Changes in the Use of Fresh-Frozen Plasma Transfusions in Preterm Neonates: A Single Center Experience

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Guidelines
2.3. Outcome Measures
2.4. Statistical Analyses and Sample Size
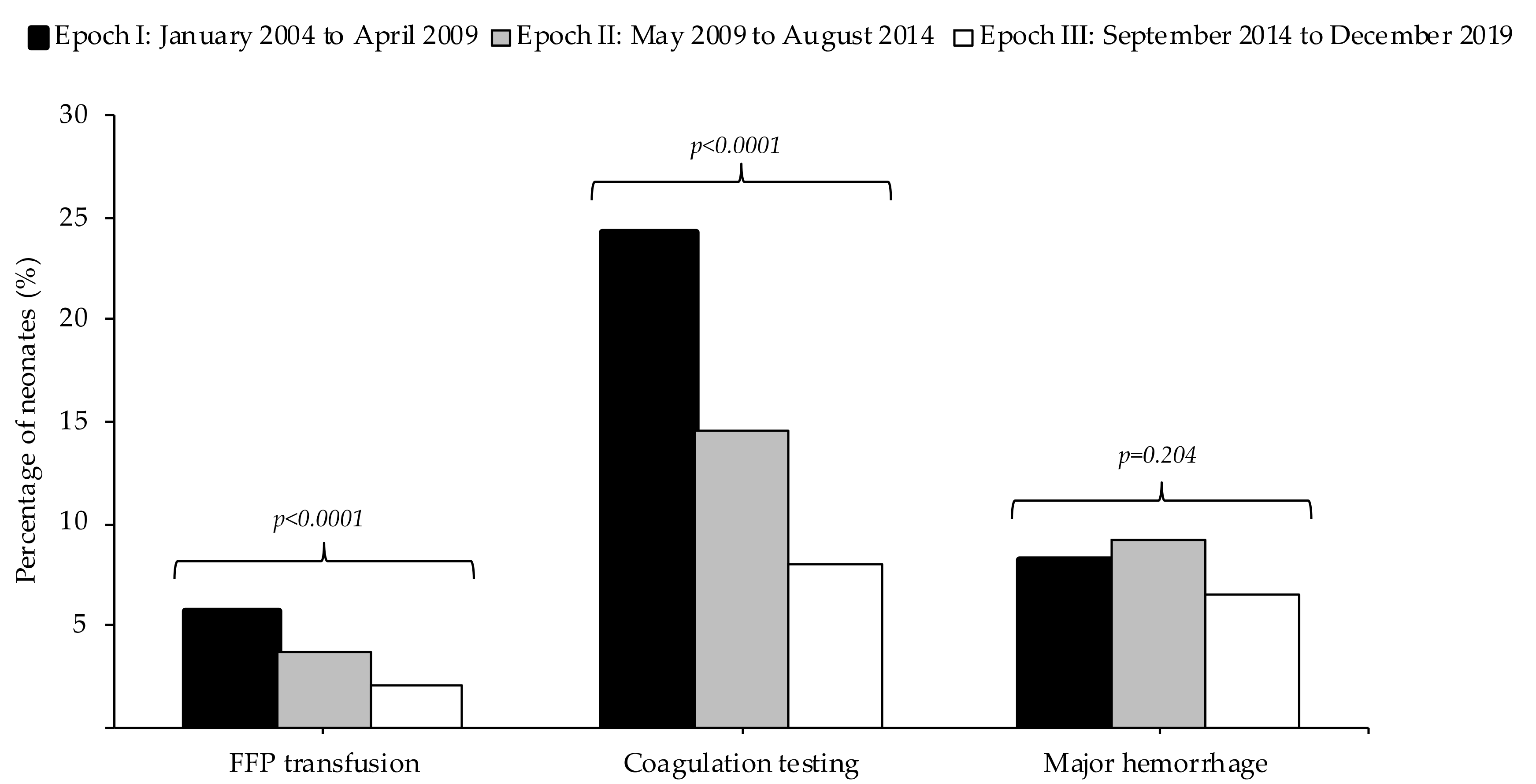
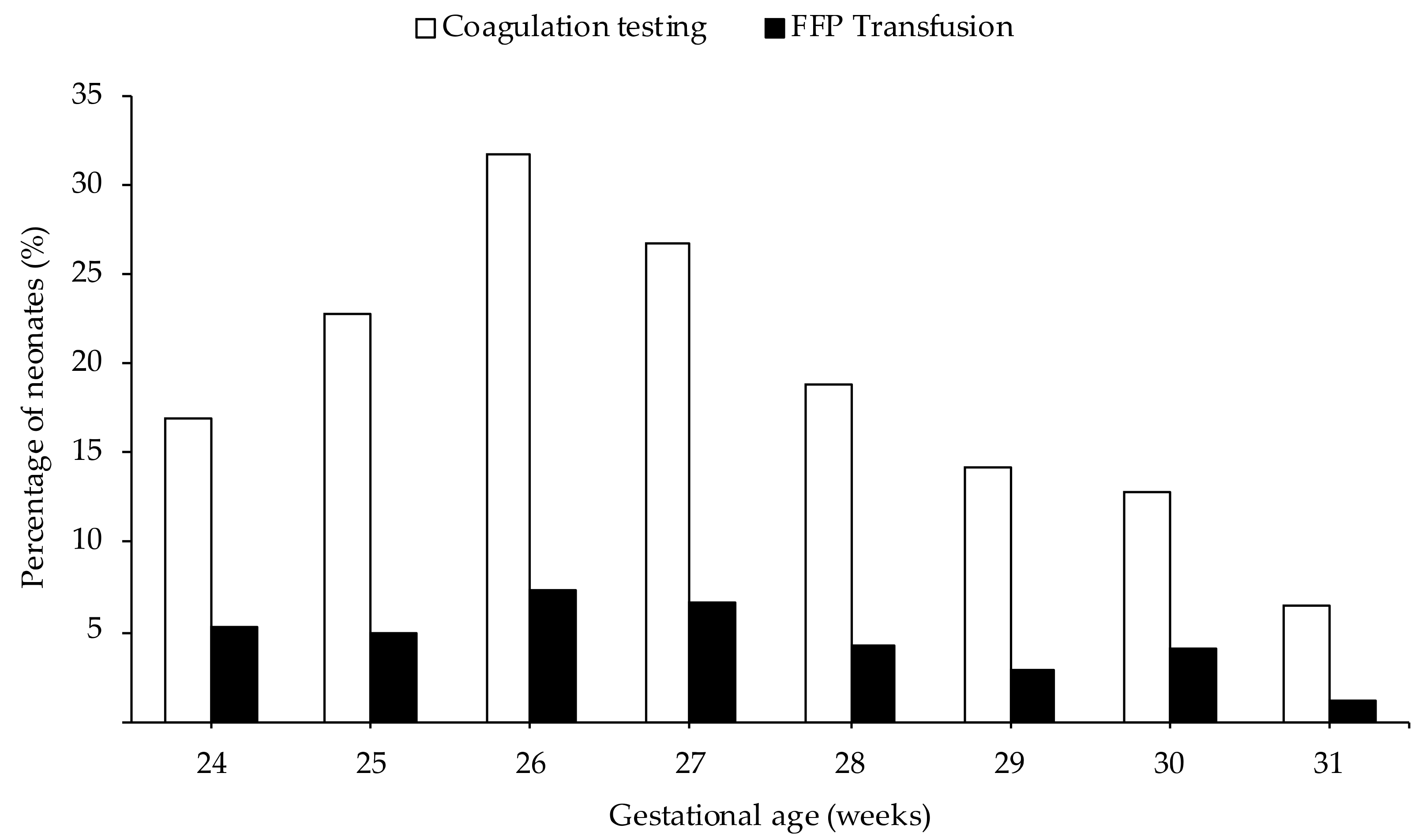
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Test | Day 1 | Day 5 | Day 30 | Day 90 |
|---|---|---|---|---|
| PT (s) (95% interval) | 13.0 (10.6–6.2) | 12.5 (10.0–15.3) | 11.8 (10.0–13.6) | 12.3 (10.0–14.6) |
| aPTT (s) (95% interval) | 53.6 (27.5–79.4) | 50.5 (26.9–74.1) | 44.7 (26.9–62.5) | 39.5 (28.3–50.7) |
References
- Motta, M.; Del Vecchio, A.; Radicioni, M. Clinical use of fresh-frozen plasma and cryoprecipitate in neonatal intensive care unit. J. Matern. Fetal Neonatal Med. 2011, 24 (Suppl. 1), 129–131. [Google Scholar] [CrossRef]
- Keir, A.K.; Stanworth, S.J. Neonatal plasma transfusion: An evidence-based review. Transfus. Med. Rev. 2016, 30, 174–182. [Google Scholar] [CrossRef]
- Motta, M.; Del Vecchio, A.; Perrone, B.; Ghirardello, S.; Radicioni, M. Fresh frozen plasma use in the NICU: A prospective, observational, multicentred study. Arch. Dis. Child. Fetal Neonatal Ed. 2014, 99, F303–F308. [Google Scholar] [CrossRef]
- Stanworth, S.J.; Grant-Casey, J.; Lowe, D.; Laffan, M.; New, H.; Murphy, M.F.; Allard, S. The use of fresh-frozen plasma in England: High levels of inappropriate use in adults and children. Transfusion 2011, 51, 62–70. [Google Scholar] [CrossRef] [PubMed]
- NNNI Trial Group. A randomized trial comparing the effect of prophylactic intravenous fresh frozen plasma, gelatin or glucose on early mortality and morbidity in preterm babies. Eur. J. Pediatr. 1996, 155, 580–588. [Google Scholar] [CrossRef] [PubMed]
- New, H.V.; Berryman, J.; Bolton-Maggs, P.H.; Cantwell, C.; Chalmers, E.A.; Davies, T.; Gottstein, R.; Kelleher, A.; Kumar, S.; Morley, S.L.; et al. Guidelines on transfusion for fetuses, neonates and older children. Br. J. Haematol. 2016, 175, 784–828. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Deorari, A.K.; Paul, V.K.; Sankar, M.J.; Sachdeva, A. AIIMS Protocols in Neonatology, 2nd ed.; Noble: Delhi, India, 2019; pp. 649–662. [Google Scholar]
