Extensive Testing and Public Health Interventions for the Control of COVID-19 in the Republic of Cyprus between March and May 2020

 , ,
, ,  , ,
, ,  , , , ,
, , , ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Source and Surveillance System
2.2. Definitions
2.3. Public Health Interventions and Measures
2.4. Contact Tracing and Testing Strategy
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Cases
3.2. Characteristics of Hospitalized Cases
3.3. Intensive Care Unit Admission
3.4. Characteristics of Patients Who Died
3.5. Characteristics of Recovered/Cured Cases
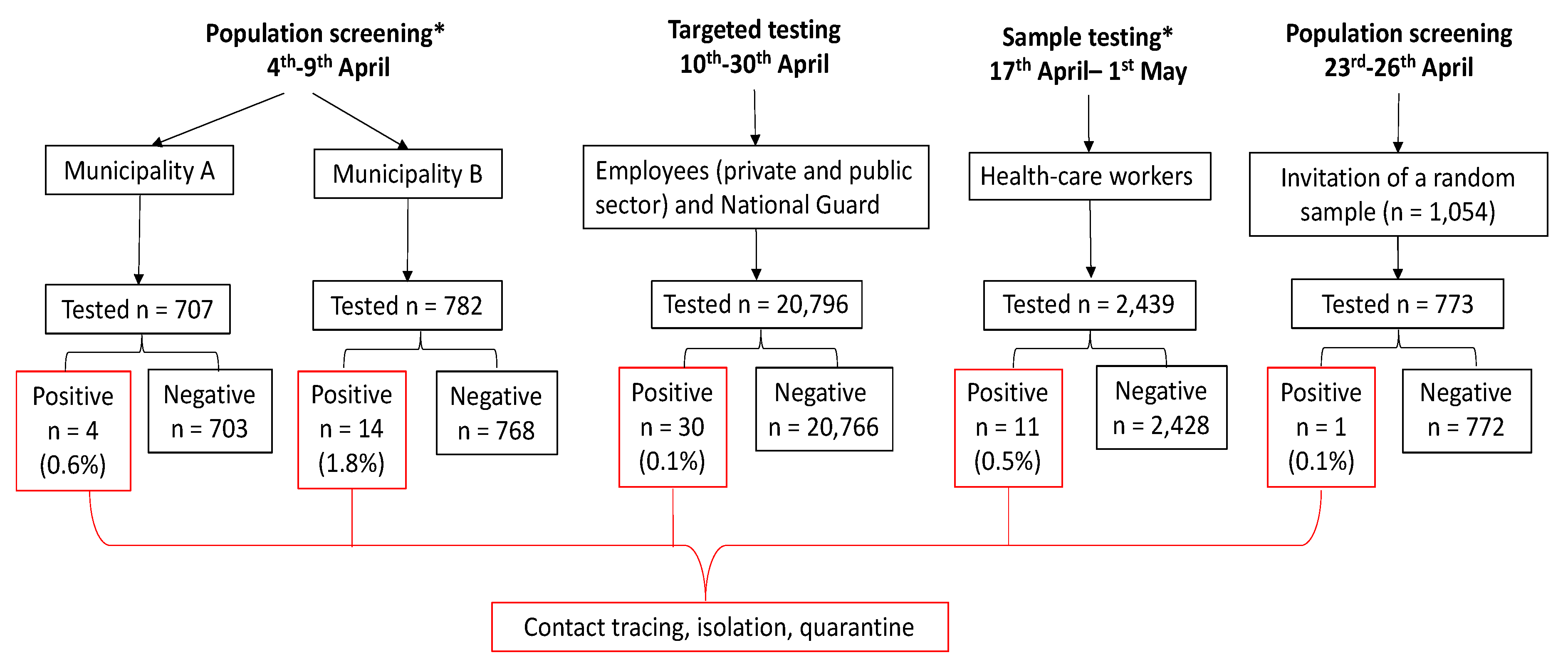
3.6. Active Case Finding
3.7. Secondary Attack Rate
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19). Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 5 October 2020).
