Genomic Profiling of Uterine Aspirates and cfDNA as an Integrative Liquid Biopsy Strategy in Endometrial Cancer

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Experimental Section
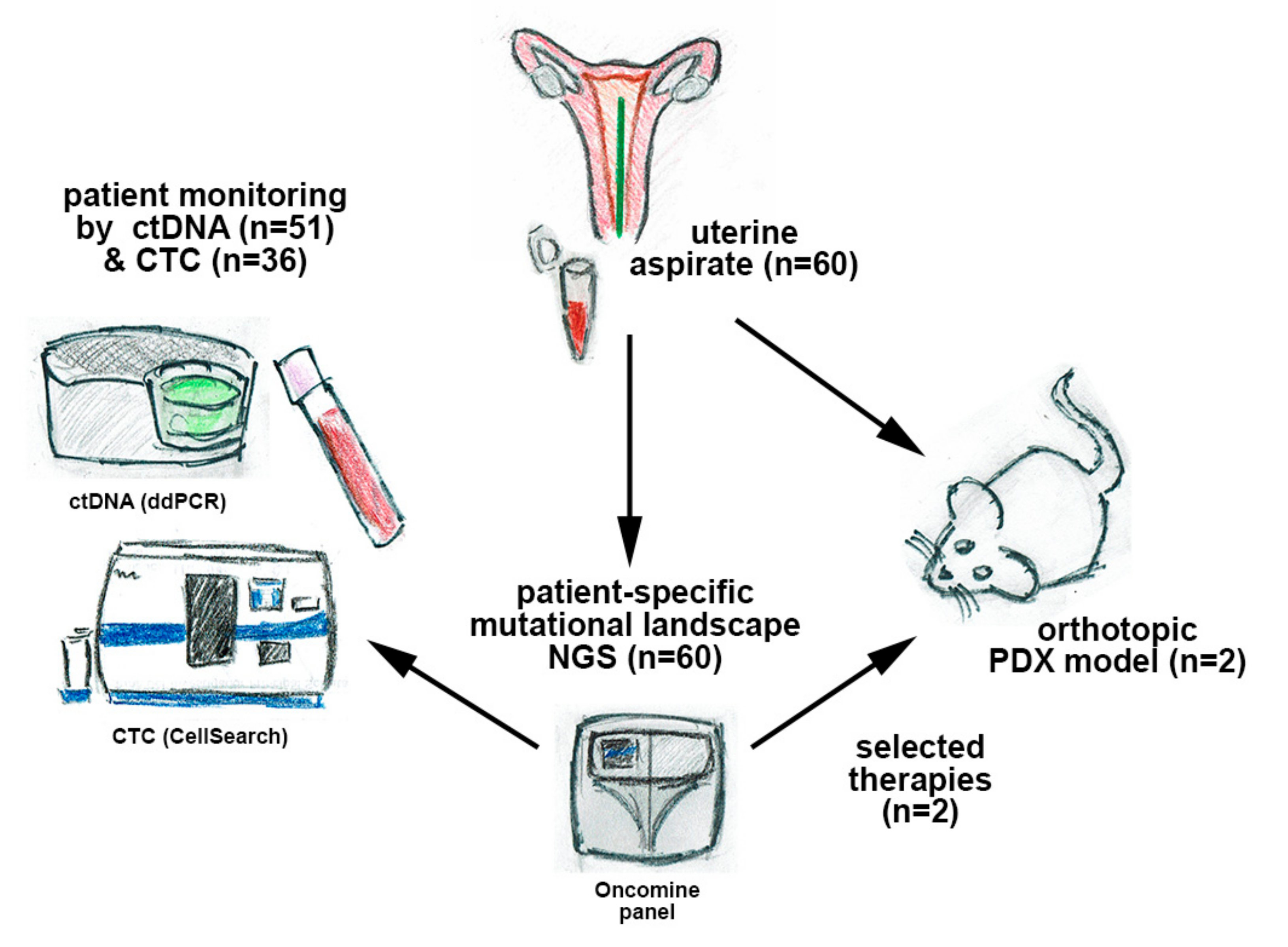
2.1. Patient Inclusion and Sample Collection
2.2. DNA Extraction
2.3. Targeted Sequencing of UA, Personalized Therapy Selection, and ddPCR Assays
2.4. Personalized Therapy Selection
2.5. Detection of ctDNA with ddPCR
2.6. PDX Generation and Therapy Testing
2.7. Statistical Analysis
3. Results
3.1. Clinicopathologic Characteristics of the EC cohort
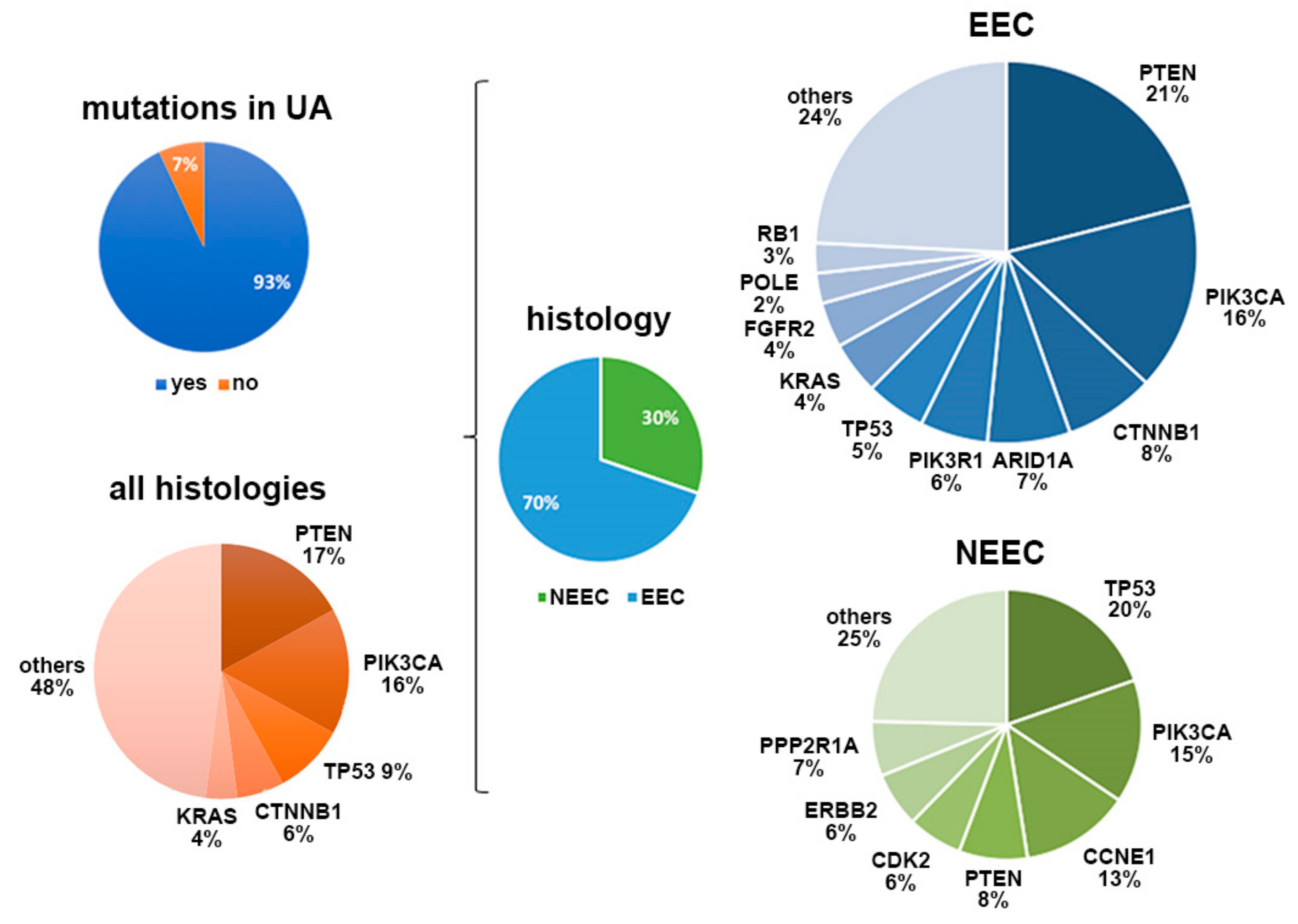
3.2. UA Sequencing to Characterize EC
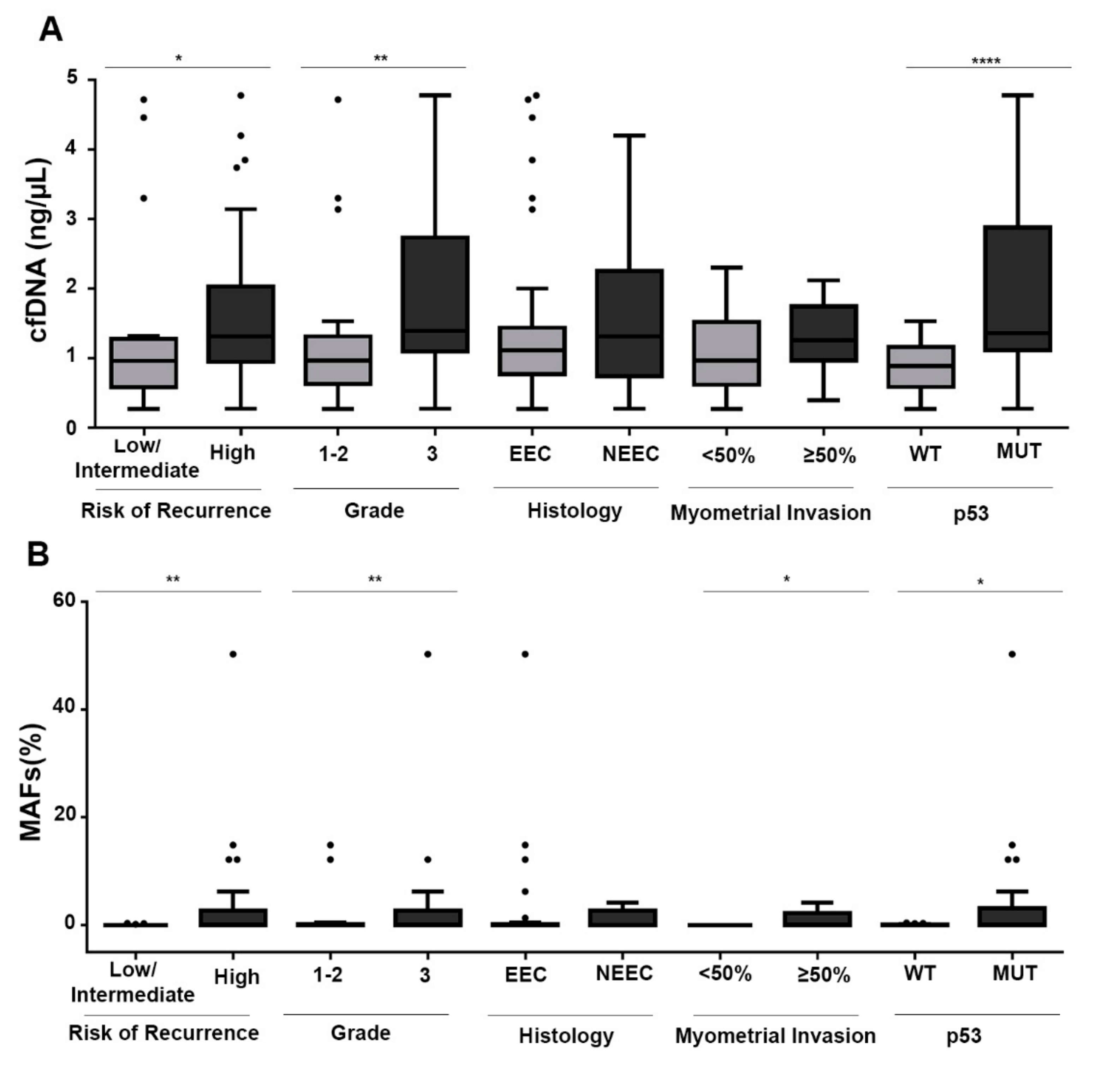
3.3. cfDNA and ctDNA are Associated with Risk Factors in EC
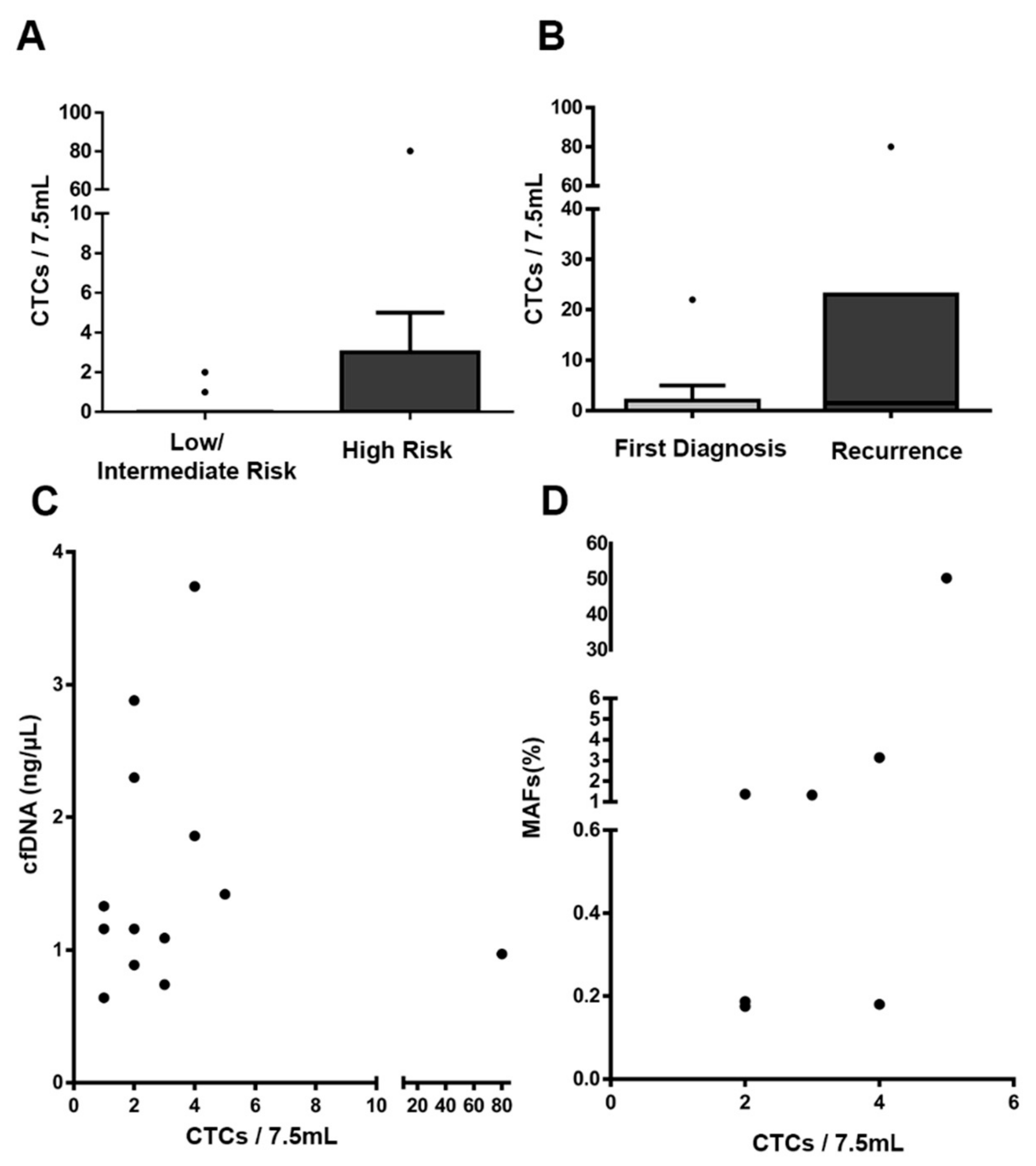
3.4. Additional Value of CTC Enumeration in EC
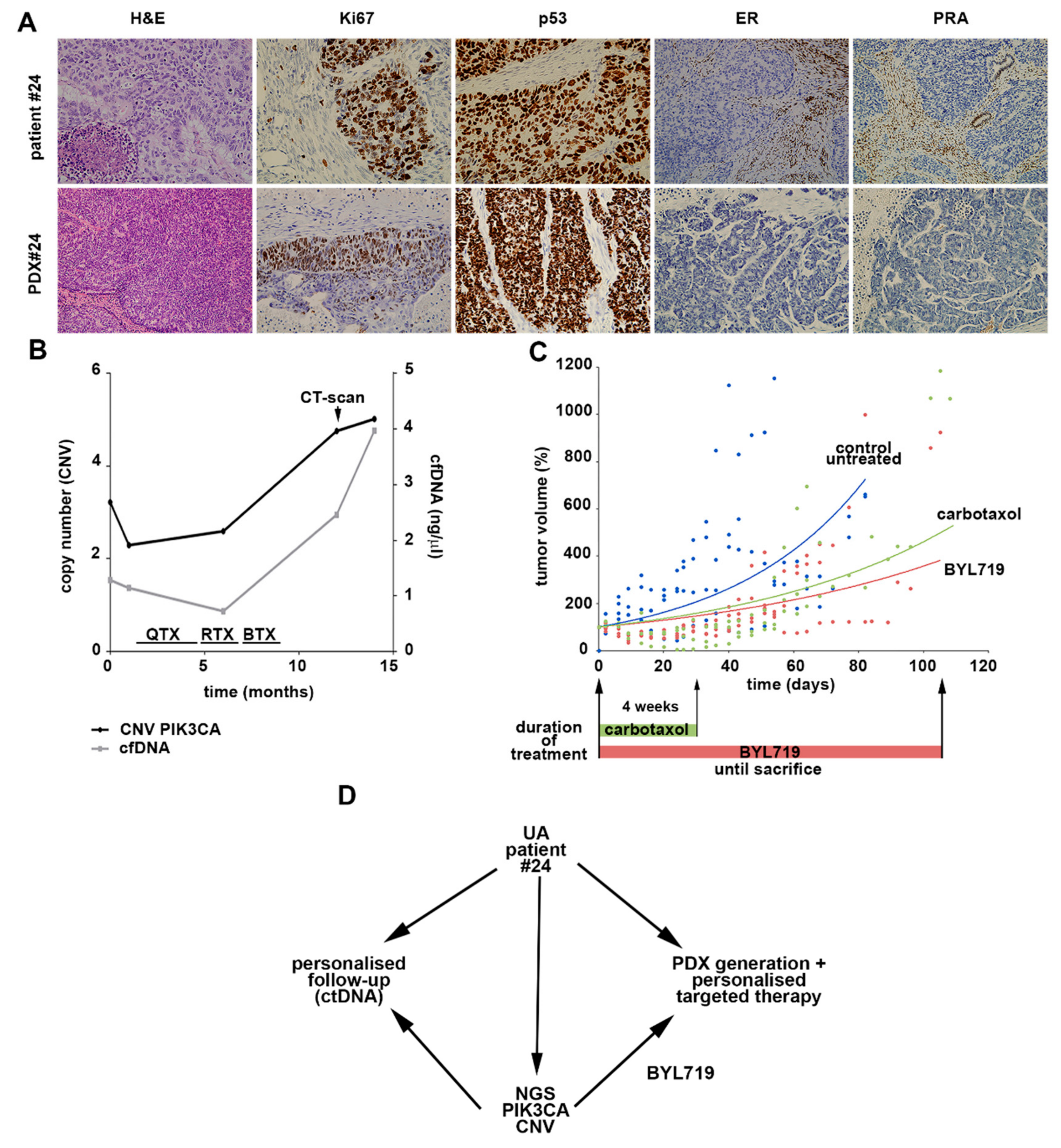
3.5. UAs for the Selection of Personalized Therapies and as a Feasible Alternative to Generate PDX Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Sasada, S.; Yunokawa, M.; Takehara, Y.; Ishikawa, M.; Ikeda, S.; Kato, T.; Tamura, K. Baseline risk of recurrence in stage I–II endometrial carcinoma. J. Gynecol. Oncol. 2018, 29, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Burmeister, C.; Hanna, R.K.; Munkarah, A.; Elshaikh, M.A. Predictors of survival after recurrence in women with early-stage endometrial carcinoma. Int. J. Gynecol. Cancer 2016, 26, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Stelloo, E.; Nout, R.A.; Osse, E.M.; Jürgenliemk-Schulz, I.J.; Jobsen, J.J.