Effect of Obstructive Sleep Apnea and CPAP Treatment on Cardiovascular Outcomes in Acute Coronary Syndrome in the RICCADSA Trial



Abstract
:1. Introduction
2. Study Design and Methods
2.1. Study Participants
2.2. Study Oversight
2.3. Sleep Studies, Group Allocation and Randomization
2.4. Interventions and Follow-Up
2.5. Statistical Analysis
2.6. Sample Size Estimation
3. Results
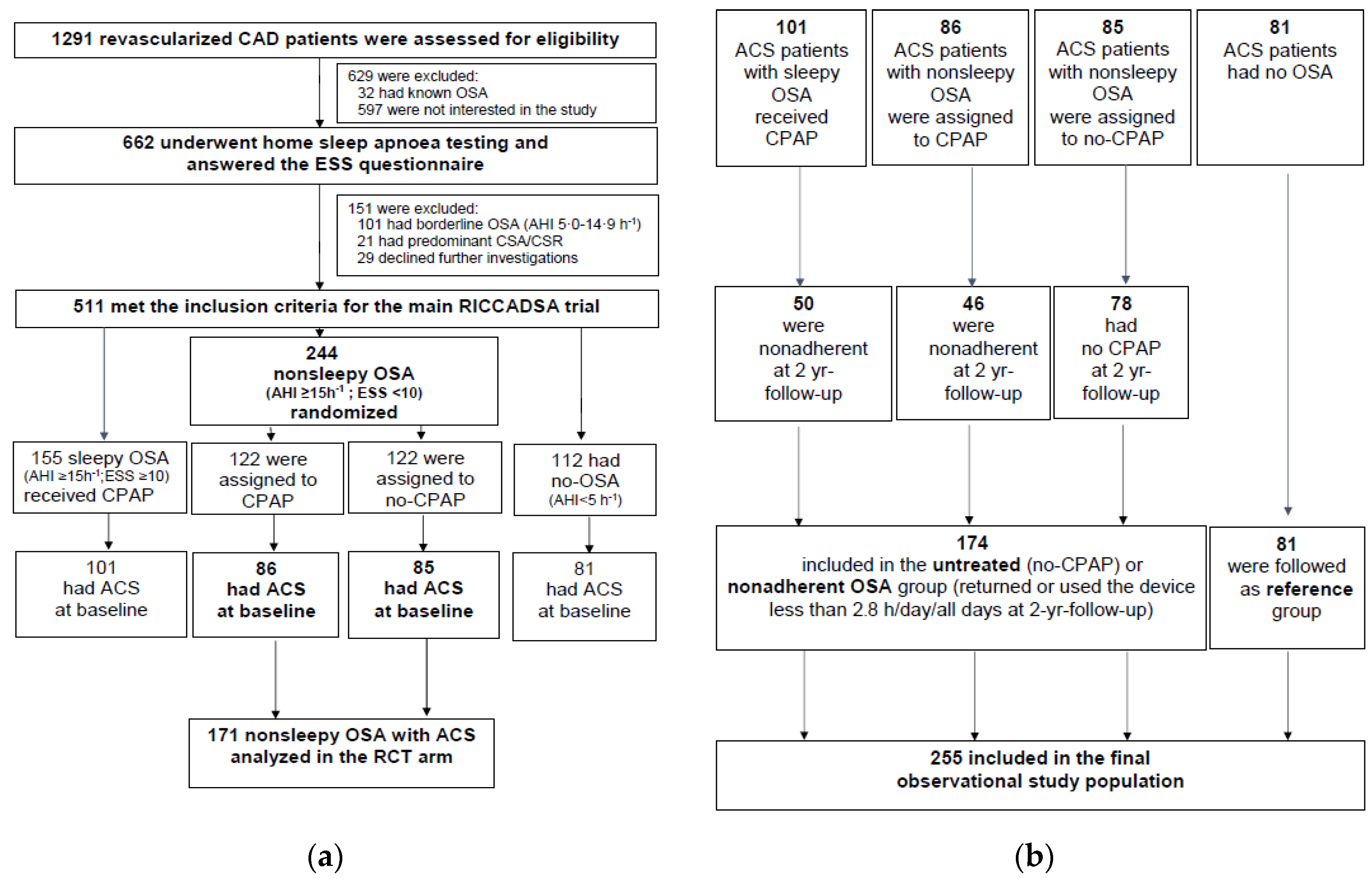
3.1. Study Participants—The RCT Arm
3.1.1. Baseline Characteristics of the RCT Arm
3.1.2. Numbers Analyzed
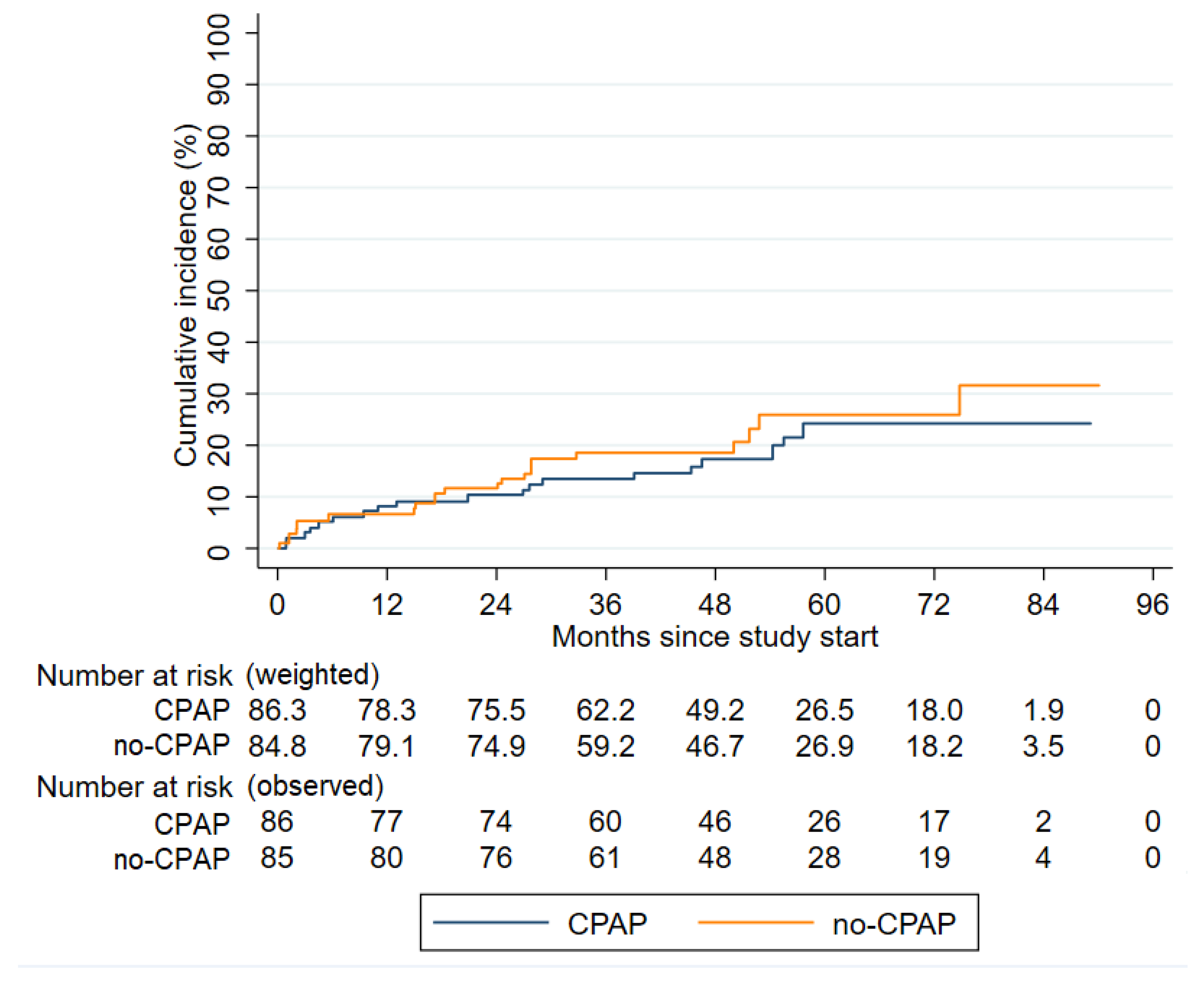
3.1.3. Outcomes in the RCT Arm
IPTW Propensity Score-Adjusted ITT Analysis
On-Treatment Analysis
3.2. Study Participants—The Observational Arm
3.2.1. Baseline Characteristics of the Observational Arm Including Nonadherent Patients
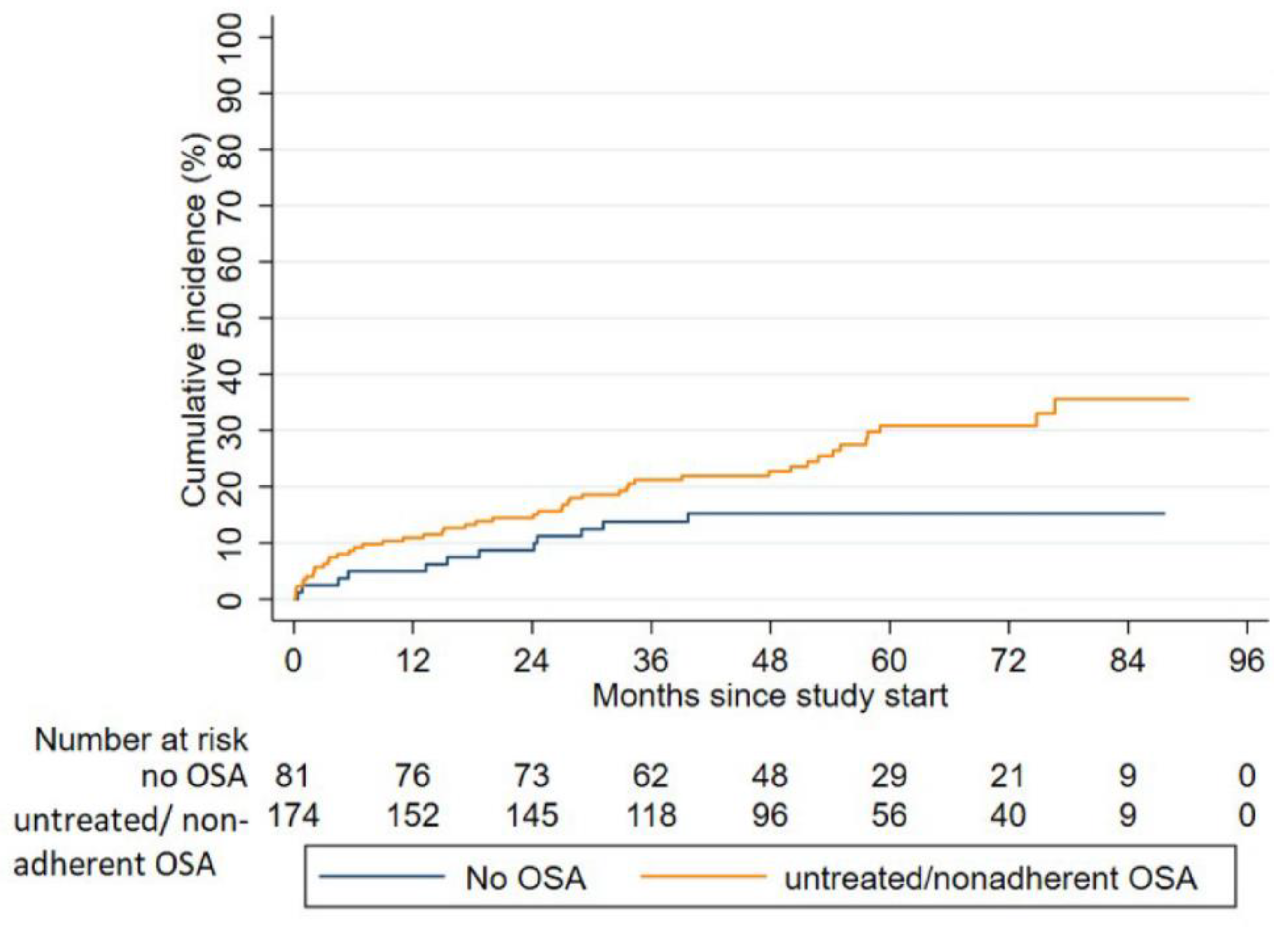
3.2.2. Outcomes in the Observational Arm
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Peker, Y.; Balcan, B. Cardiovascular outcomes of continuous positive airway pressure therapy for obstructive sleep apnea. J. Thorac. Dis. 2018, 10, S4262–S4279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.J.; Gao, X.F.; Ge, Z.; Jiang, X.M.; Xiao, P.X.; Tian, N.L.; Kan, J.; Lee, C.H.; Chen, S.L. Obstructive sleep apnea affects the clinical outcomes of patients undergoing percutaneous coronary intervention. Patient Prefer. Adherence 2016, 10, 871–878. [Google Scholar] [PubMed] [Green Version]
- Lee, C.H.; Sethi, R.; Li, R.; Ho, H.H.; Hein, T.; Jim, M.H.; Loo, G.; Koo, C.Y.; Gao, X.F.; Chandra, S.; et al. Obstructive Sleep Apnea and Cardiovascular Events After Percutaneous Coronary Intervention. Circulation 2016, 133, 2008–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchôa, C.H.G.; Danzi-Soares, N.J.; Nunes, F.S.; de Souza, A.A.L.; Nerbass, F.B.; Pedrosa, R.P.; César, L.A.M.; Lorenzi-Filho, G.; Drager, L.F. Impact of OSA on cardiovascular