- Pavenski, K.; Stanworth, S.; Fung, M.; Wood, E.M.; Pink, J.; Murphy, M.F.; Hume, H.; Nahirniak, S.; Webert, K.E.; Tanael, S.; et al. Quality of evidence-based guidelines for transfusion of red blood cells and plasma: A systematic review. Transfus. Med. Rev. 2018, 32, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Iorio, A.; Basileo, M.; Marchesini, E.; Materazzi, M.; Marchesi, M.; Esposito, A.; Palazzesi, G.P.; Pellegrini, L.; Pasqua, B.L.; Rocchetti, L.; et al. The good use of plasma. A critical analysis of five international guidelines. Blood Transfus. 2008, 6, 18–24. [Google Scholar] [CrossRef]
- Altuntas, N.; Yenicesu, I.; Beken, S.; Kulali, F.; Burcu Belen, F.; Hirfanoglu, I.M.; Onal, E.; Turkyilmaz, C.; Ergenekon, E.; Koc, E.; et al. Clinical use of fresh-frozen plasma in neonatal intensive care unit. Transfus. Apher. Sci. 2012, 47, 91–94. [Google Scholar] [CrossRef]
- Puetz, J.; Darling, G.; McCormick, K.A.; Wofford, J.D. Fresh frozen plasma and recombinant factor VIIa use in neonates. J. Pediatric Hematol. Oncol. 2009, 31, 901–906. [Google Scholar] [CrossRef]
- Christensen, R.D.; Baer, V.L.; Lambert, D.K.; Henry, E.; Ilstrup, S.J.; Bennett, S.T. Reference intervals for common coagulation tests of preterm infants (CME). Transfusion 2014, 54, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.T.; Veldman, A.; Malhotra, A. Does risk-based coagulation screening predict intraventricular haemorrhage in extreme premature infants? Blood Coagul. Fibrinolysis 2012, 23, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.M.; Starr, H.; Fincher, P.; Lam-Po-Tang, P.R. Intraventricular haemorrhage in the newborn. Med. J. Aust. 1976, 2, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Beverley, D.W.; Chance, G.W.; Inwood, M.J.; Schaus, M.; O’Keefe, B. Intraventricular haemorrhage and haemostasis defects. Arch. Dis. Child. 1984, 59, 444–448. [Google Scholar] [CrossRef] [Green Version]
- Andrew, M.; Paes, B.; Milner, R.; Johnston, M.; Mitchell, L.; Tollefsen, D.M.; Castle, V.; Powers, P. Development of the human coagulation system in the healthy premature infant. Blood 1988, 72, 1651–1657. [Google Scholar] [CrossRef] [Green Version]
- Gibson, B.E.; Todd, A.; Roberts, I.; Pamphilon, D.; Rodeck, C.; Bolton-Maggs, P.; Burbin, G.; Duguid, J.; Boulton, F.; Cohen, H.; et al. Transfusion guidelines for neonates and older children. Br. J. Haematol. 2004, 124, 433–453. [Google Scholar] [CrossRef]