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Nijman, H.W.; Putter, H.; Bosse, T.; et al. Improved risk assessment by integrating molecular and clinicopathological factors in early-stage endometrial cancer-combined analysis of the PORTEC cohorts. Clin. Cancer Res. 2016, 22, 4215–4224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lianidou, E.; Pantel, K. Liquid biopsies. Genes. Chromosomes Cancer 2019, 58, 219–232. [Google Scholar] [CrossRef]
- Muinelo-Romay, L.; Casas-Arozamena, C.; Abal, M. Liquid biopsy in endometrial cancer: New opportunities for personalized oncology. Int. J. Mol. Sci. 2018, 19, 2311. [Google Scholar] [CrossRef] [Green Version]
- Alonso-alconada, L.; Muinelo-romay, L.; Madissoo, K.; Diaz-lopez, A.; Krakstad, C.; Trovik, J.; Wik, E.; Hapangama, D.; Coenegrachts, L.; Cano, A.; et al. Molecular profiling of circulating tumor cells links plasticity to the metastatic process in endometrial cancer. Mol. Cancer 2014, 13, 223. [Google Scholar] [CrossRef] [Green Version]
- Cicchillitti, L.; Corrado, G.; de Angeli, M.; Mancini, E.; Baiocco, E.; Patrizi, L.; Zampa, A.; Merola, R.; Martayan, A.; Conti, L.; et al. Circulating cell-free DNA content as blood based biomarker in endometrial cancer. Oncotarget 2017, 8, 115230–115243. [Google Scholar] [CrossRef] [Green Version]