events after coronary artery bypass surgery. Chest 2015, 147, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- Engleman, H.M.; Martin, S.E.; Kingshott, R.N.; Mackay, T.W.; Deary, I.J.; Douglas, N.J. Randomised placebo controlled trial of daytime function after continuous positive airway pressure (CPAP) therapy for the sleep apnoea/hypopnoea syndrome. Thorax 1998, 53, 341–345. [Google Scholar] [CrossRef] [Green Version]
- Cassar, A.; Morgenthaler, T.I.; Lennon, R.J.; Rihal, C.S.; Lerman, A. Treatment of obstructive sleep apnea is associated with decreased cardiac death after percutaneous coronary intervention. J. Am. Coll. Cardiol. 2007, 50, 1310–1314. [Google Scholar] [CrossRef] [Green Version]
- Campos-Rodriguez, F.; Martinez-Garcia, M.A.; de la Cruz-Moron, I.; Almeida-Gonzalez, C.; Catalan-Serra, P.; Montserrat, J.M. Cardiovascular mortality in women with obstructive sleep apnea with or without continuous positive airway pressure treatment: A cohort study. Ann. Intern. Med. 2012, 156, 115–122. [Google Scholar] [CrossRef]
- Campos-Rodriguez, F.; Martinez-Garcia, M.A.; Reyes-Nunez, N.; Caballero-Martinez, I.; Catalan-Serra, P.; Almeida-Gonzalez, C.V. Role of sleep apnea and continuous positive airway pressure therapy in the incidence of stroke or coronary heart disease in women. Am. J. Respir. Crit. Care Med. 2014, 189, 1544–1550. [Google Scholar] [CrossRef]
- Peker, Y.; Glantz, H.; Eulenburg, C.; Wegscheider, K.; Herlitz, J.; Thunstrom, E. Effect of Positive Airway Pressure on Cardiovascular Outcomes in Coronary Artery Disease Patients with Nonsleepy Obstructive Sleep Apnea. The RICCADSA Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2016, 194, 613–620. [Google Scholar] [CrossRef]
