Differentiated Thyroid Cancer in Children in the Last 20 Years: A Regional Study in Romania

 ,
,  ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Study Definitions
2.4. Statistical Analysis
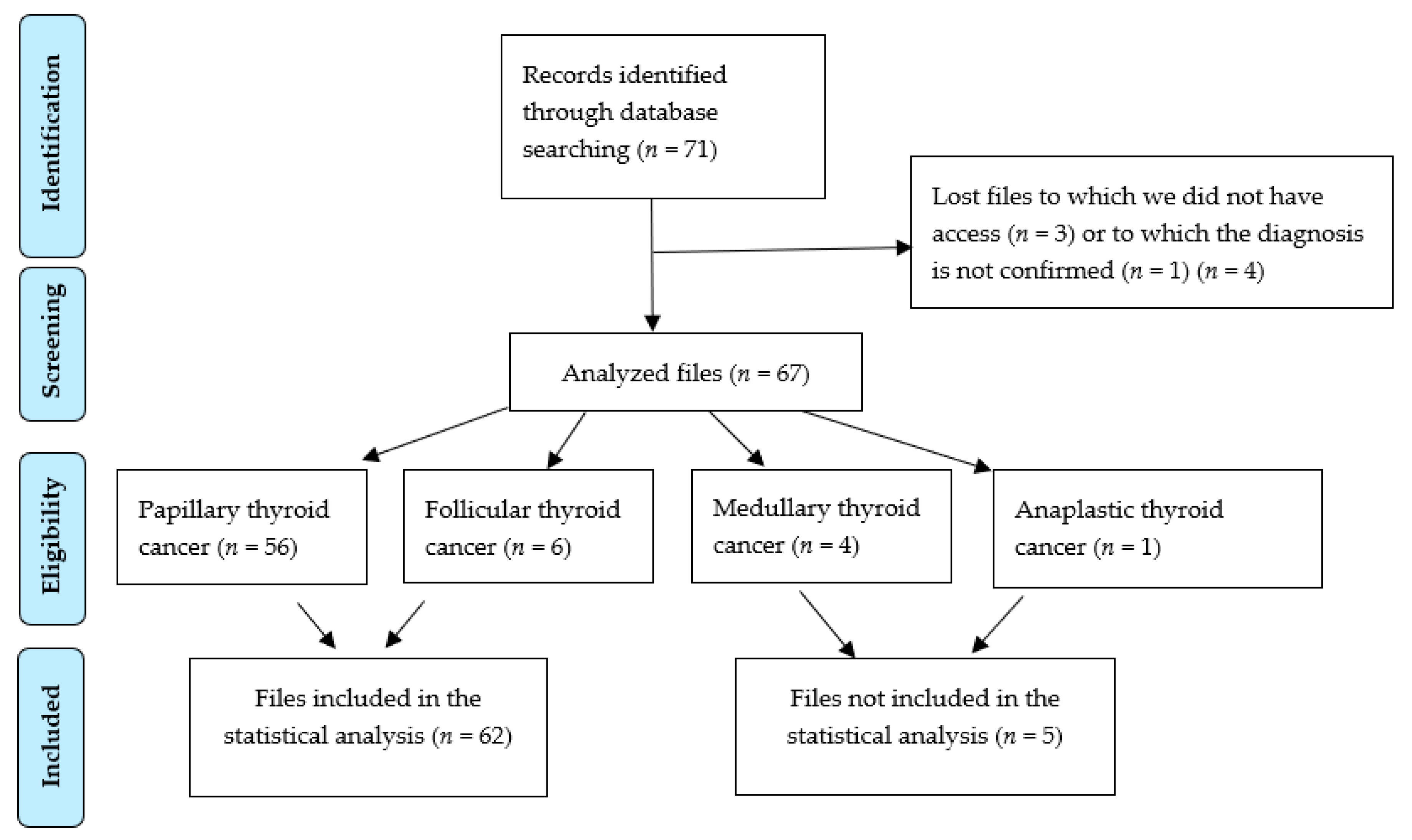
3. Results
3.1. Thyroid Cancer (Differentiated, Anaplastic, Medullary)
3.1.1. Differentiated Thyroid Cancer
3.1.2. Baseline Characteristics
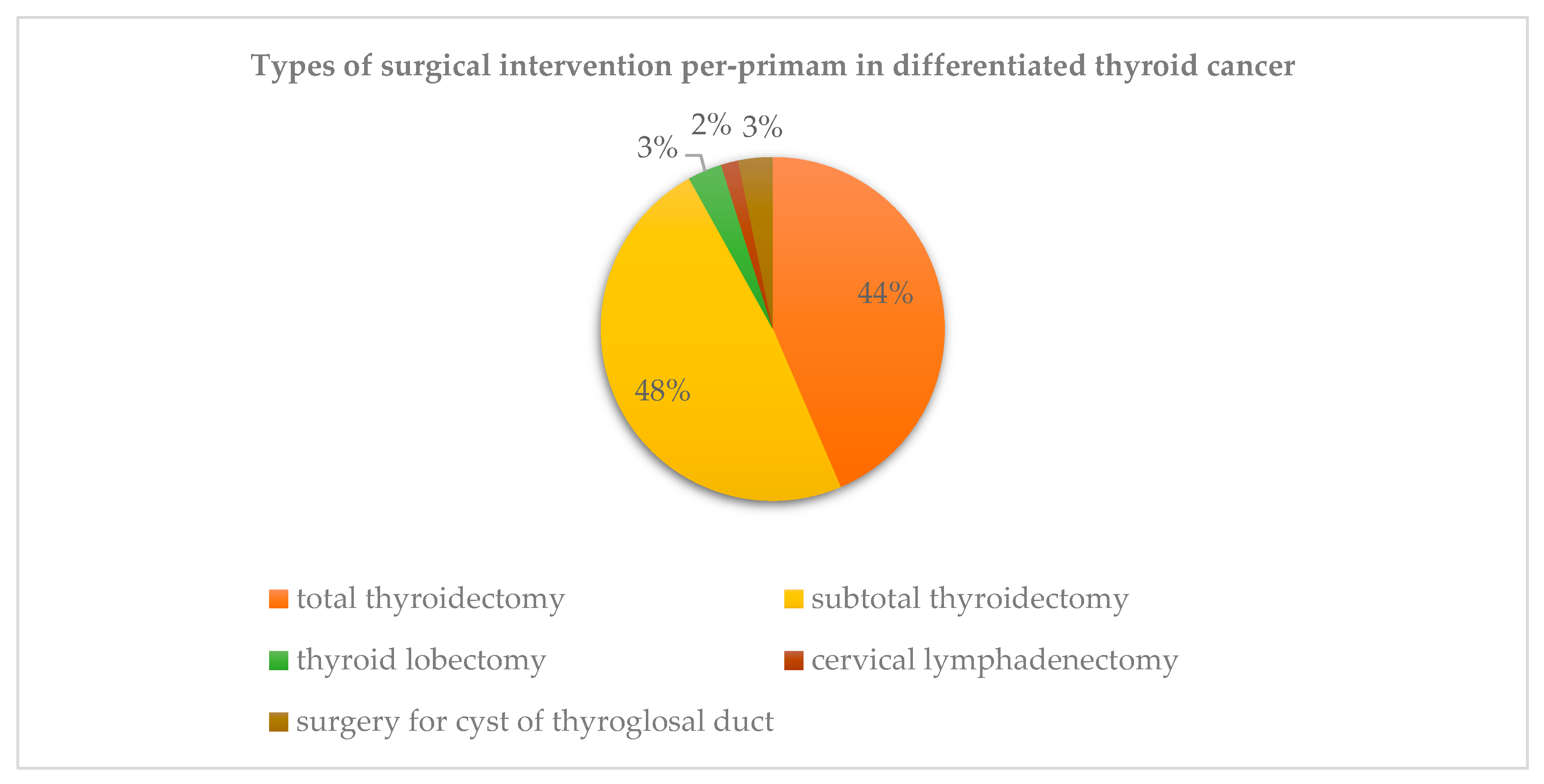
3.2. Surgical Treatment
3.2.1. Surgical Complications
3.2.2. 131-I Administration and TSH Suppression Therapy
3.3. Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vaisman, F.; Corbo, R.; Vaisman, M. Thyroid Carcinoma in Children and Adolescents—Systematic Review of the Literature. J. Thyroid. Res. 2011, 2011, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piciu, D.; Piciu, A.; Irimie, A. Thyroid cancer in children: A 20-year study at a Romanian oncology institute. Endocr. J. 2012, 59, 489–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefan, A.-I.; Piciu, A.; Mester, A.; Apostu, D.; Badan, M.; Badulescu, C.-I. Pediatric Thyroid Cancer in Europe: An Overdiagnosed Condition? A Literature Review. Diagnostics 2020, 10, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hesselink, M.S.K.; Nies, M.; Bocca, G.; Brouwers, A.H.; Burgerhof, J.G.M.; Van Dam, E.W.C.M.; Havekes, B.; Heuvel-Eibrink, M.M.V.D.; Corssmit, E.P.; Kremer, L.C.M.; et al. Pediatric Differentiated Thyroid Carcinoma in The Netherlands: A Nationwide Follow-Up Study. J. Clin. Endocrinol. Metab. 2016, 101, 2031–2039. [Google Scholar] [CrossRef] [Green Version]
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.M.; Dinauer, C.A.; Hamilton, J.K.; Hay, I.D.; Luster, M.; et al. Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucsky, P.; Parlowsky, T. Endocrinology Epidemiology and therapy of thyroid cancer in childhood and adolescence. Exp. Clin. Endocrinol. Diabetes 1997, 105, 70–73. [Google Scholar] [CrossRef] [PubMed]
