The Influence of Sex on Clinical Outcomes after Surgical Mitral Valve Replacement in Spain (2001–2015)

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Covariates
2.4. End Points
2.5. Statistical Analysis
3. Results
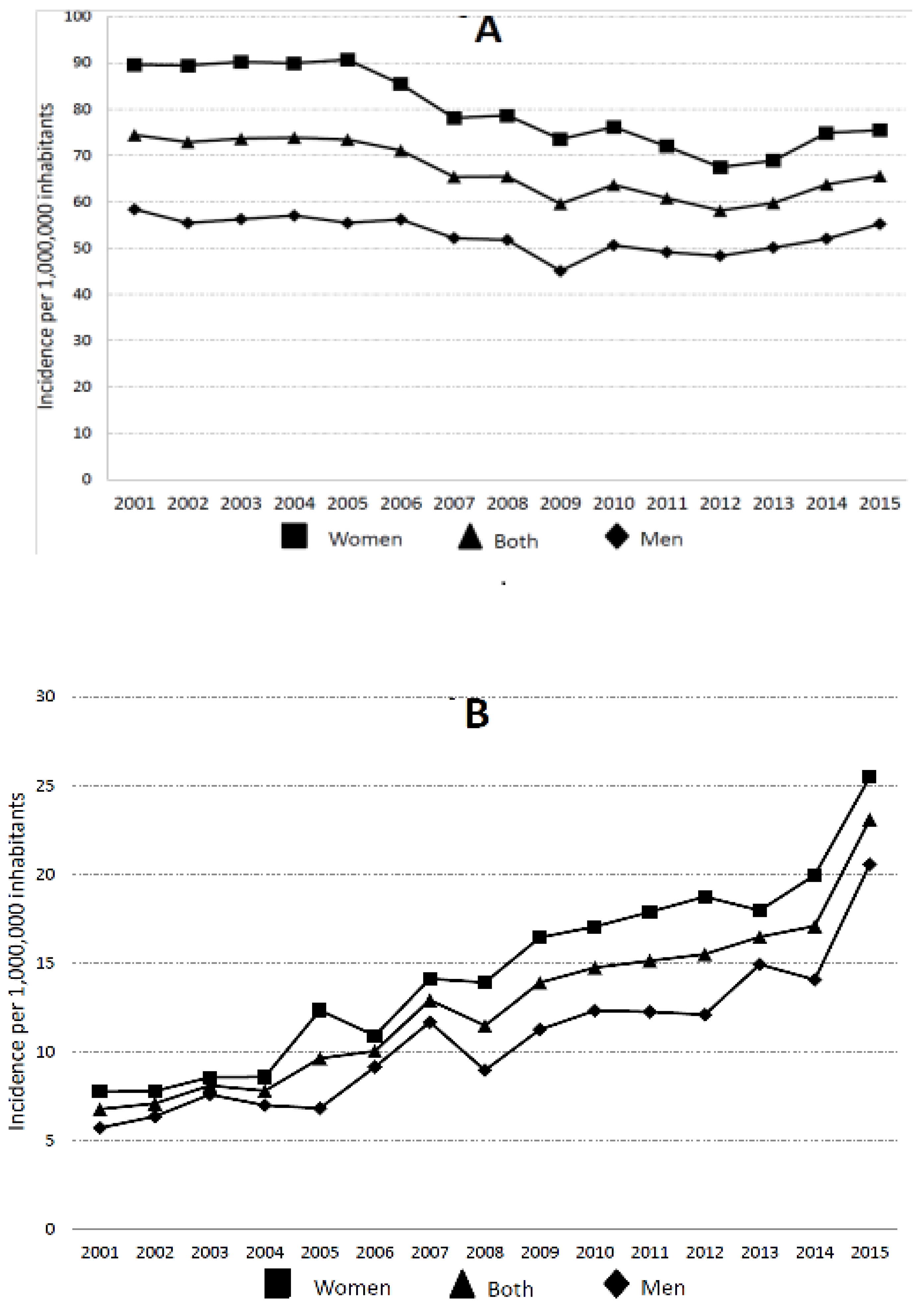
3.1. Temporal Trends in Mechanical Mitral Valve Replacement Hospitalizations
3.2. Differences between Patients Admitted for Mechanical versus Bioprosthetic Mitral Valve Replacement
3.3. Factors Associated with IHM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lancellotti, P.; Rosenhek, R.; Pibarot, P.; Iung, B.; Otto, C.M.; Tornos, P.; Donal, E.; Prendergast, B.; Magne, J.; La Canna, G.; et al. ESC Working Group on Valvular Heart Disease Position Paper--heart valve clinics: Organization, structure, and experiences. Eur. Heart J. 2013, 34, 1597–1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Beaudoin, J.; Dal-Bianco, J.P.; Aikawa, E.; Bischoff, J.; Guerrero, J.L.; Sullivan, S.; Bartko, P.E.; Handschumacher, M.D.; Kim, D.H.; Wylie-Sears, J.; et al. Mitral Leaflet Changes Following Myocardial Infarction: Clinical Evidence for Maladaptive Valvular Remodeling. Circ. Cardiovasc. Imaging 2017, 10, e006512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, J.G.; Anyanwu, A.C.; Fuster, V.; Adams, D.H. A near 100% repair for future guidelines. J. Thorac. Cardiovasc. Surg. 2012, 144, 308–312. [Google Scholar] [CrossRef] [Green Version]
- Jamieson, W.R.E.; Gudas, V.M.; Burr, L.H.; Janusz, M.T.; Fradet, G.J.; Ling, H.; Germann, E.; Lichtenstein, S.V. Mitral valve disease: If the mitral valve is not reparable/failed repair, is bioprosthesis suitable for replacement? Eur. J. Cardio-Thoracic Surg. 2009, 35, 104–110. [Google Scholar] [CrossRef]
- Meier, S.; Seeburger, J.; Borger, M.A. Advances in Mitral Valve Surgery. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 75. [Google Scholar] [CrossRef]
- Acker, M.A.; Parides, M.K.; Perrault, L.P.; Moskowitz, A.J.; Gelijns, A.C.; Voisine, P.; Smith, P.K.; Hung, J.W.; Blackstone, E.H.; Puskas, J.D.; et al. Mitral-Valve Repair versus Replacement for Severe Ischemic Mitral Regurgitation. N. Engl. J. Med. 2014, 370, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Munoz, D.; et al. 2017 ESC/EACTS guidelines for the management of valvular heart disease: The task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Seeburger, J.; Eifert, S.; Pfannmüller, B.; Garbade, J.; Vollroth, M.; Misfeld, M.; Borger, M.; Mohr, F.W. Gender differences in mitral valve surgery. Thorac. Cardiovasc. Surg. 2013, 61, 42–46. [Google Scholar] [PubMed]
- Wong, S.C.; Yeo, I.; Bergman, G.; Feldman, D.N.; Singh, H.; Minutello, R.; Kim, L.K. The influence of gender on in-hospital clinical outcome following isolated mitral or aortic heart valve surgery. Cardiovasc. Revasc. Med. 2019, 20, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Vassileva, C.M.; McNeely, C.; Mishkel, G.; Boley, T.; Markwell, S.; Hazelrigg, S. Gender differences in long-term survival of Medicare beneficiaries undergoing mitral valve operations. Ann. Thorac. Surg. 2013, 96, 1367–1373. [Google Scholar] [CrossRef]
