Analysis of Cervical Spine Alignment and its Relationship with Other Spinopelvic Parameters after Laminoplasty in Patients with Degenerative Cervical Myelopathy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
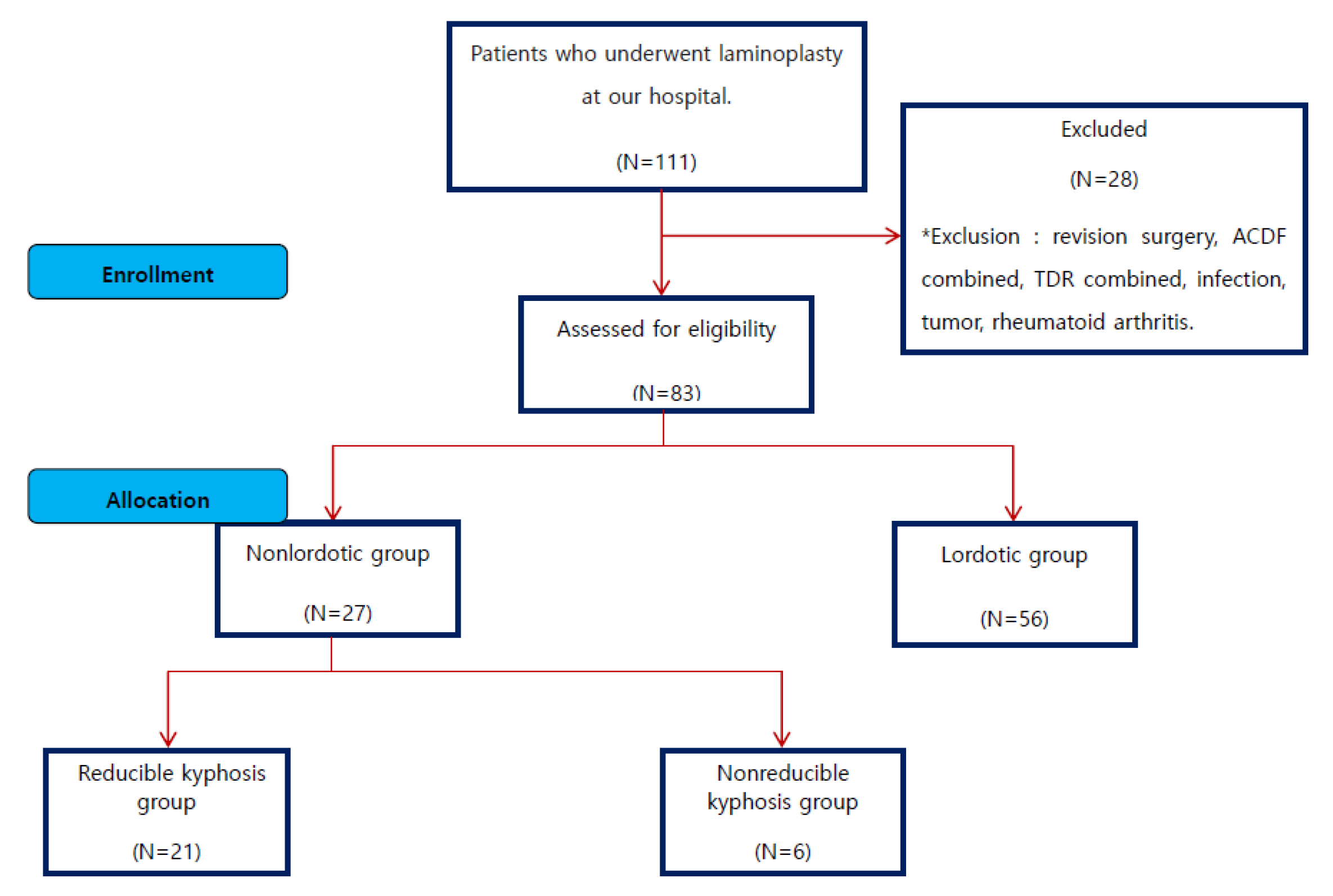
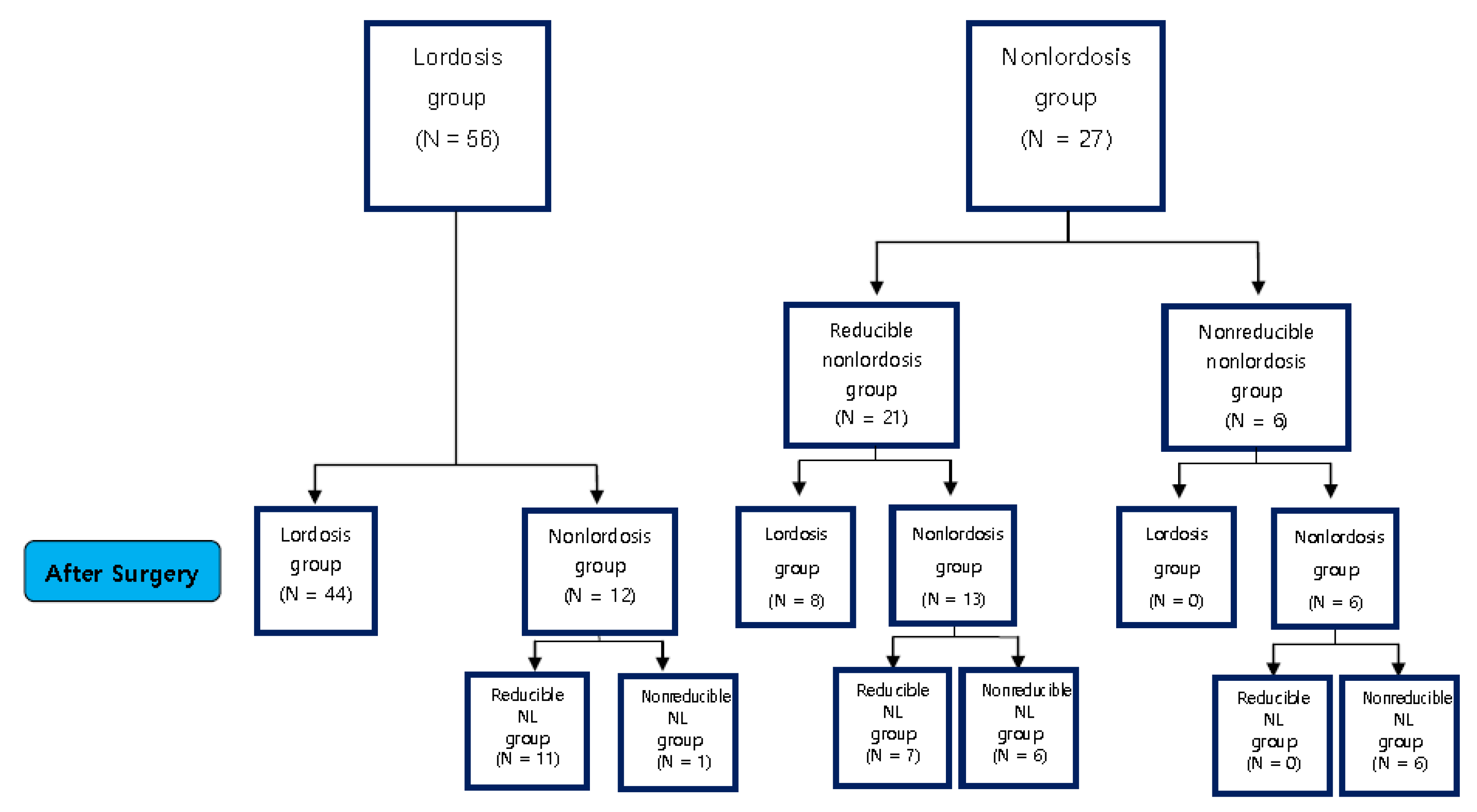
2.1. Research Subjects
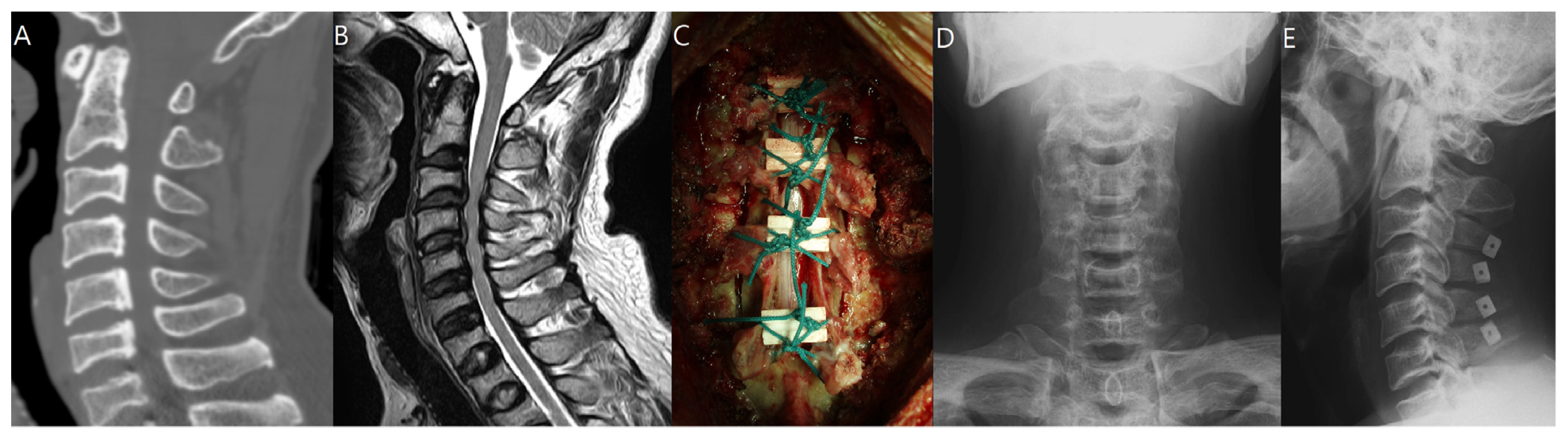
2.2. Surgical Technique
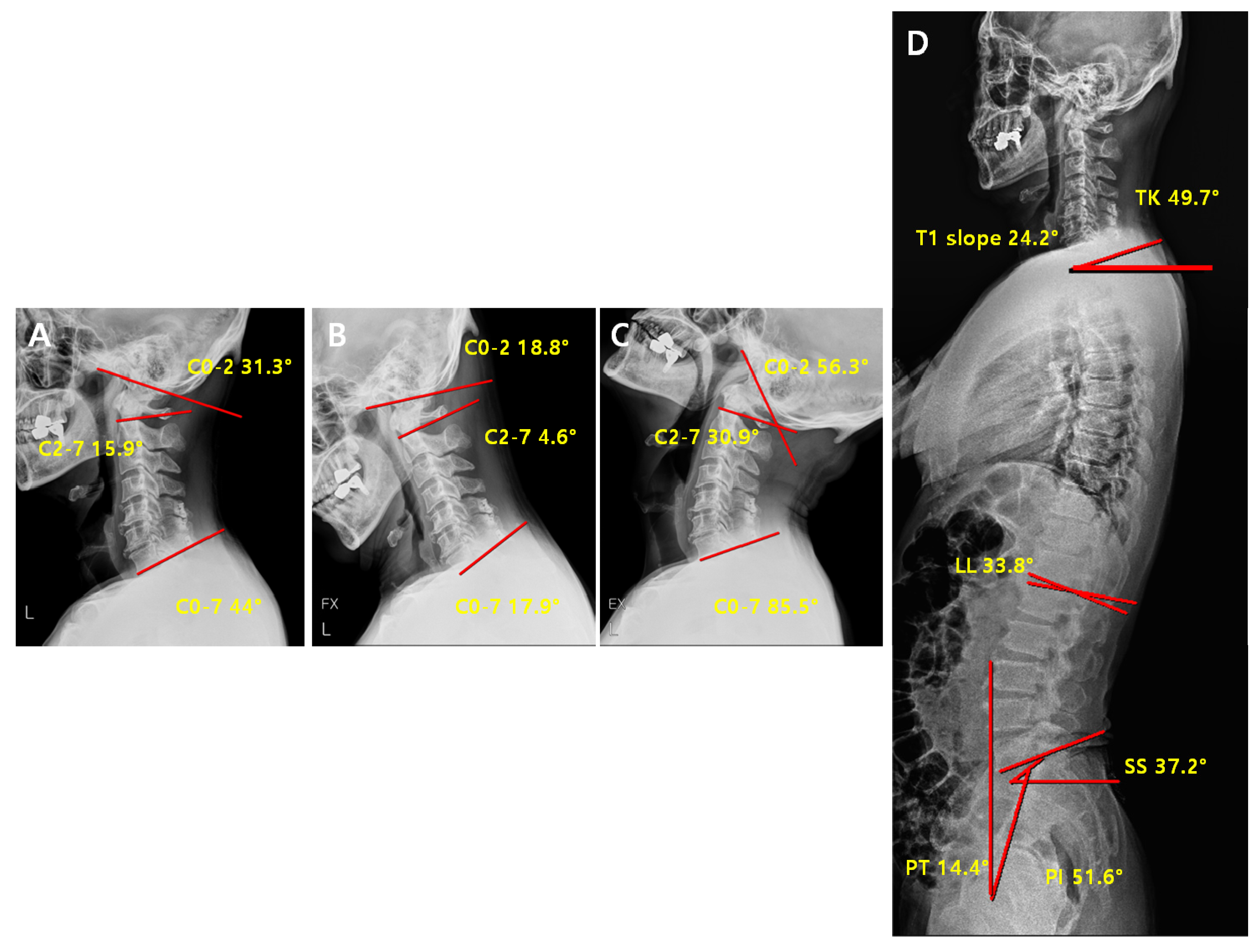
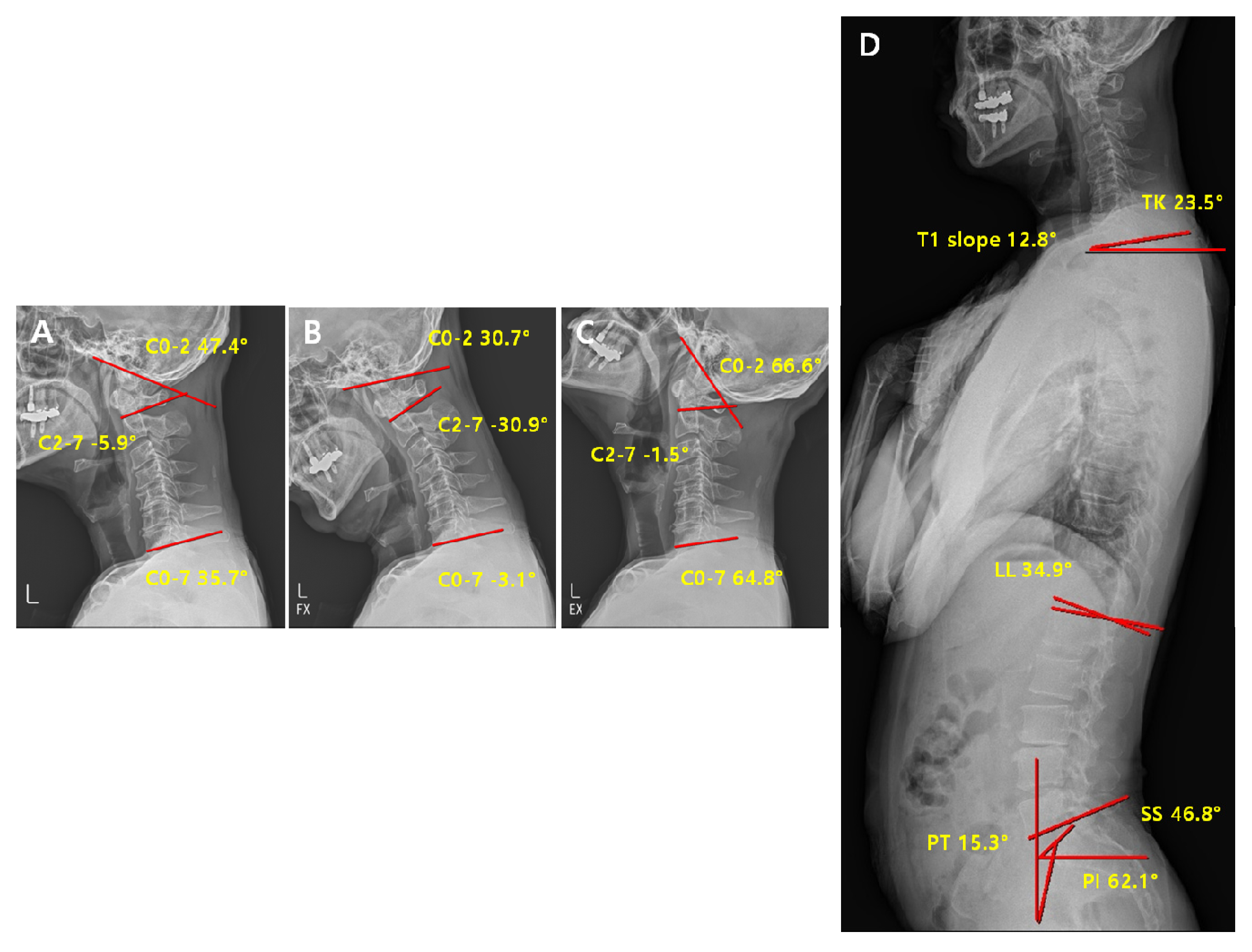
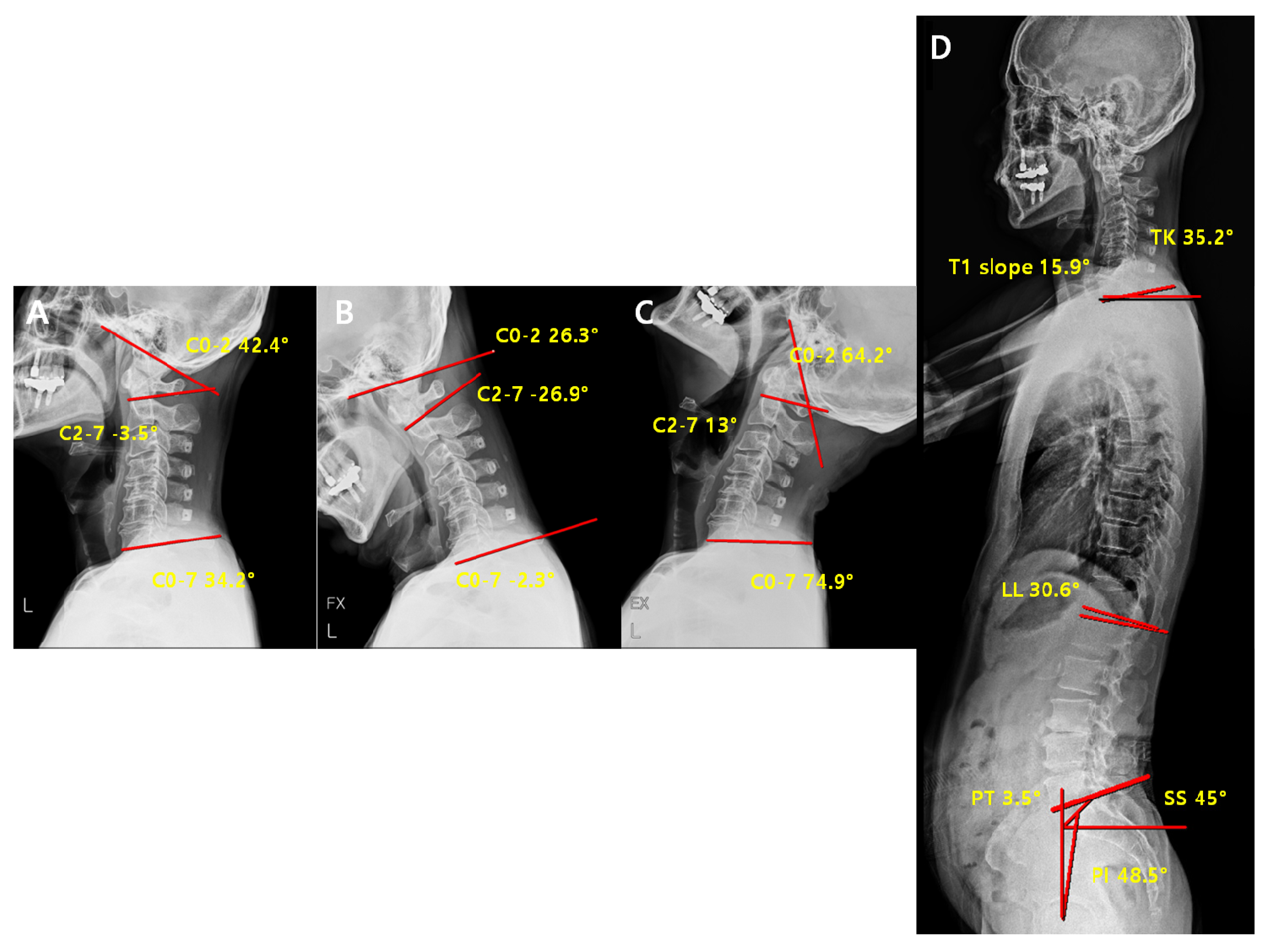
2.3. Radiographic Measurement
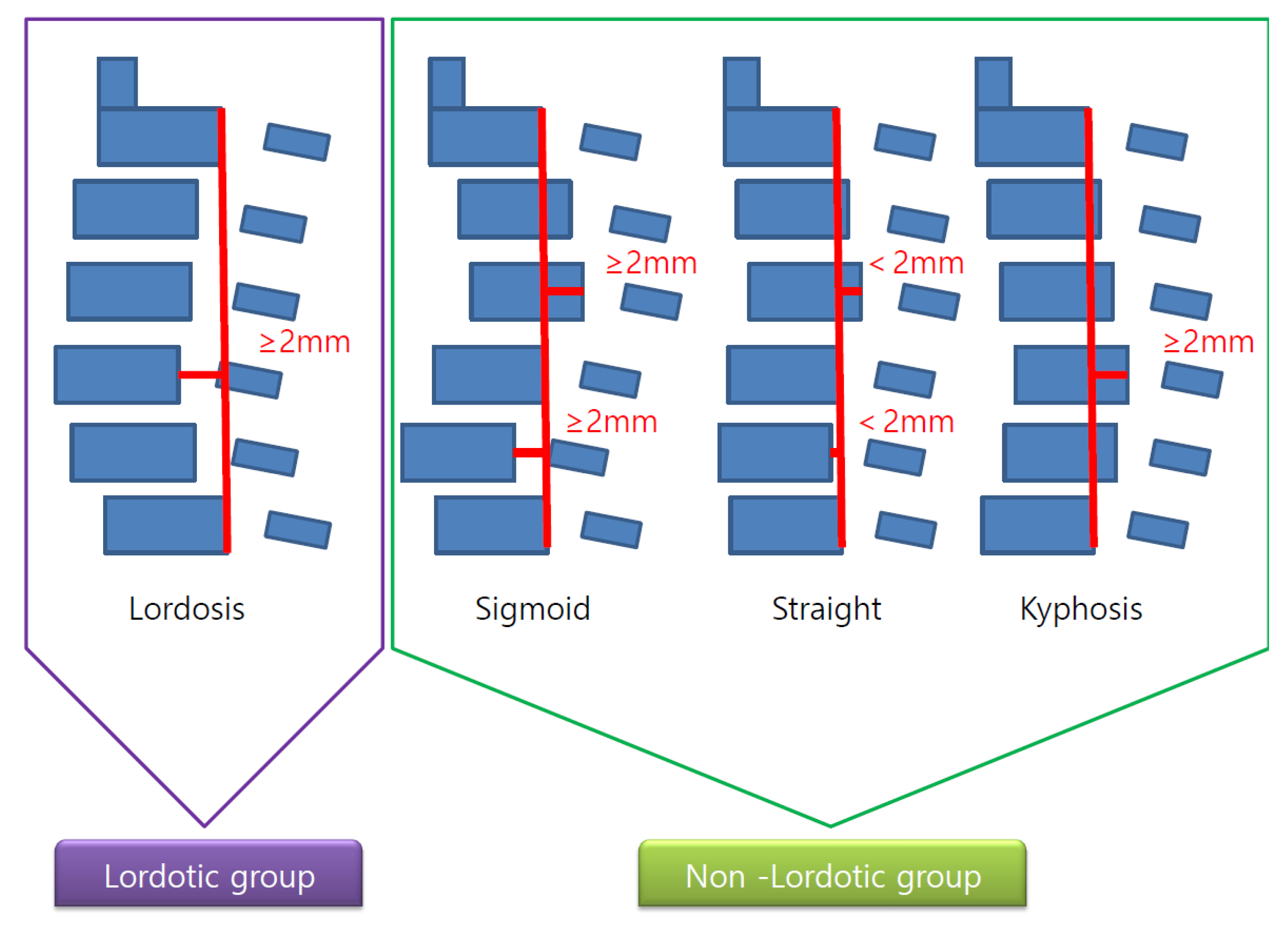
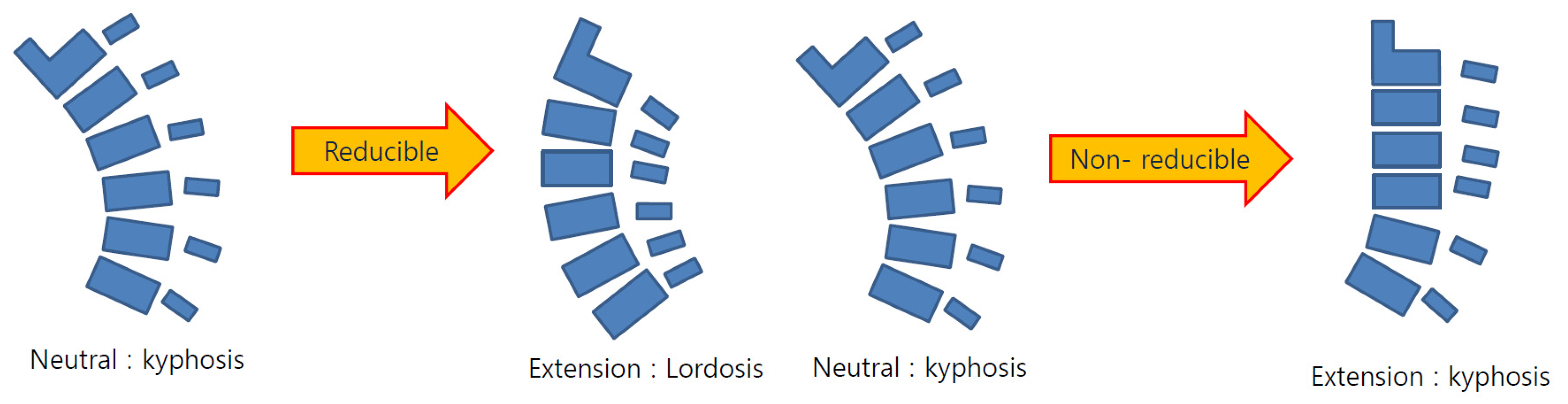
2.4. Radiological Analysis
2.5. Statistical Analysis
3. Results
3.1. Post Operative Change of Curvature
3.1.1. Comparison of Pre-Operative Radiological Parameters between the Lordosis and Non-Lordosis Groups
3.1.2. Comparison of Post-Operative Radiological Parameters between the Lordosis and Non-Lordosis Groups
3.1.3. Comparison of Pre-Operative vs. Post-Operative Radiological Parameters in the Lordosis Group
3.1.4. Comparison of Pre-Operative vs. Post-Operative Radiological Parameters in the Non- Lordosis Group
3.1.5. Comparison of Pre-Operative vs. Post-Operative Radiological Parameters in the Reducible Non-Lordosis Group
3.1.6. Comparison of Pre-Operative vs. Post-Operative Radiological Parameters in the Non-Reducible Non-Lordosis Group
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kimura, I.; Shingu, H.; Nasu, Y. Long-term follow-up of cervical spondylotic myelopathy treated by canal-expansive laminoplasty. J. Bone Joint Surg. Br. Vol. 1995, 77, 956–961. [Google Scholar] [CrossRef]
- Suk, K.S.; Kim, K.T.; Lee, J.H.; Lee, S.H.; Lim, Y.J.; Kim, J.S. Sagittal alignment of the cervical spine after the laminoplasty. Spine 2007, 32, E656–E660. [Google Scholar] [CrossRef] [PubMed]
