Effects on the Upper Airway Morphology with Intravenous Addition of Ketamine after Dexmedetomidine Administration in Normal Children

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Sedation
2.2. Imaging
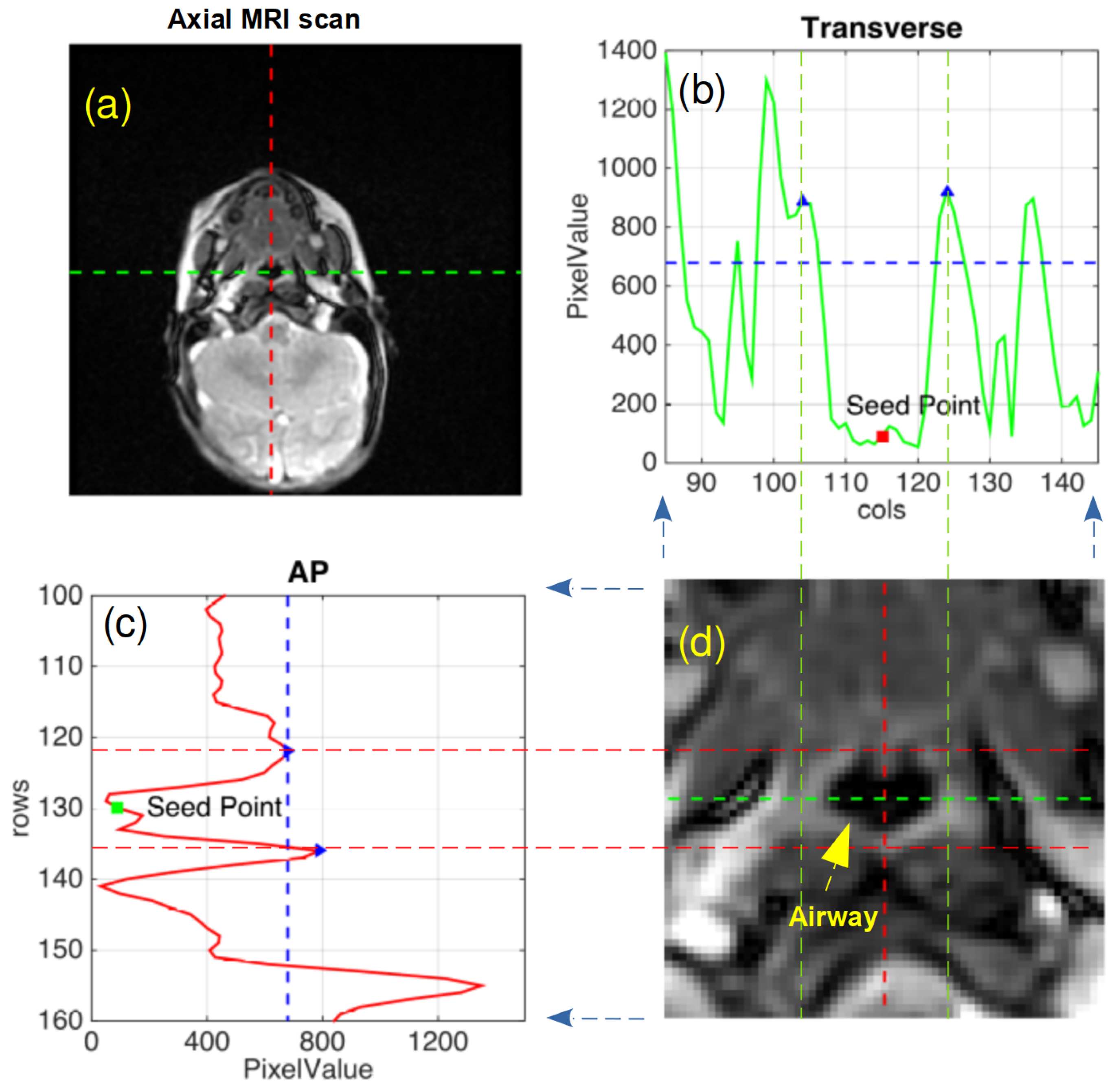
2.3. Image Analysis
2.4. Statistical Analysis
2.5. Power Analysis
3. Results
3.1. Dynamic Changes in Airway Dimensions
3.2. DEX Alone vs. DEX + Ketamine at 15 min: Paired T-test or Wilcoxon Signed Rank Test
3.3. Comparison across Treatment Groups: Linear Mixed Effects Model
3.4. Hemodynamic Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| MRI | Magnetic Resonance Imaging |
| DEX | Dexmedetomidine |
| ASA | American Society of Anesthesiologists |
| IV | Intravenous |
| UMSS | University of Michigan Sedation Scale |
| NP | Nasopharynx |
| RG | Retroglossal |
| AP | Anterior-Posterior |
| TX | Transverse |
| BMI | Body Mass Index |
| IQR | Interquartile Range |
| CI | Confidence Interval |
References
- Mason, K.P.; Lerman, J. Review article: Dexmedetomidine in children: Current knowledge and future applications. Anesth. Analg. 2011, 113, 1129–1142. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, M.; Mason, K.P. Dexmedetomidine: Review, update, and future considerations of paediatric perioperative and periprocedural applications and limitations. Br. J. Anaesth. 2015, 115, 171–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoud, M.; Barbi, E.; Mason, K.P. Dexmedetomidine: What’s New for Pediatrics? A Narrative Review. J. Clin. Med. 2020, 9, 2724. [Google Scholar] [CrossRef] [PubMed]
- Sanders, R.D.; Xu, J.; Shu, Y.; Januszewski, A.; Halder, S.; Fidalgo, A.; Sun, P.; Hossain, M.; Ma, D.; Maze, M. Dexmedetomidine attenuates isoflurane-induced neurocognitive impairment in neonatal rats. Anesthesiology 2009, 110, 1077–1085. [Google Scholar] [CrossRef] [Green Version]
- Sanders, R.D.; Sun, P.; Patel, S.; Li, M.; Maze, M.; Ma, D. Dexmedetomidine provides cortical neuroprotection: Impact on anaesthetic-induced neuroapoptosis in the rat developing brain. Acta Anaesthesiol. Scand. 2010, 54, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zeng, M.; Chen, W.; Liu, C.; Wang, F.; Han, X.; Zuo, Z.; Peng, S. Dexmedetomidine reduces isoflurane-induced neuroapoptosis partly by preserving PI3K/Akt pathway in the hippocampus of neonatal rats. PLoS ONE 2014, 9, e93639. [Google Scholar] [CrossRef]
- Tachibana, K.; Hashimoto, T.; Kato, R.; Uchida, Y.; Ito, R.; Takita, K.; Morimoto, Y. Neonatal administration with dexmedetomidine does not impair the rat hippocampal synaptic plasticity later in adulthood. Paediatr. Anaesth. 2012, 22, 713–719. [Google Scholar] [CrossRef]
- Alhashemi, J.A. Dexmedetomidine vs midazolam for monitored anaesthesia care during cataract surgery. Br. J. Anaesth. 2006, 96, 722–726. [Google Scholar] [CrossRef] [Green Version]
- Jalowiecki, P.; Rudner, R.; Gonciarz, M.; Kawecki, P.; Petelenz, M.; Dziurdzik, P. Sole use of dexmedetomidine has limited utility for conscious sedation during outpatient colonoscopy. Anesthesiology 2005, 103, 269–273. [Google Scholar] [CrossRef]
