Association between a Deficit Accumulation Frailty Index and Mobility Outcomes in Older Adults: Secondary Analysis of the Lifestyle Interventions and Independence for Elders (LIFE) Study



Abstract
:1. Introduction
2. Methods
2.1. LIFE Study Overview
2.2. Intervention
2.3. Follow-Up Visits and Outcome Assessment
2.4. Deficit Accumulation Frailty Index Development
2.5. Statistical Analysis
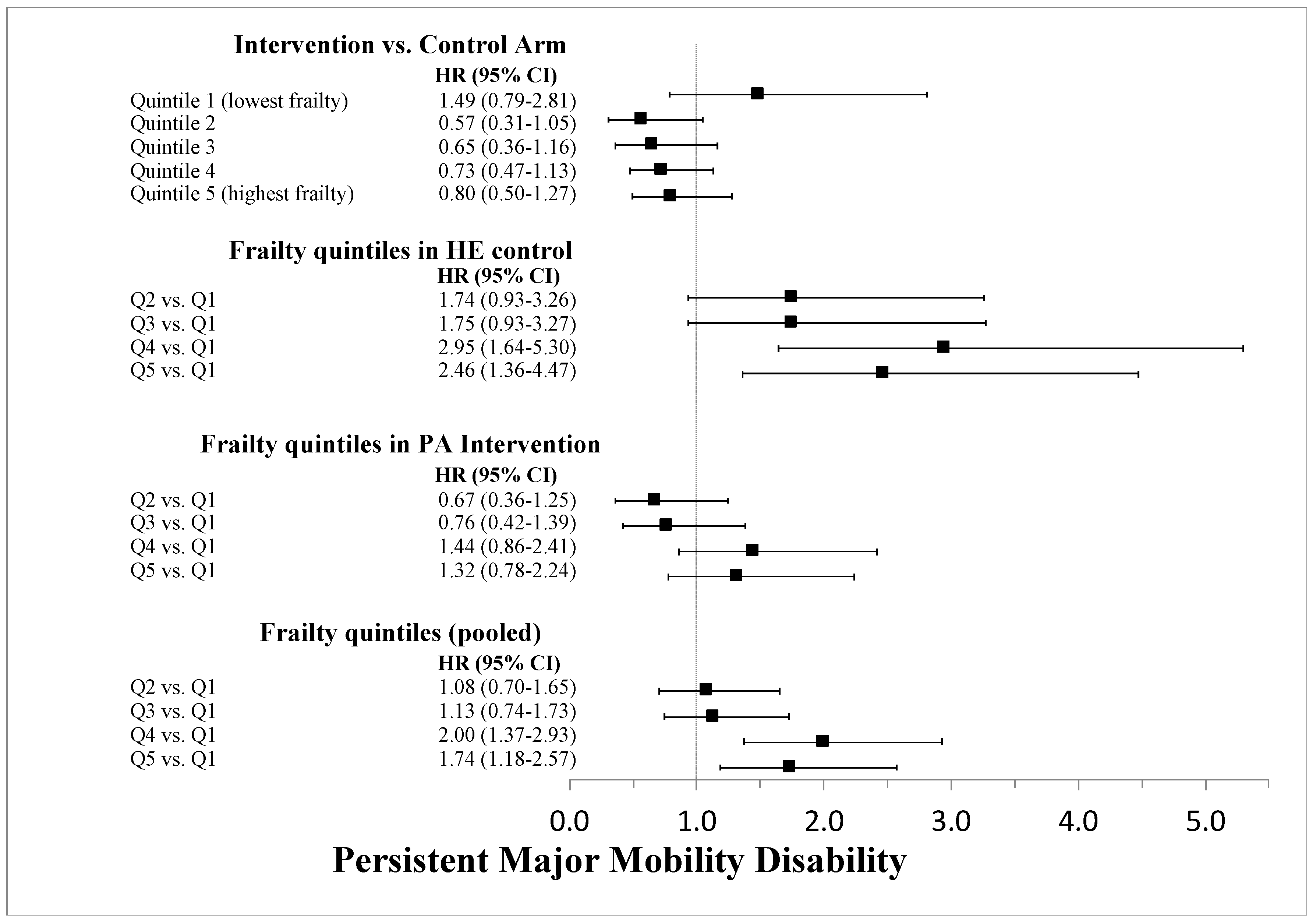
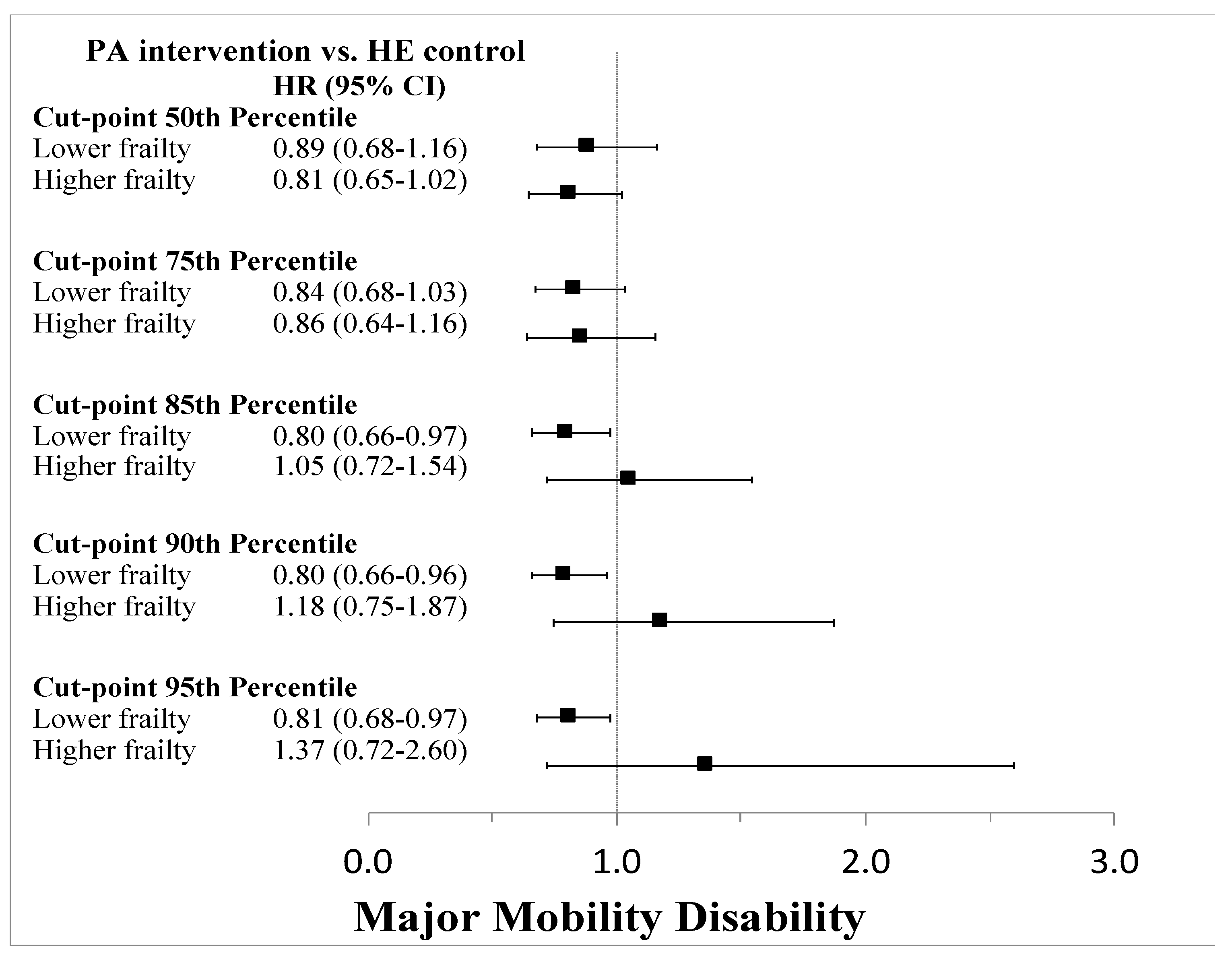
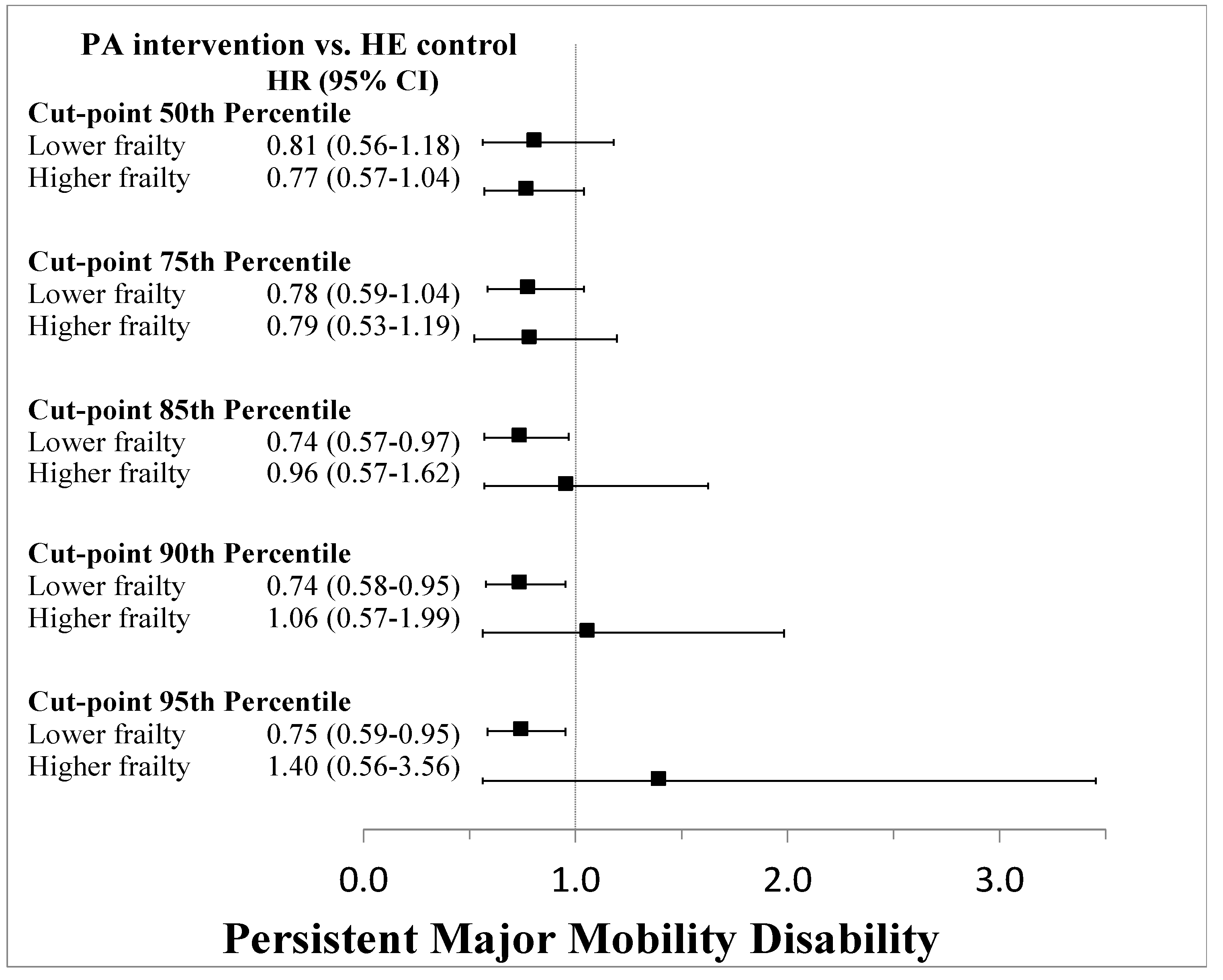
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dent, E.; Kowal, P.; Hoogendijk, E.O. Frailty measurement in research and clinical practice: A review. Eur. J. Intern. Med. 2016, 31, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Can. Med. Assoc. J. 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K.; Mitnitski, A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin. Geriatr. Med. 2011, 27, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Andrew, M.; Mitnitski, A. A comparison of two approaches to measuring frailty in elderly people. