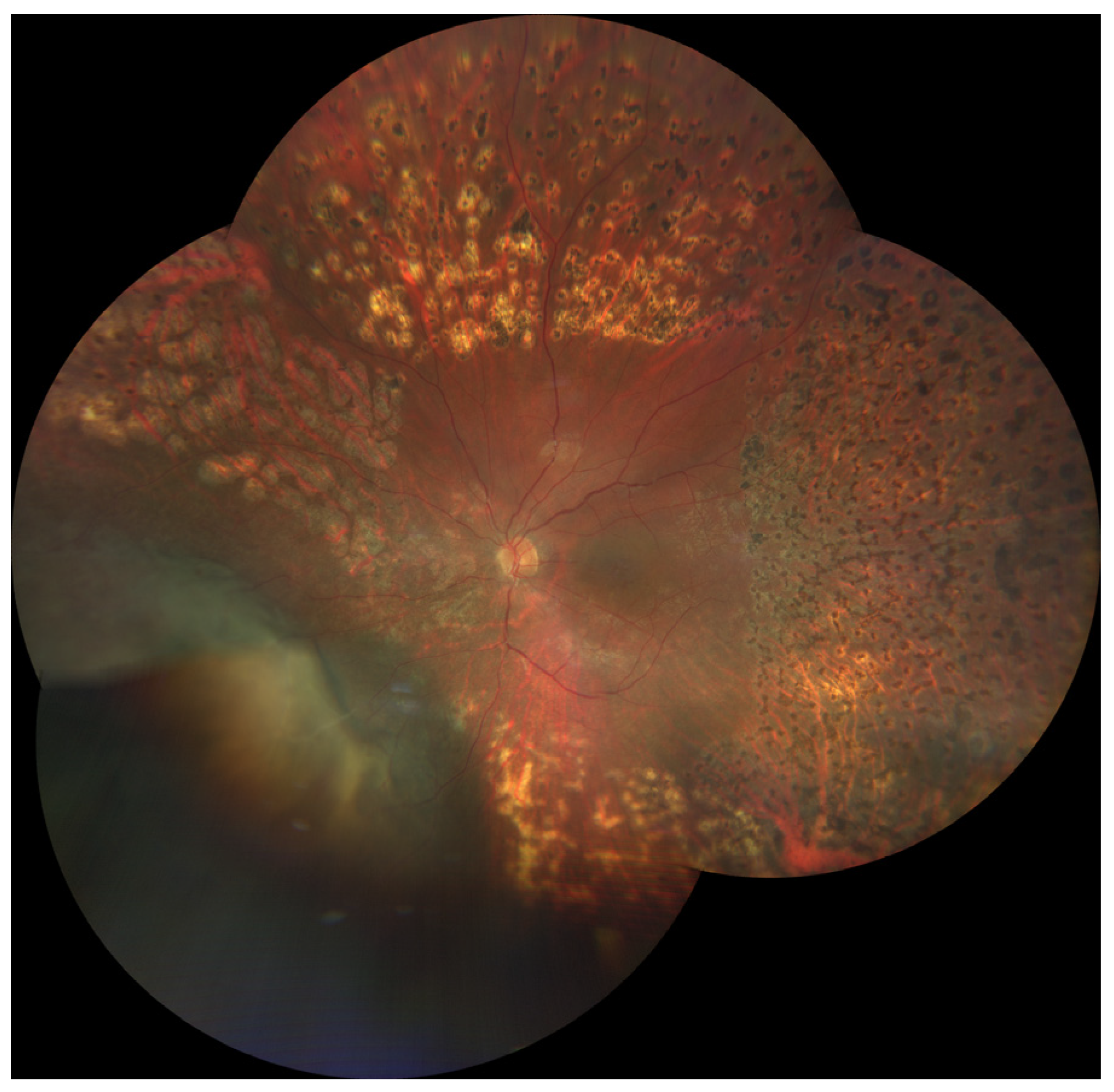
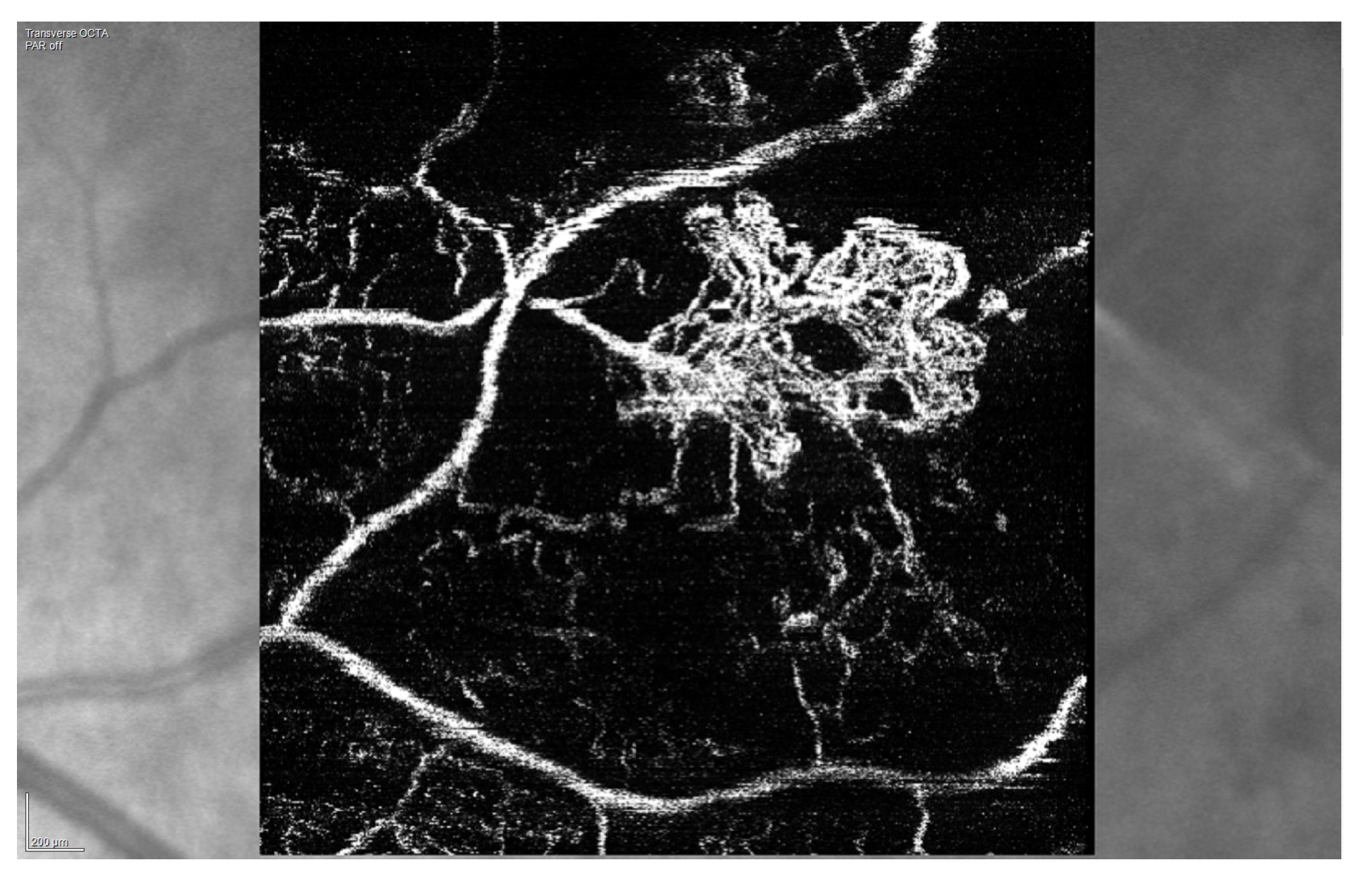
3.1. Radiation (Chorio)Retinopathy
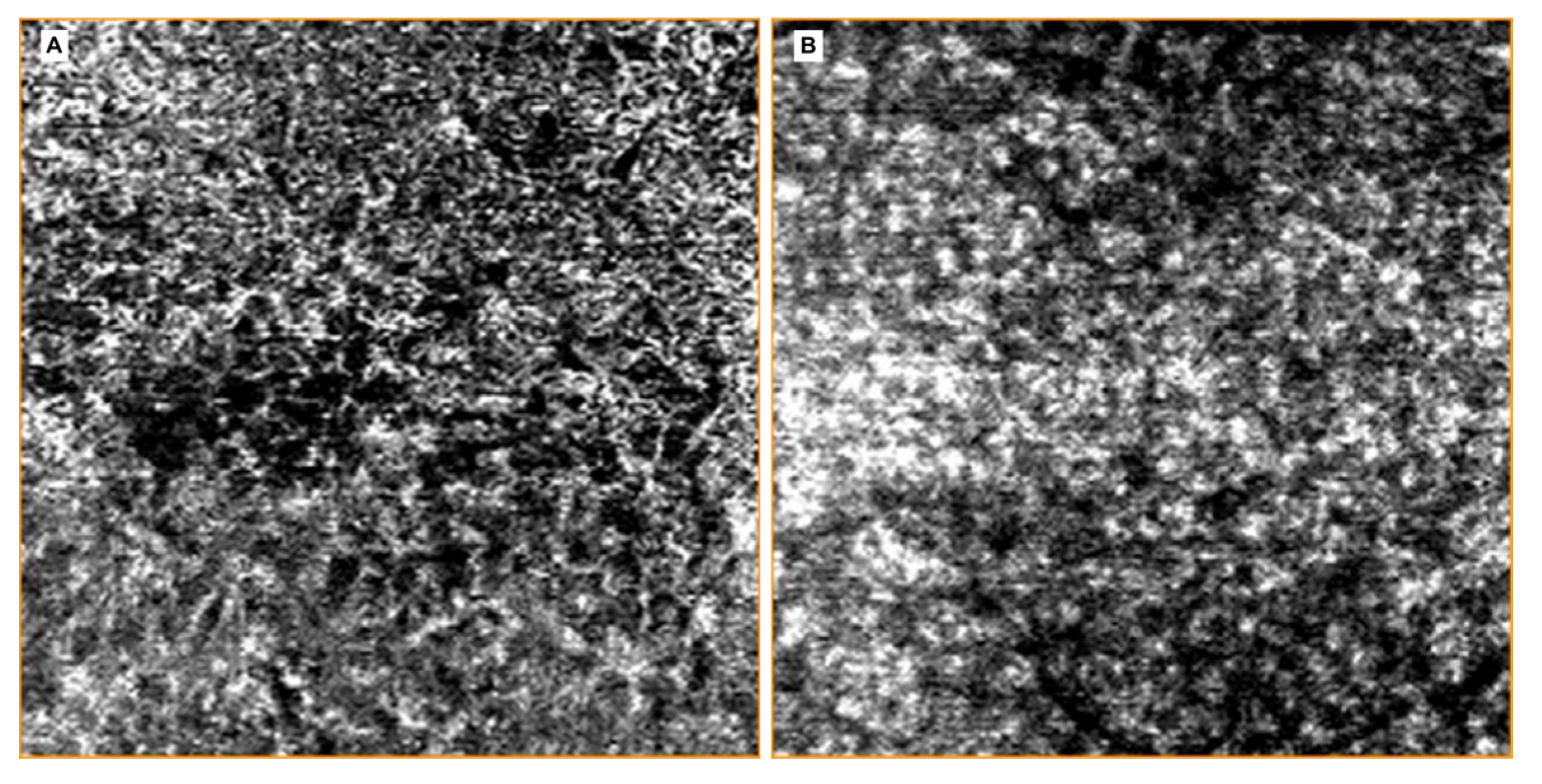
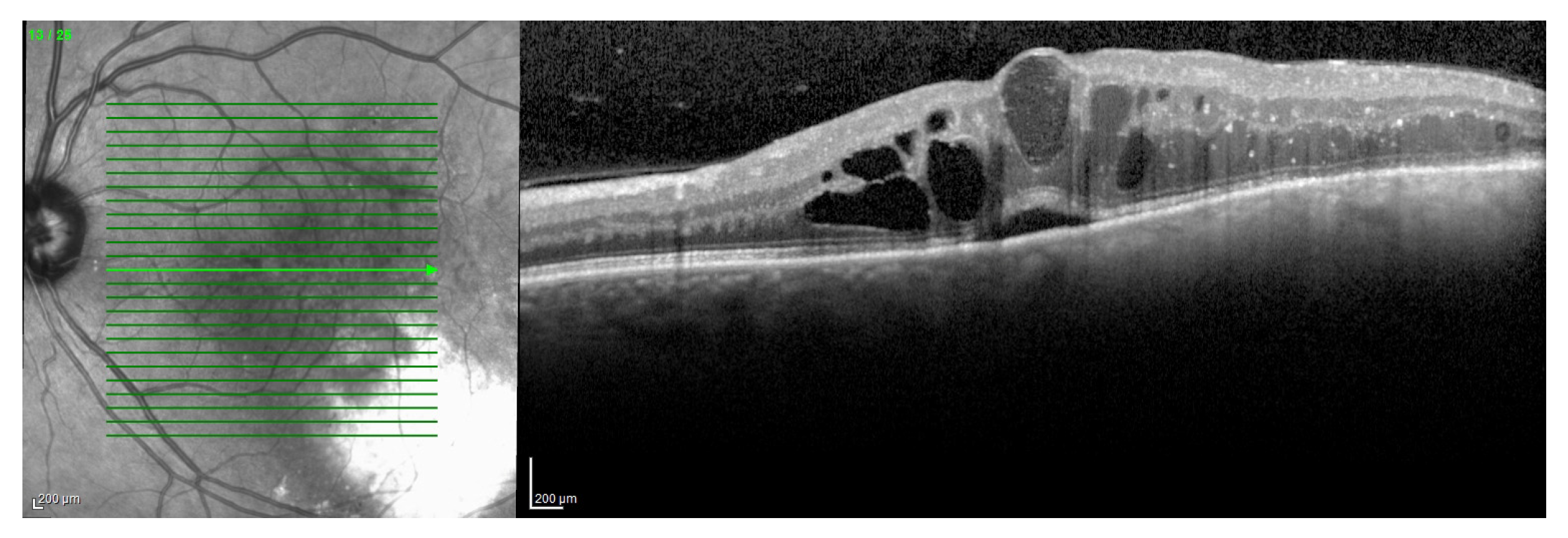
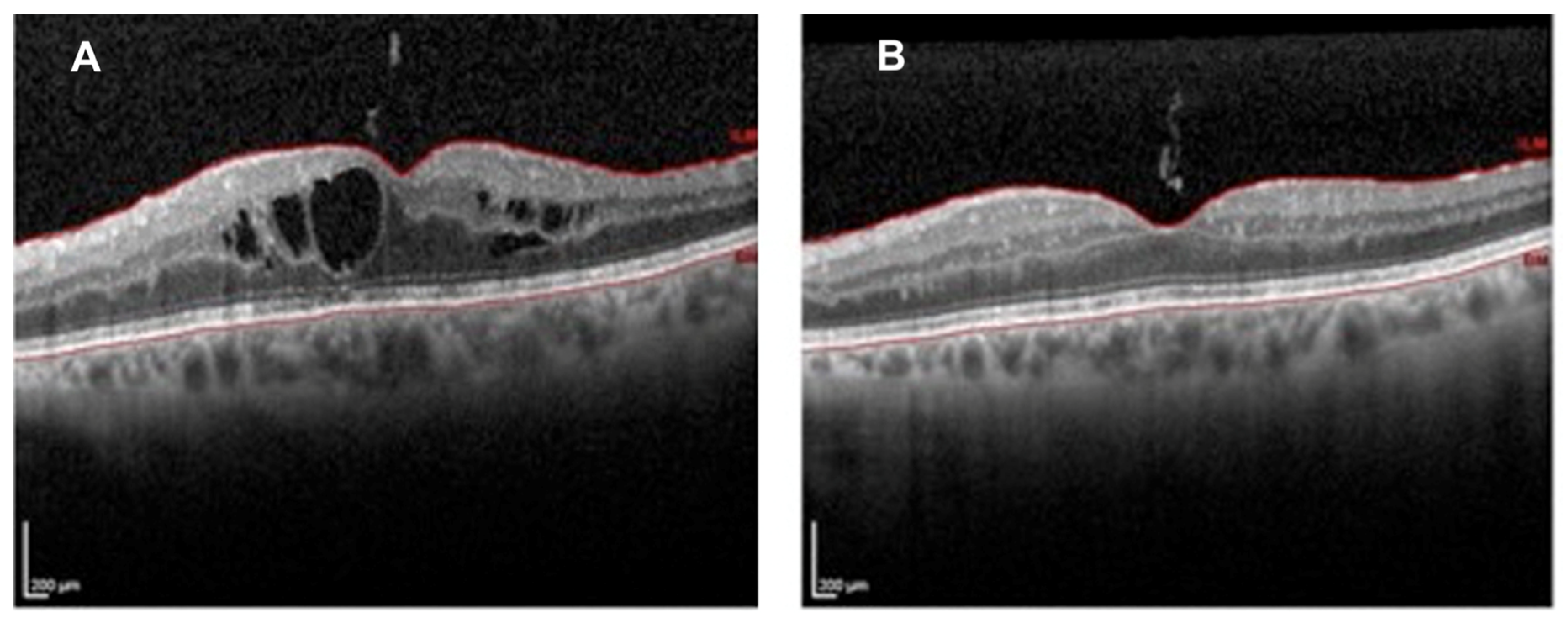
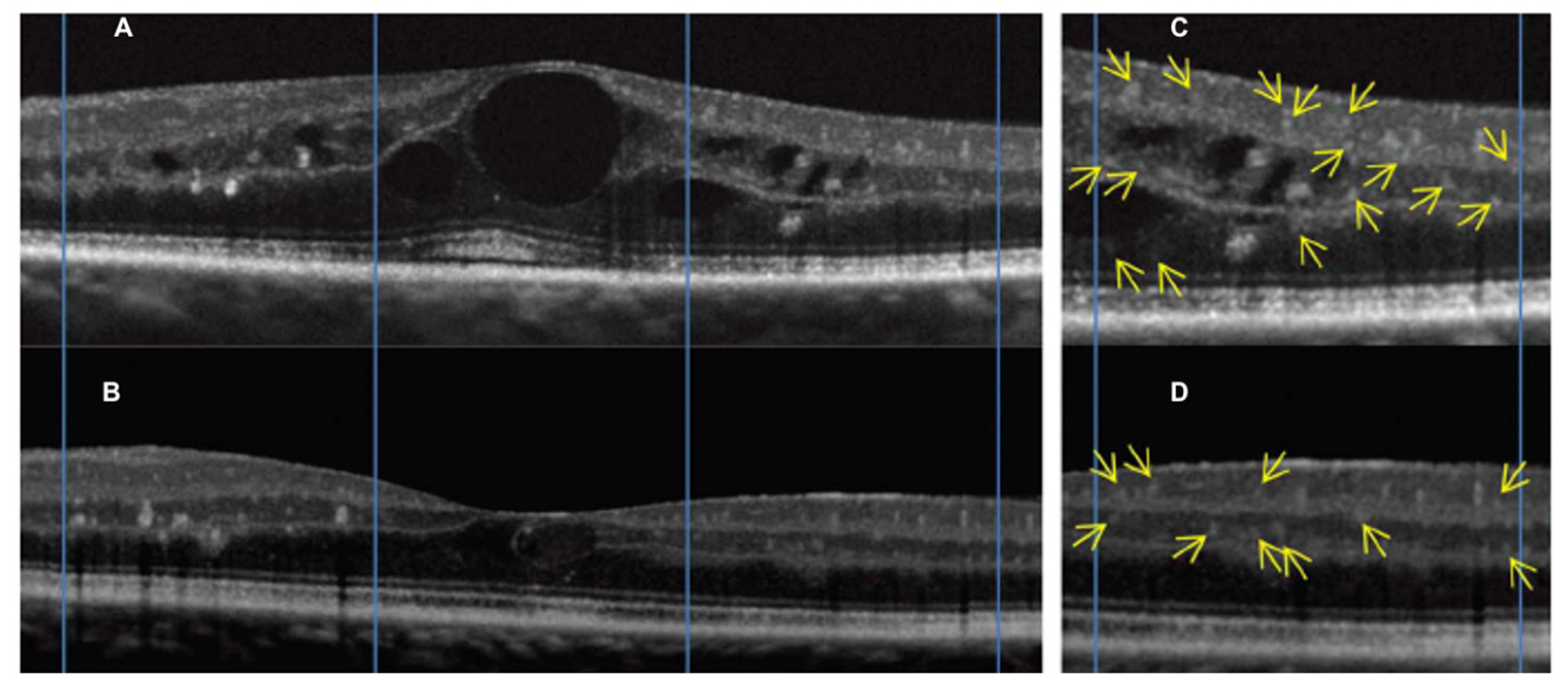
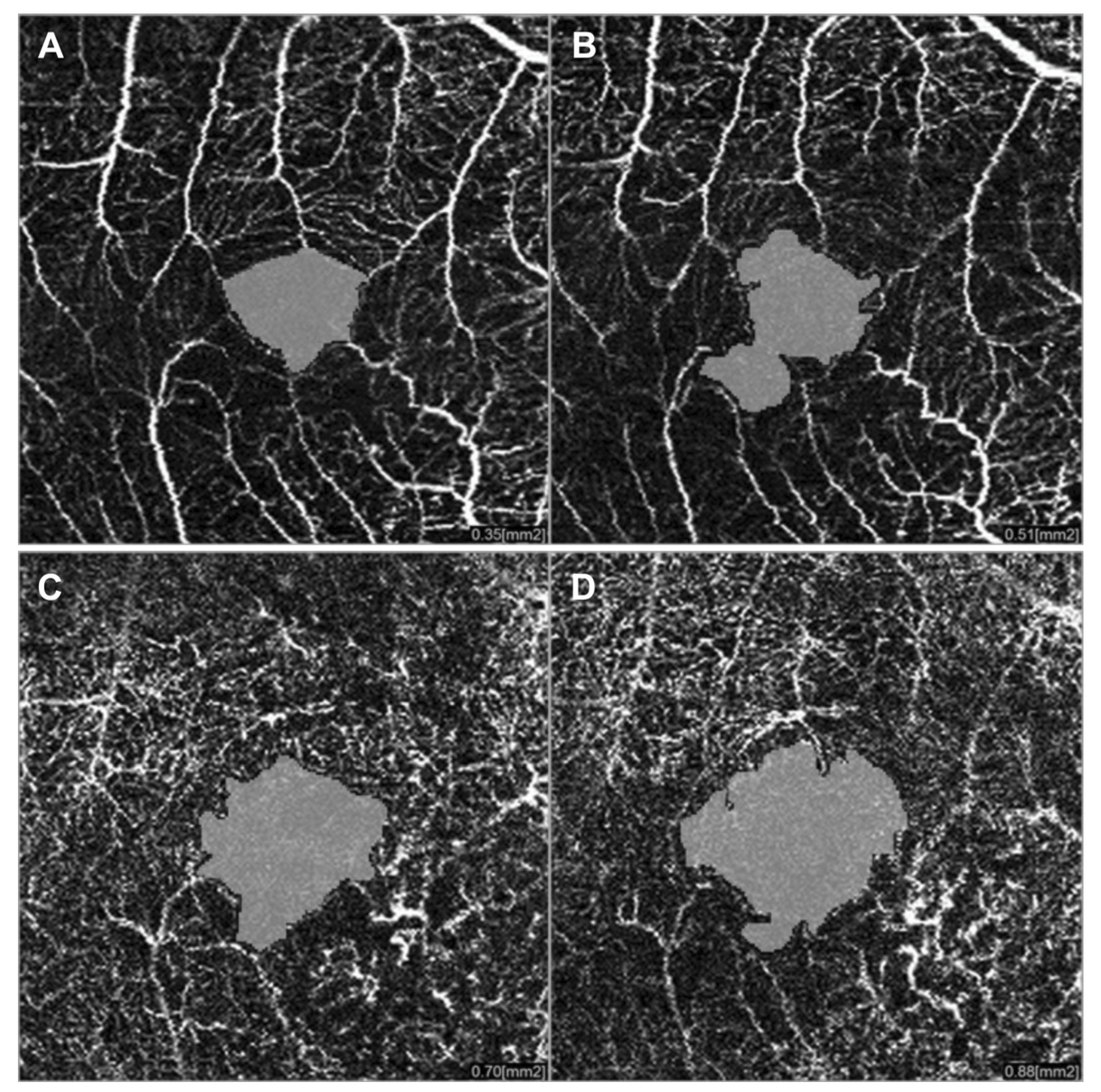
3.2. Radiation Maculopathy
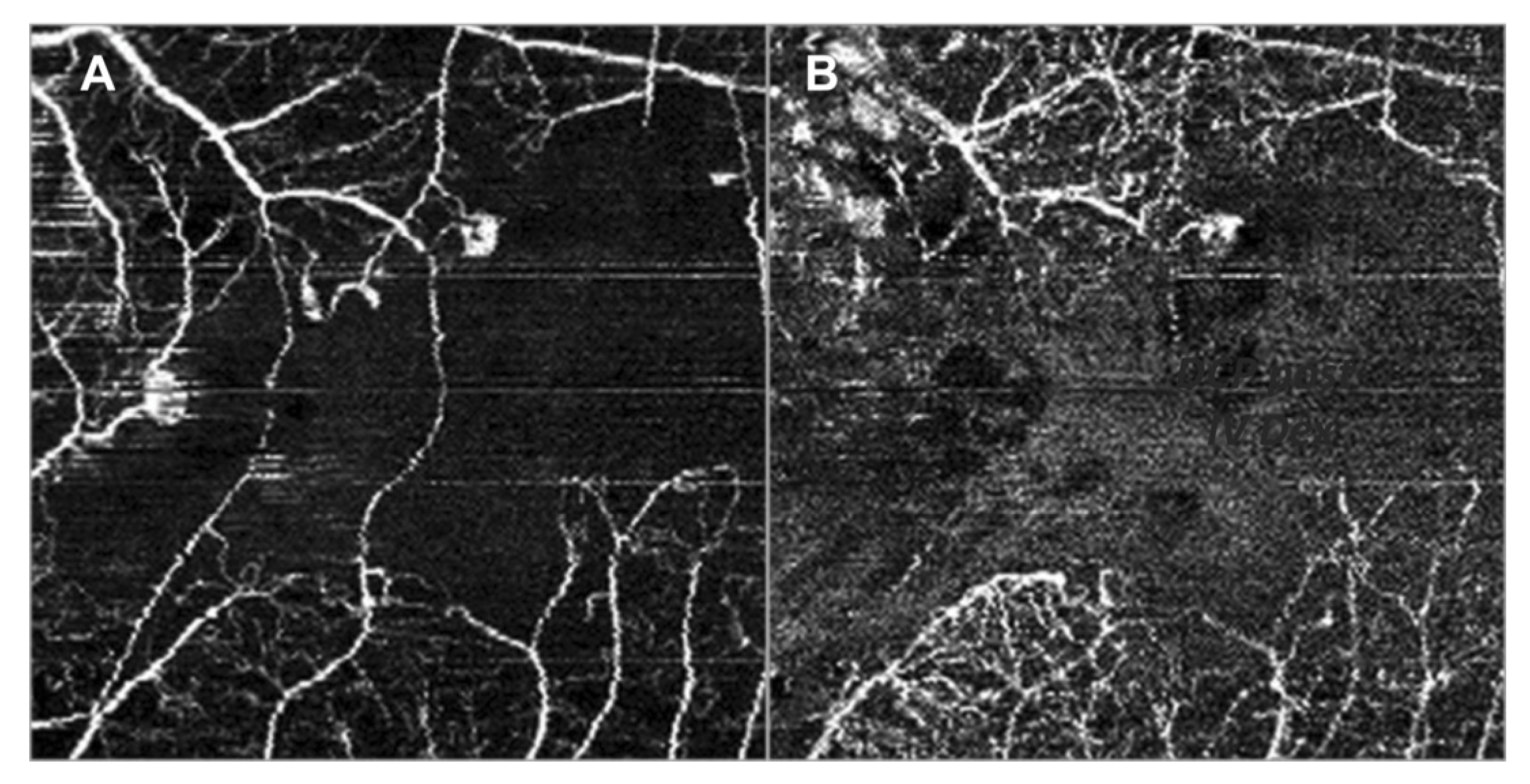
3.3. Radiation Optic Neuropathy
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, J.; Xu, Y.; Boppart, S.A. Review of optical coherence tomography in oncology. J. Biomed. Opt. 2017, 22, 121711. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, B.S. Collaborative Ocular Melanoma Study randomized trial of I-125 brachytherapy. Clin. Trials 2011, 8, 661–673. [Google Scholar] [CrossRef] [PubMed]
- Melia, B.M.; Abramson, D.H.; Albert, D.M.; Boldt, H.C.; Earle, J.D.; Hanson, W.F.; Montague, P.; Moy, C.S.; Schachat, A.P.; Simpson, E.R.; et al. Collaborative Ocular Melanoma Study Group. Collaborative ocular melanoma study (COMS) randomized trial of I-125 brachytherapy for medium choroidal melanoma. I. Visual acuity after 3 years COMS report no. 16. Ophthalmology 2001, 108, 348–366. [Google Scholar] [PubMed]
- Seregard, S. Radiation Therapy: Posterior Segment Complications. Dev. Ophthalmol. 2013, 52, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.C.; Shields, J.A.; Sanborn, G.; Augsburger, J.J.; Savino, P.J.; Schatz, N.J. Radiation Retinopathy. Ophthalmology 1982, 89, 1494–1501. [Google Scholar] [CrossRef]
- Midena, E.; Segato, T.; Valenti, M.; Degli Angeli, C.; Bertoja, E.; Piermarocchi, S. The Effect of External Eye Irradiation on Choroidal Circulation. Ophthalmology 1996, 103, 1651–1660. [Google Scholar] [CrossRef]
- Gündüz, K.; Shields, C.L.; Shields, J.A.; Cater, J.; Freire, J.E.; Brady, L.W. Radiation Retinopathy Following Plaque Radiotherapy for Posterior Uveal Melanoma. Arch. Ophthalmol. 1999, 117, 609–614. [Google Scholar] [CrossRef]
