Prediction of the Epidemic Peak of Coronavirus Disease in Japan, 2020


Abstract
:1. Introduction
2. Methods
2.1. Model
2.2. Sensitivity of the Basic Reproduction Number
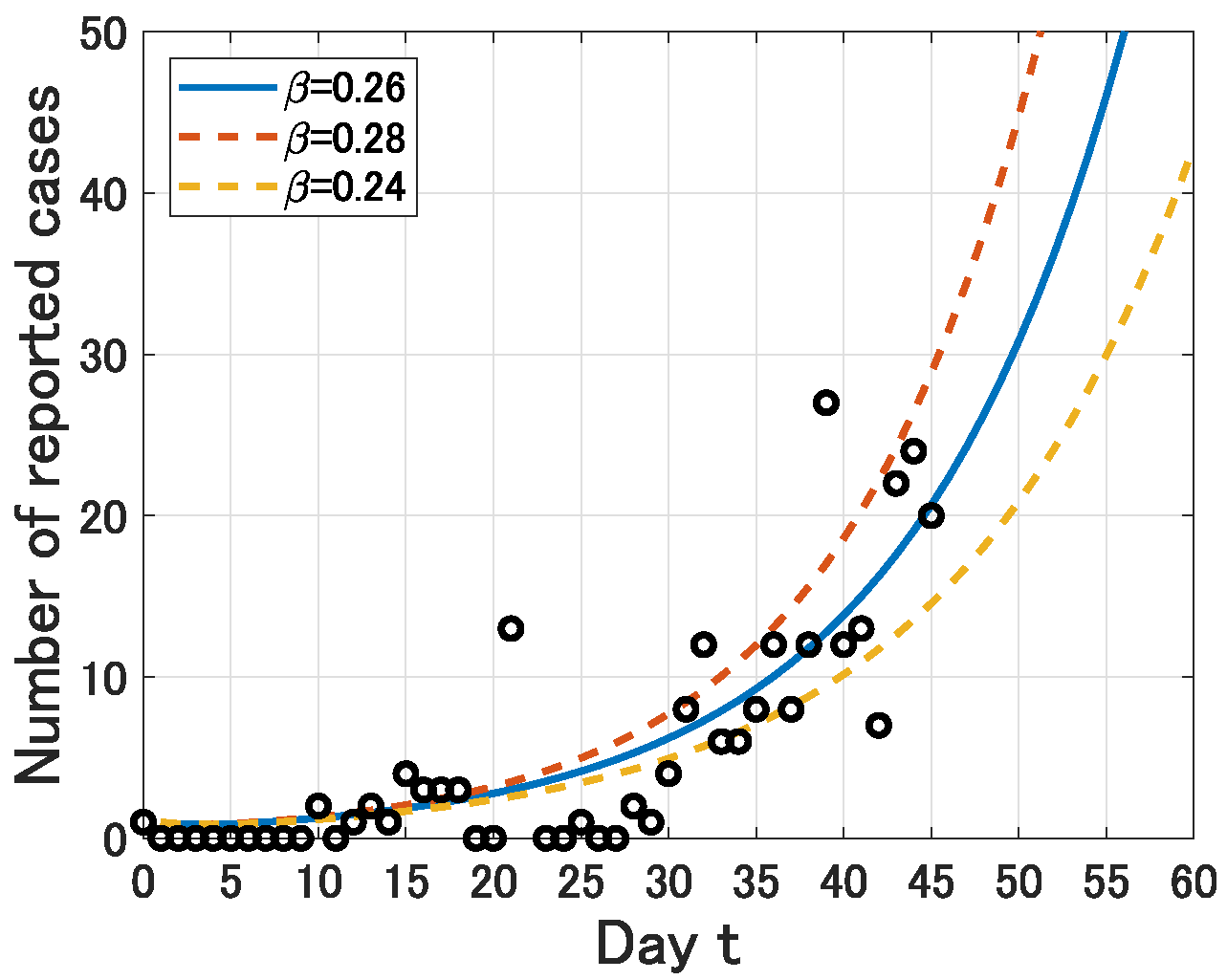
2.3. Estimation of the Infection Rate
3. Results