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 738–743. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theou, O.; Cann, L.; Blodgett, J.; Wallace, L.M.; Brothers, T.D.; Rockwood, K. Modifications to the frailty phenotype criteria: Systematic review of the current literature and investigation of 262 frailty phenotypes in the Survey of Health, Ageing, and Retirement in Europe. Ageing Res. Rev. 2015, 21, 78–94. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Glynn, R.J.; Avorn, J.; Lipsitz, L.A.; Rockwood, K.; Pawar, A.; Schneeweiss, S. Validation of a Claims-Based Frailty Index Against Physical Performance and Adverse Health Outcomes in the Health and Retirement Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 74, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Schneeweiss, S.; Glynn, R.J.; Lipsitz, L.A.; Rockwood, K.; Avorn, J. Measuring Frailty in Medicare Data: Development and Validation of a Claims-Based Frailty Index. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Pahor, M.; Guralnik, J.M.; Anton, S.D.; Ambrosius, W.T.; Blair, S.N.; Church, T.S.; Espeland, M.A.; Fielding, R.A.; Gill, T.M.; Glynn, N.W.; et al. Impact and Lessons from the Lifestyle Interventions and Independence for Elders (LIFE) Clinical Trials of Physical Activity to Prevent Mobility Disability. J. Am. Geriatr. Soc. 2020, 68, 872–881. [Google Scholar] [CrossRef] [PubMed]
- Pahor, M.; Guralnik, J.M.; Ambrosius, W.T.; Blair, S.; Bonds, D.E.; Church, T.S.; Espeland, M.A.; Fielding, R.A.; Gill, T.M.; Groessl, E.J.; et al. Effect of structured physical activity on prevention of major mobility disability in older adults: The LIFE study randomized clinical trial. JAMA 2014, 311, 2387–2396. [Google Scholar] [CrossRef] [PubMed]
- Trombetti, A.; Hars, M.; Hsu, F.C.; Reid, K.F.; Church, T.S.; Gill, T.M.; King, A.C.; Liu, C.K.; Manini, T.M.; McDermott, M.M.; et al. Effect of Physical activity on frailty: Secondary analysis of a randomized controlled trial. Ann. Intern. Med. 2018, 168, 309–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fielding, R.A.; Rejeski, W.J.; Blair, S.; Church, T.; Espeland, M.A.; Gill, T.M.; Guralnik, J.M.; Hsu, F.C.; Katula, J.; King, A.C.; et al. The Lifestyle Interventions and Independence for Elders Study: Design and methods. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66, 1226–1237. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.P.; Lovato, L.C.; Glynn, N.W.; Kennedy, K.; Castro, C.; Domanchuk, K.; McDavitt, E.; Rodate, R.; Marsiske, M.; McGloin, J.; et al. Lifestyle interventions and independence for elders study: Recruitment and baseline characteristics. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contal, C.; O‘Quigley, J. An application of changepoint methods in studying the effect of age on survival in breast cancer. Comput. Stat. Data Anal. 1999, 30, 253–270. [Google Scholar] [CrossRef]
- Mandrekar, J. Biomedical statistics and informatics software packages: FINDCUT. Division of Biomedical Statistics and Informatics. Mayo Clinic Research. Available online: http://bioinformaticstools.mayo.edu/research/findcut/ (accessed on 15 April 2020).