- AIRTUM Working Group; CCM; AIEOP Working Group. Italian cancer figures, report 2012: Cancer in children and adolescents. Epidemiol. Prev. 2013, 37, 144–149. [Google Scholar]
- Dekker, B.L.; Newbold, K.L.; Führer, D.; Waguespack, S.G.; Handkiewicz-Junak, D.; Links, T.P.; The European Initiative on Collaboration on Paediatric Thyroid Cancer. Survey on Paediatric Differentiated Thyroid Cancer Care in Europe. Horm. Res. Paediatr. 2017, 89, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Collini, P.; Massimino, M.; Leite, S.F.; Mattavelli, F.; Seregni, E.; Zucchini, N.; Spreafico, F.; Ferrari, A.; Castellani, M.R.; Cantù, G.; et al. Papillary thyroid carcinoma of childhood and adolescence: A 30-year experience at the istituto nazionale tumori in Milan. Pediatr. Blood Cancer 2006, 46, 300–306. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, C.; Moran, A.; Whelan, J.; Hough, R.; Stiller, C.; Stevens, M.; Stark, D.; Feltbower, R.; McCabe, M.G. Trends in survival for teenagers and young adults with cancer in the UK 1992–2006. Eur. J. Cancer 2015, 51, 2039–2048. [Google Scholar] [CrossRef] [PubMed]
- Reiners, C.; Biko, J.; Haenscheid, H.; Hebestreit, H.; Kirinjuk, S.; Baranowski, O.; Marlowe, R.J.; Demidchik, E.; Drozd, V.; Demidchik, Y. Twenty-Five Years after Chernobyl: Outcome of Radioiodine Treatment in Children and Adolescents with Very High-Risk Radiation-Induced Differentiated Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2013, 98, 3039–3048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piciu, D. Thyroid cancer incidence 25 years after Chernobyl, in a Romanian cancer center: is it a public health problem? Curr. Radiopharm. 2013, 6, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.A.; Bunnell, H.; Cook, H.A.; Williams, E.D.; Nerovnya, A.; Cherstvoy, D.; Tronko, N.D.; Bogdanova, T.I.; Chiappetta, G.; Viglietto, G.; et al. High Prevalence of RET/PTC Rearrangements in Ukrainian and Belarussian Post-Chernobyl Thyroid Papillary Carcinomas: A Strong Correlation between RET/PTC3 and the Solid-Follicular Variant. J. Clin. Endocrinol. Metab. 1999, 84, 4232–4238. [Google Scholar] [PubMed]