- Bolivar, A.M.; Luthra, R.; Mehrotra, M.; Chen, W.; Barkoh, B.A.; Hu, P.; Zhang, W.; Broaddus, R.R. Targeted next-generation sequencing of endometrial cancer and matched circulating tumor DNA: Identification of plasma-based, tumor-associated mutations in early stage patients. Mod. Pathol. 2019, 32, 405–414. [Google Scholar] [CrossRef]
- Mota, A.; Colás, E.; García-Sanz, P.; Campoy, I.; Rojo-Sebastián, A.; Gatius, S.; García, Á.; Chiva, L.; Alonso, S.; Gil-Moreno, A.; et al. Genetic analysis of uterine aspirates improves the diagnostic value and captures the intra-tumor heterogeneity of endometrial cancers. Mod. Pathol. 2017, 30, 134–145. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Li, L.; Douville, C.; Cohen, J.D.; Yen, T.-T.; Kinde, I.; Sundfelt, K.; Kjær, S.K.; Hruban, R.H.; Shih, I.-M.; et al. Evaluation of liquid from the Papanicolaou test and other liquid biopsies for the detection of endometrial and ovarian cancers. Physiol. Behav. 2019, 176, 139–148. [Google Scholar]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO consensus conference on endometrial cancer: Diagnosis, treatment and follow-up. Int. J. Gynecol. Cancer 2016, 26, 2–30. [Google Scholar] [CrossRef] [Green Version]