- Instituto Nacional de Gestión Sanitaria, Ministerio de Sanidad, Servicios Sociales e Igualdad. Conjunto Mínimo Básico de Datos, Hospitales del INSALUD. Available online: http://www.ingesa.msssi.gob.es/estadEstudios/documPublica/CMBD-2001.htm (accessed on 15 August 2020).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Newman, J.D.; Wilcox, T.; Smilowitz, N.R.; Berger, J.S. Influence of Diabetes on Trends in Perioperative Cardiovascular Events. Diabetes Care 2018, 41, 1268–1274. [Google Scholar] [CrossRef] [Green Version]
- López-de-Andrés, A.; Perez-Farinos, N.; de Miguel-Díez, J.; Hernández-Barrera, V.; Méndez-Bailón, M.; de Miguel-Yanes, J.M.; Jiménez-García, R. Impact of type 2 diabetes mellitus in the utilization and in-hospital outcomes of surgical aortic valve replacement in Spain (2001–2015). Cardiovasc. Diabetol. 2018, 17, 135. [Google Scholar] [CrossRef]
- Gammie, J.S.; Sheng, S.; Griffith, B.P.; Peterson, E.D.; Rankin, J.S.; O’Brien, S.M.; Brown, J.M. Trends in mitral valve surgery in the United States: Results from the Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann. Thorac. Surg. 2009, 87, 1431–1437. [Google Scholar] [CrossRef]
- Marchand, M.A.; Aupart, M.R.; Norton, R.; Goldsmith, I.R.; Pelletier, L.C.; Pellerin, M.; Dubiel, T.; Daenen, W.J.; Herijgers, P.; Casselman, F.P.; et al. Fifteen-year experience with the mitral Carpentier-Edwards PERIMOUNT pericardial bioprosthesis. Ann. Thorac. Surg. 2001, 71, S236–S239. [Google Scholar] [CrossRef]
- Jamieson, W.R.E.; Burr, L.H.; Miyagishima, R.T.; Fradet, G.J.; Janusz, M.T.; Tyers, G.F.O.; Macnab, J.; Chan, F. Structural deterioration in Carpentier-Edwards standard and supraannular porcine bioprostheses. Ann. Thorac. Surg. 1995, 60, S241–S247. [Google Scholar] [CrossRef]
- Fujita, B.; Ensminger, S.; Bauer, T.; Möllmann, H.; Beckmann, A.; Bekeredjian, R.; Bleiziffer, S.; Schäfer, E.; Hamm, C.W.; Mohr, F.W.; et al. Trends in practice and outcomes from 2011 to 2015 for surgical aortic valve replacement: An update from the German Aortic Valve Registry on 42 776 patients. Eur. J. Cardiothorac. Surg. 2018, 53, 552–559. [Google Scholar] [CrossRef]
- Isaacs, A.J.; Shuhaiber, J.; Salemi, A.; Isom, O.W.; Sedrakyan, A. National trends in utilization and in-hospital outcomes of mechanical versus bioprosthetic aortic valve replacements. J. Thorac. Cardiovasc. Surg. 2015, 149, 1262–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kislitsina, O.N.; Zareba, K.M.; Bonow, R.O.; Andrei, A.C.; Kruse, J.; Puthumana, J.; Akhter, N.; Malaisrie, S.C.; McCarthy, P.M.; Rigolin, V.H. Is mitral valve disease treated differently in men and women? Eur. J. Prev. Cardiol. 2019, 26, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.F.; Paparella, D.; Ivanov, J.; Buchanan, M.R.; Brister, S.J. Gender-related differences in morbidity and mortality during combined valve and coronary surgery. J. Thorac. Cardiovasc. Surg. 2003, 126, 959–964. [Google Scholar] [CrossRef] [Green Version]
