Assessing the Effectiveness of Pirfenidone in Idiopathic Pulmonary Fibrosis: Long-Term, Real-World Data from European IPF Registry (eurIPFreg)

 ,
,
Abstract
:1. Introduction
2. Objectives of the Study
- pts. with limited functional impairment (>80% predicted FVC at t0);
- pts. with stable disease or slow disease progression before treatment (<10% decline of predicted FVC p.a.);
- pts. with progressive disease prior to treatment (>10% decline in FVC p.a.);
- pts. progressing after start of treatment (>10% decline in FVC p.a.);
- pts. with different smoking history (“yes” for active or previous smoker, “no” for never smoked pts.);
- pts. younger and older than 60 years;
- pts. with Gender-Age-Physiology (GAP) composite scores I, II and III;
- change in individual slope prior to and after baseline (t0) of DLco (% predicted), Borg dyspnea scale (grades 0–10), and six-minute walking distance test (6MWD, meters);
- pts. surviving more than 24 months after the begin of treatment;
- survival analyses, presented by Kaplan–Meier curves;
3. Materials and Methods
4. Statistics
- Individual analysis: slopes and slope-changes were taken as estimated from each individual patient.
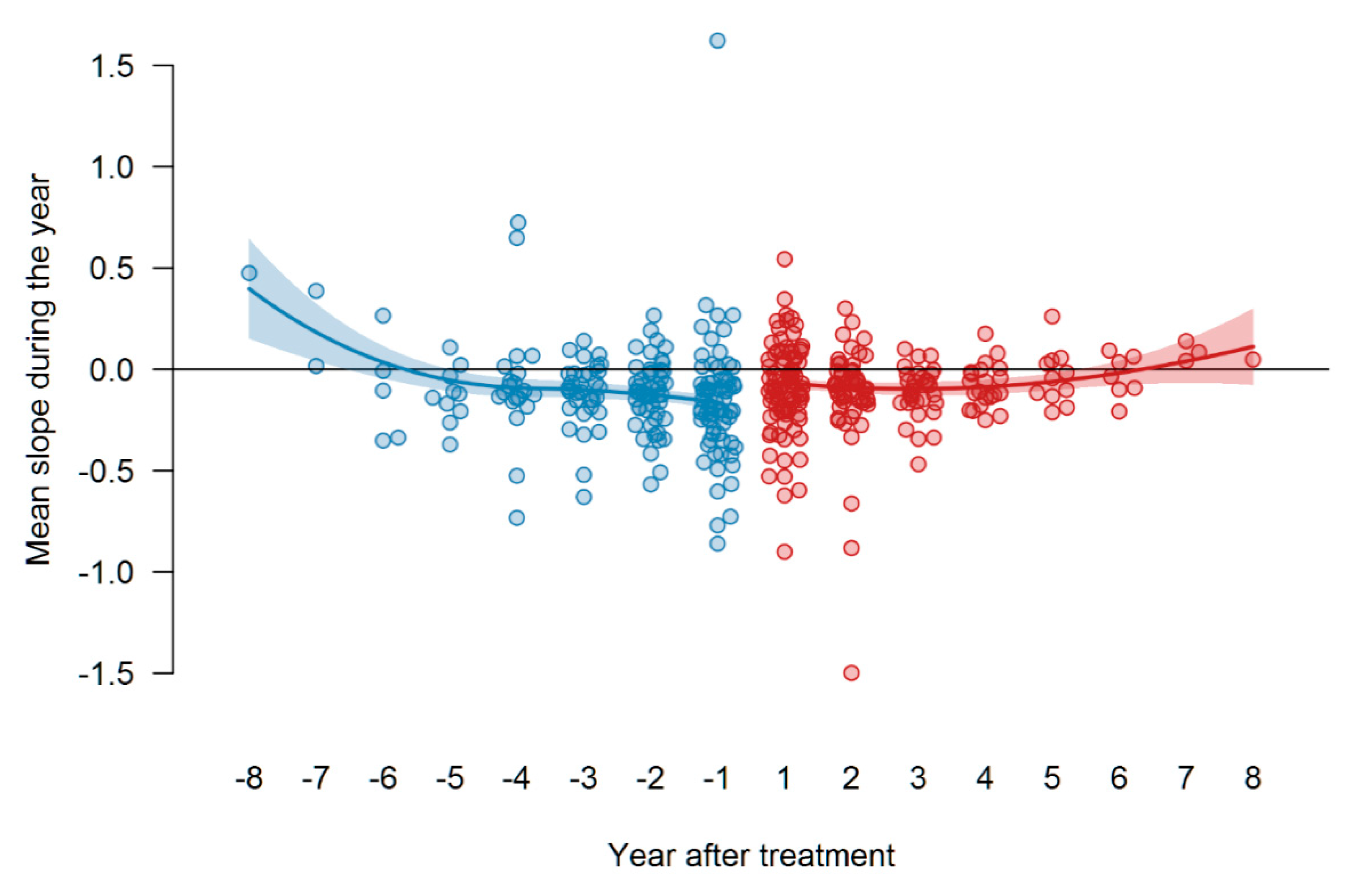
- Global analysis: the data from all patients were subtracted from the respective baseline values and then pooled. The pooled data was used to fit a global segmented regression model.
