On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
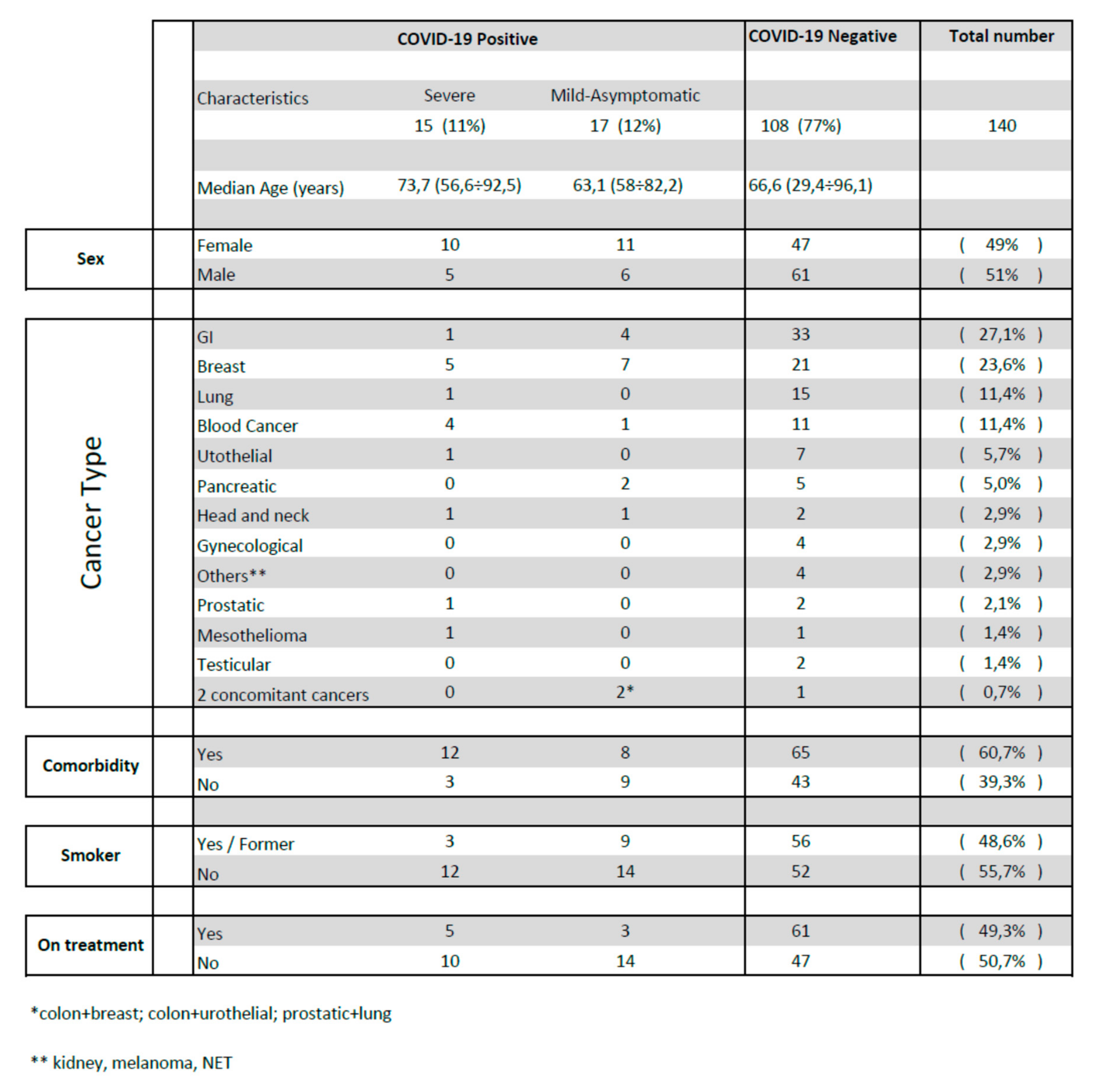
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Approval and Consent to Participate
Availability of Data and Materials
List of Abbreviations
| CT | computed tomography |
| RT-PCR | Real-time polymerase chain reaction |
| COVID-19 | coronavirus disease 19 |
| GGO | ground-glass opacities |
| CV | cardiovascular |
| OR | odds ratio |
| R-CHOP/R-DHAP | Rituximab–Cyclophosphamide–Hydroxydaunorubicin–Oncovin–Prednisone/Rituximab–Dexamethasone–Ara-C–Cisplatin |
| Mab | monoclonal antibody |
References
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 Transmission in Patients with Cancer at a Tertiary Care Hospital in Wuhan, China. JAMA Oncol. 2020, 6, 1108–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, L. Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020, 21, e181. [Google Scholar] [CrossRef]
- Moujaess, E.; Kourie, H.R.; Ghosn, M. Cancer patients and research during COVID-19 pandemic: A systematic review of current evidence. Crit. Rev. Oncol. 2020, 150, 102972. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Yin, J.; Qian, Y.; Wu, Y. Clinical characteristics and prognosis in cancer patients with COVID-19: A single center’s retrospective study. J. Infect. 2020, 81, 318–356. [Google Scholar] [CrossRef] [PubMed]
- Spezzani, V.; Piunno, A.; Iselin, H.U. Benign COVID-19 in an immunocompromised cancer patient—The case of a married couple. Swiss Med. Wkly. 2020, 150, w20246. [Google Scholar] [CrossRef]
- Bhoori, S.; Rossi, R.E.; Citterio, D.; Mazzaferro, V. COVID-19 in long-term liver transplant patients: Preliminary experience from an Italian transplant centre in Lombardy. Lancet Gastroenterol. Hepatol. 2020, 5, 532–533. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Lee, L.Y.W.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–992. [Google Scholar] [CrossRef]
- Robilotti, E.V.; Babady, N.E.; Mead, P.A.; Rolling, T.; Perez-Johnston, R.; Bernardes, M.; Bogler, Y.; Caldararo, M.; Figueroa, C.J.; Glickman, M.S.; et al. Determinants of COVID-19 disease severity in patients with cancer. Nat. Med. 2020, 26, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Albiges, L.; Foulon, S.; Bayle, A.; Gachot, B.; Pommeret, F.; Willekens, C.; Stoclin, A.; Merad, M.; Griscelli, F.; Lacroix, L.; et al. Determinants of the outcomes of patients with cancer infected with SARS-CoV-2: Results from the Gustave Roussy cohort. Nat. Cancer 2020, 1, 965–975. [Google Scholar] [CrossRef]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Yu, H.; Zhang, S. The indispensable role of chest CT in the detection of coronavirus disease 2019 (COVID-19). Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1638–1639. [Google Scholar] [CrossRef] [Green Version]
- Amalou, A.; Turkbey, B.; Sanford, T.; Harmon, S.; Turkbey, E.B.; Xu, S.; An, P.; Carrafiello, G.; Cariati, M.; Patella, F.; et al. Targeted early chest CT in COVID-19 outbreaks as diagnostic tool for containment of the pandemic—A multinational opinion. Diagn. Interv. Radiol. 2020, 26, 292–295. [Google Scholar] [CrossRef]