- Potapov, E.V.; Loebe, M.; Anker, S.; Stein, J.; Bondy, S.; Nasseri, B.A.; Sodian, R.; Hausmann, H.; Hetzer, R. Impact of body mass index on outcome in patients after coronary artery bypass grafting with and without valve surgery. Eur. Heart J. 2003, 24, 1933–1941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavie, C.J.; McAuley, P.A.; Church, T.S.; Milani, R.V.; Blair, S.N. Obesity and cardiovascular diseases: Implications regarding fitness, fatness, and severity in the obesity paradox. J. Am. Coll. Cardiol. 2014, 63, 1345–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendez-Bailon, M.; Lorenzo-Villalba, N.; Muñoz-Rivas, N.; de Miguel-Yanes, J.M.; De Miguel-Diez, J.; Comín-Colet, J.; Hernandez-Barrera, V.; Jiménez-García, R.; Lopez-De-Andres, A. Transcatheter aortic valve implantation and surgical aortic valve replacement among hospitalized patients with and without type 2 diabetes mellitus in Spain (2014–2015). Cardiovasc. Diabetol. 2017, 16, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodson, J.A.; Wang, Y.; Desai, M.M.; Barreto-Filho, J.A.; Sugeng, L.; Hashim, S.W.; Krumholz, H.M. Outcomes for mitral valve surgery among Medicare fee-for-service beneficiaries, 1999 to 2008. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Silaschi, M.; Conradi, L.; Treede, H.; Reiter, B.; Schaefer, U.; Blankenberg, S.; Reichenspurner, H. Trends in surgical aortic valve replacement in more than 3000 consecutive cases in the era of transcatheter aortic valve implantations. Thorac. Cardiovasc. Surg. 2016, 64, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Song, H.K.; Grab, J.D.; O’Brien, S.M.; Welke, K.F.; Edwards, F.; Ungerleider, R.M. Gender differences in mortality after mitral valve operation: Evidence for higher mortality in perimenopausal women. Ann. Thorac. Surg. 2008, 85, 2040–2044. [Google Scholar] [CrossRef]
- Chaker, Z.; Badhwar, V.; Alqahtani, F.; Aljohani, S.; Zack, C.J.; Holmes, D.R.; Rihal, C.S.; Alkhouli, M. Sex differences in the utilization and outcomes of surgical aortic valve replacement for severe aortic stenosis. J. Am. Heart Assoc. 2017, 6, e006370. [Google Scholar] [CrossRef]
- Avierinos, J.F.; Inamo, J.; Grigioni, F.; Gersh, B.; Shub, C.; Enriquez-Sarano, M. Sex differences in morphology and outcomes of mitral valve prolapse. Ann. Intern. Med. 2008, 149, 787–795. [Google Scholar] [CrossRef] [PubMed]