- Machino, M.; Yukawa, Y.; Hida, T.; Ito, K.; Nakashima, H.; Kanbara, S.; Morita, D.; Kato, F. Cervical alignment and range of motion after laminoplasty: Radiographical data from more than 500 cases with cervical spondylotic myelopathy and a review of the literature. Spine 2012, 37, E1243–E1250. [Google Scholar] [CrossRef] [PubMed]
- Ratliff, J.K.; Cooper, P.R. Cervical laminoplasty: A critical review. J. Neurosurg. 2003, 98, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Okuda, S.Y.; Miyauchi, A.; Sakaura, H.; Mukai, Y.; Yonenobu, K.; Yoshikawa, H. Surgical strategy for cervical myelopathy due to ossification of the posterior longitudinal ligament: Part 2: Advantages of anterior decompression and fusion over laminoplasty. Spine 2007, 32, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Seichi, A.; Takeshita, K.; Ohishi, I.; Kawaguchi, H.; Akune, T.; Anamizu, Y.; Kitagawa, T.; Nakamura, A.K. Long-term results of double-door laminoplasty for cervical stenotic myelopathy. Spine 2001, 26, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Sodeyama, T.; Goto, S.; Mochizuki, M.; Takahashi, J.; Moriya, H. Effect of decompression enlargement laminoplasty for posterior shifting of the spinal cord. Spine 1999, 24, 1527–1531. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Hai, D.M.; Sundaram, S.; Kim, Y.C.; Park, M.S.; Paik, S.H.; Kwak, Y.-H.; Kim, T.-H. Is cervical lordosis relevant in laminoplasty? Spine J. 2013, 13, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Kim, T.-H.; Bok, D.H.; Jang, C.; Yang, M.H.; Lee, S.; Yoo, J.-H.; Kwak, Y.H.; Oh, J.K. Analysis of cervical spine alignment in currently asymptomatic individuals: Prevalence of kyphotic posture and its relationship with other spinopelvic parameters. Spine J. 2018, 18, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Fujiyoshi, T.; Yamazaki, M.; Kawabe, J.; Endo, T.; Furuya, T.; Koda, M.; Okawa, A.; Takahashi, K.; Konishi, H. A new concept for making decisions regarding the surgical approach for cervical ossification of the posterior longitudinal ligament: The K-line. Spine 2008, 33, E990–E993. [Google Scholar] [CrossRef] [PubMed]