- Gross, S.J.; Filston, H.C.; Anderson, J.C. Controlled study of treatment for disseminated intravascular coagulation in the neonate. J. Pediatr. 1982, 100, 445–448. [Google Scholar] [CrossRef]
- Curley, A.; Stanworth, S.J.; Willoughby, K.; Fustolo-Gunnink, S.F.; Venkatesh, V.; Hudson, C.; Deary, A.; Hodge, R.; Hopkins, V.; Lopez Santamaria, B.; et al. Randomized trial of platelet-transfusion thresholds in neonates. N. Engl. J. Med. 2019, 380, 242–251. [Google Scholar] [CrossRef]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Kloosterman, G.J. Intrauterine growth and intrauterine growth curves. Ned. Tijdschr. Verloskd. Gynaecol. 1969, 69, 349–365. [Google Scholar]
- Bell, M.J. Neonatal necrotizing enterocolitis. N. Engl. J. Med. 1978, 298, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Heeger, L.E.; Counsilman, C.E.; Bekker, V.; Bergman, K.A.; Zwaginga, J.J.; Te Pas, A.B.; Lopriore, E. Restrictive guideline for red blood cell transfusions in preterm neonates: Effect of a protocol change. Vox Sang. 2019, 114, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Fustolo-Gunnink, S.F.; Roehr, C.C.; Lieberman, L.; Christensen, R.D.; Van Der Bom, J.G.; Dame, C.; Del Vecchio, A.; Keir, A.K.; Curley, A.; Stanworth, S.J.; et al. Platelet and red cell transfusions for neonates: Lifesavers or Trojan horses? Expert Rev. Hematol. 2019, 12, 797–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, C.M.; Curley, A. Platelet transfusion thresholds in neonatal medicine. Early Hum. Dev. 2019, 138, 104845. [Google Scholar] [CrossRef]
- Keir, A.K.; Yang, J.; Harrison, A.; Pelausa, E.; Shah, P.S. Temporal changes in blood product usage in preterm neonates born at less than 30 weeks’ gestation in Canada. Transfusion 2015, 55, 1340–1346. [Google Scholar] [CrossRef]
- Counsilman, C.E.; Heeger, L.E.; Tan, R.; Bekker, V.; Zwaginga, J.J.; Te Pas, A.B.; Lopriore, E. Iatrogenic blood loss in extreme preterm infants due to frequent laboratory tests and procedures. J. Matern. Fetal Neonatal Med. 2019, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Jakacka, N.; Snarski, E.; Mekuria, S. Prevention of iatrogenic anemia in critical and neonatal care. Adv. Clin. Exp. Med. 2016, 25, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Catford, K.; Muthukumar, P.; Reddy, C.; Al Atrash, H.; Clarke, P.; Venkatesh, V.; Curley, A.E. Routine neonatal coagulation testing increases use of fresh-frozen plasma. Transfusion 2014, 54, 1444–1445. [Google Scholar] [CrossRef]