- Puusaari, I.; Heikkonen, J.; Kivelä, T.T. Ocular complications after iodine brachytherapy for large uveal melanomas. Ophthalmology 2004, 111, 1768–1777. [Google Scholar] [CrossRef]
- Groenewald, C.; Konstantinidis, L.; Damato, B. Effects of radiotherapy on uveal melanomas and adijacents tissue. Eye 2013, 27, 163–171. [Google Scholar] [CrossRef]
- Guyer, D.R.; Mukai, S.; Egan, K.M.; Seddon, J.M.; Walsh, S.M.; Gragoudas, E. Radiation Maculopathy after Proton Beam Irradiation for Choroidal Melanoma. Ophthalmology 1992, 99, 1278–1285. [Google Scholar] [CrossRef]
- Shields, J.A.; Shields, C.L. Management of Posterior Uveal Melanoma: Past, Present, and Future. Ophthalmology 2015, 122, 414–428. [Google Scholar] [CrossRef] [PubMed]
- Damato, B.; Kacperek, A.; Errington, D.; Heimann, H. Proton beam radiotherapy of uveal melanoma. Saudi, J. Ophthalmol. 2013, 27, 151–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichstein, D.; Karan, K. Plaque brachytherapy for posterior uveal melanoma in 2018. Curr. Opin. Ophthalmol. 2018, 29, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Okunieff, P.; Vidyasagar, S. Stem cell senescence: A double-edged sword? J. Natl. Cancer Inst. 2013, 105, 1429–1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambhav, K.; Grover, S.; Chalam, K.V. The application of optical coherence tomography angiography in retinal diseases. Surv. Ophthalmol. 2017, 62, 838–866. [Google Scholar] [CrossRef] [PubMed]
- Attaallah, H.R.; Mohamed, Y.H.; Helmy, Y.M. Optical coherence tomography classification of diabetic cystoid macular edema. Clin. Ophthalmol. 2013, 7, 1731–1737. [Google Scholar] [CrossRef] [Green Version]
- Horgan, N.; Shields, C.L.; Mashayekhi, A.; Shields, J. Classification and treatment of radiation maculopathy. Curr. Opin. Ophthalmol. 2010, 21, 233–238. [Google Scholar] [CrossRef]
- Frizziero, L.; Parrozzani, R.; Trainiti, S.; Pilotto, E.; Miglionico, G.; Pulze, S.; Midena, E. Intravitreal dexamethasone implant in radiation-induced macular oedema. Br. J. Ophthalmol. 2017, 101, 1699–1703. [Google Scholar] [CrossRef]