- Mahase, E. China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ 2020, 368, m408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health System Response monitor (HSRM). Covid-19 Health System Response Monitor, Policy Responses for Cyprus. Available online: https://www.covid19healthsystem.org/countries/cyprus/livinghit.aspx?Section=1.2 Physical distancing&Type=Section (accessed on 27 May 2020).
- Pan American Health Organization. Ethics Guidance on Issues Raised by the Novel Coronavirus Disease (COVID-19) Pandemic. Available online: https://iris.paho.org/handle/10665.2/52091 (accessed on 28 September 2020).
- Republic of Cyprus Ministry of Health Medical and Public Health Services. New Case Definition and Laboratory Testing Criteria. Available online: https://www.pio.gov.cy/coronavirus/en/ (accessed on 5 June 2020).
- European Centre for Disease Prevention and Control (ECDC). Testing Strategies. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/testing-strategies (accessed on 13 July 2020).
- European Centre for Disease Prevention and Control (ECDC). Coronavirus Disease 2019 (COVID-19) in the EU/EEA and the UK– Ninth Update. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-rapid-risk-assessment-coronavirus-disease-2019-ninth-update-23-april-2020.pdf (accessed on 7 November 2020).
- World Health Organization. The First Few X Cases and Contacts (FFX) Investigation Protocol for Coronavirus Disease 2019 (COVID-19). Available online: https://apps.who.int/iris/bitstream/handle/10665/331235/WHO-2019-nCoV-FFXprotocol-2020.2-eng.pdf (accessed on 28 September 2020).
- European Centre for Disease Prevention and Control. Public Health Management of Persons, Including Healthcare Workers, Having Had Contact with COVID-19 Cases in the European Union. Available online: www.eurosurveillance.org (accessed on 28 September 2020).
- World Health Organization. Protocol for Assessment of Potential Risk Factors for 2019-Novel Coronavirus (COVID-19) Infection among Health Care Workers in a Health Care Setting. Available online: https://www.who.int/publications-detail/protocol-for-assessment-of-potential-risk-factors-for-2019-novel-coronavirus-(2019-ncov)-infection-among-health-care-workers-in-a-health-care-setting (accessed on 5 June 2020).
- European Centre for Disease Prevention and Control Novel Coronavirus (SARS-CoV-2): Discharge Criteria for Confirmed COVID-19 Cases. Available online: https://www.ecdc.europa.eu/en/publications-data/novel-coronavirus-sars-cov-2-discharge-criteria-confirmed-covid-19-cases (accessed on 28 August 2020).
- Liu, Y.; Eggo, R.M.; Kucharski, A.J. Secondary attack rate and superspreading events for SARS-CoV-2. Lancet 2020, 395, e47. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Contact Tracing in the Context of COVID-19. Available online: https://apps.who.int/iris/bitstream/handle/10665/332049/WHO-2019-nCoV-Contact_Tracing-2020.1-eng.pdf?sequence=1&isAllowed=y (accessed on 31 May 2020).
- Statistical Service of the Republic of Cyprus. Demographic Statistics 2018. Available online: http://www.cystat.gov.cy/mof/cystat/statistics.nsf/All/0F27BA4B99ABE197C22584BA003C9DED?OpenDocument&sub=1&sel=1&e=&print (accessed on 5 October 2020).
- Eurostat. Revision of the European Standard Population; Publication Office of the European Union: Luxemburg, 2013; ISBN 9789279310942. [Google Scholar]
- Kwok, K.O.; Yu Wong, V.W.; Wei, W.I.; Shan Wong, S.Y.; Tang, J.W.T. Epidemiological characteristics of the first 53 laboratory-confirmed cases of COVID-19 epidemic in Hong Kong, 13 February 2020. Eurosurveillance 2020. [Google Scholar] [CrossRef] [PubMed]
- FINDDX. SARS-CoV-2 Test Tracker - FIND. Available online: https://www.finddx.org/covid-19/test-tracker/ (accessed on 13 July 2020).