- Chiba, K.; Toyama, Y.; Watanabe, M.; Maruiwa, H.; Matsumoto, M.; Hirabayashi, K. Impact of longitudinal distance of the cervical spine on the results of expansive open-door laminoplasty. Spine 2000, 25, 2893–2898. [Google Scholar] [CrossRef] [PubMed]
- Steinmetz, M.P.; Kager, C.D.; Benzel, E.C. Ventral correction of postsurgical cervical kyphosis. J. Neurosurg. 2003, 98, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.-H.; Ha, J.-K.; Chung, J.-H.; Hwang, C.J.; Lee, C.S.; Cho, J.H. A retrospective study to reveal the effect of surgical correction of cervical kyphosis on thoraco-lumbo-pelvic sagittal alignment. Eur. Spine J. 2016, 25, 2286–2293. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H.; Son, E.-S.; Seo, E.-M.; Suk, K.-S.; Kim, K.-T. Factors determining cervical spine sagittal balance in asymptomatic adults: Correlation with spinopelvic balance and thoracic inlet alignment. Spine J. 2015, 15, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Sugrue, P.A.; McClendon, J.; Smith, T.R.; Halpin, R.J.; Nasr, F.F.; O’shaughnessy, B.A.; Koski, T.R. Redefining global spinal balance: Normative values of cranial center of mass from a prospective cohort of asymptomatic individuals. Spine 2013, 38, 484–489. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Definition |
|---|---|
| C2-7 Cobb angle | The intersection angle between the line perpendicular to the line parallel to the C2 lower endplate and the line perpendicular to the line parallel to the C7 lower endplate |
| C0-2 Cobb angle | The occipito-cervical angle, which is the intersection angle between the McGregor line and the line parallel to the C2 lower endplate and is used to evaluate the curvature of the upper cervical spine |