- Hope-Ross, M.; Yannuzzi, L.A.; Gragoudas, E.; Guyer, D.R.; Slakter, J.S.; Sorenson, J.A.; Krupsky, S.; Orlock, D.A.; Puliafito, C.A. Adverse Reactions due to Indocyanine Green. Ophthalmology 1994, 101, 529–533. [Google Scholar] [CrossRef]
- Lopez-Saez, M.; Ordoqui, E.; Tornero, P.; Baeza, A.; Sainza, T.; Zubeldia, J.; Baeza, M.L. Fluorescein-Induced Allergic Reaction. Ann. Allergy Asthma Immunol. 1998, 81, 428–430. [Google Scholar] [CrossRef]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog. Retin Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Finger, P.T. Laser photocoagulation for radiation retinopathy after ophthalmic plaque radiation therapy. Br. J. Ophthalmol. 2005, 89, 730–738. [Google Scholar] [CrossRef] [Green Version]
- Giuliari, G.P.; Sadaka, A.; Hinkle, D.M.; Simpson, E.R. Current treatments for radiation retinopathy. Acta Oncol. 2010, 50, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Sellam, A.; Coscas, F.; Rouic, L.L.-L.; Dendale, R.; Lupidi, M.; Coscas, G.; Desjardins, L.; Cassoux, N. Optical Coherence Tomography Angiography of Macular Features After Proton Beam Radiotherapy for Small Choroidal Melanoma. Am. J. Ophthalmol. 2017, 181, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Say, E.A.T.; Samara, W.A.; Khoo, C.T.L.; Mashayekhi, A.; Shields, J.A. Optical coherence tomography angiography of the macula after plaque radiotherapy of choroidal melanoma. Retina 2016, 36, 1493–1505. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.A.S.; Camp, D.A.; Ancona-Lezama, D.; Mazloumi, M.; Patel, S.P.; McLaughlin, J.W.; Ferenczy, S.R.; Mashayekhi, A.; Shields, C.L. Wide-Field (15 × 9 mm) Swept-Source Optical Coherence Tomography Angiography Following Plaque Radiotherapy of Choroidal Melanoma: An Analysis of 105 eyes. Asia Pac. J. Ophthalmol. 2020, 9, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Say, E.A.T.; Samara, W.A.; Khoo, C.T.L.; Magrath, G.N.; Sharma, P.; Ferenczy, S.; Shields, C.L. Parafoveal capillary density after plaque radiotherapy for choroidal melanoma. Retina 2016, 36, 1670–1678. [Google Scholar] [CrossRef]