- Niedziela, M.; Korman, E. Thyroid carcinoma in a fourteen-year-old boy with Graves disease. Med. Pediatr. Oncol. 2002, 38, 290–291. [Google Scholar] [CrossRef] [PubMed]
- Szántó, Z.; Kun, I.Z.; Borda, A.; Jung, J. Thyroid cancer in two representative medical centers in mureş county between 1984–2007. Acta Endocrinol. 2009, 5, 199–211. [Google Scholar]
- de Benoist, B.; Andersson, M.; Egli, I.; Takkouche, B.; Allen, H. Iodine Status Worldwide. WHO Global Database Iodine Deficiency; World Health Organization: Geneva, Switzerland, 2004; pp. 1–12. [Google Scholar]
- American Joint Committee on Cancer. AJCC Cancer Staging Manual, 8th ed.; Amin, M.B., Edge, S.B., Green, F.L., Byrd, D.R., Brookland, R.K., Washington, M.K., Gershenwald, J.E., Compton, C.C., Hess, K.R., Sullivan, D.C., et al., Eds.; Springer: New York, NY, USA, 2017; pp. 873–890. [Google Scholar]
- Tuttle, M.; Haugen, B.; Perrier, N. The Updated AJCC/TNM Staging System for Differentiated and Anaplastic Thyroid Cancer (8th edition): What changed and why? Thyroid 2017. [Google Scholar] [CrossRef] [PubMed]
- Saxebøl, G.; Olerud, H.M.; Hjardemaal, O.; Leitz, W.; Servomaa, A.; Walderhaug, T. Nordic guidance levels for patient doses in diagnostic radiology. Radiat. Prot. Dosim. 1998, 80, 99–101. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 62) | 0–10 y (n = 6) | 11–14 y (n = 23) | 15–18 y (n = 33) | p-Value a |
|---|---|---|---|---|---|
| Sex, n (%) | 0.655 | ||||
| Male | 12 (19.3) | 0 | 5 (21.7) | 7 (21.2) | |
| Female | 50 (80.6) | 6 (100) | 18 (78.2) | 26 (78.7) | |
| Age at diagnosis, years | n.a. | ||||
| Median (range) | 13.1 (8.2–18) | 9.6 (8.2–10.8) | 13.6 (11.7–14.9) | 16.5 (15.1–18) | |
| Histology, n (%) | 0.540 | ||||
| Papillary | 56 (90.3) | 5 (83.3) | 22 (95.6) | 29 (87.8) | |
| Follicular | 6 (9.6) | 1 (16.6) | 1 (4.3) | 4 (12.1) | |
