Effect of Severe External Airborne Agents’ Exposure on Dementia





Abstract
:1. Introduction
2. Methods
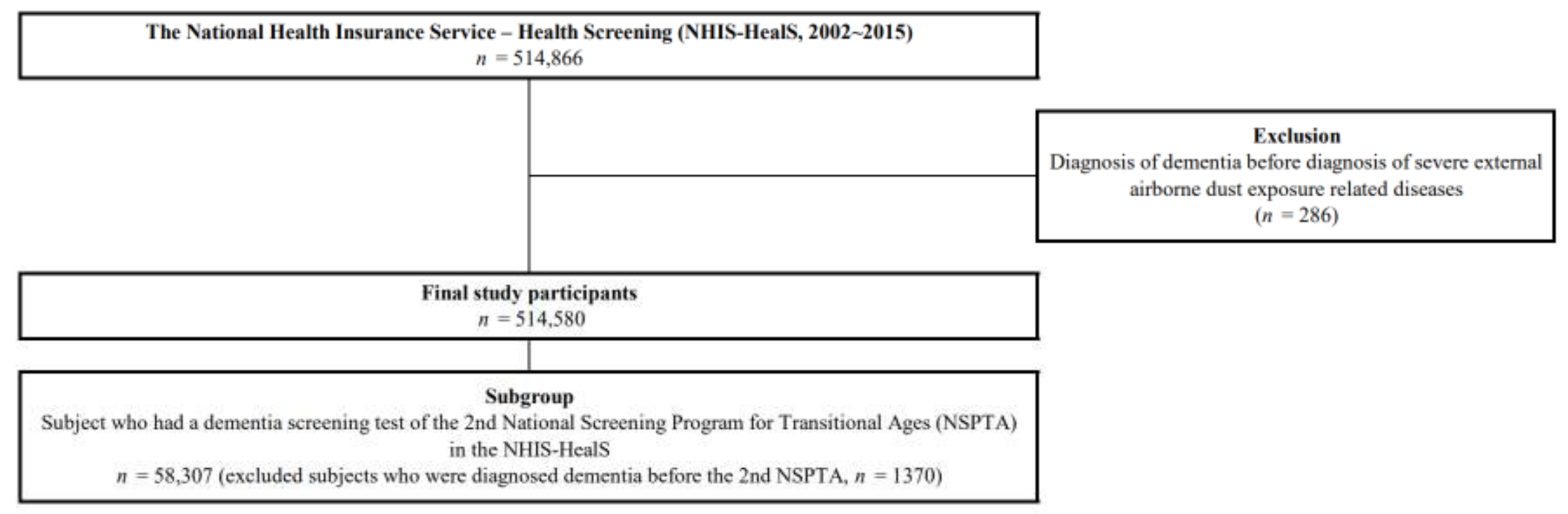
2.1. Data and Study Participants
2.2. Dementia
2.3. Exposure to Severe External Airborne Agents
2.4. Other Covariates
2.5. Statistical Analysis
2.6. Ethical Consideration and Consents for Publication
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hubbard, R. Occupational dust exposure and the aetiology of cryptogenic fibrosing alveolitis. Eur. Respir. J. 2001, 18, 119–121. [Google Scholar]
- Lee, W.; Ahn, Y.S.; Lee, S.; Song, B.M.; Hong, S.; Yoon, J.H. Occupational exposure to crystalline silica and gastric cancer: A systematic review and meta-analysis. Occup. Environ. Med. 2016, 73, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Costello, S.; Attfield, M.D.; Lubin, J.H.; Neophytou, A.M.; Blair, A.; Brown, D.M.; Stewart, P.A.; Vermeulen, R.; Eisen, E.A.; Silverman, D.T. Ischemic heart disease mortality and diesel exhaust and respirable dust exposure in the diesel exhaust in miners study. Am. J. Epidemiol. 2018, 187, 2623–2632. [Google Scholar] [CrossRef] [PubMed]
- Schyllert, C.; Rönmark, E.; Andersson, M.; Hedlund, U.; Lundbäck, B.; Hedman, L.; Lindberg, A. Occupational exposure to chemicals drives the increased risk of asthma and rhinitis observed for exposure to vapours, gas, dust and fumes: A cross-sectional population-based study. Occup. Environ. Med. 2016, 73, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Kilian, J.; Kitazawa, M. The emerging risk of exposure to air pollution on cognitive decline and Alzheimer’s disease–evidence from epidemiological and animal studies. Biomed. J. 2018, 41, 141–162. [Google Scholar] [CrossRef] [PubMed]
- Hancock, D.G.; Langley, M.E.; Chia, K.L.; Woodman, R.J.; Shanahan, E.M. Wood dust exposure and lung cancer risk: A meta-analysis. Occup. Environ. Med. 2015, 72, 889–898. [Google Scholar] [CrossRef]
- Abubakar, I.; Tillmann, T.; Banerjee, A. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- Oberdörster, G.; Sharp, Z.; Atudorei, V.; Elder, A.; Gelein, R.; Kreyling, W.; Cox, C. Translocation of inhaled ultrafine particles to the brain. Inhal. Toxicol. 2004, 16, 437–445. [Google Scholar] [CrossRef]
- Clifford, A.; Lang, L.; Chen, R.; Anstey, K.J.; Seaton, A. Exposure to air pollution and cognitive functioning across the life course–a systematic literature review. Environ. Res. 2016, 147, 383–398. [Google Scholar] [CrossRef]
- Jung, C.-R.; Lin, Y.-T.; Hwang, B.-F. Ozone, particulate matter, and newly diagnosed Alzheimer’s disease: A population-based cohort study in Taiwan. J. Alzheimers Dis. 2015, 44, 573–584. [Google Scholar] [CrossRef] [Green Version]
- Ranft, U.; Schikowski, T.; Sugiri, D.; Krutmann, J.; Krämer, U. Long-term exposure to traffic-related particulate matter impairs cognitive function in the elderly. Environ. Res. 2009, 109, 1004–1011. [Google Scholar] [CrossRef]