- Ng, Y.; Li, Z.; Chua, Y.X.; Chaw, W.L.; Zhao, Z.; Er, B.; Pung, R.; Chiew, C.J.; Lye, D.C.; Heng, D.; et al. Evaluation of the effectiveness of surveillance and containment measures for the first 100 patients with COVID-19 in Singapore - January 2-February 29, 2020. Morb. Mortal. Wkly. Rep. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA J. Am. Med. Assoc. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region — Case Series. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients with COVID-19. JAMA Intern. Med. 2020. [Google Scholar] [CrossRef]
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients with COVID-19 Pneumonia: the CALL Score. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Buitrago-Garcia, D.C.; Egli-Gany, D.; Counotte, M.J.; Hossmann, S.; Imeri, H.; Salanti, G.; Low, N. The role of asymptomatic sars-cov-2 infections: rapid living systematic review and meta-analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Xie, J.; Tong, Z.; Guan, X.; Du, B.; Qiu, H. Clinical Characteristics of Patients Who Died of Coronavirus Disease 2019 in China. JAMA Netw. Open 2020. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control (ECDC). COVID-19 Situation Update for the EU/EEA and the UK, as of 4 June 2020. Available online: https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (accessed on 5 June 2020).
- Burrer, S.L.; de Perio, M.A.; Hughes, M.M.; Kuhar, D.T.; Luckhaupt, S.E.; McDaniel, C.J.; Porter, R.M.; Silk, B.; Stuckey, M.J.; Walters, M. Characteristics of health care personnel with Covid-19 - United States, February 12-April 9, 2020. Morb. Mortal. Wkly. Rep. 2020. [Google Scholar] [CrossRef] [Green Version]
- Cheng, V.C.C.; Wong, S.C.; Yuen, K.Y. Estimating Coronavirus Disease 2019 Infection Risk in Health Care Workers. JAMA Netw. Open 2020, 3, e209787. [Google Scholar] [CrossRef]
- Lytras, T.; Dellis, G.; Flountzi, A.; Hatzianastasiou, S.; Nikolopoulou, G.; Tsekou, K.; Diamantis, Z.; Stathopoulou, G.; Togka, M.; Gerolymatos, G.; et al. High prevalence of SARS-CoV-2 infection in repatriation flights to Greece from three European countries. J. Travel Med. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantino, V.; Heslop, D.J.; MacIntyre, C.R. The effectiveness of full and partial travel bans against COVID-19 spread in Australia for travellers from China during and after the epidemic peak in China. J. Travel Med. 2020. [Google Scholar] [CrossRef]