- Munro, H.M.; Tirotta, C.F.; Felix, D.E.; Lagueruela, R.G.; Madril, D.R.; Zahn, E.M.; Nykanen, D.G. Initial experience with dexmedetomidine for diagnostic and interventional cardiac catheterization in children. Paediatr. Anaesth. 2007, 17, 109–112. [Google Scholar] [CrossRef]
- Char, D.; Drover, D.R.; Motonaga, K.S.; Gupta, S.; Miyake, C.Y.; Dubin, A.M.; Hammer, G.B. The effects of ketamine on dexmedetomidine-induced electrophysiologic changes in children. Paediatr. Anaesth. 2013, 23, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Kandil, A.; Subramanyam, R.; Hossain, M.M.; Ishman, S.; Shott, S.; Tewari, A.; Mahmoud, M. Comparison of the combination of dexmedetomidine and ketamine to propofol or propofol/sevoflurane for drug-induced sleep endoscopy in children. Paediatr. Anaesth. 2016, 26, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Koruk, S.; Mizrak, A.; Gul, R.; Kilic, E.; Yendi, F.; Oner, U. Dexmedetomidine-ketamine and midazolam-ketamine combinations for sedation in pediatric patients undergoing extracorporeal shock wave lithotripsy: A randomized prospective study. J. Anesth. 2010, 24, 858–863. [Google Scholar] [CrossRef] [PubMed]
- McVey, J.D.; Tobias, J.D. Dexmedetomidine and ketamine for sedation during spinal anesthesia in children. J. Clin. Anesth. 2010, 22, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Zor, F.; Ozturk, S.; Bilgin, F.; Isik, S.; Cosar, A. Pain relief during dressing changes of major adult burns: Ideal analgesic combination with ketamine. Burn. J. Int. Soc. Burn. Inj. 2010, 36, 501–505. [Google Scholar] [CrossRef]
- Shank, E.S.; Sheridan, R.L.; Ryan, C.M.; Keaney, T.J.; Martyn, J.A.J. Hemodynamic responses to dexmedetomidine in critically injured intubated pediatric burned patients: A preliminary study. J. Burn. Care Res. Off. Publ. Am. Burn. Assoc. 2013, 34, 311–317. [Google Scholar] [CrossRef]
- Barton, K.P.; Munoz, R.; Morell, V.O.; Chrysostomou, C. Dexmedetomidine as the primary sedative during invasive procedures in infants and toddlers with congenital heart disease. Pediatr. Crit. Care Med. J. Soc. Crit. Care Med. World Fed. Pediatr. Intensive Crit. Care Soc. 2008, 9, 612–615. [Google Scholar] [CrossRef]
- Mahmoud, M.; Radhakrishman, R.; Gunter, J.; Sadhasivam, S.; Schapiro, A.; McAuliffe, J.; Kurth, D.; Wang, Y.; Nick, T.G.; Donnelly, L.F. Effect of increasing depth of dexmedetomidine anesthesia on upper airway morphology in children. Paediatr. Anaesth. 2010, 20, 506–515. [Google Scholar] [CrossRef]
- Mahmoud, M.; Jung, D.; Salisbury, S.; McAuliffe, J.; Gunter, J.; Patio, M.; Donnelly, L.F.; Fleck, R. Effect of increasing depth of dexmedetomidine and propofol anesthesia on upper airway morphology in children and adolescents with obstructive sleep apnea. J. Clin. Anesth. 2013, 25, 529–541. [Google Scholar] [CrossRef]
- Mahmoud, M.; Ishman, S.L.; McConnell, K.; Fleck, R.; Shott, S.; Mylavarapu, G.; Gutmark, E.; Zou, Y.; Szczesniak, R.; Amin, R.S. Upper Airway Reflexes are Preserved During Dexmedetomidine Sedation in Children With Down Syndrome and Obstructive Sleep Apnea. J. Clin. Sleep Med. Jcsm Off. Publ. Am. Acad. Sleep Med. 2017, 13, 721–727. [Google Scholar] [CrossRef] [Green Version]