- Weuve, J.; Puett, R.C.; Schwartz, J.; Yanosky, J.D.; Laden, F.; Grodstein, F. Exposure to particulate air pollution and cognitive decline in older women. Arch. Intern. Med. 2012, 172, 219–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calderón-Garcidueñas, L.; Franco-Lira, M.; Mora-Tiscareño, A.; Medina-Cortina, H.; Torres-Jardón, R.; Kavanaugh, M. Early Alzheimer’s and Parkinson’s disease pathology in urban children: Friend versus foe responses—It is time to face the evidence. BioMed. Res. Int. 2013, 161687, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Gatto, N.M.; Henderson, V.W.; Hodis, H.N.; John, J.A.S.; Lurmann, F.; Chen, J.C.; Mack, W.J. Components of air pollution and cognitive function in middle-aged and older adults in Los Angeles. Neurotoxicology 2014, 40, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.-C.; Schwartz, J. Neurobehavioral effects of ambient air pollution on cognitive performance in US adults. Neurotoxicology 2009, 30, 231–239. [Google Scholar] [CrossRef]
- Kioumourtzoglou, M.-A.; Schwartz, J.D.; Weisskopf, M.G.; Melly, S.J.; Wang, Y.; Dominici, F.; Zanobetti, A. Long-term PM2. 5 exposure and neurological hospital admissions in the northeastern United States. Environ. Health Perspect 2016, 124, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Block, M.L.; Zecca, L.; Hong, J.-S. Microglia-mediated neurotoxicity: Uncovering the molecular mechanisms. Nat. Rev. Neurosci. 2007, 8, 57–69. [Google Scholar] [CrossRef]
- Dimakakou, E.; Johnston, H.J.; Streftaris, G.; Cherrie, J.W. Exposure to environmental and occupational particulate air pollution as a potential contributor to neurodegeneration and diabetes: A systematic review of epidemiological research. Int. J. Environ. Res. Public Health 2018, 15, 1704. [Google Scholar] [CrossRef] [Green Version]
- Seong, S.C.; Kim, Y.-Y.; Khang, Y.-H.; Park, J.H.; Kang, H.-J.; Lee, H.; Do, C.-H.; Song, J.-S.; Bang, J.H.; Ha, S.; et al. Data resource profile: The national health information database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar]
- Lee, J.; Lee, J.S.; Park, S.-H.; Shin, S.A.; Kim, K. Cohort profile: The national health insurance service–national sample cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.-Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.-J.; Do, C.-H.; Song, J.-S.; Lee, E.-J.; et al. Cohort profile: The national health insurance service-national health screening cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.-S.; Lee, Y.R.; Chae, Y.; Park, S.Y.; Oh, I.H.; Jang, B.H. Translation of Korean medicine use to ICD-codes using national health insurance service-national sample cohort. Evid Based Complement Altern. Med. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, A.; Kim, S.Y.; Park, K.W.; Park, K.H.; Youn, Y.C.; Lee, D.W.; Lee, J.Y.; Lee, J.H.; Jeong, J.H.; Choi, S.H.; et al. Reliability and Validity of a Short Form of the Korean Dementia Screening Questionnaire-Cognition. J. Clin. Neurol. 2020, 16, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Kim, S.; Park, K.W.; Park, K.H.; Youn, Y.C.; Lee, D.W.; Lee, J.Y.; Lee, J.H.; Jeong, J.H.; Choi, S.H.; et al. A comparative evaluation of the KDSQ-C, AD8, and SMCQ as a cognitive screening test to be used in national medical check-ups in Korea. J. Korean Med. Sci. 2019, 34, e111. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Lee, W.; Kim, J.; Lim, S.S.; Kim, Y.; Ahn, Y.S.; Yoon, J.H. external Airborne-agent exposure increase Risk of Digestive tract cancer. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Bettcher, B.M.; Kramer, J.H. Longitudinal inflammation, cognitive decline, and Alzheimer’s disease: A mini-review. Clin. Pharmacol. Ther. 2014, 96, 464–469. [Google Scholar] [CrossRef] [Green Version]