- Archer, D.B.; Amoaku, W.M.K.; Gardiner, T. Radiation retinopathy—Clinical, histopathological, ultrastructural and experimental correlations. Eye 1991, 5, 239–251. [Google Scholar] [CrossRef]
- Shields, C.L.; Demirci, H.; Dai, V.; Marr, B.P.; Mashayekhi, A.; Materin, M.A.; Manquez, M.E.; Shields, J.A. Intravitreal triamcinolone acetonide for radiation maculopathy after plaque radiotherapy for choroidal melanoma. Retina 2005, 25, 868–874. [Google Scholar] [CrossRef]
- Mashayekhi, A.; Schonbach, E.; Shields, J.A.; Shields, C.L. Early subclinical macular edema in eyes with uveal melanoma. Association with future cystoid macular edema following plaque radiotherapy. Ophthalmology 2015, 122, 1023–1029. [Google Scholar]
- Caminal, J.M.; Flores-Moreno, I.; Arias, L.; Gutiérrez, C.; Piulats, J.M.; Català, J.; Rubio, M.J.; Cobos, E.; García, P.; Pera, J.; et al. Intravitreal dexamethasone implant for radiation maculopathy secondary to plaque brachytherapy in choroidal melanoma. Retina 2015, 35, 1890–1897. [Google Scholar] [CrossRef] [PubMed]
- Murray, T.G.; Shah, N.V.; Houston, S.K.; Markoe, A. Combination therapy with triamcinolone acetonide and bevacizumab for the treatment of severe radiation maculopathy in patients with posterior uveal melanoma. Clin. Ophthalmol. 2013, 7, 1877–1882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sergouniotis, P.I.; Holder, G.E.; Robson, A.G.; Michaelides, M.; Webster, A.R.; Moore, A.T. High-resolution optical coherence tomography imaging inKCNV2retinopathy. Br. J. Ophthalmol. 2011, 96, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Sharma, T.; Gella, L.; Nittala, M.G.; Pal, S.S.; Raman, R. Morphological and functional changes in spectral domain optical coherence tomography and microperimetry in macular microhole variants: Spectral domain optical coherence tomography and microperimetry correlation. Indian J. Ophthalmol. 