5. Results
5.1. Descriptive Characteristic of the IPF Cohort
5.2. Response to Treatment with Pirfenidone
5.2.1. Individual FVC Slope Analysis
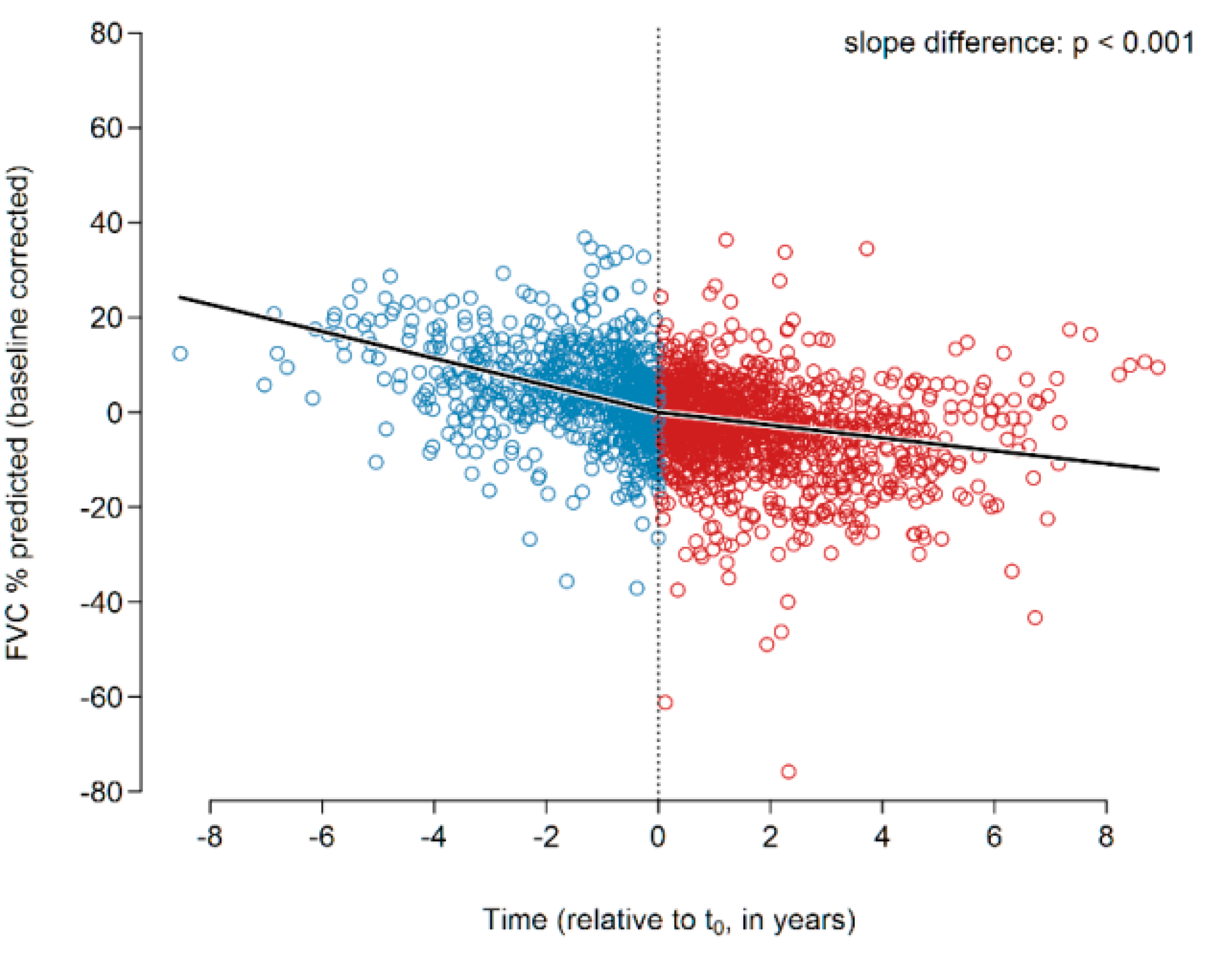
5.2.2. Global FVC Slope Analysis
5.2.3. Subgroup Analysis
Patients with Limited Functional Impairment (>80% Predicted FVC at t0)
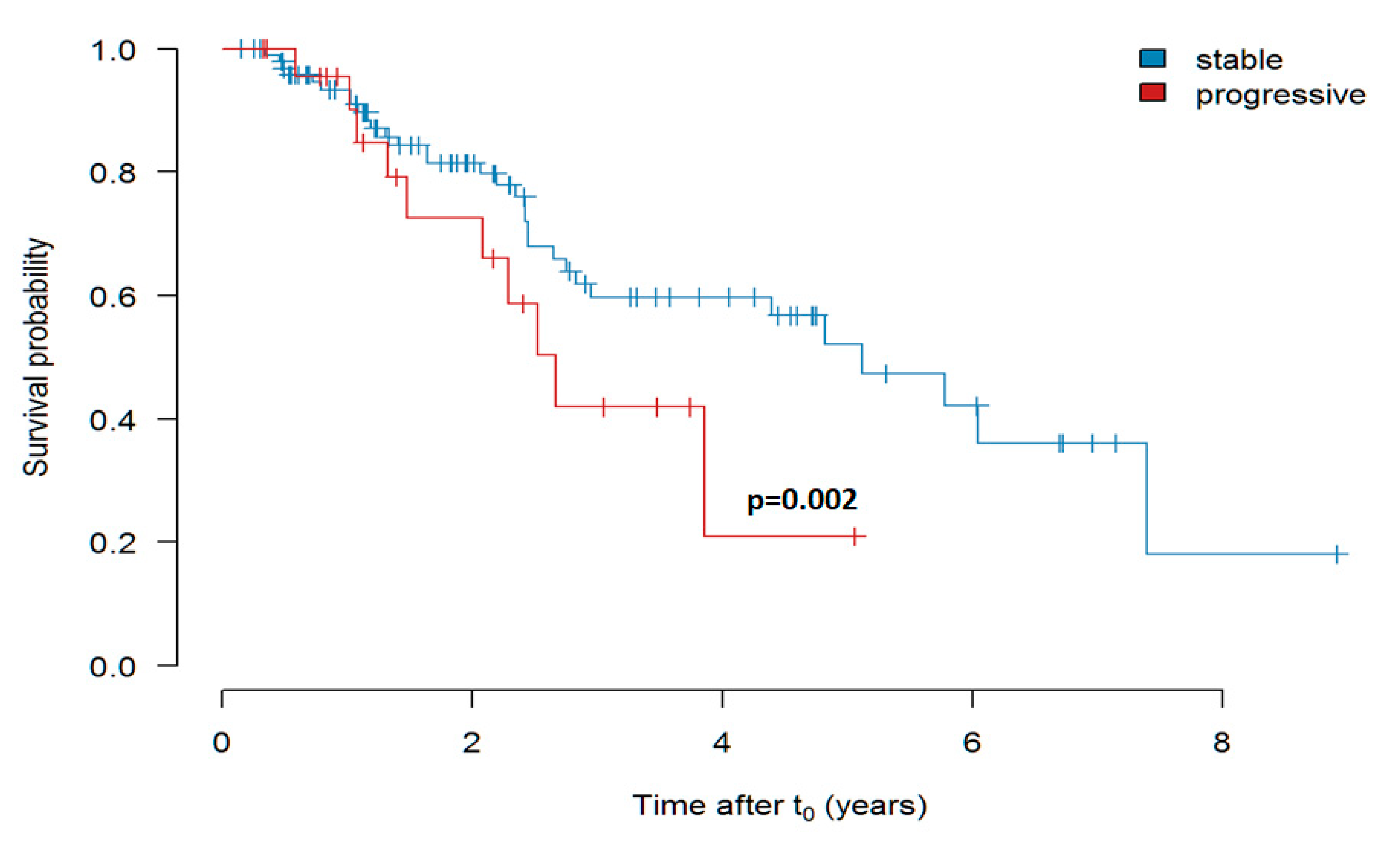
Response of Patients with Stable or Slow Progression versus Fast Progression before Treatment (>10% Decline of Predicted FVC p.a)
Patients Progressing after Start of Treatment (>10% Decline in FVC p.a.)