- Cheng, Y.; Goodin, A.J.; Pahor, M.; Manini, T.; Brown, J.D. Healthcare utilization and physical functioning in older adults in the United States. J. Am. Geriatr. Soc. 2020, 68, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Fallah, N.; Mitnitski, A.; Searle, S.D.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. Transitions in frailty status in older adults in relation to mobility: A multistate modeling approach employing a deficit count. J. Am. Geriatr. Soc. 2011, 59, 524–529. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frailty Index Quintiles | Q1 (Least Frail) | Q2 | Q3 | Q4 | Q5 (Most Frail) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable Name | N/ mean | %/SD | N/ mean | %/SD | N/ mean | %/SD | N/ mean | %/SD | N/ mean | %/SD |
| PA intervention assignment | 179 | 54.7 | 158 | 48.6 | 163 | 49.5 | 165 | 50.5 | 168 | 51.4 |
| Age (years) | 79.4 | 5.3 | 79.1 | 5.1 | 78.5 | 5.3 | 78.9 | 5.3 | 78.5 | 5.1 |
| Education ≥ High school | 233 | 71.3 | 223 | 68.6 | 218 | 66.3 | 225 | 68.8 | 207 | 63.3 |
| Female gender | 178 | 54.4 | 215 | 66.2 | 229 | 69.6 | 239 | 73.1 | 245 | 74.9 |
| Race | ||||||||||
| Black | 67 | 20.6 | 57 | 17.7 | 63 | 19.6 | 41 | 12.6 | 55 | 17.2 |
| Other | 22 | 6.8 | 22 | 6.8 | 21 | 6.5 | 15 | 4.6 | 27 | 8.4 |
| White | 236 | 72.6 | 243 | 75.5 | 238 | 73.9 | 269 | 82.8 | 238 | 74.4 |
| Self-reported health status | ||||||||||
| Bad or poor health | 20 | 6.1 | 32 | 9.9 | 38 | 11.6 | 61 | 18.7 | 124 | 37.9 |
| Health worsened last 6 months | 15 | 4.6 | 21 | 6.5 | 23 | 7.0 | 45 | 13.8 | 59 | 18.0 |
| Past medical history | ||||||||||
| Overweight | 99 | 30.3 | 150 | 46.2 | 168 | 51.1 | 151 | 46.2 | 184 | 56.3 |
| High blood pressure | 190 | 58.1 | 215 | 66.2 | 236 | 71.7 | 250 | 76.5 | 264 | 80.7 |
| Heart attack | 12 | 3.7 | 20 | 6.2 | 24 | 7.3 | 41 | 12.5 | 65 | 19.9 |
| Heart failure | 9 | 2.8 | 9 | 2.8 | 13 | 4.0 | 28 | 8.6 | 41 | 12.5 |
| Stroke | 14 | 4.3 | 17 | 5.2 | 30 | 9.1 | 25 | 7.7 | 34 | 10.4 |
| Cancer | 62 | 19.0 | 62 | 19.1 | 80 | 24.3 | 82 | 25.1 | 106 | 32.4 |
| Diabetes | 50 | 15.3 | 79 | 24.3 | 85 | 25.8 | 103 | 31.5 | 135 | 41.3 |
| Broke hip | 20 | 6.1 | 16 | 4.9 | 16 | 4.9 | 7 | 2.1 | 22 | 6.7 |
| Arthritis | 28 | 8.6 | 53 | 16.3 | 67 | 20.4 | 67 | 20.5 | 107 | 32.7 |
| Back injury | 19 | 5.8 | 28 | 8.6 | 29 | 8.8 | 45 | 13.8 | 75 | 22.9 |
| Fainting | 6 | 1.8 | 13 | 4.0 | 18 | 5.5 | 23 | 7.0 | 45 | 13.8 |
| Anxiety | 32 | 9.8 | 47 | 14.5 | 70 | 21.3 | 109 | 33.3 | 174 | 53.2 |
| Fatigue | 59 | 18.0 | 134 | 41.2 | 162 | 49.2 | 223 | 68.2 | 277 | 84.7 |
| Decreased appetite | 19 | 5.8 | 28 | 8.6 | 34 | 10.3 | 62 | 19.0 | 89 | 27.2 |
| Insomnia | 38 | 11.6 | 72 | 22.2 | 88 | 26.8 | 136 | 41.6 | 168 | 51.4 |