2012, 60, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Frizziero, L.; Parrozzani, R.; Midena, G.; Miglionico, G.; Vujosevic, S.; Pilotto, E.; Midena, E. Hyperreflective intraretinal spots in radiation macular edema on spectral domain optical coherence tomography. Retina 2016, 36, 1664–1669. [Google Scholar] [CrossRef] [PubMed]
- Veverka, K.K.; AbouChehade, J.E.; Iezzi, R., Jr.; Pulido, J.S. Non-invasive grading of radiation retinopathy: The use of optical coherence tomography angiography. Retina 2015, 35, 2400–2410. [Google Scholar] [CrossRef] [PubMed]
- Parrozzani, R.; Midena, E.; Trainiti, S.; Londei, D.; Miglionico, G.; Annunziata, T.; Frisina, R.; Pilotto, E.; Frizziero, L. Identification and classification of macular morphologic biomarkers related to visual acuity in radiation maculopathy. Retina 2020, 40, 1419–1428. [Google Scholar] [CrossRef]
- Matet, A.; Daruich, A.; Zografos, L. Radiation Maculopathy After Proton Beam Therapy for Uveal Melanoma: Optical Coherence Tomography Angiography Alterations Influencing Visual Acuity. Investig. Opthalmol. Vis. Sci. 2017, 58, 3851–3861. [Google Scholar] [CrossRef]
- Daruich, A.; Matet, A.; Schalenbourg, A.; Zografos, L. Intravitreal anti–vascular endothelial growth factor treatment at 2-month intervals reduces foveal avascular zone enlargement and vision loss in radiation maculopathy. Retina 2019, 39, 1519–1526. [Google Scholar] [CrossRef]
- Cennamo, G.; Montorio, D.; Bernardo, R.; Farella, A.; Liuzzi, R.; Breve, M.A.; Reibaldi, M.; Cennamo, G. Retinal Vascular Changes in Radiation Maculopathy after Intravitreal Ranibizumab by Optical Coherence Tomography Angiography. J. Clin. Med. 2020, 9, 1618. [Google Scholar] [CrossRef]
- Li, Y.; Say, E.A.T.; Ferenczy, S.; Agni, M.; Shields, C.L. Altered parafoveal microvasculature in treatment-naive choroidal melanoma eyes detected by optical coherence tomography angiography. Retin 2017, 37, 32–40. [Google Scholar] [CrossRef]