Never Smokers versus Patients with Smoking History
Patients Younger and Older than 60 Years
Patients with GAP Stages I, II and II
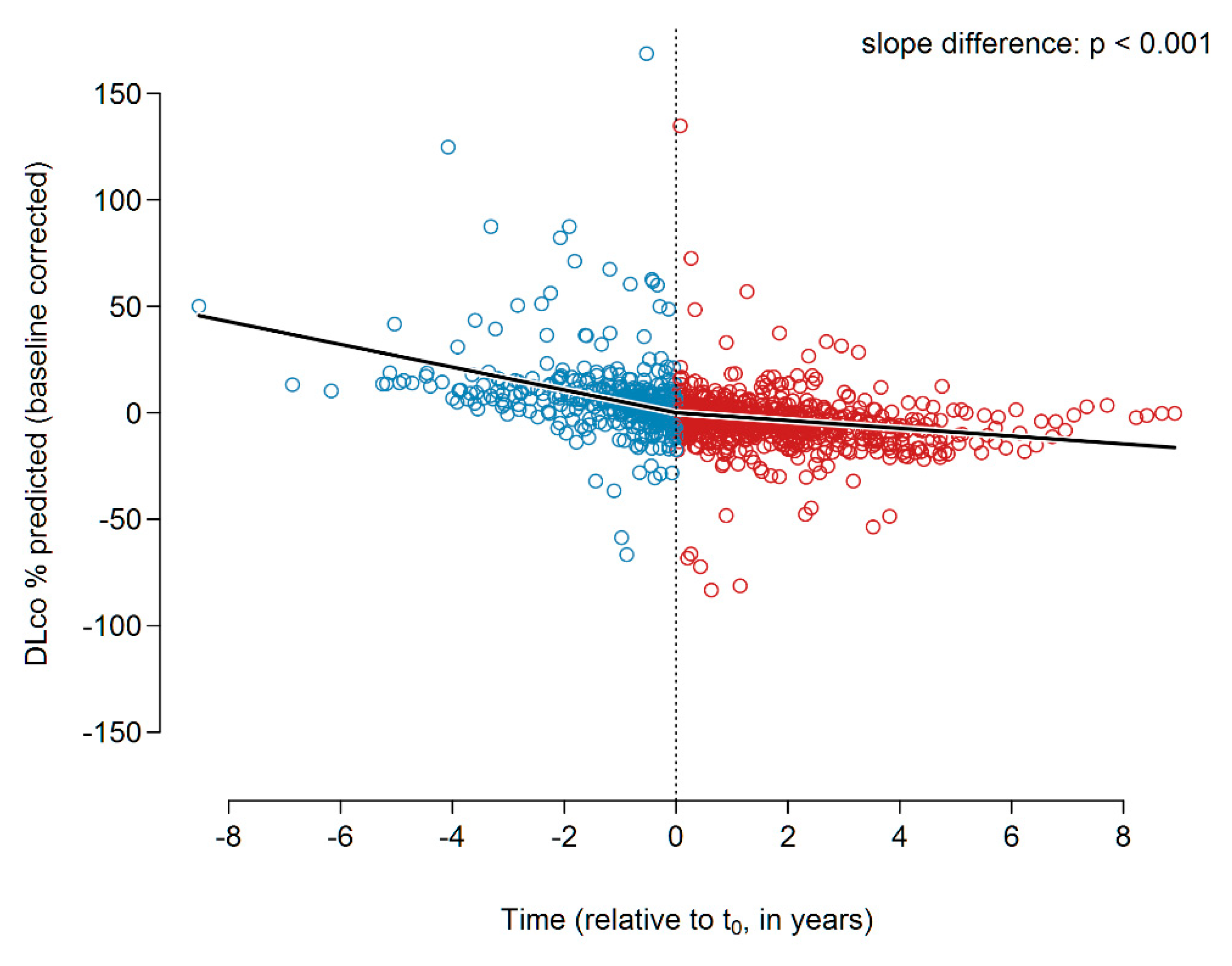
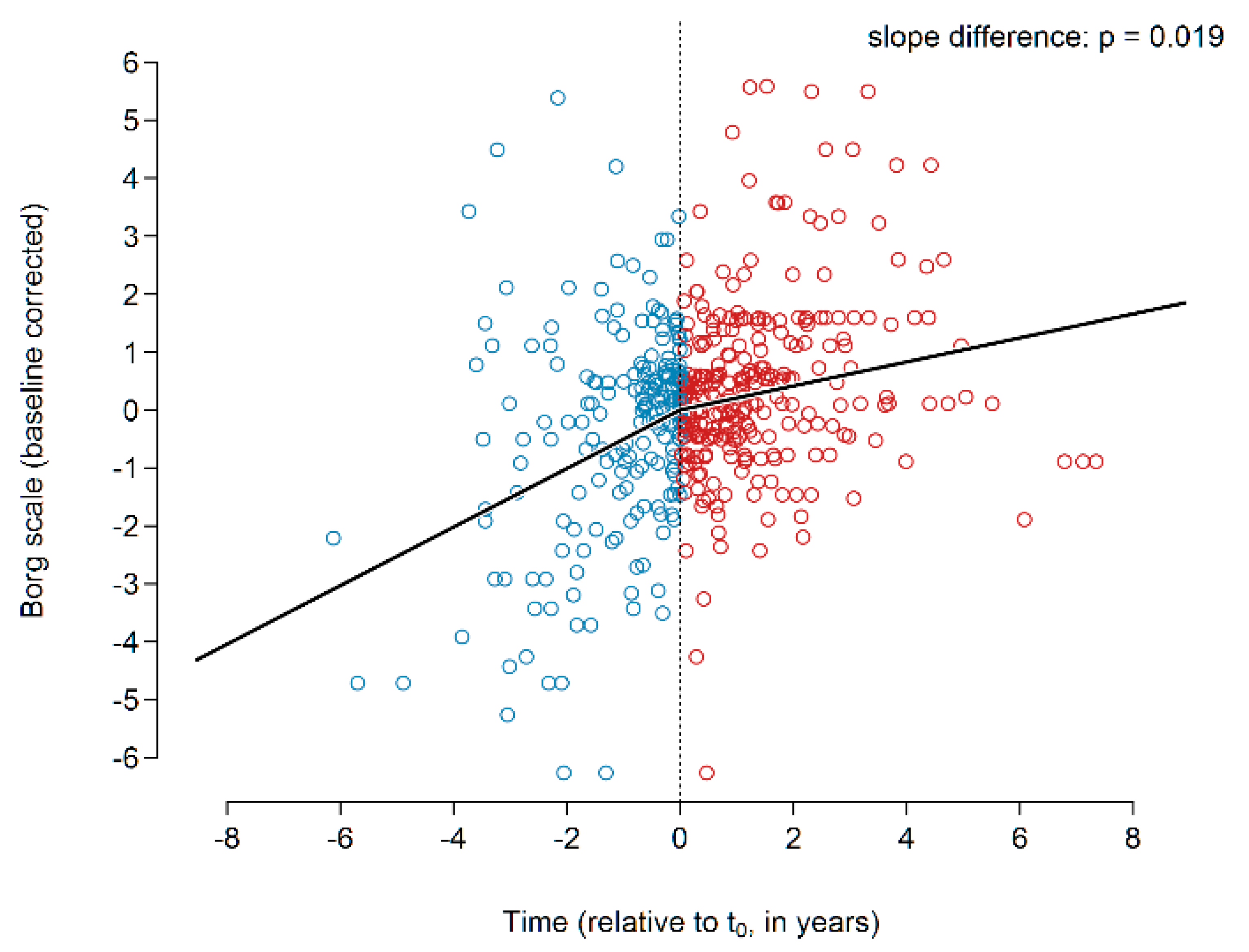
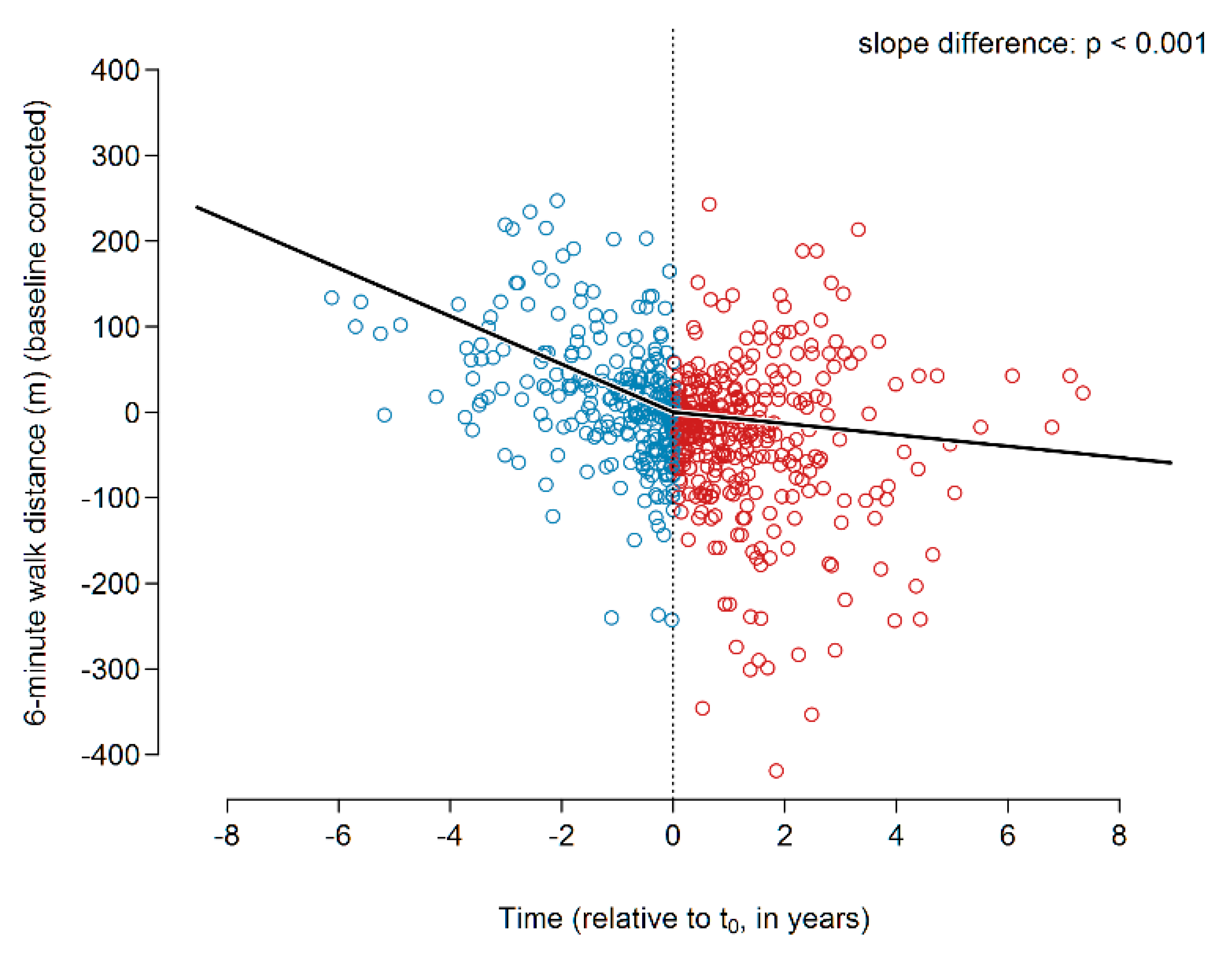
5.2.4. Change in Individual Slope Prior to and after t0 of DLco (% pred.), Borg Scale (Dyspnea Grade 1–6), and 6MWD (m)
DLco
Borg Dyspnea Scale
6MWD
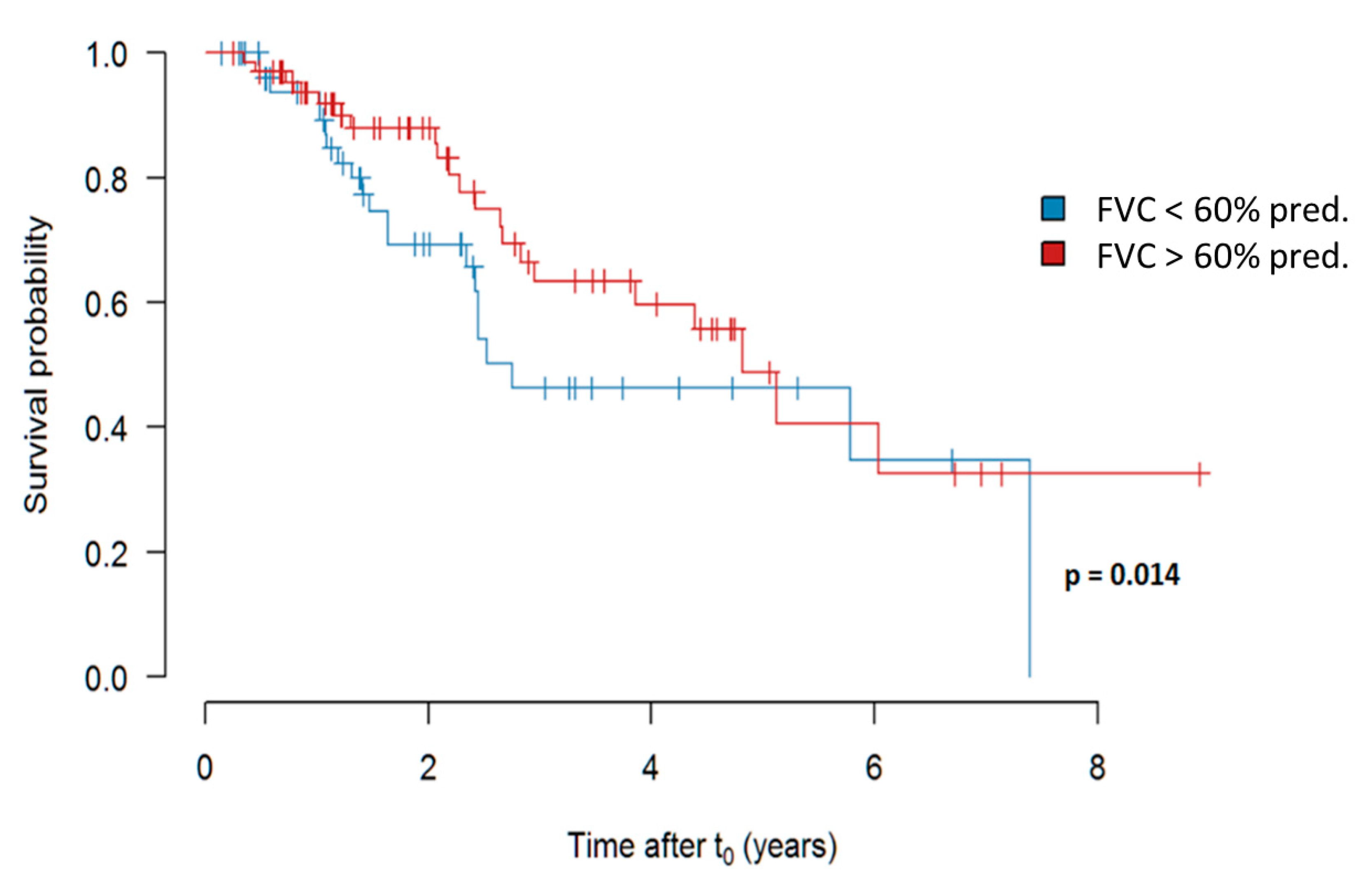
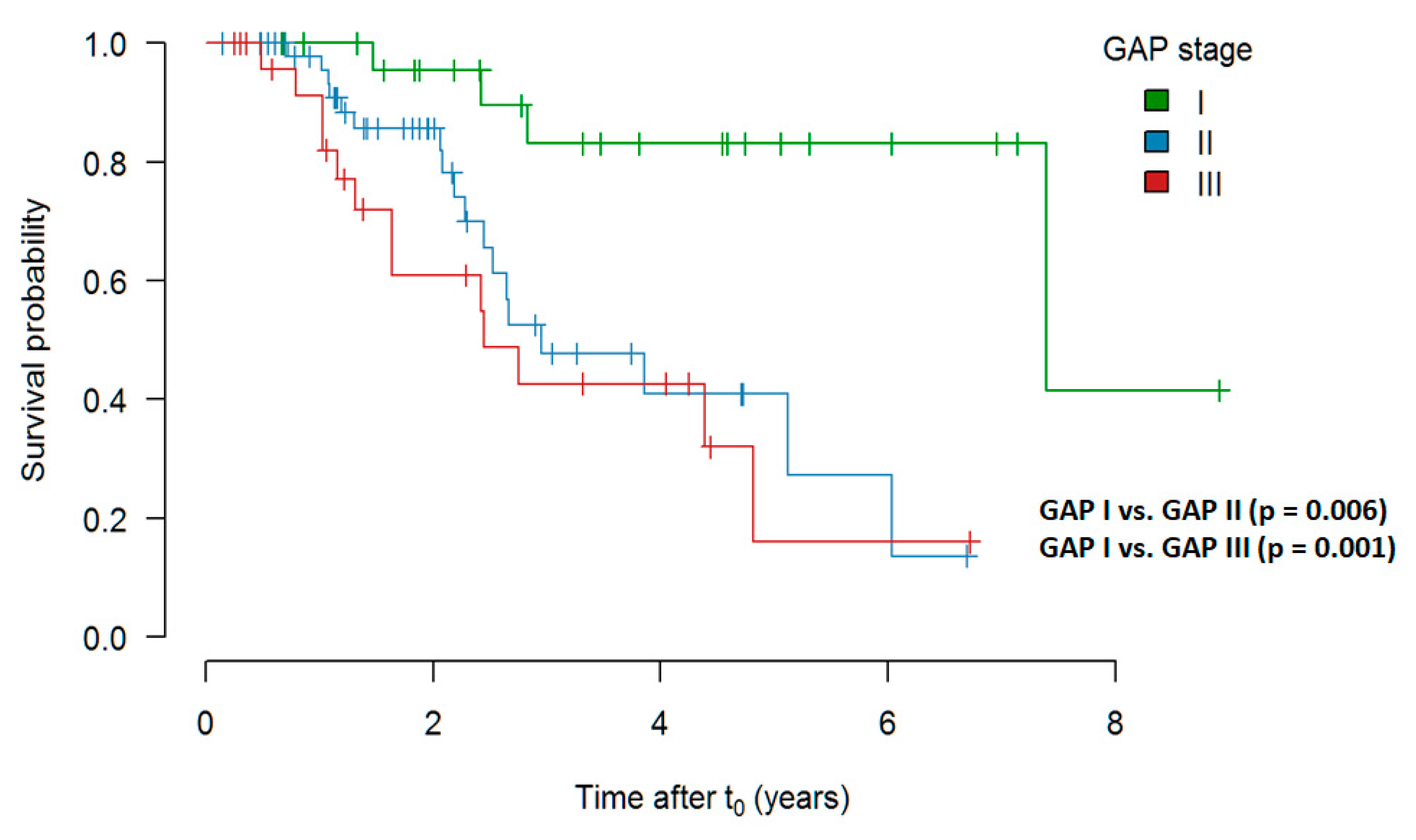
5.2.5. Survival Analysis, Presented by Kaplan–Meier Curves
Overall Survival
Survival in Dependency of the FVC Decline Prior to Treatment
Survival in Dependency of Age Prior to Initiation of Treatment
Survival in Dependency of the FVC at the Timepoint of Treatment Initiation
Survival Depending on GAP Stage at t0
Evaluation of a Risk Score Adjusted for FVC Decline, Age and GAP Prior to Initiation of Treatment
6. Discussion
7. Study Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Trial Registration
Take Home Message
Declarations: Ethics Approval and Consent to Participate
References
- Barratt, S.L.; Creamer, A.; Hayton, C.; Chaudhuri, N. Idiopathic Pulmonary Fibrosis (IPF): An Overview. J. Clin. Med. 2018, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolb, M.; Vašáková, M. The Natural History of Progressive Fibrosing Interstitial Lung Diseases. Respir. Res. 2019, 20, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krauss, E.; Gehrken, G.; Drakopanagiotakis, F.; Tello, S.; Dartsch, R.C.; Maurer, O.; Windhorst, A.; Beck, D. von der; Griese, M.; Seeger, W.; et al. Clinical characteristics of patients with familial idiopathic pulmonary fibrosis (f-IPF). BMC Pulm. Med. 2019, 19, 130. [Google Scholar] [CrossRef] [PubMed]
- Graney, B.A.; Lee, J.S. Impact of novel antifibrotic therapy on patient outcomes in idiopathic pulmonary fibrosis: Patient selection and perspectives. Patient Relat. Outcome Meas. 2018, 9, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Witt, S.; Krauss, E.; Barbero, M.A.N.; Müller, V.; Bonniaud, P.; Vancheri, C.; Wells, A.U.; Vasakova, M.; Pesci, A.; Klepetko, W.; et al. Psychometric properties and minimal important differences of SF-36 in Idiopathic Pulmonary Fibrosis. Respir. Res. 2019, 20, 47. [Google Scholar] [CrossRef] [Green Version]