- McEvoy, R.D.; Antic, N.A.; Heeley, E.; Luo, Y.; Ou, Q.; Zhang, X.; Mediano, O.; Chen, R.; Drager, L.F.; Liu, Z.; et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. N. Engl. J. Med. 2016, 375, 919–931. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-de-la-Torre, M.; Sánchez-de-la-Torre, A.; Bertran, S.; Abad, J.; Duran-Cantolla, J.; Cabriada, V.; Mediano, O.; Masdeu, M.J.; Alonso, M.L.; Masa, J.F.; et al. Effect of obstructive sleep apnoea and its treatment with continuous positive airway pressure on the prevalence of cardiovascular events in patients with acute coronary syndrome (ISAACC study): A randomised controlled trial. Lancet Respir. Med. 2020, 8, 359–367. [Google Scholar] [CrossRef]
- Peker, Y.; Glantz, H.; Thunstrom, E.; Kallryd, A.; Herlitz, J.; Ejdeback, J. Rationale and design of the Randomized Intervention with CPAP in Coronary Artery Disease and Sleep Apnoea—RICCADSA trial. Scand. Cardiovasc. J. 2009, 43, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Peker, Y.; Thunstrom, E.; Glantz, H.; Wegscheider, K.; Eulenburg, C. Outcomes in coronary artery disease patients with sleepy obstructive sleep apnoea on CPAP. Eur. Respir. J. 2017, 50. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, A.M.; Gooneratne, N.S.; Marcus, C.L.; Ofer, D.; Richards, K.C.; Weaver, T.E. A systematic review of CPAP adherence across age groups: Clinical and empiric insights for developing CPAP adherence interventions. Sleep Med. Rev. 2011, 15, 343–356. [Google Scholar] [CrossRef] [Green Version]
- Lederer, D.J.; Bell, S.C.; Branson, R.D.; Chalmers, J.D.; Marshall, R.; Maslove, D.M.; Ost, D.E.; Punjabi, N.M.; Schatz, M.; Smyth, A.R.; et al. Control of Confounding and Reporting of Results in Causal Inference Studies. Guidance for Authors from Editors of Respiratory, Sleep, and Critical Care Journals. Ann. Am. Thorac. Soc. 2019, 16, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Peker, Y.; Wegscheider, K.; Eulenburg, C. Reply: Effect of Continuous Positive Airway Pressure Therapy on Cardiovascular Outcomes: Risk Assessment. Am. J. Respir. Crit. Care Med. 2017, 196, 662–663. [Google Scholar] [CrossRef]