- Valverde-Megías, A.; Say, E.A.T.; Ferenczy, S.R.; Shields, C.L. Differential Macular Features on Optical Coherence Tomography Angiography in Eyes with Choroidal Nevus and Melanoma. Retin 2017, 37, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Danesh-Meyer, H.V. Radiation-induced optic neuropathy. J. Clin. Neurosci. 2008, 15, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Mayo, C.; Martel, M.K.; Marks, L.B.; Flickinger, J.; Nam, J.; Kirkpatrick, J. Radiation Dose–Volume Effects of Optic Nerves and Chiasm. Int. J. Radiat. Oncol. 2010, 76, S28–S35. [Google Scholar] [CrossRef]
- Yousef, Y.A.; Finger, P.T. Optical Coherence Tomography of Radiation Optic Neuropathy. Ophthalmic Surg. Lasers Imaging 2012, 43, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Higashiyama, T.; Nishida, Y.; Ohji, M. Optical coherence tomography angiography in eyes with good visual acuity recovery after treatment for optic neuritis. PLoS ONE 2017, 12, e0172168. [Google Scholar] [CrossRef] [PubMed]
- Mammo, Z.; Heisler, M.; Balaratnasingam, C.; Lee, S.; Yu, D.-Y.; MacKenzie, P.; Schendel, S.; Merkur, A.; Kirker, A.; Albiani, D.; et al. Quantitative Optical Coherence Tomography Angiography of Radial Peripapillary Capillaries in Glaucoma, Glaucoma Suspect, and Normal Eyes. Am. J. Ophthalmol. 2016, 170, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Jia, Y.; Spain, R.; Potsaid, B.M.; Liu, J.J.; Baumann, B.; Hornegger, J.; Fujimoto, J.G.; Wu, Q.; Huang, D. Optical coherence tomography angiography of optic nerve head and parafovea in multiple sclerosis. Br. J. Ophthalmol. 2014, 98, 1368–1373. [Google Scholar] [CrossRef] [Green Version]
- Parrozzani, R.; Leonardi, F.; Frizziero, L.; Trevisson, E.; Clementi, M.; Pilotto, E.; Fusetti, S.; Miglionico, G.; Midena, E. Retinal Vascular and Neural Remodeling Secondary to Optic Nerve Axonal Degeneration: A Study Using OCT Angiography. Ophthalmol. Retin 2018, 2, 827–835. [Google Scholar] [CrossRef]