| Primary tumor size, cm | 0.587 | ||||
| Median (range) | 2.15 (0.15–6.4) | 1.9 (0.4–3) | 2.1 (0.6–4.5) | 2.14 (0.15–6.4) | |
| Localization, n (%) | 0.422 | ||||
| Unilateral | 45 (72.5) | 4 (66.6) | 14 (60.8) | 27 (81.8) | |
| RTL | 27 (43.5) | 2 (33.3) | 9 (39.1) | 16 (48.4) | |
| LTL | 15 (24.1) | 2 (33.3) | 4 (17.3) | 9 (27.2) | |
| RTL + Isthmus | 1 (1.6) | 0 | 1 (4.34) | 0 | |
| LTL + Isthmus | 2 (3.2) | 0 | 0 | 2 (6.06) | |
| Bilateral | 12 (19.3) | 1 (16.6) | 6 (26) | 5 (15.1) | |
| Other b | |||||
| Isthmus | 1 (1.6) | 0 | 1 (4.3) | 0 | |
| Thyroglossal duct | 2 (3.2) | 1 (16.6) | 1 (4.3) | 0 | |
| Unknown | 2 (3.2) | 0 | 1 (4.3) | 1 (3.03) | |
| Multifocality, n (%) | 0.218 | ||||
| No | 37 (59.6) | 3 (50) | 11 (47.8) | 23 (69.6) | |
| Yes | 25 (40.3) | 3 (50) | 12 (52.1) | 10 (30.3) | |
| TNM stage, n (%) | 0.856 | ||||
| T | |||||
| T1–T2 | 39 (62.9) | 3 (50) | 15 (65.2) | 21 (63.6) | |
| T3–T4 | 23 (37) | 3 (50) | 8 (34.7) | 12 (36.3) | |
| N | 0.390 | ||||
| N0 | 26 (41.9) | 1 (16.6) | 8 (34.7) | 17 (51.5) | |
| N1a–N1b | 22 (35.4) | 2 (33.3) | 11 (47.8) | 9 (27.2) | |
| Nx b | 14 (22.5) | 3 (50) | 4 (17.3) | 7 (21.2) | |
| M | 0.448 | ||||
| M0 | 56 (90.3) | 5 (83.3) | 20 (86.9) | 31 (93.9) | |
| M1 c | 6 (9.6) | 1 (16.6) | 3 (13) | 2 (6) | |
| Lung | 6 | 1 | 3 | 2 | |
| Bone | 0 | 0 | 0 | 0 | |
| Surgery, n (%) | n.a. | ||||
| Total thyroidectomy | 27 + 26 = 53 | 2 + 4 = 6 | 10 + 10 = 20 | 15 + 12 = 27 | |
| (S1 + S2) | (85.4) | (100) | (86.9) | (81.8) | |
| Lymph node dissection | 0.183 | ||||
| None | 40 (64.5) | 3 (50) | 15 (65.2) | 22 (66.6) | |
| Central LND | 3 (4.8) | 2 (33.3) | 1 (4.3) | 0 | |
| LND incl. Lateral levels | 15 (24.1) | 1 (16.6) | 6 (26) | 8 (24.2) | |
| Unknown | 4 (6.4) | 0 | 1 (4.34) | 3 (9.09) |
| Hypoparathyroidism, n (%) | Recurrent Laryngeal Nerve Injury, n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Group | Present * | n.a. | p-Value a | Left | Right | Bilateral | n.a. | p-Value a |