- Yumino, D.; Tsurumi, Y.; Takagi, A.; Suzuki, K.; Kasanuki, H. Impact of obstructive sleep apnea on clinical and angiographic outcomes following percutaneous coronary intervention in patients with acute coronary syndrome. Am. J. Cardiol. 2007, 99, 26–30. [Google Scholar] [CrossRef]
- Peker, Y. Obstructive sleep apnoea in acute coronary syndrome. Lancet Respir. Med. 2020, 8, e14. [Google Scholar] [CrossRef]
- Schiza, S.E.; Simantirakis, E.; Bouloukaki, I.; Mermigkis, C.; Kallergis, E.M.; Chrysostomakis, S.; Arfanakis, D.; Tzanakis, N.; Vardas, P.; Siafakas, N.M. Sleep disordered breathing in patients with acute coronary syndromes. J. Clin. Sleep Med. 2012, 8, 21–26. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javaheri, S.; Martinez-Garcia, M.A.; Campos-Rodriguez, F.; Muriel, A.; Peker, Y. Continuous Positive Airway Pressure Adherence for Prevention of Major Adverse Cerebrovascular and Cardiovascular Events in Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2020, 201, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Wise, M.S. Objective measures of sleepiness and wakefulness: Application to the real world? J. Clin. Neurophysiol. 2006, 23, 39–49. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| CPAP n = 86 | No-CPAP n = 85 | |
|---|---|---|
| Age, y | 65.2 (8.4) | 65.5 (8.5) |
| AHI, events/h | 28.0 (12.2) | 28.6 (13.1) |
| ODI, events/h | 16.0 (12.8) | 10.5 (10.9) |
| Mean SpO2, % | 93.7 (2.4) | 93.2 (1.9) |
| Minimum SpO2, % | 82.4 (5.9) | 82.9 (6.6) |
| Time spent below 90% SpO2, % | 6.6 (16.7) | 7.8 (14.2) |
| ESS score | 5.5 (2.3) | 5.3 (2.2) |
| BMI, kg/m2 | 28.4 (4.0) | 28.7 (3.6) |
| LVEF, % | 57.9 (8.4) | 56.1 (10.3) |
| Obesity, % | 30.2 | 31.8 |
| Female, % | 20.9 | 12.9 |
| Current smoker, % | 19.8 | 18.8 |
| Pulmonary disease. % | 3.5 | 9.4 |