- Teunissen, C.E.; van Boxtel, M.P.J.; Bosma, H.; Bosmans, E.; Delanghe, J.; De Bruijn, C.; Wauters, A.; Maes, M.; Jolles, J.; Steinbusch, H.W.M.; et al. Inflammation markers in relation to cognition in a healthy aging population. J. Neuroimmunol. 2003, 134, 142–150. [Google Scholar] [CrossRef]
- Lin, Q.; Rosenberg, M.D.; Yoo, K.; Hsu, T.W.; O’Connell, T.P.; Chun, M.M. Resting-state functional connectivity predicts cognitive impairment related to Alzheimer’s disease. Front. Aging Neurosci. 2018, 10, 94. [Google Scholar] [CrossRef]
- Sankowski, R.; Mader, S.; Valdés-Ferrer, S.I. Systemic inflammation and the brain: Novel roles of genetic, molecular, and environmental cues as drivers of neurodegeneration. Front. Cell. Neurosci. 2015, 9, 28. [Google Scholar] [CrossRef] [Green Version]
- Varatharaj, A.; Liljeroth, M.; Cramer, S.; Stuart, C.; Zotova, E.; Darekar, A.; Larsson, H.; Galea, I. Systemic inflammation and blood–brain barrier abnormality in relapsing–remitting multiple sclerosis. Lancet 2017, 389, S96. [Google Scholar] [CrossRef] [Green Version]
- Brydon, L.; Harrison, N.A.; Walker, C.; Steptoe, A.; Critchley, H.D. Peripheral inflammation is associated with altered substantia nigra activity and psychomotor slowing in humans. Biol. Psychiatry 2008, 63, 1022–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanc, P.D.; Iribarren, C.; Trupin, L.; Earnest, G.; Katz, P.P.; Balmes, J.; Sidney, S.; Eisner, M.D. Occupational exposures and the risk of COPD: Dusty trades revisited. Thorax 2009, 64, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Hazard Prevention and Control in the Work Environment: Airborne Dust; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]



{kind=link}
{kind=link}
| Total Participants, n (% of Column) | Dementia, n (% of Row) | p-Value | ||
|---|---|---|---|---|
| No | Yes | |||
| Total participants | 514,580 (100.0) | 488,530 (94.9) | 26,050 (5.1) | |
| Sex | <0.0001 | |||
| Male | 278,967 (54.2) | 269,131 (96.5) | 9836 (3.5) | |
| Female | 235,613 (45.8) | 219,399 (93.1) | 16,214 (6.9) | |
| Age (years) at baseline | <0.0001 | |||
| ~50 | 236,960 (46.0) | 235,987 (99.6) | 973 (0.4) | |
| 51–60 | 144,987 (28.2) | 140,954 (97.2) | 4033 (2.8) | |
| >60 | 132,633 (25.8) | 111,589 (84.1) | 21,044 (15.9) | |
| Severe external airborne dust exposure | <0.0001 | |||
| No | 513,240 (99.7) | 487,301 (95.0) | 25,939 (5.0) | |
| Yes | 1340 (0.3) | 1229 (91.7) | 111 (8.3) | |
| Incidence (Cases, %) | SIR (95% CI) | ||
|---|---|---|---|
| Severe External Airborne Dust Exposure | |||
| No | Yes | ||
| Dementia (F00-03) * | 25,939 (5.0) | 111 (8.3) | 1.04 (0.85–1.24) |