| C0-7 Cobb angle | The intersection angle between the McGregor line and the line parallel to the C7 lower endplate |
| C0-2/C0-7 | The value of C0-2 Cobb angle divided by C0-7 Cobb angle |
| C2-7/C0-7 | The value of C2-7 Cobb angle divided by C0-7 Cobb angle |
| T1 slope | The intersection angle between the tangent line and the upper plate of the T1 vertebral body |
| SS (Sacral Slope) | The angle formed by a line drawn along the endplate of the sacrum and a horizontal reference line |
| PT (Pelvic Tilt) | The angle formed by a line drawn from the midpoint of the sacral endplate to the center of the bicoxofemoral axis and a vertical and a vertical plumb line |
| PI (Pelvic incidence) | The angle formed by two vectors: (1) The line joining the bicoxo-femoral axis to the center of the sacral end plate and (2) A line perpendicular to the sacral endplate |
| Patient Who Underwent Laminoplasty (n = 83). | |||
|---|---|---|---|
| Lordosis | Non-Lordosis | p-Value * | |
| No. of participants | 56 (67.4%) | 27 (32.6%) | |
| Sex ratio (M:F) | 40:16 | 19:8 | 0.921 |
| Age [95% CI] | 61.9 [60.4~63.4] | 64.8 [62.6~67.0] | 0.292 |
| Parameter | Lordosis Mean (Degrees) | Non-Lordosis Mean (Degrees) | Between-Group Difference Mean (Degrees) (95% CI) | p-Value |
|---|---|---|---|---|
| C2-7angle | 13.2(10.9~15.9) | 1.1(−2.6~4.9) | 12.1(7.7~16.5) | 0.01 * |
| C0-2angle | 24.2(21.2~26.8) | 31.9(27.9~35.9) | −7.7 (−12.6~-2.8) | 0.01 * |
| C0-7angle | 36.8(33.3~40.4) | 33.4(29.6~37.3) | 3.4 (−2.4~9.1) | 0.25 |
| C0-2ROM | 17.8(15.3~20.1) | 23.1(16.2~30.1) | −5.3(−11.1~0.5) | 0.07 |
| C2-7ROM | 34.3(30.7~37.6) | 29.7(24.9~34.5) | 4.6(−1.3~10.5) | 0.12 |
| C0-7ROM | 52.4(47.7~56.4) | 50.1(44.9~55.3) | 2.3(−4.9~9.5) | 0.53 |
| C0-2/C0-7 | 0.3(0.3~0.4) | 0.5(0.3~0.7) | −0.1(−0.3~0) | 0.05 * |