| Hypertension, % | 67.4 | 54.1 |
| ACS type | ||
| STEMI, % | 27.9 | 29.4 |
| Non-STEMI, % | 45.3 | 45.9 |
| Unstable angina, % | 26.7 | 24.7 |
| AMI at baseline, % | 73.2 | 75.3 |
| CABG at baseline, % | 16.3 | 14.1 |
| Previous PCI or CABG, % | 11.8 | 7.7 |
| Diabetes mellitus, % | 29.1 | 18.8 |
| β-blocker use, % | 91.6 | 86.7 |
| Diuretic use, % | 18.1 | 18.3 |
| CCB use, % | 22.9 | 14.5 |
| ACE inhibitor use, % | 55.4 | 50.6 |
| ARB use, % | 10.8 | 16.9 |
| Clopidogrel use, % | 70.2 | 61.4 |
| Aspirin use, % | 96.4 | 90.4 |
| Warfarin use, % | 3.6 | 7.2 |
| Lipid-lowering agent use, % | 96.4 | 95.2 |
| Multivariate | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| CPAP vs. no-CPAP | 1.23 | 0.64–2.38 | 0.54 |
| Age | 1.03 | 0.99–1.08 | 0.18 |
| CABG vs. PCI | 0.37 | 0.09–1.55 | 0.17 |
| Current smoking | 2.06 | 0.92–4.60 | 0.08 |
| Diabetes mellitus | 3.34 | 1.72–6.48 | <0.01 |
| Previous PCI or CABG | 3.81 | 2.03–7.14 | <0.01 |
| Multivariate * | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| CPAP usage ≥3 h/day vs. <3 h/day or no-CPAP | 1.11 | 0.20–6.32 | 0.90 |
| CPAP usage ≥4 h/day vs. <4 h/day or no-CPAP | 0.17 | 0.03–0.81 | 0.03 |
| CPAP usage ≥5 h/day vs. <5 h/day or no-CPAP | 0.26 | 0.07–1.05 | 0.06 |
| Untreated/Nonadherent OSA n = 174 | No-OSA n = 81 | |
|---|---|---|
| Age *, y | 64.7 (8.2) | 61.4 (9.9) |
| AHI *, events/h | 26.8 (11.8) | 2.9 (1.4) |
| ODI *, events/h | 14.4 (12.8) | 1.6 (1.3) |
| ESS score * | 7.3 (3.9) | 5.5 (2.9) |
| BMI *, kg/m2 | 28.7 (4.0) | 25.4 (2.7) |
| LVEF, % | 56.4 (9.6) | 57.7 (7.6) |
| Obesity, % | 32.2 | 4.9 |
| Female, % | 11.5 | 19.8 |
| Current smoker, % | 22.4 | 32.1 |
| Pulmonary disease. % | 8.0 | 11.1 |
| Hypertension, % | 55.7 | 44.1 |
| ACS type | ||
| STEMI, % | 27.0 | 33.3 |
| Non-STEMI, % | 45.4 | 53.1 |
| Unstable angina, % | 27.6 | 13.6 |
| AMI at baseline *, % | 72.4 | 86.4 |
| CABG at baseline, % | 16.7 | 11.1 |