- Böhmer, M.M.; Buchholz, U.; Corman, V.M.; Hoch, M.; Katz, K.; Marosevic, D.V.; Böhm, S.; Woudenberg, T.; Ackermann, N.; Konrad, R.; et al. Investigation of a COVID-19 outbreak in Germany resulting from a single travel-associated primary case: a case series. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Ali, S.T.; Wang, L.; Lau, E.H.Y.; Xu, X.K.; Du, Z.; Wu, Y.; Leung, G.M.; Cowling, B.J. Serial interval of SARS-CoV-2 was shortened over time by nonpharmaceutical interventions. Science 2020, 369, 1106–1109. [Google Scholar] [CrossRef]
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and how should multiple imputation be used for handling missing data in randomised clinical trials - A practical guide with flowcharts. BMC Med. Res. Methodol. 2017, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Russell, T.W.; Golding, N.; Hellewell, J.; Abbott, S.; Pearson, C.A.B.; van Zandvoort, K.; Jarvis, C.I.; Gibbs, H.; Liu, Y.; Eggo, R.M.; et al. Reconstructing the global dynamics of under-ascertained COVID-19 cases and infections. medRxiv 2020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Cases (n = 873) | Alive (n = 853) | Deaths (n = 20) | CFR (95%CI) | P * | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Origin of infection | ||||||||
| Imported | 125 | 17.1 | 122 | 17.1 | 3 | 17.6 | 2.4 (0.5–6.9) | 1 |
| Locally acquired | 604 | 82.9 | 590 | 82.9 | 14 | 82.4 | 2.3 (1.3–3.9) | |
| Missing | 144 | 141 | 3 | |||||
| Sex | ||||||||
| Male | 437 | 50.1 | 421 | 49.4 | 16 | 80.0 | 3.7 (2.1–5.9) | 0.011 |
| Female | 436 | 49.9 | 432 | 50.6 | 4 | 20.0 | 0.9 (0.3–2.3) | |
| Age group (years) | ||||||||
| 0–9 | 27 | 3.1 | 27 | 3.2 | 0 | 0.0 | 0 | <0.001 |
| 10–19 | 34 | 3.9 | 34 | 4.0 | 0 | 0.0 | 0 | |
| 20–29 | 112 | 12.8 | 112 | 13.1 | 0 | 0.0 | 0 | |
| 30–39 | 173 | 19.8 | 173 | 20.3 | 0 | 0.0 | 0 | |
| 40–49 | 152 | 17.4 | 151 | 17.7 | 1 | 5.0 | 0.7 (0–3.6) | |
| 50–59 | 159 | 18.2 | 158 | 18.5 | 1 | 5.0 | 0.6 (0–3.5) | |
| 60–69 | 111 | 12.7 | 105 | 12.3 | 6 | 30.0 | 5.4 (2–11.4) | |
| 70–79 | 80 | 9.2 | 72 | 8.4 | 8 | 40.0 | 10 (4.4–18.8) | |
| 80+ | 25 | 2.9 | 21 | 2.5 | 4 | 20.0 | 16 (4.5–36.1) | |
| Mean ± SD (Median; (IQR)) | 46 ± 18.8 (46; (32–59)) | 45 ± 18.4 (45; (32–59)) | 73 ± 10.2 (76; (67–79)) | <0.001 | ||||
| District | ||||||||
| Famagusta | 41 | 4.7 | 38 | 4.5 | 3 | 15.0 | 7.3 (1.5– 9.9) | 0.067 |
| Larnaca | 228 | 26.1 | 222 | 26.0 | 6 | 30.0 | 2.6 (1.0–5.6) | |
| Limassol | 97 | 11.1 | 95 | 11.1 | 2 | 10.0 | 2.1 (0.3–7.3) | |
| Nicosia | 334 | 38.3 | 331 | 38.8 | 3 | 15.0 | 0.9 (0.2–2.6) | |
| Pafos | 154 | 17.6 | 148 | 17.4 | 6 | 30.0 | 3.9 (1.4–8.3) | |
| Other (Unknown, abroad, British bases) | 19 | 2.2 | 19 | 2.2 | 0 | 0.0 | 0 | |
| Healthcare–worker | ||||||||
| No | 686 | 78.6 | 666 | 78.1 | 20 | 100.0 | 2.9 (1.8–4.5) | 0.011 |
| Yes | 187 | 21.4 | 187 | 21.9 | 0 | 0 | 0 | |
| Physician | 39 | 20.9 | 39 | 20.9 | 0 | 0 | 0 | NC |