- De Bonis, M.; Lapenna, E.; Barili, F.; Nisi, T.; Calabrese, M.; Pappalardo, F.; La Canna, G.; Pozzoli, A.; Buzzatti, N.; Giacomini, A.; et al. Long-term results of mitral repair in patients with severe left ventricular dysfunction and secondary mitral regurgitation: Does the technique matter? Eur. J. Cardio-Thorac. Surg. 2016, 50, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Ribera, A.; Marsal, J.R.; Ferreira-González, I.; Cascant, P.; Pons, J.M.; Mitjavila, F.; Salas, T.; Permanyer-Miralda, G. Predicting in-hospital mortality with coronary bypass surgery using hospital discharge data: Comparison with a prospective observational study. Rev. Esp. Cardiol. 2008, 61, 843–852. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 2001–2003 | 2004–2006 | 2007–2009 | 2010–2012 | 2013–2015 | Total | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Charlson Comorbidity Index, mean (SD) * | Men | 0.90 (0.9) | 1.00 (0.9) | 1.03 (0.9) | 1.07 (1.0) | 1.15 (1.0) | 1.03 (0.9) | <0.001 |
| Women | 0.80 (0.9) | 0.92 (0.9) | 0.96 (0.9) | 0.99 (0.9) | 1.09 (1.0) | 0.95 (0.9) | <0.001 | |
| Chronic obstructive pulmonary disease, n (%) * | Men | 328 (11) | 371 (12) | 307 (11) | 311 (11) | 315 (11) | 1632 (11) | 0.304 |
| Women | 149 (3) | 173 (3) | 139 (3) | 176 (4) | 157 (4) | 794 (3) | 0.063 | |
| Type 2 diabetes mellitus, n (%) * | Men | 262 (9) | 360 (12) | 421(15) | 441 (16) | 521 (18) | 2005 (14) | <0.001 |
| Women | 623 (13) | 807 (16) | 785 (18) | 765 (18) | 785 (18) | 3765 (16) | <0.001 | |
| Peripheral vascular disease, n (%) * | Men | 95 (3) | 158 (5) | 175 (6) | 184 (6) | 196 (7) | 808 (6) | <0.001 |
| Women | 58 (1) | 72 (1) | 97 (2) | 84 (2) | 129 (3) | 440 (2) | <0.001 | |
| Acute renal disease, n (%) | Men | 264 (9) | 309 (10) | 366 (13) | 447 (16) | 563 (19) | 1949 (13) | <0.001 |
| Women | 261 (5) | 315 (6) | 388 (9) | 487 (11) | 534 (12) | 1985 (9) | <0.001 | |
| Cerebrovascular disease, n (%) * | Men | 123 (4) | 131 (4) | 117 (4) | 121 (4) | 186 (6) | 678 (5) | <0.001 |
| Women | 217 (4) | 226 (5) | 208 (5) | 215 (5) | 240 (5) | 1106 (5) | 0.145 | |
| Congestive heart failure, n (%) * | Men | 610 (21) | 671 (22) | 633 (23) | 655 (23) | 810 (27) | 3379 (23) | <0.001 |
| Women | 907 (19) | 953 (19) | 884 (20) | 821 (19) | 1050 (24) | 4615 (20) | <0.001 | |
| Atrial fibrillation, n (%) * | Men | 1334 (47) | 1502 (50) | 1346 (48) | 1385 (50) | 1494 (51) | 7061 (49) | 0.026 |
| Women | 2780 (58) | 3148 (64) | 2862 (64) | 2714 (63) | 2822 (65) | 14,326 (63) | <0.001 | |
| Pulmonary hypertension, n (%) * | Men | 576 (20) | 630 (21) | 578 (21) | 564 (20) | 626 (21) | 2974 (21) | 0.759 |
| Women | 1351 (28) | 1632 (33) | 1463 (33) | 1386 (32) | 1469 (34) | 7301 (32) | <0.001 | |
| Coronary artery disease, n (%) * | Men | 749 (26) | 820 (27) | 747 (27) | 811 (29) | 899 (30) | 4026 (28) | 0.002 |
| Women | 554 (12) | 654 (13) | 580 (13) | 527 (12) | 562 (13) | 2877 (13) | 0.111 | |
| Obesity, n (%) * | Men | 86 (3) | 110 (4) | 112 (4) | 174 (6) | 209 (7) | 691 (5) | <0.001 |
| Women | 271 (6) | 355 (7) | 371 (8) | 402 (9) | 450 (10) | 1849 (8) | <0.001 | |
| Cardiogenic shock, n (%) * | Men | 136 (5) | 135 (4) | 139 (5) | 169 (6) | 172 (6) | 751 (5) | 0.033 |
| Women | 135 (3) | 151 (3) | 149 (3) | 149 (3) | 111 (3) | 695 (3) | 0.082 | |