| Previous PCI or CABG, % | 19.2 | 13.6 |
| Diabetes mellitus *, % | 25.9 | 12.3 |
| β-Blocker use, % | 89.2 | 82.1 |
| Diuretic use, % | 15.1 | 7.8 |
| CCB use, % | 15.6 | 9.0 |
| ACE inhibitor use, % | 53.9 | 46.2 |
| ARB use, % | 12.6 | 7.7 |
| Clopidogrel use, % | 67.5 | 75.3 |
| Aspirin use, % | 90.4 | 97.4 |
| Warfarin use, % | 7.8 | 2.6 |
| Lipid-lowering agent use, % | 97.0 | 93.5 |
| Multivariate | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Untreated/Nonadherent OSA vs. no-OSA | 1.97 | 1.03–3.77 | 0.04 |
| Age | 1.02 | 0.98–1.05 | 0.33 |
| CABG vs. PCI | 0.18 | 0.04–0.76 | 0.02 |
| Current smoking | 1.51 | 0.82–2.77 | 0.18 |
| Diabetes mellitus | 1.71 | 0.97–3.00 | 0.06 |
| Previous PCI or CABG | 2.88 | 1.67–4.95 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peker, Y.; Thunström, E.; Glantz, H.; Eulenburg, C. Effect of Obstructive Sleep Apnea and CPAP Treatment on Cardiovascular Outcomes in Acute Coronary Syndrome in the RICCADSA Trial. J. Clin. Med. 2020, 9, 4051. https://doi.org/10.3390/jcm9124051
Peker Y, Thunström E, Glantz H, Eulenburg C. Effect of Obstructive Sleep Apnea and CPAP Treatment on Cardiovascular Outcomes in Acute Coronary Syndrome in the RICCADSA Trial. Journal of Clinical Medicine. 2020; 9(12):4051. https://doi.org/10.3390/jcm9124051
Chicago/Turabian StylePeker, Yüksel, Erik Thunström, Helena Glantz, and Christine Eulenburg. 2020. "Effect of Obstructive Sleep Apnea and CPAP Treatment on Cardiovascular Outcomes in Acute Coronary Syndrome in the RICCADSA Trial" Journal of Clinical Medicine 9, no. 12: 4051. https://doi.org/10.3390/jcm9124051
APA StylePeker, Y., Thunström, E., Glantz, H., & Eulenburg, C. (2020). Effect of Obstructive Sleep Apnea and CPAP Treatment on Cardiovascular Outcomes in Acute Coronary Syndrome in the RICCADSA Trial. Journal of Clinical Medicine, 9(12), 4051. https://doi.org/10.3390/jcm9124051