- Collard, H.R.; Tino, G.; Noble, P.W.; Shreve, M.A.; Michaels, M.; Carlson, B.; Schwarz, M.I. Patient experiences with pulmonary fibrosis. Respir. Med. 2007, 101, 1350–1354. [Google Scholar] [CrossRef] [Green Version]
- Vietri, L.; Cameli, P.; Perruzza, M.; Cekorja, B.; Bergantini, L.; d’Alessandro, M.; Refini, R.M.; Pieroni, M.; Fossi, A.; Bennett, D.; et al. Pirfenidone in idiopathic pulmonary fibrosis: Real-life experience in the referral centre of Siena. Ther. Adv. Respir. Dis. 2020, 14, 1753466620906326. [Google Scholar] [CrossRef] [Green Version]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Lynch, D.A.; Sverzellati, N.; Travis, W.D.; Brown, K.K.; Colby, T.V.; Galvin, J.R.; Goldin, J.G.; Hansell, D.M.; Inoue, Y.; Johkoh, T.; et al. Diagnostic criteria for idiopathic pulmonary fibrosis: A Fleischner Society White Paper. Lancet Respir. Med. 2018, 6, 138–153. [Google Scholar] [CrossRef]
- Atsumi, K.; Saito, Y.; Kuse, N.; Kobayashi, K.; Tanaka, T.; Kashiwada, T.; Inomata, M.; Kokuho, N.; Hayashi, H.; Kamio, K.; et al. Prognostic Factors in the Acute Exacerbation of Idiopathic Pulmonary Fibrosis: A Retrospective Single-center Study. Intern. Med. 2018, 57, 655–661. [Google Scholar] [CrossRef] [Green Version]
- Clay, E.; Cristeau, O.; Chafaie, R.; Pinta, A.; Mazaleyrat, B.; Cottin, V. Cost-effectiveness of pirfenidone compared to all available strategies for the treatment of idiopathic pulmonary fibrosis in France. J. Mark. Access Health Policy 2019, 7, 1626171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krauss, E.; Froehler, M.; Degen, M.; Mahavadi, P.; Dartsch, R.C.; Korfei, M.; Ruppert, C.; Seeger, W.; Guenther, A. Exhalative Breath Markers Do Not Offer for Diagnosis of Interstitial Lung Diseases: Data from the European IPF Registry (eurIPFreg) and Biobank. J. Clin. Med. 2019, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loeh, B.; Brylski, L.T.; Beck, D. von der; Seeger, W.; Krauss, E.; Bonniaud, P.; Crestani, B.; Vancheri, C.; Wells, A.U.; Markart, P.; et