| Gastrointestinal hemorrhage, n (%) | Men | 17 (1) | 13 (0) | 11 (0) | 12 (0) | 11 (0) | 64 (0) | 0.740 |
| Women | 17 (0) | 17 (0) | 20 (0) | 20 (0) | 8 (0) | 82 (0) | 0.192 | |
| Endocarditis, n (%) * | Men | 334 (12) | 377 (13) | 448 (16) | 465 (16) | 602 (20) | 2226 (15) | <0.001 |
| Women | 244 (5) | 278 (6) | 326 (7) | 370 (9) | 405 (9) | 1623 (7) | <0.001 | |
| Pneumonia, n (%) * | Men | 101 (3) | 123 (4) | 105 (4) | 85 (3) | 70 (2) | 484 (3) | 0.002 |
| Women | 122 (3) | 133 (3) | 121 (3) | 84 (2) | 75 (2) | 535 (2) | 0.003 | |
| Renal disease, n (%) * | Men | 158 (5) | 213 (7) | 204 (7) | 255 (9) | 272 (9) | 1102 (8) | <0.001 |
| Women | 133 (3) | 203 (4) | 216 (5) | 247 (6) | 324 (7) | 1123 (5) | <0.001 | |
| Liver disease, n (%) * | Men | 94 (3) | 111 (4) | 120 (4) | 150 (5) | 170 (6) | 645 (4) | <0.001 |
| Women | 95 (2) | 129 (3) | 130 (3) | 153 (4) | 170 (4) | 677 (3) | <0.001 | |
| Cancer, n (%) * | Men | 21 (1) | 44 (1) | 37 (1) | 41 (1) | 49 (2) | 192 (1) | 0.027 |
| Women | 21 (0) | 32 (1) | 34 (1) | 29 (1) | 26 (1) | 142 (1) | 0.371 | |
| Weight loss, n (%) | Men | 2 (0) | 22 (1) | 15 (0) | 9 (0) | 18 (1) | 66 (0) | 0.002 |
| Women | 6 (0) | 25 (0) | 16 (0) | 22 (0) | 17 (0) | 86 (0) | 0.015 |
| 2001–2003 | 2004–2006 | 2007–2009 | 2010–2012 | 2013–2015 | Total | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Number of procedures (Incidence per 1,000,000 inhabitants) | Men | 332 (7) | 410 (8) | 595 (11) | 697 (12) | 928 (17) | 2962 (11) | <0.001 |
| Women | 428 (8) | 593 (11) | 862 (15) | 1065 (18) | 1253 (21) | 4201 (15) | <0.001 | |
| Both | 760 (7) | 1003 (9) | 1457 (13) | 1762 (15) | 2181 (19) | 7163 (13) | <0.001 | |
| Age, mean (SD) * | Men | 70.2 (11.0) | 70.2 (10.4) | 71.4 (10.4) | 72.8 (8.8) | 73.6 (7.9) | 72.1 (9.5) | <0.001 |
| Women | 71.0 (9.9) | 72.5 (8.4) | 72.7 (9.2) | 74.0 (8.1) | 74.6 (7.3) | 73.4 (8.4) | <0.001 | |
| Rheumatic mitral insufficiency, n (%) | Men | 15 (5) | 18 (4) | 21 (3) | 22 (3) | 27 (3) | 102 (3) | 0.732 |
| Women | 16 (4) | 24 (4) | 32 (4) | 30 (3) | 33 (3) | 180 (4) | 0.580 | |
| Coronary artery bypass graft, n (%) * | Men | 72 (22) | 91 (22) | 142 (24) | 182 (26) | 261 (28) | 748 (25) | 0.056 |
| Women | 63 (15) | 83 (14) | 113 (13) | 142 (13) | 148 (12) | 549 (13) | 0.511 | |
| Surgical aortic valve replacement, n (%) * | Men | 87 (26) | 146 (36) | 227 (38) | 266 (38) | 343 (37) | 1069 (36) | 0.002 |
| Women | 125 (29) | 188 (32) | 274 (32) | 362 (34) | 445 (35) | 1394 (33) | 0.100 | |
| Other valve procedures: pulmonary or tricuspid valves, n (%) * | Men | 41 (12) | 58 (14) | 110 (19) | 140 (20) | 213 (23) | 562 (19) | <0.001 |
| Women | 90 (21) | 169 (28) | 287 (33) | 376 (35) | 449 (36) | 1371 (33) | <0.001 | |
| Intra-aortic balloon counterpulsation, n (%) * | Men | 23 (7) | 31 (8) | 48 (8) | 54 (8) | 60 (6) | 216 (7) | 0.774 |
| Women | 16 (4) | 20 (3) | 39 (4) | 45 (4) | 60 (5) | 180 (4) | 0.659 | |