| C2-7/C0-7 | 0.7(0.6~0.7) | 0.6(0.5~0.7) | 0.1(0~0.2) | 0.18 |
| T1slope | 29.7(27.2~32.4) | 26.9(23.5~30.3) | 2.8(−1.6~7.2) | 0.21 |
| Lumbar lordosis | 37.6(25.9~49.3) | 26.4(12.3~39.9) | 11.2(−0.8~23.3) | 0.07 |
| sacral slope | 34.0(29.6~38.5) | 30.9(21.7~40.1) | 3.1(−5.9~12.1) | 0.49 |
| pelvic tilt | 15.5(12.1~18.8) | 16.5(9.6~23.4) | −1.0(−7.8~5.8) | 0.76 |
| pelvic incidence | 47.4(40.8~53.9) | 41.6 (23.8~50.5) | 5.7 (−6.6~18.1) | 0.35 |
| Parameter | Lordosis Mean (Degrees) | Non-Lordosis Mean (Degrees) | Between-Group Difference Mean (Degrees) (95% CI) | p-Value |
|---|---|---|---|---|
| C2-7angle | 11.3(8.4~14.4) | −0.1(-4.9~4.8) | 11.4(5.9~16.9) | 0.01 * |
| C0-2angle | 27.2(24.2~30.5) | 33.7(29.8~37.7) | −6.5(−11.8~-1.3) | 0.02 * |
| C0-7angle | 39.7(36.1~43.7) | 32.9(29.5~36.3) | 6.9(1.0~12.8) | 0.02 * |
| C0-2ROM | 21.7(18.6~24.7) | 24.8(20.9~28.7) | −3.1(−8.2~2.0) | 0.23 |
| C2-7ROM | 20.9(18.1~23.9) | 19.8(14.6~24.9) | 1.2(−4.2~6.6) | 0.66 |
| C0-7ROM | 42.8(39.2~46.6) | 40.9(35.2~46.7)) | 1.9(−4.7~8.5) | 0.57 |
| C0-2/C0-7 | 0.5(0.4~0.6) | 0.6(0.5~0.7) | −0.1(−0.2~0) | 0.03 * |
| C2-7/C0-7 | 0.5(0.4~0.6) | 0.5(0.4~0.6) | 0.0(−0.1~0.1) | 0.85 |
| T1slope | 29.3(26.9~32.3) | 23.3(20.3~26.3) | 6.0(1.7~10.3) | 0.01 * |
| Lumbar lordosis | 32.7(21.2~44.2) | 36.2(27.8~44.6) | −3.5(−20.2~13.2) | 0.64 |
| sacral slope | 36.0(32.6~43.8) | 39.1(31.0~47.2) | −3.0(−7.7~1.6) | 0.17 |
| pelvic tilt | 19.0(12.4~28.0) | 20.1(-2.7~42.9) | −1.1(−16.0~13.8) | 0.87 |
| pelvic incidence | 55.0(48.3~68.3) | 55.6(35.4~75.7) | −0.5(−13.4~12.3) | 0.93 |
| Parameter | Lordosis | |||
|---|---|---|---|---|
| Pre-op | Post-op | Between-Group Difference Mean (Degrees) (95% CI) | p-Value | |
| Mean (Degrees) | Mean (Degrees) | |||
| C2-7angle | 13.2(10.9~15.9) | 11.3(8.4~14.4) | 2.0(0.6~4.6) | 0.13 |
| C0-2angle | 24.2(21.2~26.8) | 27.2(24.2~30.5) | −3.4(−5.4~−1.3) | <0.01 * |