| Dementia in Alzheimer’s disease (F00) | 15,828 (3.0) | 80 (6.0) | 1.24 (1.01–1.49) |
| Vascular dementia (F01) | 3541 (0.7) | 12 (0.9) | 0.88 (0.37–1.32) |
| Dementia in other diseases classified elsewhere (F02) | 428 (0.1) | 2 (0.1) | 1.16 (0.01–2.77) |
| Unspecified dementia (F03) | 6142 (1.2) | 17 (1.3) | 0.69 (0.36–1.02) |
| Total Participants n (% of Column) | Dementia Screening Test n (% of Row) | p-Value | ||
|---|---|---|---|---|
| Negative | Positive | |||
| Total participants | 58,307 (100.0) | 48,463 (83.1) | 9844 (16.9) | |
| Sex | <0.0001 | |||
| Male | 29,018 (49.7) | 24,870 (88.7) | 4148 (14.3) | |
| Female | 29,289 (50.3) | 23,593 (80.6) | 5696 (19.5) | |
| Age (years) at baseline | <0.0001 | |||
| ~60 | 43,698 (74.9) | 37,313 (85.4) | 6385 (14.6) | |
| >60 | 14,609 (25.1) | 11,150 (76.3) | 3459 (23.7) | |
| Household income level | 0.4097 | |||
| Lowest | 10,685 (18.3) | 8917 (83.5) | 1768 (16.5) | |
| Moderate-low | 10,679 (18.3) | 8847 (82.9) | 1832 (17.1) | |
| Moderate-high | 18,208 (31.2) | 15,003 (82.4) | 3205 (17.6) | |
| Highest | 18,735 (32.2) | 15,696 (83.8) | 3039 (16.2) | |
| Cerebral vascular disease | <0.0001 | |||
| No | 55,648 (95.4) | 46,527 (83.6) | 9121 (16.4) | |
| Yes | 2659 (4.6) | 1936 (72.8) | 723 (27.2) | |
| Cardiovascular disease | <0.0001 | |||
| No | 53,519 (91.8) | 44,714 (83.6) | 8805 (16.5) | |
| Yes | 4788 (8.2) | 3749 (78.3) | 1039 (21.7) | |
| Body mass index | 0.0545 | |||
| Underweight (<18.5 kg/m2) | 1122 (1.9) | 917 (81.7) | 205 (18.3) | |
| Normal (18.5–24.9 kg/m2) | 35,112 (60.2) | 29,125 (82.9) | 5987 (17.1) | |
| Overweight (≥25 kg/m2) | 22,073 (37.9) | 18,421 (83.5) | 3652 (16.5) | |
| Smoking | 0.0003 | |||
| Never or past | 51,729 (88.7) | 42,892 (82.9) | 8837 (17.1) | |
| Current | 6578 (11.3) | 5571 (84.7) | 1007 (15.3) | |
| Drinking | 0.3095 | |||
| Never or moderate | 51,121 (87.7) | 42,460 (83.1) | 8661 (16.9) | |
| Severe | 7186 (12.3) | 6003 (83.6) | 1183 (16.5) | |
| Severe external airborne dust exposure | 0.0011 | |||
| No | 58,084 (95.6) | 48,304 (82.8) | 9800 (17.2) | |
| Yes | 223 (0.4) | 167 (74.9) | 56 (25.1) | |
| Severe External Airborne Dust Exposure | Odds Ratio (95% Confidence Interval) | |
|---|---|---|
| Model 1 | Model 2 | |
| No | Reference | Reference |
| Yes | 1.45 (1.04–2.03) | 1.42 (1.02–1.98) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Choi, J.Y.; Yoon, J.-H.; Lee, W. Effect of Severe External Airborne Agents’ Exposure on Dementia. J. Clin. Med. 2020, 9, 4069. https://doi.org/10.3390/jcm9124069
Lee S, Choi JY, Yoon J-H, Lee W. Effect of Severe External Airborne Agents’ Exposure on Dementia. Journal of Clinical Medicine. 2020; 9(12):4069. https://doi.org/10.3390/jcm9124069
Chicago/Turabian StyleLee, Seunghyun, Joon Yul Choi, Jin-Ha Yoon, and Wanhyung Lee. 2020. "Effect of Severe External Airborne Agents’ Exposure on Dementia" Journal of Clinical Medicine 9, no. 12: 4069. https://doi.org/10.3390/jcm9124069
APA StyleLee, S., Choi, J. Y., Yoon, J. -H., & Lee, W. (2020). Effect of Severe External Airborne Agents’ Exposure on Dementia. Journal of Clinical Medicine, 9(12), 4069. https://doi.org/10.3390/jcm9124069