| Pacemaker implantation, n (%) * | Men | 23 (7) | 28 (7) | 47 (8) | 49 (7) | 82 (9) | 229 (8) | 0.581 |
| Women | 19 (4) | 29 (5) | 45 (5) | 66 (6) | 77 (6) | 236 (6) | 0.509 | |
| Blood transfusion, n (%) | Men | 67 (20) | 97 (24) | 140 (23) | 195 (28) | 288 (31) | 787 (27) | <0.001 |
| Women | 100 (23) | 150 (25) | 198 (23) | 303 (28) | 367 (29) | 1118 (27) | 0.004 | |
| Length of hospital stay, mean (SD) * | Men | 29.0 (25) | 27.3 (24) | 26.7 (25) | 26.4 (25) | 24.2 (24) | 26.2 (25) | 0.019 |
| Women | 25.3 (22) | 25.7 (25) | 25.0 (26) | 22.7 (22) | 20.5 (17) | 23.2 (22) | <0.001 | |
| In-hospital mortality, n (%) * | Men | 61 (18) | 59 (14) | 118 (20) | 104 (15) | 129 (14) | 471 (16) | 0.015 |
| Women | 79 (18) | 84 (14) | 123 (14) | 154 (14) | 148 (12) | 588 (14) | 0.015 | |
| MACCE, n (%) * | Men | 88 (26) | 83 (20) | 151 (25) | 138 (20) | 168 (18) | 628 (21) | 0.001 |
| Women | 93 (22) | 110 (18) | 154 (18) | 195 (18) | 192 (15) | 744 (18) | 0.037 |
| 2001–2003 | 2004–2006 | 2007–2009 | 2010–2012 | 2013–202015 | Total | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Charlson Comorbidity Index, mean (SD) * | Men | 1.11 (1.1) | 1.17 (1.0) | 1.24 (1.0) | 1.24 (1.0) | 1.37 (1.1) | 1.26 (1.0) | <0.001 |
| Women | 0.93 (0.9) | 1.04 (0.9) | 1.14 (1.0) | 1.10 (1.0) | 1.23 (1.0) | 1.12 (1.0) | <0.001 | |
| Chronic obstructive pulmonary disease, n (%) | Men | 47 (14) | 61 (15) | 81 (14) | 89 (13) | 143 (15) | 421 (14) | 0.626 |
| Women | 10 (2) | 18 (3) | 26 (3) | 35 (3) | 38 (3) | 127 (3) | 0.919 | |
| Type 2 diabetes mellitus, n (%) * | Men | 52 (16) | 64 (16) | 102 (17) | 116 (17) | 172 (18) | 506 (17) | 0.631 |
| Women | 69 (16) | 99 (17) | 174 (20) | 202 (19) | 247 (18) | 791 (19) | 0.239 | |
| Peripheral vascular disease, n (%) * | Men | 18 (5) | 24 (6) | 37 (6) | 69 (10) | 69 (7) | 217 (7) | 0.027 |
| Women | 9 (2) | 13 (2) | 33 (4) | 39 (4) | 35 (3) | 129 (3) | 0.190 | |
| Acute renal disease, n (%) | Men | 54 (16) | 81 (20) | 116 (19) | 170 (24) | 242 (26) | 663 (22) | <0.001 |
| Women | 41 (10) | 62 (10) | 124 (15) | 164 (15) | 233 (19) | 624 (15) | <0.001 | |
| Cerebrovascular disease, n (%) | Men | 14 (4) | 22 (5) | 22 (4) | 46 (7) | 45 (5) | 149 (5) | 0.170 |
| Women | 17 (4) | 30 (5) | 36 (4) | 63 (6) | 75 (6) | 221 (5) | 0.219 | |
| Congestive heart failure, n (%) * | Men | 81 (24) | 107 (26) | 170 (29) | 196 (28) | 310 (33) | 864 (29) | 0.007 |
| Women | 110 (26) | 157 (26) | 222 (26) | 270 (25) | 383 (31) | 1142 (27) | 0.032 | |
| Atrial fibrillation, n (%) * | Men | 123 (37) | 176 (43) | 283 (48) | 332 (48) | 474 (51) | 1388 (47) | <0.001 |
| Women | 217 (51) | 379 (64) | 529 (61) | 655 (61) | 829 (66) | 2609 (62) | <0.001 | |
| Pulmonary hypertension, n (%) * | Men | 52 (16) | 87 (21) | 138 (23) | 148 (21) | 238 (26) | 663 (22) | 0.004 |
| Women | 104 (24) | 200 (34) | 317 (37) | 329 (31) | 431 (34) | 1381 (33) | <0.001 | |