- Xu, B.; Xing, Y.; Peng, J.; Zheng, Z.; Tang, W.; Sun, Y.; Xu, C.; Peng, F. Chest CT for detecting COVID-19: A systematic review and meta-analysis of diagnostic accuracy. Eur. Radiol. 2020, 30, 5720–5727. [Google Scholar] [CrossRef]
- Sverzellati, N.; Milanese, G.; Milone, F.; Balbi, M.; Ledda, R.E.; Silva, M. Integrated Radiologic Algorithm for COVID-19 Pandemic. J. Thorac. Imaging 2020, 35, 228–233. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Kelesidis, T.; Daikos, G.; Boumpas, D.; Tsiodras, S. Does rituximab increase the incidence of infectious complications? A narrative review. Int. J. Infect. Dis. 2011, 15, e2–e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancman, G.; Mascarenhas, J.; Bar-Natan, M. Severe COVID-19 virus reactivation following treatment for B cell acute lymphoblastic leukemia. J. Hematol. Oncol. 2020, 13, 131. [Google Scholar] [CrossRef] [PubMed]
- Sahu, K.K.; Jindal, V.; Siddiqui, A.D.; Cerny, J. Facing COVID-19 in the hematopoietic cell transplant setting: A new challenge for transplantation physicians. Blood Cells Mol. Dis. 2020, 83, 102439. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient | Sex | Age | CT Features | Cancer Type | Chemotherapy or Follow Up | Radiotherapy | Setting | Comorbidities | Smoking | SIAARTI Stage | Hospital Admission | Nasofaringeal Swabbing | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B.G. | F | 74.8 | GGO (24 March 2020) | Pancreas | Gemcitabine-Abraxane | T2 N + M0 | Diabetes mellitus; Hypertension | former | Asymptomatic | No | Negative (30 March 2020) | Alive | |
| B.V. | M | 56.8 | GGO (28 April 2020) | Colon | FOLFIRI–Bevacizumab | Advanced | No | No | II (fever) | No | Negative (27 April 2020) | Alive | |
| B.M. | F | 53.5 | GGO (resolving) 28 April 2020 | Breast | Follow-up | T2N3M0 | No | Former | Asymtomatic | No | No | Alive | |
| B.G. | M | 73.0 | GGO (12 March 2020) | Abdominal mesothelioma | Carboplatin–pemetrexed | Advanced, progression of disease | Dyslipidemia, previous colon cancer | No | III (fatigue, anorexia, abdominal pain) | No | Negative (12 March 2020) | Alive | |
| C.M. | F | 61.01 | GGO (7 February 2020) | Colon + breast | FOLFOX; Everolimus + exemestane ongoing | T3 N1b M0 (colon); IV stadio (breast) | No | Former | Asymptomatic | No | No | Alive | |
| F.G. | F | 72.1 | GGO (6 February 2020) | Breast | Follow-up | T1bN0 | Diabetes mellitus; Hypertension; ischemic cardiomiopathy | Former | Asymtpomatic | No | No (household members affected by COVID-19) | Alive | |
| F.T. | F | 79.52 | GGO (12 March 2020) | Colon and Breast | Yes | Advanced (colon); T2N0 (breast) | Pulmonary Embolism; Hypertension; Congestive heart failure; Chronic kidney disease | No | Asymptomatic | No | No | Alive | |
| G.M. | F | 74.5 | GGO and left pulmonary consolidation (27 April 2020) | Breast | Carboplatin | Advanced | Pulmonary embolism; dyslipidemia | No | II (cought) | No | No (symptoms referred after remission) | Alive | |
| M.M. | F | 58.02 | GGO (1 February 2020) | Oesophageal | FLOT | Locally advanced (neoadjuvant) | Si | Asymptomatic | No | No | Alive | ||