- Spaide, R.F.; Klancnik, J.M.; Cooney, M.J. Retinal Vascular Layers Imaged by Fluorescein Angiography and Optical Coherence Tomography Angiography. JAMA Ophthalmol. 2015, 133, 45–50. [Google Scholar] [CrossRef]
- Falavarjani, K.G.; Akil, H.; Sadda, S.R.; Sadun, A.A. Optical coherence tomography angiography of the optic disc; an overview. J. Ophthalmic Vis. Res. 2017, 12, 98–105. [Google Scholar] [CrossRef]
- Skalet, A.H.; Liu, L.; Binder, C.; Miller, A.K.; Wang, J.; Wilson, D.J.; Crilly, R.; Thomas, C.R.; Hung, A.Y.; Huang, D.; et al. Quantitative OCT Angiography Evaluation of Peripapillary Retinal Circulation after Plaque Brachytherapy. Ophthalmol. Retin 2018, 2, 244–250. [Google Scholar] [CrossRef]
- Naseripour, M.; Falavarjani, K.G.; Mirshahi, R.; Sedaghat, A. Optical coherence tomography angiography (OCTA) applications in ocular oncology. Eye 2020, 34, 1535–1545. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Abbreviation | Grades | Grade Definition |
|---|---|---|---|
| Vertical size of the largest macular cyst * | C (cyst) | Cx | Cx: the vertical size of the largest macular cyst cannot be assessed; † |
| C0 | C0: no evidence of measurable cysts; | ||
| Cn | Cn: n indicate the vertical size of the largest macular cyst in μm ‡ | ||
| IS/OS junction alterations * | J (IS/OS junction) | Jx | Jx: the presence of IS/OS junction alterations cannot be assessed; † |
| J0 | J0: no evidence of IS/OS junction alterations; | ||
| J1 | J1: presence of IS/OS junction alterations; | ||
| RPE atrophy * | A (RPE atrophy) | Ax | Ax: the presence of RPE atrophy cannot be assessed; † |
| A0 | A0: no evidence of RPE atrophy | ||
| A1 | A1: presence of RPE atrophy |
| Features | Ophthalmoscopy | FA | OCT | OCTA |
|---|---|---|---|---|
| Hemorrage | + | +/− | − | − |
| Microaneurysm | + | + | − | + |
| Telangiectasia | + | + | − | + |
| Hard exudate | + | +/− | +/− | − |
| Cotton wool spot | + | +/− | − | − |