| C0-7angle | 36.8(33.3~40.4) | 39.7(36.1~43.7) | −3.1(−5.9~−0.3) | 0.03 * |
| C0-2ROM | 17.8(15.3~20.1) | 21.7(18.6~24.7) | −4.0(−7.2~−0.8) | 0.02 * |
| C2-7ROM | 34.3(30.7~37.6) | 20.9(18.1~23.9) | 13.1(9.8~16.4) | <0.01 * |
| C0-7ROM | 52.4(47.7~56.4) | 42.8(39.2~46.6) | 9.2(4.7~13.7) | <0.01 * |
| C0-2/C0-7 | 0.3(0.3~0.4) | 0.5(0.4~0.6) | −0.2(−0.2~−0.1) | <0.01 * |
| C2-7/C0-7 | 0.7(0.6~0.7) | 0.5(0.4~0.6) | 0.2(0.1~0.2) | <0.01 * |
| T1slope | 29.7(27.2~32.4) | 29.3(26.9~32.3) | 0.2(-2.1~2.4) | 0.89 |
| Lumbar lordosis | 37.6(25.9~49.3) | 32.7(21.2~44.2) | −1.1(−6.4~4.3) | 0.57 |
| sacral slope | 34.0(29.6~38.5) | 36.0(32.6~43.8) | −0.7(−10.8~9.5) | 0.85 |
| pelvic tilt | 15.5(12.1~18.8) | 19.0(12.4~28.0) | 1.2(−10.1~12.4) | 0.77 |
| pelvic incidence | 47.4(40.8~53.9) | 55.0(48.3~68.3) | 0.8(−14.0~15.6) | 0.88 |
| Parameter | Non-Lordosis | |||
|---|---|---|---|---|
| Pre-op | Post-op | Between-Group Difference MEAN (Degrees) (95% CI) | p-Value | |
| Mean (Degrees) | Mean (Degrees) | |||
| C2-7angle | 1.1(-2.6~4.9) | −0.1(−4.9~4.8) | 1.2(2.6~5.0) | 0.53 |
| C0-2angle | 31.9(27.9~35.9) | 33.7(29.8~37.7) | −1.9(−5.1~1.4) | 0.26 |
| C0-7angle | 33.4(29.6~37.3) | 32.9(29.5~36.3) | 0.6(−3.6~4.7) | 0.78 |
| C0-2ROM | 23.1(16.2~30.1) | 24.8(20.9~28.7) | −1.7(−9.5~6.2) | 0.67 |
| C2-7ROM | 29.7(24.9~34.5) | 19.8(14.6~24.9) | 9.9(4.5~15.4) | <0.01 * |
| C0-7ROM | 50.1(44.9~55.3) | 40.9(35.2~46.7) | 9.2(2.6~15.8) | <0.01 * |
| C0-2/C0-7 | 0.5(0.3~0.7) | 0.6(0.5~0.7) | −0.1(−0.3~0.1) | 0.14 |
| C2-7/C0-7 | 0.6(0.5~0.7) | 0.5(0.4~0.6) | 0.1(−0.02~0.2) | 0.1 |
| T1slope | 26.9(23.5~30.3) | 23.3(20.3~26.3) | 3.6(0.1~7.0) | 0.04 * |
| Lumbar lordosis | 26.4(12.3~39.9) | 36.2(27.8~44.6) | 2.4(−4.0~8.9) | 0.35 |
| sacral slope | 30.9(21.7~40.1) | 39.1(31.0~47.2) | −0.7(−4.3~3.0) | 0.64 |
| pelvic tilt | 16.5(9.6~23.4) | 20.1(−2.7~42.9) | −0.9(−13.6~11.8) | 0.85 |