| All patients (n = 62) | 10 (16.1) | 52 (83.8) | 1 | 1 | 1 | 59 (95.10) | 0.047 | |
| T1–T2 (n = 39) | 6 (15.3) | 33 (84.6) | 0.596 | 0 | 0 | 0 | 39 (100.00) | |
| T3–T4 (n = 23) | 4 (17.3) | 19 (82.6) | 1 (4.34) | 1 (4.34) | 1 (4.34) | 20 (8.69) | ||
| No LND (n = 40) | 5 (12.5) | 35 (87.5) | 0.102 | 0 | 0 | 0 | 40 (100.00) | 0.025 |
| LND (n = 18) | 4 (22.2) | 14 (77.7) | 1 (5.55) | 1 (5.55) | 1 (5.55) | 16 (88.80) | ||
| LND unknown (n = 4) | 1 (25.0) | 3 (75.0) | 0 | 0 | 1 (25.00) | 3 (75.00) | ||
| Group | Cumulative 131-I Activity | p-Value a | 131-I Therapeutic Administrations, n | p-Value a | |
|---|---|---|---|---|---|
| mCi | GBq | ||||
| All patients (n = 52) b | 186.68 (17.88–990.15) | 6.90 (0.66–36.63) | 2.38 (1–9) | ||
| T1–T2 (n = 29) | 100.34 (17.88–351.10) | 3.71 (0.66–12.99) | 0.001 | 1.65 (1–5) | 0.005 |
| T3–T4 (n = 23) | 295.54 (38.85–990.15) | 10.9 (1.43–36.63) | 3.30 (1–9) | ||
| N0 (n = 19) | 88.85 (17.88–267.20) | 3.28 (0.66–9.88) | ˂0.001 | 1.57 (1–5) | 0.005 |
| N1a–N1b (n = 19) | 344.35 (38.85–990.15) | 12.74 (1.43–36.63) | 3.54 (1–9) | ||
| Nx (n = 14) | 105.46 (50–265.51) | 3.90 (1.85–9.82) | 1.85 (1–3) | ||
| M0 (n = 46) | 153.88 (17.88–629.99) | 5.69 (0.66–23.30) | 0.022 | 2.15 (1–6) | 0.059 |
| M1 (n = 6) | 438.14 (64.75–990.15) | 16.21 (2.39–36.63) | 4.16 (1–9) | ||
| 0–10 y (n = 6) | 79.42 (30.0–200.7) | 2.93 (1.11–7.42) | 0.066 | 1.66 (1–3) | 0.217 |
| 11–14 y (n = 21) | 258.02 (17.88–990.15) | 9.54 (0.66–36.63) | 3.04 (1–9) | ||
| 15–18 y (n = 25) | 152.35 (50–629.99) | 5.63 (1.85–23.30) | 2 (1–6) | ||
| Sex and Age at Diagnosis, y | Follow-up, y | Histology, TNM * | Initial Treatment | Evidence of Disease | Localization of Disease |
|---|---|---|---|---|---|
| F, 15.1 | 2.1 | FTC, T3aN0M0 | TT, 131-I | Scintigraphy | Thyroid bed |
| F, 14.9 | 5.1 | PTC, T3N1bM0 | TT, LND, 131-I | PET–CT | Thyroid bed |
| F, 16.8 | 8.9 | PTC, T4N1bM0 | TT, LND, 131-I | WBS, PET–CT, histology | Thyroid bed, cervical lymph node |