| M.T. | F | 70.3 | GGO (14 March 2020) | Breast | Paclitaxel–Bevacizumab | 20 Gy (bone metastasis) | T2 N0 M1 | Pulmonary embolism | former | III (fever dyspnea) | Yes | Positive (14 March 2020) | Alive |
| S.G. | M | 82.15 | GGO and pulmonary consolidation (20 April 2020) | Urothelial and colon | FOLFOX | T3N2b (colon) adjuvant | Hypertension, COPD | Former | II (fever) | No | Positive (20 April 2020) | Alive | |
| S.G. | M | 68.6 | GGO (6 April 2020) | Bone metastasis of gastric cancer | 20 Gy (bone metastasis) | Advanced | Pulmonary embolism | Asymptomatic | yes for pulmonary embolism | Negative (16 April 2020) 10 days after CT scan) | Alive | ||
| S.O. | F | 41.95 | GGO and pulmonary consolidation (17 March 2020) | Breast | Adriamycine-cyclophosphamide–taxol | T4 N2bM0 (neoadjuvant) | No | No | Asymptomatic | No | Positive (24 March 2020) | Alive | |
| T.E. | M | 56.8 | GGO (1 April 2020) | Pancreas | FOLFIRINOX | T4N1 | Hypertension | No | II (fever, cought) | No | Positive (2 April 2020) | Alive | |
| T.A. | F | 70.8 | GGO (28 February 2020) | Breast | Adriamycine–cyclophosphamide | T1c N0 M0 (adjuvant) | HBV-related HCC; hypothyroidism, previous gastric cancer; coeliac disease; COPD | former | Asymptomatic | No | No | Alive | |
| V.G. | M | 76.3 | GGO and pulmonary consolidation (17 March 2020) | NHL DLBCL | Follow-up | I A Ann Arbor | Hypertension, rheumatoid arthritis | No | Asymptomatic | No | No | Alive | |
| V.M. | M | 51.6 | GGO (7 April 2020) | Head and neck | Cisplatin | Yes | T3 N0/1 M0 | HCV | Yes | Asymptomatic | No | Negative (17 April 2020) | Alive |
| Z.L. | F | 56.7 | GGO (26 March 2020) | NHL MCL | R-CHOP/R-DHAP | IV Ann Arbor | Previous choroidal melanoma | No | III → VI (fever and cough at the onset) | Yes ICU | Positive (26 March 2020) | Dead | |
| S.G. | M | 74.3 | GGO (2 April 2020) | Prostatic | Follow-up | Not followed in our hospital | Hypovitaminosis D | No | III (fever, cought) | Yes | Positive (2 April 2020) | Alive | |
| R.R. | F | 65.47 | patchy shadowing pulmonary consolidation (8 April 2020) | Head and neck | Carboplatin | Yes | T1N3b adjuvant. Not followed in our hospital | Hypertension, COPD, peripheral arterial disease, pulmonary embolism | Former | III (dyspnea, cough) concomitant pulmonary embolism | Yes | Negative (8 April 2020) | Alive |
| M.L. | F | 78.15 | GGO (19 March 2020) | Breast | Follow-up | Not followed in our hospital | Hypertension, radiation induced pulmonary fibrosis | No | III → VI (fever, dyspnea, cough at the onset) | Yes ICU | Positive (19 March 2020) | Dead | |
| B.A. | F | 72.27 | GGO (16 March 2020) | Breast | Follow-up | T1cN0 | Hypertension, Diabetes mellitus, Dyslipidemia | No | III (fever, dyspnea) | Yes | Positive (16 March 2020) | Alive | |
| C.M. | F | 77.4 | GGO, pulmonary consolidation (30 March 2020) | Breast | Follow-up | Advanced | Hypertension | No | II → VI (nausea, fever, anorexia) | Yes ICU | Positive (30 March 2020) | Dead | |
| R.M. | M | 78.3 | GGO (16 March 2020) | Urothelial | Follow-up | Not followed in our hospital | Hypertension, COPD, congestive heart failure, atrial fibrilation, ictus | No | III → VI (nausea, fever, anorexia) | Yes | Positive (16 March 2020) | Dead | |