al. Lung CT Densitometry in Idiopathic Pulmonary Fibrosis for the Prediction of Natural Course, Severity, and Mortality. Chest 2019, 155, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Drakopanagiotakis, F.; Wujak, L.; Wygrecka, M.; Markart, P. Biomarkers in idiopathic pulmonary fibrosis. Matrix Biol. 2018. [Google Scholar] [CrossRef]
- Krauss, E.; Haberer, J.; Maurer, O.; Barreto, G.; Drakopanagiotakis, F.; Degen, M.; Seeger, W.; Guenther, A. Exploring the Ability of Electronic Nose Technology to Recognize Interstitial Lung Diseases (ILD) by Non-Invasive Breath Screening of Exhaled Volatile Compounds (VOC): A Pilot Study from the European IPF Registry (eurIPFreg) and Biobank. J. Clin. Med. 2019, 8, 1698. [Google Scholar] [CrossRef]
- Guenther, A.; Krauss, E.; Tello, S.; Wagner, J.; Paul, B.; Kuhn, S.; Maurer, O.; Heinemann, S.; Costabel, U.; Barbero, M.A.N.; et al. The European IPF registry (eurIPFreg): Baseline characteristics and survival of patients with idiopathic pulmonary fibrosis. Respir. Res. 2018, 19, 141. [Google Scholar] [CrossRef] [Green Version]
- Culver, D.A.; Behr, J.; Belperio, J.A.; Corte, T.J.; de Andrade, J.A.; Flaherty, K.R.; Gulati, M.; Huie, T.J.; Lancaster, L.H.; Roman, J.; et al. Patient Registries in Idiopathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2019, 200, 160–167. [Google Scholar] [CrossRef]
- Fang, C.; Huang, H.; Guo, J.; Ferianc, M.; Xu, Z. Real-world experiences: Efficacy and tolerability of pirfenidone in clinical practice. PLoS ONE 2020, 15, e0228390. [Google Scholar] [CrossRef] [Green Version]
- Noble, P.W.; Albera, C.; Bradford, W.Z.; Costabel, U.; Du Bois, R.M.; Fagan, E.A.; Fishman, R.S.; Glaspole, I.; Glassberg, M.K.; Lancaster, L.; et al. Pirfenidone for idiopathic pulmonary fibrosis: Analysis of pooled data from three multinational phase 3 trials. Eur. Respir. J. 2016, 47, 243–253. [Google Scholar] [CrossRef]
- Taniguchi, H.; Ebina, M.; Kondoh, Y.; Ogura, T.; Azuma, A.; Suga, M.; Taguchi, Y.; Takahashi, H.; Nakata, K.; Sato, A.; et al. Pirfenidone in idiopathic pulmonary fibrosis. Eur. Respir. J. 2010, 35, 821–829. [Google Scholar] [CrossRef]