| F, 14.0 | 3.4 | PTC, T4aN1bM1 | TT, LND, 131-I | WBS, PET-CT, CT | Cervical lymph node lung |
| F, 8.2 | 5 | PTC, T2NxM0 | TT, 131-I | WBS | Thyroid bed |
| F, 15.7 | 7.2 | PTC, T3N1bM1 | TT, 131-I | WBS | Cervical lymph node, thyroid bed, lung |
| M, 13.8 | 5.8 | PTC, T3N1bM1 | TT, LND, 131-I | WBS | Cervical lymph node, mediastinum, lung |
| F, 14.3 | 10.6 | PTC, T4N1bM1 | TT, LND, 131-I | WBS | Cervical lymph node, lung |
| F, 12.0 | 9.4 | PTC, T3N1M0 | TT, LND, 131-I | WBS | Cervical lymph node |
| F, 14.7 | 4.9 | PTC, T3N1bM0 | TT, 131-I | WBS | Thyroid bed |
| F, 15.9 | 2.4 | PTC, T2N0M0 | STT | Biochemical ** | |
| F, 17.3 | 0.9 | PTC, T1aN0M0 | TT | Biochemical | |
| F, 8.5 | 4.4 | PTC, T3N1bM0 | TT, LND, 131-I | Biochemical | |
| M, 15.2 | 4.2 | PTC, T1bN1bM0 | TT, LND, 131-I | Biochemical | |
| F, 10.5 | 7.6 | PTC, T1aNxM0 | TT, 131-I | Biochemical | |
| F, 15.5 | 12.3 | PTC, T2N0M0 | TT, 131-I | Biochemical | |
| M, 12.2 | 11.8 | PTC, T1N1aM0 | TT, 131-I | Biochemical | |
| F, 14.0 | 10.1 | PTC, T2N1M0 | TT, LND, 131-I | Biochemical | |
| F, 12.0 | 14.9 | PTC, T4N1M0 | TT, LND, 131-I | Biochemical | |
| F, 12.8 | 10.7 | PTC, T2aNxM0 | TT, 131-I | Biochemical | |
| F, 16.0 | 7.8 | PTC, T2NxM0 | TT, 131-I | Biochemical | |
| F, 17.8 | 7.7 | FTC, T2N0M0 | TT, LND, 131-I | Biochemical | |
| F, 13.3 | 18.4 | PTC, T2N0M0 | TT, 131-I | Biochemical | |
| F, 18.0 | 17.4 | PTC, T2N0M0 | TT, LND, 131-I | Biochemical | |
| M, 15.2 | 8.8 | PTC, T1N0M0 | STT, 131-I | Biochemical | |
| M, 14.8 | 7.1 | PTC, T3N1bM0 | TT, LND, 131-I | Biochemical |
| Group | Remission n (%) | Recurrence n (%) ** | Persistent Disease n (%) | p-Value | Unknown n (%) |
|---|---|---|---|---|---|
| All patients (n = 62) | 32 (51.6) | 1 (1.6) | 26 (41.9) | 3 (4.8) | |
| T1–T2 (n = 39) | 23 (58.9) | 14 (35.8) | 0.155 | 2 (5.1) | |
| T3–T4 (n = 23) | 9 (39.1) | 12 (52.1) | 1 (4.3) | ||
| Multifocality *Yes (n = 22) | 11 (50.0) | 11 (50) | 0.598 | 0 | |
| No (n = 35) | 20 (57.1) | 15 (42.9) | 3 (100.0) | ||