- Gibson, W.J.; Hoivik, E.A.; Halle, M.K.; Taylor-Weiner, A.; Cherniack, A.D.; Berg, A.; Holst, F.; Zack, T.I.; Werner, H.M.J.; Staby, K.M.; et al. The genomic landscape and evolution of endometrial carcinoma progression and abdominopelvic metastasis. Physiol. Behav. 2017, 176, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Getz, G.; Gabriel, S.B.; Cibulskis, K.; Lander, E.; Sivachenko, A.; Sougnez, C.; Lawrence, M.; Kandoth, C.; Dooling, D.; Fulton, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar]
- May, K.; Bryant, A.; Ho, D.; Kehoe, S.; Morrison, J. Lymphadenectomy for the management of endometrial cancer (Review). Cochrane Database Syst. Rev. 2010, 30. [Google Scholar] [CrossRef]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating liquid biopsies into the management of cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar] [CrossRef]
- Mcconechy, M.K.; Ding, J.; Cheang, M.C.U.; Wiegand, K.; Tone, A.; Yang, W.; Prentice, L.; Tse, K.; Zeng, T.; Schmidt, A.P.; et al. Use of mutation profiles to refine the classification of endometrial carcinomas. J. Pathol. 2012, 228, 20–30. [Google Scholar] [CrossRef] [Green Version]
- Hong, B.; Le Gallo, M.; Bell, D.W. The mutational landscape of endometrial cancer. Curr. Opin. Genet. Dev. 2015, 30, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Tsuda, H.; Nishimura, S.; Nomura, H.; Kataoka, F.; Chiyoda, T.; Tanaka, K.; Iguchi, Y.; Susumu, N.; Aoki, D. Role of circulating free alu DNA in endometrial cancer. Int. J. Gynecol. Cancer 2012, 22, 82–86. [Google Scholar] [CrossRef]