- King, T.E.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costabel, U.; Albera, C.; Lancaster, L.H.; Lin, C.-Y.; Hormel, P.; Hulter, H.N.; Noble, P.W. An Open-Label Study of the Long-Term Safety of Pirfenidone in Patients with Idiopathic Pulmonary Fibrosis (RECAP). Respiration 2017, 94, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Noble, P.W.; Albera, C.; Bradford, W.Z.; Costabel, U.; Glassberg, M.K.; Kardatzke, D.; King, T.E.; Lancaster, L.; Sahn, S.A.; Szwarcberg, J.; et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): Two randomised trials. Lancet 2011, 377, 1760–1769. [Google Scholar] [CrossRef]
- King, C.S.; Nathan, S.D. Idiopathic pulmonary fibrosis: Effects and optimal management of comorbidities. Lancet Respir. Med. 2017, 5, 72–84. [Google Scholar] [CrossRef]
- Neighbors, M.; Cabanski, C.R.; Ramalingam, T.R.; Sheng, X.R.; Tew, G.W.; Gu, C.; Jia, G.; Peng, K.; Ray, J.M.; Ley, B.; et al. Prognostic and predictive biomarkers for patients with idiopathic pulmonary fibrosis treated with pirfenidone: Post-hoc assessment of the CAPACITY and ASCEND trials. Lancet Respir. Med. 2018, 6, 615–626. [Google Scholar] [CrossRef]
- Costabel, U.; Albera, C.; Glassberg, M.K.; Lancaster, L.H.; Wuyts, W.A.; Petzinger, U.; Gilberg, F.; Kirchgaessler, K.-U.; Noble, P.W. Effect of Pirfenidone in Patients with More Advanced Idiopathic Pulmonary Fibrosis. Respir Res. 2019, 20, 55. [Google Scholar] [CrossRef] [Green Version]
- Tzouvelekis, A.; Ntolios, P.; Karampitsakos, T.; Tzilas, V.; Anevlavis, S.; Bouros, E.; Steiropoulos, P.; Koulouris, N.; Stratakos, G.; Froudarakis, M.; et al. Safety and efficacy of pirfenidone in severe Idiopathic Pulmonary Fibrosis: A real-world observational study. Pulm. Pharmacol. Ther. 2017, 46, 48–53. [Google Scholar] [CrossRef]
- Majewski, S.; Białas, A.J.; Buchczyk, M.; Gomółka, P.; Górska, K.; Jagielska-Len, H.; Jarzemska, A.; Jassem, E.; Jastrzębski, D.; Kania, A.; et al. A multicentre retrospective observational study on Polish experience of pirfenidone therapy in patients with idiopathic pulmonary fibrosis: The PolExPIR study. BMC Pulm. Med. 2020, 20, 122. [Google Scholar] [CrossRef]