| pelvic incidence | 41.6 (23.8~50.5) | 55.6(35.4~75.7) | −4.1(−18.9~10.7) | 0.49 |
| Parameter | Reducible Non-Lordosis | |||
|---|---|---|---|---|
| Pre-op | Post-op | Between-Group Difference Mean (Degrees) (95% CI) | p-Value | |
| Mean (Degrees) | Mean (Degrees) | |||
| C2-7angle | 2.0(−2.3~6.2) | 2.5(−2.9~7.9) | −0.5(−4.8~3.8) | 0.81 |
| C0-2angle | 29.9(25.5~34.4) | 31.5(27.6~35.5) | −1.6(−5.6~2.4) | 0.42 |
| C0-7angle | 32.2(27.7~36.6) | 33.3(29.2~37.4) | −1.1(−6.1~3.8) | 0.64 |
| C0-2ROM | 23.7(−14.8~32.5) | 23.6(19.4~27.9) | 0.03(−10.0~10.0) | 0.99 |
| C2-7ROM | 30.3(24.2~36.4) | 18.7(12.3~25.2) | 11.6(5.2~18.0) | <0.01 * |
| C0-7ROM | 51.5(45.1~57.9) | 37.9(32.0~43.8) | 13.6(6.7~20.5) | <0.01 * |
| C0-2/C0-7 | 0.5(0.2~0.7) | 0.6(0.5~0.8) | −0.2(−0.4~0.1) | 0.20 |
| C2-7/C0-7 | 0.6(0.5~0.7) | 0.5(0.3~0.7) | −0.2(−0.4~0.1) | 0.27 |
| T1slope | 26.3(22.1~30.5) | 25.6(22.6~28.6) | 0.7(2.5~3.9) | 0.67 |
| Lumbar lordosis | 37.0(35.0~39.0) | 32.4(25.4~39.4) | 4.7(76.0~85.3) | 0.60 |
| sacral slope | 40.9(36.5~47.3) | 40.8(38.7~42.9) | 0.1(−39.3~39.5) | 0.98 |
| pelvic tilt | 13.3(8.1~18.5) | 15.3(10.1~20.5) | −2.0(−2.6~-1.3) | 0.02 * |
| pelvic incidence | 54.8(44.5~65.1) | 50.9(49.9~51.9) | 3.9(−79.4~87.1) | 0.66 |
| Parameter | Nonreducible Non-Lordosis | |||
|---|---|---|---|---|
| Pre-op | Post-op | Between-Group Difference Mean (Degrees) (95% CI) | p-Value | |
| Mean (Degrees) | Mean (Degrees) | |||
| C2-7angle | −1.8(−12.5~8.8) | −9.0(−19.5~−1.6) | 7.1(−1.8~16.0) | 0.10 |
| C0-2angle | 38.7(29.7~47.8) | 41.5(30.0~53.0) | −2.8(−10.1~4.6) | 0.37 |
| C0-7angle | 37.9(28.9~47.0) | 31.5(24.3~38.6) | 6.5(1.5~14.4) | 0.09 |
| C0-2ROM | 21.4(12.2~30.5) | 28.9(16.6~41.3) | −7.6(−16.4~1.3) | 0.08 |
| C2-7ROM | 27.5(20.6~34.5) | 23.3(15.2~31.4) | 4.2(−8.5~16.9) | 0.43 |
| C0-7ROM | 45.1(36.0~54.2) | 51.4(34.7~68.1) | −6.3(−19.7~7.1) | 0.28 |