| Tumoral foci (cm) * ˂1 cm (n = 9) | 5 (55.5) | 3 (33.3) | 0.092 | 1 (11.1) | |
| 1–2 cm (n = 15) | 13 (86.7) | 2 (13.3) | |||
| 2–3 cm (n = 13) | 6 (46.1) | 6 (46.1) | 1 (7.6) | ||
| 3–4 cm (n = 8) | 2 (28.6) | 5 (71.4) | 1 (12.5) | ||
| 4–5 cm (n = 3) | 1 (33.3) | 2 (66.7) | |||
| 5–6 cm (n = 1) | 0 | 0 | 1 (100.0) | ||
| 6–7 cm (n = 1) | 1 (100.0) | 0 | |||
| N0 (n = 26) | 17 (65.3) | 8 (30.7) | 0.020 | 1 (3.8) | |
| N1a–N1b (n = 22) | 6 (27.2) | 14 (63.6) | 1 (4.5) | ||
| Nx (n = 14) | 9 (64.2) | 4 (28.5) | 1 (7.14) | ||
| M1 (n = 6) | 2 (33.3) | 4 (66.6) | 0.393 | 0 | |
| M0 (n = 56) | 30 (53.5) | 22 (39.2) | 3 (5.3) | ||
| FTC (n = 6) | 4 (66.6) | 2 (33.3) | 0.55 | 0 | |
| PTC (n = 56) | 28 (50.0) | 24 (42.8) | 3 (5.35) | ||
| Age groups: 0–10 y (n = 6) | 3 (50.0) | 3 (50.0) | 0.425 | 0 | |
| 11–14 y (n = 23) | 10 (45.5) | 12 (54.5) | 1 (4.3) | ||
| 15–18 y (n = 33) | 19 (63.3) | 11 (36.7) | 2 (6.06) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ștefan, A.-I.; Piciu, A.; Căinap, S.S.; Gabora, K.; Piciu, D. Differentiated Thyroid Cancer in Children in the Last 20 Years: A Regional Study in Romania. J. Clin. Med. 2020, 9, 3617. https://doi.org/10.3390/jcm9113617
Ștefan A-I, Piciu A, Căinap SS, Gabora K, Piciu D. Differentiated Thyroid Cancer in Children in the Last 20 Years: A Regional Study in Romania. Journal of Clinical Medicine. 2020; 9(11):3617. https://doi.org/10.3390/jcm9113617
Chicago/Turabian StyleȘtefan, Andreea-Ioana, Andra Piciu, Simona Sorana Căinap, Katalin Gabora, and Doina Piciu. 2020. "Differentiated Thyroid Cancer in Children in the Last 20 Years: A Regional Study in Romania" Journal of Clinical Medicine 9, no. 11: 3617. https://doi.org/10.3390/jcm9113617
APA StyleȘtefan, A. -I., Piciu, A., Căinap, S. S., Gabora, K., & Piciu, D. (2020). Differentiated Thyroid Cancer in Children in the Last 20 Years: A Regional Study in Romania. Journal of Clinical Medicine, 9(11), 3617. https://doi.org/10.3390/jcm9113617