- Bando, M.; Yamauchi, H.; Ogura, T.; Taniguchi, H.; Watanabe, K.; Azuma, A.; Homma, S.; Sugiyama, Y. Clinical Experience of the Long-term Use of Pirfenidone for Idiopathic Pulmonary Fibrosis. Intern. Med. 2016, 55, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Ley, B.; Swigris, J.; Day, B.-M.; Stauffer, J.L.; Raimundo, K.; Chou, W.; Collard, H.R. Pirfenidone Reduces Respiratory-related Hospitalizations in Idiopathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2017, 196, 756–761. [Google Scholar] [CrossRef]
- Lancaster, L.H.; Andrade, J.A. de; Zibrak, J.D.; Padilla, M.L.; Albera, C.; Nathan, S.D.; Wijsenbeek, M.S.; Stauffer, J.L.; Kirchgaessler, K.-U.; Costabel, U. Pirfenidone safety and adverse event management in idiopathic pulmonary fibrosis. Eur. Respir. Rev. 2017, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoniou, K.M.; Hansell, D.M.; Rubens, M.B.; Marten, K.; Desai, S.R.; Siafakas, N.M.; Nicholson, A.G.; Du Bois, R.M.; Wells, A.U. Idiopathic pulmonary fibrosis: Outcome in relation to smoking status. Am. J. Respir. Crit. Care Med. 2008, 177, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Zurkova, M.; Kriegova, E.; Kolek, V.; Lostakova, V.; Sterclova, M.; Bartos, V.; Doubkova, M.; Binkova, I.; Svoboda, M.; Strenkova, J.; et al. Effect of pirfenidone on lung function decline and survival: 5-yr experience from a real-life IPF cohort from the Czech EMPIRE registry. Respir. Res. 2019, 20, 16. [Google Scholar] [CrossRef] [PubMed]
- Nathan, S.D.; Albera, C.; Bradford, W.Z.; Costabel, U.; Glaspole, I.; Glassberg, M.K.; Kardatzke, D.R.; Daigl, M.; Kirchgaessler, K.-U.; Lancaster, L.H.; et al. Effect of pirfenidone on mortality: Pooled analyses and meta-analyses of clinical trials in idiopathic pulmonary fibrosis. Lancet Respir. Med. 2017, 5, 33–41. [Google Scholar] [CrossRef]
- Albera, C.; Costabel, U.; Fagan, E.A.; Glassberg, M.K.; Gorina, E.; Lancaster, L.; Lederer, D.J.; Nathan, S.D.; Spirig, D.; Swigris, J.J. Efficacy of pirfenidone in patients with idiopathic pulmonary fibrosis with more preserved lung function. Eur. Respir. J. 2016, 48, 843–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters at t0 | Pirfenidone Study Cohort |