| Coronary artery disease, n (%) * | Men | 109 (33) | 151 (37) | 218 (37) | 249 (36) | 365 (39) | 1092 (37) | 0.272 |
| Women | 92 (21) | 139 (23) | 176 (20) | 248 (23) | 273 (22) | 928 (22) | 0.546 | |
| Obesity, n (%) * | Men | 7 (2) | 11 (3) | 23 (4) | 38 (5) | 54 (6) | 133 (4) | 0.010 |
| Women | 29 (7) | 34 (6) | 59 (7) | 75 (7) | 114 (9) | 311 (7) | 0.075 | |
| Cardiogenic shock, n (%) * | Men | 23 (7) | 29 (7) | 39 (6) | 47 (7) | 54 (6) | 192 (6) | 0.894 |
| Women | 24 (6) | 24 (4) | 47 (5) | 44 (4) | 47 (4) | 186 (4) | 0.255 | |
| Gastrointestinal hemorrhage, n (%) | Men | 1 (0) | 4 (1) | 2 (0) | 7 (1) | 3 (0) | 17 (1) | 0.243 |
| Women | 10 (2) | 5 (1) | 3 (0.3) | 4 (0) | 6 (0) | 28 (1) | <0.001 | |
| Endocarditis, n (%) * | Men | 55 (17) | 87 (21) | 133 (22) | 183 (26) | 260 (28) | 718 (24) | <0.001 |
| Women | 47 (11) | 59 (10) | 112 (13) | 188 (18) | 240 (19) | 646 (15) | <0.001 | |
| Pneumonia, n (%) * | Men | 18 (5) | 17 (4) | 28 (5) | 27 (4) | 50 (5) | 140 (5) | 0.611 |
| Women | 23 (5) | 24 (4) | 21 (2) | 26 (2) | 33 (3) | 127 (3) | 0.011 | |
| Renal disease, n (%) * | Men | 24 (7) | 49 (12) | 71 (12) | 87 (12) | 134 (14) | 365 (12) | 0.018 |
| Women | 16 (4) | 36 (6) | 58 (7) | 85 (8) | 141 (11) | 336 (8) | <0.001 | |
| Liver disease, n (%) * | Men | 15 (4) | 15 (4) | 24 (4) | 36 (5) | 55 (6) | 145 (5) | 0.328 |
| Women | 10 (2) | 16 (3) | 27 (3) | 30 (3) | 45 (4) | 128 (3) | 0.655 | |
| Cancer, n (%) * | Men | 6 (2) | 6 (1) | 9 (1) | 16 (2) | 19 (2) | 56 (2) | 0.806 |
| Women | 5 (1) | 2 (0) | 10 (1) | 9 (1) | 7 (1) | 33 (1) | 0.313 | |
| Weight loss, n (%) | Men | 1 (0) | 0 (0) | 2 (0) | 3 (0) | 4 (0) | 10 (0) | 0.769 |
| Women | 0 (0) | 2 (0) | 2 (0) | 5 (0) | 7 (1) | 16 (0) | 0.488 |
| Mechanical Mitral Valve Replacement | Bioprosthetic Mitral Valve Replacement | |||||
|---|---|---|---|---|---|---|
| Men | Women | Both | Men | Women | Both | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Age | 1.06 (1.05–1.06) | 1.05 (1.05–1.06) | 1.05 (1.05–1.06) | 1.03 (1.02–1.05) | 1.03 (1.01–1.04) | 1.03 (1.02–1.04) |
| Surgical aortic valve replacement | 1.24 (1.11–1.38) | 1.17 (1.08–1.27) | 1.32 (1.05–1.67) | 1.22 (0.99–1.52) | 1.26 (1.08–1.48) | |
| Other valve procedures: pulmonary or tricuspid valves | 1.2 (1.03–1.4) | 1.21 (1.08–1.35) | 1.2 (1.1–1.32) | |||
| Intra-aortic balloon counterpulsation | 2.93 (2.4–3.59) | 3.39 (2.71–4.23) | 3.07 (2.65–3.57) | 3.28 (2.32–4.64) | 5.64 (3.88–8.19) | 4.09 (3.18–5.27) |
| Pacemaker implantation | 0.62 (0.46–0.83) | 0.57 (0.43–0.76) | 0.6 (0.49–0.73) | 0.53 (0.32–0.87) | 0.31 (0.16–0.59) | 0.44 (0.3–0.64) |
| Blood transfusion | 1.56 (1.38–1.76) | 1.49 (1.34–1.66) | 1.52 (1.4–1.65) | 1.66 (1.34–2.05) | 1.35 (1.15–1.58) | |
| Peripheral vascular disease | 2.42 (1.49–3.93) | 1.56 (1.14–2.13) | ||||
| Acute Renal disease | 3.58 (3.13–4.08) | 4.25 (3.75–4.83) | 3.92 (3.57–4.29) | 2.54 (2–3.21) | 3.39 (2.68–4.28) | 2.83 (2.4–3.35) |