- Dobrzycka, B.; Terlikowski, S.J.; Mazurek, A.; Kowalczuk, O.; Niklinska, W.; Chyczewski, L.; Kulikowski, M. Circulating free DNA, p53 antibody and mutations of KRAS gene in endometrial cancer. Int. J. Cancer 2010, 127, 612–621. [Google Scholar] [CrossRef]
- Pereira, E.; Camacho-Vanegas, O.; Anand, S.; Sebra, R.; Camacho, S.C.; Garnar-Wortzel, L.; Nair, N.; Moshier, E.; Wooten, M.; Uzilov, A.; et al. Personalized circulating tumor DNA biomarkers dynamically predict treatment response and survival in gynecologic cancers. PLoS ONE 2015, 10, e0145754. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Dowdy, S.C.; Cliby, W.A.; Gostout, B.S.; Kumar, S.; Ghezzi, F.; Multinu, F.; Mariani, A. Incisional recurrences after endometrial cancer surgery. Anticancer Res. 2015, 35, 6097–6104. [Google Scholar] [PubMed]
- Chalfin, H.J.; Glavaris, S.A.; Gorin, M.A.; Kates, M.R.; Fong, M.H.; Dong, L.; Matoso, A.; Bivalacqua, T.J.; Johnson, M.H.; Pienta, K.J.; et al. Circulating tumor cell and circulating tumor DNA assays reveal complementary information for patients with metastatic urothelial cancer. Eur. Urol. Oncol. 2019, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Förnvik, D.; Aaltonen, K.E.; Chen, Y.; George, A.M.; Brueffer, C.; Rigo, R.; Loman, N.; Saal, L.H.; Rydén, L. Detection of circulating tumor cells and circulating tumor DNA before and after mammographic breast compression in a cohort of breast cancer patients scheduled for neoadjuvant treatment. Breast Cancer Res. Treat. 2019, 177, 447–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Low/Intermediate Risk n = 24 | High Risk n = 36 | Total n = 60 |