- Lieberman, L.; Lin, Y.; Cserti-Gazdewich, C.; Yi, Q.L.; Pendergrast, J.; Lau, W.; Callum, J. Utilization of frozen plasma, cryoprecipitate, and recombinant factor VIIa for children with hemostatic impairments: An audit of transfusion appropriateness. Pediatric Blood Cancer 2018, 65, e26933. [Google Scholar] [CrossRef]
- Johnson, C.A.; Snyder, M.S.; Weaver, R.L. Effects of fresh frozen plasma infusions on coagulation screening tests in neonates. Arch. Dis. Child. 1982, 57, 950–952. [Google Scholar] [CrossRef] [Green Version]
- Andrew, M.; Paes, B.; Milner, R.; Johnston, M.; Mitchell, L.; Tollefsen, D.M.; Powers, P. Development of the human coagulation system in the full-term infant. Blood 1987, 70, 165–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Go, H.; Ohto, H.; Nollet, K.E.; Kashiwabara, N.; Ogasawara, K.; Chishiki, M.; Hiruta, S.; Sakuma, I.; Kawasaki, Y.; Hosoya, M. Risk factors and treatments for disseminated intravascular coagulation in neonates. Ital. J. Pediatr. 2020, 46, 54. [Google Scholar] [CrossRef] [PubMed]
- Manuck, T.A.; Rice, M.M.; Bailit, J.L.; Grobman, W.A.; Reddy, U.M.; Wapner, R.J.; Thorp, J.M.; Caritis, S.N.; Prasad, M.; Tita, A.T.; et al. Preterm neonatal morbidity and mortality by gestational age: A contemporary cohort. Am. J. Obstet. Gynecol. 2016, 215, 103.e101–103.e114. [Google Scholar] [CrossRef] [Green Version]
- Kong, X.; Xu, F.; Wu, R.; Wu, H.; Ju, R.; Zhao, X.; Tong, X.; Lv, H.; Ding, Y.; Liu, F.; et al. Neonatal mortality and morbidity among infants between 24 to 31 complete weeks: A multicenter survey in China from 2013 to 2014. BMC Pediatr. 2016, 16, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roback, J.D.; Caldwell, S.; Carson, J.; Davenport, R.; Drew, M.J.; Eder, A.; Fung, M.; Hamilton, M.; Hess, J.R.; Luban, N.; et al. Evidence-based practice guidelines for plasma transfusion. Transfusion 2010, 50, 1227–1239. [Google Scholar] [CrossRef] [Green Version]
- De Backer, D.; Vandekerckhove, B.; Stanworth, S.; Williamson, L.; Hermans, C.; Van der Linden, P.; Hubner, R.; Baele, P.; Jochmans, K.; Ferrant, A.; et al. Guidelines for the use of fresh frozen plasma. Acta Clin. Belg. 2008, 63, 381–390. [Google Scholar] [CrossRef] [PubMed]