| C0-2/C0-7 | 0.5 (0.3~0.7) | 0.5(0.4~0.7) | −0.1(−0.2~0.1) | 0.24 |
| C2-7/C0-7 | 0.6(0.4~0.8) | 0.5(0.4~0.5) | 0.2(0.0~0.4) | 0.09 |
| T1slope | 28.8(22.9~34.7) | 15.2(9.7~20.6) | 13.7(7.1~20.2) | <0.01 * |
| Lumbar lordosis | 31.3(16.2~46.4) | 28.0(18.1~37.9) | 3.0(−4.1~10.1) | 0.28 |
| sacral slope | 33.4(22.2~44.6) | 35.0(26.9~43.1) | −0.4(−4.5~3.8) | 0.79 |
| pelvic tilt | 12.8(5.0~20.6) | 15.0(9.2~20.8) | −2.8(−23.4~17.7) | 0.69 |
| pelvic incidence | 46.1(33.1~59.1) | 41.7(20.7~62.7) | −3.2(−25.1~18.7) | 0.67 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.W.; Jang, S.B.; Lee, H.M.; Lee, J.H.; Lee, M.U.; Kim, J.W.; Yee, J.S. Analysis of Cervical Spine Alignment and its Relationship with Other Spinopelvic Parameters after Laminoplasty in Patients with Degenerative Cervical Myelopathy. J. Clin. Med. 2020, 9, 713. https://doi.org/10.3390/jcm9030713
Kim SW, Jang SB, Lee HM, Lee JH, Lee MU, Kim JW, Yee JS. Analysis of Cervical Spine Alignment and its Relationship with Other Spinopelvic Parameters after Laminoplasty in Patients with Degenerative Cervical Myelopathy. Journal of Clinical Medicine. 2020; 9(3):713. https://doi.org/10.3390/jcm9030713
Chicago/Turabian StyleKim, Seok Woo, Seung Bo Jang, Hyung Min Lee, Jeong Hwan Lee, Min Uk Lee, Jeong Woo Kim, and Jae Sung Yee. 2020. "Analysis of Cervical Spine Alignment and its Relationship with Other Spinopelvic Parameters after Laminoplasty in Patients with Degenerative Cervical Myelopathy" Journal of Clinical Medicine 9, no. 3: 713. https://doi.org/10.3390/jcm9030713
APA StyleKim, S. W., Jang, S. B., Lee, H. M., Lee, J. H., Lee, M. U., Kim, J. W., & Yee, J. S. (2020). Analysis of Cervical Spine Alignment and its Relationship with Other Spinopelvic Parameters after Laminoplasty in Patients with Degenerative Cervical Myelopathy. Journal of Clinical Medicine, 9(3), 713. https://doi.org/10.3390/jcm9030713