| N.G. | F | 86.7 | Bilateral interstitial abnormalities; pulmonary consolidation (6 April 2020) | CLL | Watch-and-wait follow up (never treated) | Hypertension, diabetes mellitus | No | III → VI (fever, cough, dyspnea, asthenia) | Yes | Positive (6 April 2020) | Dead | ||
| M.L. | F | 62.29 | GGO (4 April 2020) | HD | ABVD 6 cycles | IV b Ann Arbor. Not followed in our hospital | Previous gynecological cancer | No | III (fever) | Yes | Positive (4 April 2020) | Alive | |
| S.M. | F | 75.13 | GGO (30 March 2020) | Breast | Follow-up | Not followed in our hospital | Hypertension, atrial fibrillation, diabetes mellitus | No | III → VI (fever, asthenia, cough) | Yes | Positive (30 March 2020) | Dead | |
| G.C. | F | 92.54 | GGO (30 April 2020) | Gastric | Follow-up | T3N0 | Previous breast cancer, hypertension, chronic gastric reflux | No | III (dyspnea) concomitant atrial fibrillation and congestive heart failure | Yes | Negative (30 April 2020) | Alive | |
| C.E. | M | 56.5 | GGO and pulmonary consolidations (9 April 2020) | CLL | Follow-up | Not followed in our hospital | No | No | III (fever, cought, dyspnea) | Yes | Positive (9 April 2020) | Alive | |
| M.L. | M | 85.79 | GGO (31 March 2020) | Lung | Follow-up | Advanced, Progression disease. Not followed in our hospital | Dyslipidemia, hypertension, COPD, chronic renal disease | Former | III (dyspnea, fever) | Yes | Positive (31 March 2020) | Alive | |
| F.N. | F | 54 | Negative (14 March 2020) | Breast | Adriamycine–cyclophosphamide | Locally advanced (neoadjuvant) | No | No | II (fever) | No | Positive (3 March 2020) | Alive | |
| S.A. | F | 40 | Negative (2 April 2020) CT scan after symptoms’ remission | Breast | Trastuzumab | T2N1M1 | Hypothyroidism, multiple sclerosis | No | II (fever, cought) | No | Positive (20th March 2020) | Alive |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martini, F.; D’Alessio, A.; Bracchi, F.; Di Mauro, D.; Fargnoli, A.; Motta, M.; Giussani, C.; Meazza Prina, M.; Gobbin, G.; Taverna, M. On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study. J. Clin. Med. 2020, 9, 3935. https://doi.org/10.3390/jcm9123935
Martini F, D’Alessio A, Bracchi F, Di Mauro D, Fargnoli A, Motta M, Giussani C, Meazza Prina M, Gobbin G, Taverna M. On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study. Journal of Clinical Medicine. 2020; 9(12):3935. https://doi.org/10.3390/jcm9123935
Chicago/Turabian StyleMartini, Francesca, Andrea D’Alessio, Federico Bracchi, Daniela Di Mauro, Anna Fargnoli, Marco Motta, Cristina Giussani, Marco Meazza Prina, Giovanni Gobbin, and Monica Taverna. 2020. "On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study" Journal of Clinical Medicine 9, no. 12: 3935. https://doi.org/10.3390/jcm9123935
APA StyleMartini, F., D’Alessio, A., Bracchi, F., Di Mauro, D., Fargnoli, A., Motta, M., Giussani, C., Meazza Prina, M., Gobbin, G., & Taverna, M. (2020). On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study. Journal of Clinical Medicine, 9(12), 3935. https://doi.org/10.3390/jcm9123935