- De Vries, R.; Haas, F. English translation of the Dutch Blood Transfusion guideline 2011. Vox Sang. 2012, 103, 363. [Google Scholar] [CrossRef]
- National Blood Authority. Patient Blood Management Guidelines: Module 6—Neonatal and Paediatrics; NBA: Canberra, Australia, 2016.


| All Neonates (n = 2577) | |
|---|---|
| Male gender, n (%) | 1372 (53) |
| Multiple birth, n (%) | 1013 (39) |
| Caesarean section, n (%) | 1253 (49) |
| Small for gestational age, n (%) | 224 (9) |
| Birth weight (g), median (IQR) | 1252 (980–1520) |
| Gestational age at birth (weeks), median (IQR) | 29 (28–31) |
| FFP Transfusion (n = 94) | |
|---|---|
| Abnormal coagulation, n (%) | 53 (56) |
| Prolonged PT and aPTT | 52 (55) |
| Prolonged aPTT | 1 (1) |
| DIC, n (%) | 19 (20) |
| Clinical bleeding, n (%) | 16 (17) |
| Indication not recorded, n (%) | 4 (4) |
| Surgery, n (%) | 1 (1) |
| Suspected abnormal coagulation | 1 (1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Houben, N.A.M.; Heeger, L.E.; Stanworth, S.J.; New, H.V.; van der Bom, J.G.; Fustolo-Gunnink, S.; Lopriore, E. Changes in the Use of Fresh-Frozen Plasma Transfusions in Preterm Neonates: A Single Center Experience. J. Clin. Med. 2020, 9, 3789. https://doi.org/10.3390/jcm9113789
Houben NAM, Heeger LE, Stanworth SJ, New HV, van der Bom JG, Fustolo-Gunnink S, Lopriore E. Changes in the Use of Fresh-Frozen Plasma Transfusions in Preterm Neonates: A Single Center Experience. Journal of Clinical Medicine. 2020; 9(11):3789. https://doi.org/10.3390/jcm9113789
Chicago/Turabian StyleHouben, Nina A. M., Lisanne E. Heeger, Simon J. Stanworth, Helen V. New, Johanna G. van der Bom, Suzanne Fustolo-Gunnink, and Enrico Lopriore. 2020. "Changes in the Use of Fresh-Frozen Plasma Transfusions in Preterm Neonates: A Single Center Experience" Journal of Clinical Medicine 9, no. 11: 3789. https://doi.org/10.3390/jcm9113789
APA StyleHouben, N. A. M., Heeger, L. E., Stanworth, S. J., New, H. V., van der Bom, J. G., Fustolo-Gunnink, S., & Lopriore, E. (2020). Changes in the Use of Fresh-Frozen Plasma Transfusions in Preterm Neonates: A Single Center Experience. Journal of Clinical Medicine, 9(11), 3789. https://doi.org/10.3390/jcm9113789