|---|---|---|---|
| AGE (38–88 y/o*) | |||
| <66 y/o | 10 (41.67%) | 14 (38.89%) | 24 (40.00%) |
| ≥66 y/o | 14 (58.33%) | 22 (61.11%) | 36 (60.00%) |
| Time of diagnosis | |||
| Recently diagnosed | 22 (91.67%) | 31 (86.11%) | 53 (88.33%) |
| Recurrence | 2 (8.33%) | 5 (13.88%) | 7 (11.66%) |
| Histology | |||
| Endometrioid | 24 (100.00%) | 19 (52.78%) | 43 (71.67%) |
| Non-endometrioid | 0 (0.00%) | 17 (47.22%) | 17 (28.33%) |
| Histologic grade | |||
| Grade 1 | 15 (62.50%) | 5 (13.89%) | 20 (33.33%) |
| Grade 2 | 8 (33.33%) | 7 (19.44%) | 15 (41.66%) |
| Grade 3 | 1 (4.17%) | 24 (66.66%) | 25 (69.44%) |
| Figo stage | |||
| I | 23 (95.83% | 13 (36.11%) | 36 (60.00%) |
| II | 1 (4.17%) | 9 (25.00%) | 10 (16.67%) |
| III | 0 (0.00%) | 11 (30.56%) | 11 (18.33%) |
| IV | 0 (0.00%) | 3 (8.33%) | 3 (5.00%) |
| Myometrial invasion | |||
| <50% | 15 (62.50%) | 10 (27.78%) | 25 (41.67%) |
| ≥50% | 9 (37.50%) | 25 (69.44%) | 34 (56.67%) |
| Unknown | 0 (0.00%) | 1 (2.78%) | 1 (1.67%) |
| LVSI** | |||
| No | 13 (54.17%) | 18 (50.00%) | 31 (51.67%) |
| Yes | 3 (12.50%) | 11 (30.56%) | 14 (23.33%) |
| Unknown | 8 (33.33%) | 7 (19.44%) | 15 (25.00%) |
| Feature | cfDNA Mean ± SEM** (ng/µL) | p | ctDNA-Positive Patients | p | CTCs/7.5 mL-Positive Patients | p |