| Nurse | 94 | 50.3 | 94 | 50.3 | 0 | 0 | 0 | NC |
| Other healthcare worker | 13 | 7 | 13 | 7 | 0 | 0 | 0 | NC |
| Auxiliary staff | 41 | 21.9 | 41 | 21.9 | 0 | 0 | 0 | NC |
| Smoking status | ||||||||
| No | 444 | 80.9 | 439 | 81.1 | 5 | 62.5 | 1.1 (0.4–2.6) | 0.183 |
| Yes | 105 | 19.1 | 102 | 18.9 | 3 | 37.5 | 2.9 (0.6 –8.1) | |
| Missing | 324 | 312 | 12 | |||||
| Symptoms at diagnosis | ||||||||
| No | 265 | 30.8 | 264 | 31.4 | 1 | 5.6 | 0.4 (0–2.1) | 0.018 |
| Yes | 594 | 69.2 | 577 | 68.6 | 17 | 94.4 | 2.9 (1.7–4.5) | |
| ≥3 symptoms | 240 | 27.9 | 234 | 27.8 | 6 | 33.3 | 2.5 (0.9–5.4) | NC |
| Cough | 303 | 51.0 | 293 | 35.2 | 10 | 58.8 | 3.3 (1.6–6.0) | NC |
| Fever | 276 | 46.5 | 268 | 32.3 | 8 | 47.1 | 2.9 (1.3–5.6) | NC |
| Sore throat | 153 | 25.8 | 151 | 18.2 | 2 | 12.5 | 1.3 (0.2–4.6) | NC |
| Myalgia | 194 | 32.7 | 191 | 23 | 3 | 18.8 | 1.6 (0.3–4.5) | NC |
| Shortness of breath/respiratory distress | 104 | 17.5 | 98 | 12 | 6 | 37.5 | 5.8 (2.1–12.1) | NC |
| Anosmia | 122 | 20.5 | 122 | 16.3 | 0 | 0 | 0 | NC |
| Diarrhea | 94 | 15.8 | 92 | 11.1 | 2 | 11.8 | 2.1 (0.3–7.5) | NC |
| Missing | 14 | 12 | 2 | |||||
| Underlying health conditions | ||||||||
| No | 450 | 58.8 | 447 | 60.0 | 3 | 15.0 | 0.7 (0–1.9) | <0.001 |
| Yes | 315 | 41.2 | 298 | 40.0 | 17 | 85.0 | 5.4 (3.2–8.5) | |
| ≥2 conditions | 98 | 12.8 | 86 | 11.5 | 12 | 60.0 | 12.2 (6.5–20.4) | NC |
| Diabetes | 68 | 8.9 | 61 | 8.2 | 7 | 35.0 | 10.3 (4.2–20.1) | NC |
| Hypertension | 124 | 16.4 | 119 | 16.1 | 5 | 25.0 | 4 (1.3–9.2) | NC |
| Heart disease (excluding Hypertension) | 61 | 8 | 52 | 7.0 | 9 | 45.0 | 14.8 (7.0–26.2) | NC |
| Chronic kidney disease | 14 | 1.9 | 9 | 1.2 | 5 | 25.0 | 35.7 (12.8–64.9) | NC |
| Chronic respiratory disease, excluding asthma | 15 | 2.2 | 12 | 1.8 | 3 | 15.0 | 20 (4.3–48.1) | NC |
| Chronic liver disease | 7 | 0.9 | 4 | 0.6 | 3 | 15.0 | 42.9 (9.9–81.6) | NC |
| Immunosuppression/HIV | 15 | 2 | 15 | 2.1 | 0 | 0.0 | 0 | NC |
| Cancer | 21 | 2.7 | 18 | 2.4 | 3 | 15.0 | 14.3 (3.0–36.3) | NC |
| Neuromuscular disorder, chronic neurological | 11 | 1.4 | 11 | 1.5 | 0 | 0.0 | 0 | NC |
| Rheumatic diseases including arthritis | 8 | 1 | 8 | 1.1 | 0 | 0.0 | 0 | NC |
| Asthma | 26 | 3.4 | 26 | 3.5 | 0 | 0.0 | 0 | NC |
| Other endocrine disorder (excluding Diabetes) | 22 | 2.9 | 22 | 3.0 | 0 | 0.0 | 0 | NC |
| Missing | 108 | 108 | 0 | |||||
| Hospitalization | ||||||||
| No | 706 | 80.9 | 706 | 82.8 | 0 | 0.0 | 0 | <0.001 |
| Yes | 167 | 19.1 | 147 | 17.2 | 20 | 100.0 | 12 (7.5–17.9) | |
| ICU admission | ||||||||
| No | 841 | 96.3 | 834 | 97.8 | 7 | 35.0 | 0.8 (0.3–1.7) | <0.001 |
| Yes | 32 | 3.7 | 19 | 2.2 | 13 | 65.0 | 40.6 (23.7–59.4) | |