| Cerebrovascular disease | 1.67 (1.33–2.11) | 1.75 (1.44–2.13) | 1.71 (1.47–1.99) | 1.83 (1.24–2.7) | 1.61 (1.21–2.16) | |
| Congestive heart failure | 1.34 (1.18–1.52) | 1.82 (1.63–2.04) | 1.59 (1.47–1.73) | 1.68 (1.34–2.11) | 1.55 (1.25–1.92) | 1.64 (1.4–1.91) |
| Atrial fibrillation | 0.56 (0.5–0.63) | 0.48 (0.44–0.54) | 0.51 (0.47–0.56) | 0.59 (0.47–0.75) | 0.63 (0.51–0.78) | 0.6 (0.52–0.7) |
| Coronary artery disease | 1.42 (1.21–1.66) | 1.49 (1.31–1.7) | 1.48 (1.32–1.66) | |||
| Cardiogenic shock | 5.09 (4.22–6.15) | 8.17 (6.75–9.89) | 6.38 (5.58–7.29) | 4.5 (3.15–6.43) | 8.83 (6.04–12.91) | 6.09 (4.72–7.87) |
| Gastrointestinal hemorrhage | 2.06 (1.13–3.76) | 3.34 (2–5.58) | 2.74 (1.86–4.05) | |||
| Endocarditis | 2.14 (1.86–2.47) | 1.66 (1.41–1.94) | 1.89 (1.7–2.1) | 1.44 (1.12–1.86) | 1.6 (1.24–2.07) | 1.5 (1.25–1.79) |
| Pneumonia | 2.53 (2.01–3.18) | 3.15 (2.53–3.93) | 2.85 (2.43–3.34) | 2.3 (1.52–3.48) | 4.02 (2.61–6.19) | 2.95 (2.19–3.98) |
| Renal disease | 1.66 (1.39–1.98) | 1.79 (1.5–2.14) | 1.73 (1.53–1.96) | 1.97 (1.45–2.69) | 1.59 (1.28–1.98) | |
| Liver disease | 3.62 (2.93–4.47) | 4.33 (3.53–5.32) | 3.93 (3.4–4.55) | 3.06 (2.04–4.59) | 3.99 (2.55–6.26) | 3.51 (2.6–4.73) |
| Cancer | 1.6 (1.06–2.42) | 1.47 (1.06–2.04) | ||||
| Year | 0.92 (0.90–0.93) | 0.92 (0.91–0.93) | 0.92 (0.91–0.93) | 0.94 (0.92–0.97) | 0.93 (0.9–0.95) | 0.93 (0.92–0.95) |
| Male sex | 1.05 (0.97–1.14) | 1.28 (1.1–1.5) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Rivas, N.; López-de-Andrés, A.; Méndez-Bailón, M.; Andrès, E.; Hernández-Barrera, V.; de Miguel-Yanes, J.M.; Miguel-Díez, J.d.; Lorenzo-Villalba, N.; Jiménez-García, R. The Influence of Sex on Clinical Outcomes after Surgical Mitral Valve Replacement in Spain (2001–2015). J. Clin. Med. 2020, 9, 4108. https://doi.org/10.3390/jcm9124108
Muñoz-Rivas N, López-de-Andrés A, Méndez-Bailón M, Andrès E, Hernández-Barrera V, de Miguel-Yanes JM, Miguel-Díez Jd, Lorenzo-Villalba N, Jiménez-García R. The Influence of Sex on Clinical Outcomes after Surgical Mitral Valve Replacement in Spain (2001–2015). Journal of Clinical Medicine. 2020; 9(12):4108. https://doi.org/10.3390/jcm9124108
Chicago/Turabian StyleMuñoz-Rivas, Nuria, Ana López-de-Andrés, Manuel Méndez-Bailón, Emmanuel Andrès, Valentín Hernández-Barrera, José María de Miguel-Yanes, Javier de Miguel-Díez, Noel Lorenzo-Villalba, and Rodrigo Jiménez-García. 2020. "The Influence of Sex on Clinical Outcomes after Surgical Mitral Valve Replacement in Spain (2001–2015)" Journal of Clinical Medicine 9, no. 12: 4108. https://doi.org/10.3390/jcm9124108
APA StyleMuñoz-Rivas, N., López-de-Andrés, A., Méndez-Bailón, M., Andrès, E., Hernández-Barrera, V., de Miguel-Yanes, J. M., Miguel-Díez, J. d., Lorenzo-Villalba, N., & Jiménez-García, R. (2020). The Influence of Sex on Clinical Outcomes after Surgical Mitral Valve Replacement in Spain (2001–2015). Journal of Clinical Medicine, 9(12), 4108. https://doi.org/10.3390/jcm9124108