- Mahmoud, M.; Gunter, J.; Donnelly, L.F.; Wang, Y.; Nick, T.G.; Sadhasivam, S. A comparison of dexmedetomidine with propofol for magnetic resonance imaging sleep studies in children. Anesth. Analg. 2009, 109, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Malviya, S.; Voepel-Lewis, T.; Tait, A.R.; Merkel, S.; Tremper, K.; Naughton, N. Depth of sedation in children undergoing computed tomography: Validity and reliability of the University of Michigan Sedation Scale (UMSS). Br. J. Anaesth. 2002, 88, 241–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleck, R.J.; Shott, S.R.; Mahmoud, M.; Ishman, S.L.; Amin, R.S.; Donnelly, L.F. Magnetic resonance imaging of obstructive sleep apnea in children. Pediatr. Radiol. 2018, 48, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.; Bischof, L. Seeded region growing. IEEE Trans. Pattern Anal. Mach. Intell. 1994, 16, 641–647. [Google Scholar] [CrossRef] [Green Version]
- Evans, R.G.; Crawford, M.W.; Noseworthy, M.D.; Yoo, S.J. Effect of increasing depth of propofol anesthesia on upper airway configuration in children. Anesthesiology 2003, 99, 596–602. [Google Scholar] [CrossRef]
- Remmers, J.E.; deGroot, W.J.; Sauerland, E.K.; Anch, A.M. Pathogenesis of upper airway occlusion during sleep. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1978, 44, 931–938. [Google Scholar] [CrossRef]
- Eikermann, M.; Malhotra, A.; Fassbender, P.; Zaremba, S.; Jordan, A.S.; Gautam, S.; White, D.P.; Chamberlin, N.L. Differential effects of isoflurane and propofol on upper airway dilator muscle activity and breathing. Anesthesiology 2008, 108, 897–906. [Google Scholar] [CrossRef] [Green Version]
- Eikermann, M.; Fassbender, P.; Zaremba, S.; Jordan, A.S.; Rosow, C.; Malhotra, A.; Chamberlin, N.L. Pentobarbital dose-dependently increases respiratory genioglossus muscle activity while impairing diaphragmatic function in anesthetized rats. Anesthesiology 2009, 110, 1327–1334. [Google Scholar] [CrossRef] [Green Version]
- Eikermann, M.; Eckert, D.J.; Chamberlin, N.L.; Jordan, A.S.; Zaremba, S.; Smith, S.; Rosow, C.; Malhotra, A. Effects of pentobarbital on upper airway patency during sleep. Eur. Respir. J. 2010, 36, 569–576. [Google Scholar] [CrossRef]
- Lakhlani, P.P.; MacMillan, L.B.; Guo, T.Z.; McCool, B.A.; Lovinger, D.M.; Maze, M.; Limbird, L.E. Substitution of a mutant alpha2a-adrenergic receptor via “hit and run” gene targeting reveals the role of this subtype in sedative, analgesic, and anesthetic-sparing responses in vivo. Proc. Natl. Acad. Sci. USA 1997, 94, 9950–9955. [Google Scholar] [CrossRef] [Green Version]