| Intubation | ||||||||
| No | 846 | 96.9 | 836 | 98.0 | 10 | 50.0 | 1.2 (0.6–2.2) | <0.001 |
| Yes | 27 | 3.1 | 17 | 2.0 | 10 | 50.0 | 37.0 (19.4–57.6) | |
| Characteristics | Hospitalized (n = 167) | Not Hospitalized (n = 706) | OR (95%CI) | aOR (95%CI) | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Male | 110 | 65.9 | 327 | 46.3 | 2.2 (1.6–3.2) | 3.0 (2.0–4.7) |
| Age group | ||||||
| 0–9 | 4 | 2.4 | 23 | 3.3 | Ref | 1.6 (1.4–1.8) 2 |
| 10–19 | 1 | 0.6 | 33 | 4.7 | 0.2 (0.0–1.7) | |
| 20–29 | 7 | 4.2 | 105 | 14.9 | 0.4 (0.1–1.4) | |
| 30–39 | 9 | 5.4 | 164 | 23.2 | 0.3 (0.1–1.1) | |
| 40–49 | 21 | 12.6 | 131 | 18.6 | 0.9 (0.3–2.9) | |
| 50–59 | 33 | 19.8 | 126 | 17.8 | 1.5 (0.5–4.7) | |
| 60–69 | 39 | 23.4 | 72 | 10.2 | 3.1 (1.0–9.7) | |
| 70–79 | 35 | 21 | 45 | 6.4 | 4.5 (1.4–14.1) | |
| 80+ | 18 | 10.8 | 7 | 1 | 14.8 (3.7–58.5) | |
| Smoking status (yes) | 14 | 17.5 | 91 | 19.4 | 0.9 (0.5–1.6) | NI |
| Symptoms at diagnosis (yes) | 144 | 88.9 | 450 | 64.6 | 4.4 (2.6–7.3) | 6.1 (3.2–11.5) |
| Cough (yes) | 90 | 57.3 | 213 | 30.8 | 3.0 (2.1–4.3) | NI |
| Fever (yes) | 87 | 55.4 | 189 | 27.4 | 3.3 (2.3–4.7) | NI |
| Sore throat (yes) | 26 | 16.7 | 127 | 18.5 | 0.9 (0.6–1.4) | NI |
| Myalgia (yes) | 53 | 34.2 | 141 | 20.4 | 2.0 (1.4–3.0) | NI |
| Shortness of breath/respiratory distress (yes) | 45 | 29.6 | 59 | 8.7 | 4.4 (2.9–6.9) | NI |
| Anosmia (yes) | 16 | 12.8 | 106 | 16.7 | 0.7 (0.4–1.3) | NI |
| Diarrhea (yes) | 21 | 13.5 | 73 | 10.6 | 1.3 (0.8–2.2) | NI |
| Underlying health conditions (yes) | 98 | 69.5 | 217 | 34.8 | 4.3 (2.9–6.3) | 2.1 (1.3–3.3) |
| Diabetes (yes) | 34 | 24.1 | 34 | 5.4 | 5.5 (3.3–9.3) | NI |
| Hypertension (yes) | 44 | 31.4 | 80 | 12.9 | 3.1 (2.0–4.7) | NI |
| Heart disease (excluding Hypertension) (yes) | 31 | 22.1 | 30 | 4.8 | 5.6 (3.3–9.6) | NI |
| Chronic kidney disease (yes) | 10 | 7.2 | 4 | 0.6 | 11.9 (3.7–38.5) | NI |
| Chronic respiratory disease, excluding asthma (yes) | 5 | 4.1 | 10 | 1.8 | 2.4 (0.8–7.0) | NI |
| Chronic liver disease (yes) | 5 | 3.6 | 2 | 0.3 | 11.4 (2.2–59.5) | NI |
| Immunosuppression/HIV (yes) | 4 | 2.9 | 11 | 1.8 | 1.6 (0.5–5.1) | NI |
| Cancer (yes) | 9 | 6.4 | 12 | 1.9 | 3.5 (1.4–8.4) | NI |
| Neuromuscular disorder, chronic neurological (yes) | 3 | 2.1 | 8 | 1.3 | 1.7 (0.4–6.4) | NI |
| Rheumatic diseases including arthritis (yes) | 0 | 0 | 8 | 1.3 | – | NI |
| Asthma (yes) | 7 | 5 | 19 | 3 | 1.7 (0.1–4.0) | NI |
| Other endocrine disorder (excluding Diabetes) (yes) | 2 | 1.4 | 20 | 3.2 | 0.4 (0.1–1.9) | |
| Death (yes) | 20 | 12 | 0 | 0 | – | NI |
| Age Groups (years) | Male | Female | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Screened | Positive | Screened | Positive | Screened | Positive | ||||