|---|---|
| Patients in the analysis (n) | 122 |
| Male (%) | 73.2 |
| BMI (mean value ± SD (kg/m2)) | 28.3 ± 4.56 |
| Age at t0 (mean value ± SD (years)) | 67.2 ± 10.3 |
| Current smokers/previous smokers/never smoked (%) | 4.1%/ 64.8%/31.1% |
| Pack years (mean value ± SD) | 28.0 ± 21.0 |
| GAP Stage I/II/III (% of the whole cohort) | 21.1%/41.5%/21.1% (16.3% were missing values) |
| VC (% pred.; mean value ± SD) | 64.5 ± 17.5 |
| FVC (% pred.; mean value ± SD) | 63.0 ± 18.3 |
| DLco (% pred.; mean value ± SD) | 42.4 ± 20.4 |
| pO2 (mm Hg) at rest (mean value ± SD) | 67.6 ± 72.4 |
| pCO2 (mm Hg) at rest (mean value ± SD) | 33.5 ± 44.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krauss, E.; Tello, S.; Wilhelm, J.; Schmidt, J.; Stoehr, M.; Seeger, W.; Dartsch, R.C.; Crestani, B.; Guenther, A. Assessing the Effectiveness of Pirfenidone in Idiopathic Pulmonary Fibrosis: Long-Term, Real-World Data from European IPF Registry (eurIPFreg). J. Clin. Med. 2020, 9, 3763. https://doi.org/10.3390/jcm9113763
Krauss E, Tello S, Wilhelm J, Schmidt J, Stoehr M, Seeger W, Dartsch RC, Crestani B, Guenther A. Assessing the Effectiveness of Pirfenidone in Idiopathic Pulmonary Fibrosis: Long-Term, Real-World Data from European IPF Registry (eurIPFreg). Journal of Clinical Medicine. 2020; 9(11):3763. https://doi.org/10.3390/jcm9113763
Chicago/Turabian StyleKrauss, Ekaterina, Silke Tello, Jochen Wilhelm, Johanna Schmidt, Mark Stoehr, Werner Seeger, Ruth C. Dartsch, Bruno Crestani, and Andreas Guenther. 2020. "Assessing the Effectiveness of Pirfenidone in Idiopathic Pulmonary Fibrosis: Long-Term, Real-World Data from European IPF Registry (eurIPFreg)" Journal of Clinical Medicine 9, no. 11: 3763. https://doi.org/10.3390/jcm9113763
APA StyleKrauss, E., Tello, S., Wilhelm, J., Schmidt, J., Stoehr, M., Seeger, W., Dartsch, R. C., Crestani, B., & Guenther, A. (2020). Assessing the Effectiveness of Pirfenidone in Idiopathic Pulmonary Fibrosis: Long-Term, Real-World Data from European IPF Registry (eurIPFreg). Journal of Clinical Medicine, 9(11), 3763. https://doi.org/10.3390/jcm9113763