- Correa-Sales, C.; Rabin, B.C.; Maze, M. A hypnotic response to dexmedetomidine, an alpha 2 agonist, is mediated in the locus coeruleus in rats. Anesthesiology 1992, 76, 948–952. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.P.; O’Mahony, E.; Zurakowski, D.; Libenson, M.H. Effects of dexmedetomidine sedation on the EEG in children. Paediatr. Anaesth. 2009, 19, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Huupponen, E.; Maksimow, A.; Lapinlampi, P.; Särkelä, M.; Saastamoinen, A.; Snapir, A.; Scheinin, H.; Scheinin, M.; Meriläinen, P.; Himanen, S.L.; et al. Electroencephalogram spindle activity during dexmedetomidine sedation and physiological sleep. Acta Anaesthesiol. Scand. 2008, 52, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.C.; Jamin, C.T.; Elamin, E.M. Continuous intravenous infusion of ketamine for maintenance sedation. Minerva Anestesiol. 2011, 77, 812–820. [Google Scholar]
- Eikermann, M.; Grosse-Sundrup, M.; Zaremba, S.; Henry, M.E.; Bittner, E.A.; Hoffmann, U.; Chamberlin, N.L. Ketamine activates breathing and abolishes the coupling between loss of consciousness and upper airway dilator muscle dysfunction. Anesthesiology 2012, 116, 35–46. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Nelson, L.E.; Franks, N.; Maze, M.; Chamberlin, N.L.; Saper, C.B. Role of endogenous sleep-wake and analgesic systems in anesthesia. J. Comp. Neurol. 2008, 508, 648–662. [Google Scholar] [CrossRef] [Green Version]
- Mishima, G.; Sanuki, T.; Sato, S.; Kobayashi, M.; Kurata, S.; Ayuse, T. Upper-airway collapsibility and compensatory responses under moderate sedation with ketamine, dexmedetomidine, and propofol in healthy volunteers. Physiol. Rep. 2020, 8, e14439. [Google Scholar] [CrossRef]
- Sherwin, C.M.T.; Stockmann, C.; Grimsrud, K.; Herd, D.W.; Anderson, B.J.; Spigarelli, M.G. Development of an optimal sampling schedule for children receiving ketamine for short-term procedural sedation and analgesia. Paediatr. Anaesth. 2015, 25, 211–216. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mylavarapu, G.; Fleck, R.J.; Ok, M.S.; Ding, L.; Kandil, A.; Amin, R.S.; Das, B.; Mahmoud, M. Effects on the Upper Airway Morphology with Intravenous Addition of Ketamine after Dexmedetomidine Administration in Normal Children. J. Clin. Med. 2020, 9, 3723. https://doi.org/10.3390/jcm9113723
Mylavarapu G, Fleck RJ, Ok MS, Ding L, Kandil A, Amin RS, Das B, Mahmoud M. Effects on the Upper Airway Morphology with Intravenous Addition of Ketamine after Dexmedetomidine Administration in Normal Children. Journal of Clinical Medicine. 2020; 9(11):3723. https://doi.org/10.3390/jcm9113723
Chicago/Turabian StyleMylavarapu, Goutham, Robert J. Fleck, Michale S. Ok, Lili Ding, Ali Kandil, Raouf S. Amin, Bobby Das, and Mohamed Mahmoud. 2020. "Effects on the Upper Airway Morphology with Intravenous Addition of Ketamine after Dexmedetomidine Administration in Normal Children" Journal of Clinical Medicine 9, no. 11: 3723. https://doi.org/10.3390/jcm9113723
APA StyleMylavarapu, G., Fleck, R. J., Ok, M. S., Ding, L., Kandil, A., Amin, R. S., Das, B., & Mahmoud, M. (2020). Effects on the Upper Airway Morphology with Intravenous Addition of Ketamine after Dexmedetomidine Administration in Normal Children. Journal of Clinical Medicine, 9(11), 3723. https://doi.org/10.3390/jcm9113723