| Dizziness | 21 | 6.4 | 49 | 15.1 | 53 | 16.1 | 89 | 27.2 | 135 | 41.3 |
| Muscle stiffness | 96 | 29.4 | 160 | 49.2 | 131 | 60.2 | 95 | 71.0 | 60 | 81.7 |
| Foot pain | 42 | 12.8 | 66 | 20.3 | 85 | 25.8 | 113 | 34.6 | 149 | 45.6 |
| Previous hospitalization | 8 | 2.5 | 22 | 6.8 | 17 | 5.2 | 31 | 9.5 | 56 | 17.1 |
| Angina | 15 | 4.6 | 27 | 8.3 | 34 | 10.3 | 37 | 11.3 | 75 | 22.9 |
| Transient ischemic attach | 19 | 5.8 | 34 | 10.5 | 53 | 16.1 | 55 | 16.8 | 83 | 25.4 |
| Physical assessments | ||||||||||
| CHAMPS | 21.2 | 35.5 | 18.8 | 35.0 | 18.2 | 33.8 | 16.9 | 32.8 | 10.4 | 26.4 |
| ADL limitations | 1.1 | 0.2 | 1.2 | 0.3 | 1.3 | 0.4 | 1.4 | 0.4 | 1.6 | 0.4 |
| IADL limitations | 1.0 | 0.1 | 1.1 | 0.2 | 1.1 | 0.3 | 1.1 | 0.3 | 1.3 | 0.4 |
| Gait speed (m/s) | 0.9 | 0.2 | 0.8 | 0.2 | 0.8 | 0.2 | 0.8 | 0.2 | 0.8 | 0.1 |
| Number of medications | 3.4 | 2.5 | 4.3 | 2.6 | 5.0 | 2.9 | 5.4 | 3.2 | 6.7 | 3.5 |
| Grip strength (kg) | 26.6 | 10.7 | 24.4 | 10.3 | 23.4 | 9.4 | 23.4 | 9.8 | 22.1 | 8.6 |
| Total steps at moderate pace | 1381.9 | 1467.4 | 1058.9 | 1143.7 | 948.4 | 1008.3 | 880.2 | 858.5 | 617.0 | 571.7 |
| SPPB score | 7.6 | 1.7 | 7.5 | 1.6 | 7.4 | 1.5 | 7.2 | 1.6 | 7.2 | 1.5 |
| SPPB Score | Gait Speed (m/s) | Grip Strength (kg) | |
|---|---|---|---|
| Pearson correlation coefficient (r) | −0.104 | −0.218 | −0.145 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, J.D.; Alipour-Haris, G.; Pahor, M.; Manini, T.M. Association between a Deficit Accumulation Frailty Index and Mobility Outcomes in Older Adults: Secondary Analysis of the Lifestyle Interventions and Independence for Elders (LIFE) Study. J. Clin. Med. 2020, 9, 3757. https://doi.org/10.3390/jcm9113757
Brown JD, Alipour-Haris G, Pahor M, Manini TM. Association between a Deficit Accumulation Frailty Index and Mobility Outcomes in Older Adults: Secondary Analysis of the Lifestyle Interventions and Independence for Elders (LIFE) Study. Journal of Clinical Medicine. 2020; 9(11):3757. https://doi.org/10.3390/jcm9113757
Chicago/Turabian StyleBrown, Joshua D., Golnoosh Alipour-Haris, Marco Pahor, and Todd M. Manini. 2020. "Association between a Deficit Accumulation Frailty Index and Mobility Outcomes in Older Adults: Secondary Analysis of the Lifestyle Interventions and Independence for Elders (LIFE) Study" Journal of Clinical Medicine 9, no. 11: 3757. https://doi.org/10.3390/jcm9113757
APA StyleBrown, J. D., Alipour-Haris, G., Pahor, M., & Manini, T. M. (2020). Association between a Deficit Accumulation Frailty Index and Mobility Outcomes in Older Adults: Secondary Analysis of the Lifestyle Interventions and Independence for Elders (LIFE) Study. Journal of Clinical Medicine, 9(11), 3757. https://doi.org/10.3390/jcm9113757