| N | n | % | N | n | % | N | n | % | |
| <20 | 104 | 0 | 0.00 | 43 | 0 | 0.00 | 153 | 0 | 0.00 |
| 20–24 | 388 | 1 | 0.26 | 444 | 0 | 0.00 | 884 | 1 | 0.11 |
| 25–29 | 922 | 1 | 0.11 | 920 | 1 | 0.11 | 1953 | 2 | 0.10 |
| 30–34 | 1213 | 3 | 0.25 | 850 | 0 | 0.00 | 2179 | 3 | 0.14 |
| 35–39 | 1351 | 2 | 0.15 | 965 | 1 | 0.10 | 2423 | 3 | 0.12 |
| 40–44 | 1379 | 3 | 0.22 | 1218 | 1 | 0.08 | 2696 | 4 | 0.15 |
| 45–49 | 1374 | 1 | 0.07 | 1281 | 5 | 0.39 | 2758 | 6 | 0.22 |
| 50–54 | 1229 | 3 | 0.24 | 1202 | 1 | 0.08 | 2516 | 4 | 0.16 |
| 55–59 | 1040 | 3 | 0.29 | 937 | 2 | 0.21 | 2033 | 5 | 0.25 |
| 60–64 | 619 | 0 | 0.00 | 598 | 2 | 0.33 | 1244 | 2 | 0.16 |
| 65+ | 220 | 0 | 0.00 | 133 | 0 | 0.00 | 359 | 0 | 0.00 |
| Unknown | 906 | 0 | 0.00 | 591 | 0 | 0.00 | 1598 | 0 | 0.00 |
| Total | 10,745 | 17 | 0.16 | 9182 | 13 | 0.14 | 20,796 | 30 | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quattrocchi, A.; Mamais, I.; Tsioutis, C.; Christaki, E.; Constantinou, C.; Koliou, M.; Pana, Z.-D.; Silvestros, V.; Theophanous, F.; Haralambous, C.; et al. Extensive Testing and Public Health Interventions for the Control of COVID-19 in the Republic of Cyprus between March and May 2020. J. Clin. Med. 2020, 9, 3598. https://doi.org/10.3390/jcm9113598
Quattrocchi A, Mamais I, Tsioutis C, Christaki E, Constantinou C, Koliou M, Pana Z-D, Silvestros V, Theophanous F, Haralambous C, et al. Extensive Testing and Public Health Interventions for the Control of COVID-19 in the Republic of Cyprus between March and May 2020. Journal of Clinical Medicine. 2020; 9(11):3598. https://doi.org/10.3390/jcm9113598
Chicago/Turabian StyleQuattrocchi, Annalisa, Ioannis Mamais, Constantinos Tsioutis, Eirini Christaki, Costas Constantinou, Maria Koliou, Zoi-Dorothea Pana, Valentinos Silvestros, Fani Theophanous, Christos Haralambous, and et al. 2020. "Extensive Testing and Public Health Interventions for the Control of COVID-19 in the Republic of Cyprus between March and May 2020" Journal of Clinical Medicine 9, no. 11: 3598. https://doi.org/10.3390/jcm9113598
APA StyleQuattrocchi, A., Mamais, I., Tsioutis, C., Christaki, E., Constantinou, C., Koliou, M., Pana, Z. -D., Silvestros, V., Theophanous, F., Haralambous, C., Stylianou, A., Sotiriou, S., Athanasiadou, M., Kyprianou, T., Demetriou, A., Demetriou, C. A., Kolokotroni, O., Gregoriou, I., Paphitou, N., ... Nikolopoulos, G. (2020). Extensive Testing and Public Health Interventions for the Control of COVID-19 in the Republic of Cyprus between March and May 2020. Journal of Clinical Medicine, 9(11), 3598. https://doi.org/10.3390/jcm9113598