| Neovasculararization | +/− | + | − | + |
| Hyperreflective intraretinal foci | − | − | + | − |
| Macular edema | +/− | +/− | + | +/− |
| Macular intraretinal cysts | − | +/− | + | +/− |
| Subfoveal fluid | − | +/− | + | − |
| IS/OS disruption | − | − | + | − |
| RPE atrophy | +/− | +/− | + | − |
| Vitreoretinal interface alteration | +/− | − | + | − |
| Macular thickness | − | − | + | − |
| Foveal avascular zone area | − | +/− | − | + |
| Macular ischemia | − | + | − | + |
| Grade 0 | - Regular radial distribution of the peripapillary capillaries - Absence of vessels abnormalities |
| Grade 1 * | - Loss of the radial pattern of the RPCP - Absence of peripapillary ischemia |
| Grade 2 * | - Peripapillary hypoperfusion in less than two quadrants (defined area of RPCP dropout) |
| Grade 3 * | - Peripapillary hypoperfusion in more than two quadrants (RPCP dropout > 180°) |
| Grade 4 † | - Peripapillary hypoperfusion, (complete RPCP dropout or poor OCT image quality) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Midena, G.; Parrozzani, R.; Frizziero, L.; Midena, E. Chorioretinal Side Effects of Therapeutic Ocular Irradiation: A Multimodal Imaging Approach. J. Clin. Med. 2020, 9, 3496. https://doi.org/10.3390/jcm9113496
Midena G, Parrozzani R, Frizziero L, Midena E. Chorioretinal Side Effects of Therapeutic Ocular Irradiation: A Multimodal Imaging Approach. Journal of Clinical Medicine. 2020; 9(11):3496. https://doi.org/10.3390/jcm9113496
Chicago/Turabian StyleMidena, Giulia, Raffaele Parrozzani, Luisa Frizziero, and Edoardo Midena. 2020. "Chorioretinal Side Effects of Therapeutic Ocular Irradiation: A Multimodal Imaging Approach" Journal of Clinical Medicine 9, no. 11: 3496. https://doi.org/10.3390/jcm9113496
APA StyleMidena, G., Parrozzani, R., Frizziero, L., & Midena, E. (2020). Chorioretinal Side Effects of Therapeutic Ocular Irradiation: A Multimodal Imaging Approach. Journal of Clinical Medicine, 9(11), 3496. https://doi.org/10.3390/jcm9113496