|---|---|---|---|---|---|---|
| Histology | ||||||
| Endometrioid | 1.44 ± 0.17 | 14/35 (40.00%) | 8/23 (34.78%) | |||
| Non-endometrioid | 1.65 ± 0.28 | 0.28 | 7/16 (43.75%) | 1.0 | 6/13 (46.15%) | 0.72 |
| Histologic grade | ||||||
| Grade 1/2 | 1.17 ± 0.15 | 8/27 (29.63%) | 5/27 (18.52%) | |||
| Grade 3 | 2.02 ± 0.26 | 0.003 | 13/24 (54.17%) | 0.049 | 9/19 (65.89%) | 0.18 |
| Figo stage | ||||||
| I/II | 1.42 ± 0.17 | 12/35 (34.29%) | 6/22 (27.27%) | |||
| III/IV | 1.79 ± 0.38 | 0.38 | 7/12 (58.33%) | 0.18 | 5/9 (55.55%) | 0.21 |
| Myometrial invasion | ||||||
| <50% | 1.30 ± 0.21 | 4/21 (19.05%) | 4/12 (33.33%) | |||
| ≥50% | 1.67 ± 0.21 | 0.08 | 17/29 (58.62%) | 0.008 | 10/23 (43.48%) | 0.72 |
| LVSI | ||||||
| No | 1.38 ± 0.18 | 10/27 (37.04%) | 5/15 (33.33%) | |||
| Yes | 2.15 ± 0.41 | 0.07 | 7/13 (53.85%) | 0.49 | 5/10 (50.00%) | 0.44 |
| Risk of recurrence | ||||||
| Low/intermediate | 1.24 ± 0.23 | 3/19 (15.79%) | 2/11 (18.18%) | |||
| High | 1.65 ± 0.19 | 0.017 | 18/32 (56.25%) | 0.007 | 12/25 (48.00%) | 0.14 |
| Time of diagnosis | ||||||
| Recently diagnosed | 1.50 ± 0.16 | 17/45 (37.78%) | 10/30 (33.33%) | |||
| Recurrence | 1.44 ± 0.23 | 0.45 | 4/6 (66.67%) | 0.21 | 4/6 (66.67%) | 0.11 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casas-Arozamena, C.; Díaz, E.; Moiola, C.P.; Alonso-Alconada, L.; Ferreiros, A.; Abalo, A.; López Gil, C.; Oltra, S.S.; de Santiago, J.; Cabrera, S.; et al. Genomic Profiling of Uterine Aspirates and cfDNA as an Integrative Liquid Biopsy Strategy in Endometrial Cancer. J. Clin. Med. 2020, 9, 585. https://doi.org/10.3390/jcm9020585
Casas-Arozamena C, Díaz E, Moiola CP, Alonso-Alconada L, Ferreiros A, Abalo A, López Gil C, Oltra SS, de Santiago J, Cabrera S, et al. Genomic Profiling of Uterine Aspirates and cfDNA as an Integrative Liquid Biopsy Strategy in Endometrial Cancer. Journal of Clinical Medicine. 2020; 9(2):585. https://doi.org/10.3390/jcm9020585
Chicago/Turabian StyleCasas-Arozamena, Carlos, Eva Díaz, Cristian Pablo Moiola, Lorena Alonso-Alconada, Alba Ferreiros, Alicia Abalo, Carlos López Gil, Sara S. Oltra, Javier de Santiago, Silvia Cabrera, and et al. 2020. "Genomic Profiling of Uterine Aspirates and cfDNA as an Integrative Liquid Biopsy Strategy in Endometrial Cancer" Journal of Clinical Medicine 9, no. 2: 585. https://doi.org/10.3390/jcm9020585
APA StyleCasas-Arozamena, C., Díaz, E., Moiola, C. P., Alonso-Alconada, L., Ferreiros, A., Abalo, A., López Gil, C., Oltra, S. S., de Santiago, J., Cabrera, S., Sampayo, V., Bouso, M., Arias, E., Cueva, J., Colas, E., Vilar, A., Gil-Moreno, A., Abal, M., Moreno-Bueno, G., & Muinelo-Romay, L. (2020). Genomic Profiling of Uterine Aspirates and cfDNA as an Integrative Liquid Biopsy Strategy in Endometrial Cancer. Journal of Clinical Medicine, 9(2), 585. https://doi.org/10.3390/jcm9020585