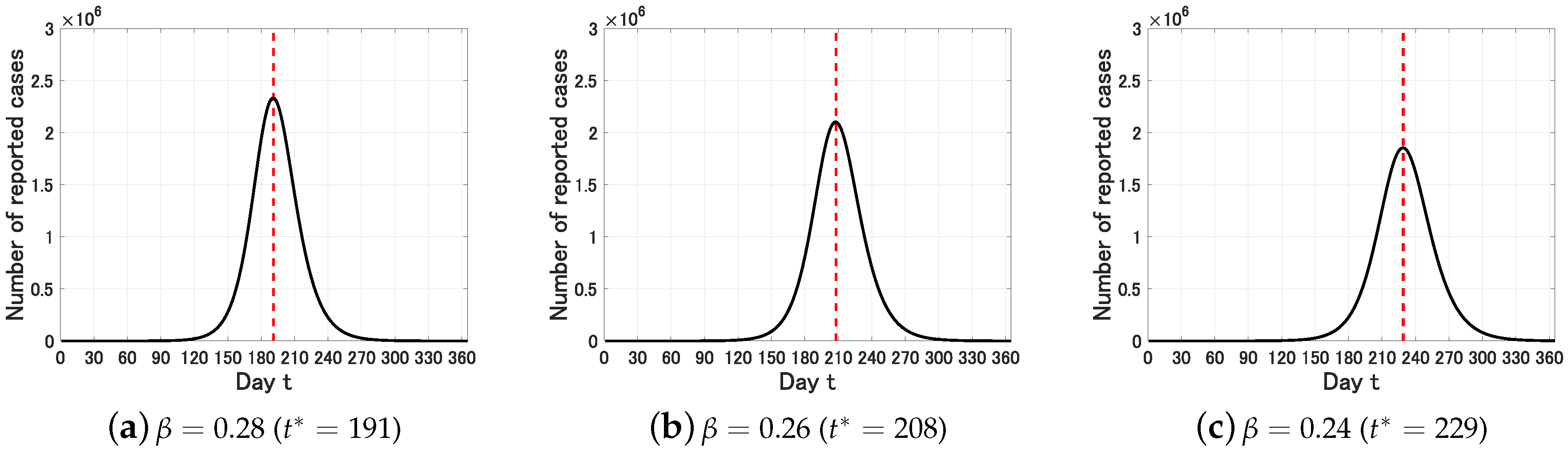
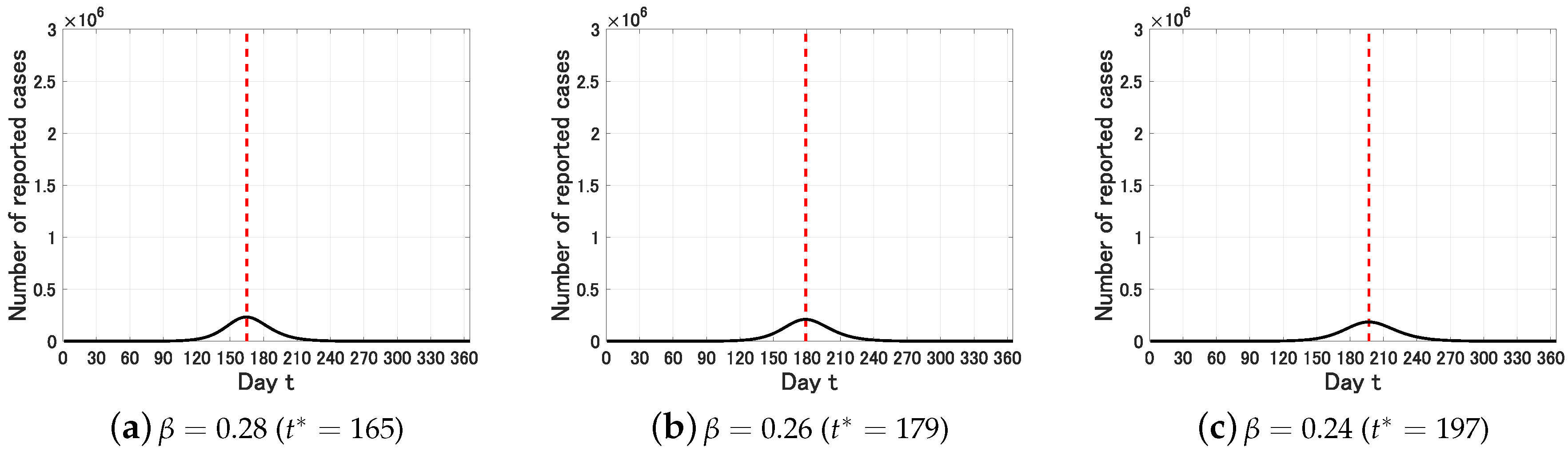
3.1. Peak Prediction
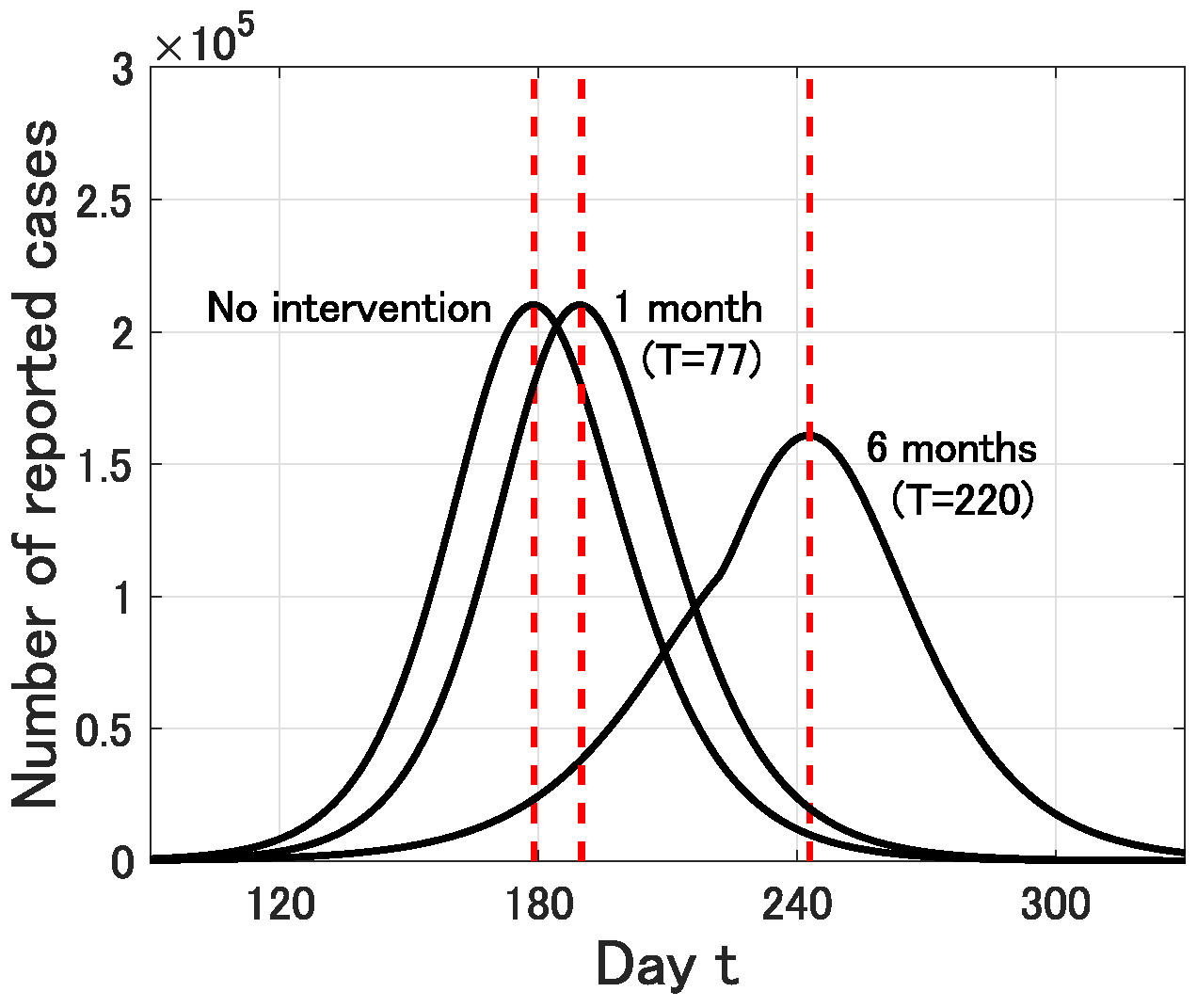
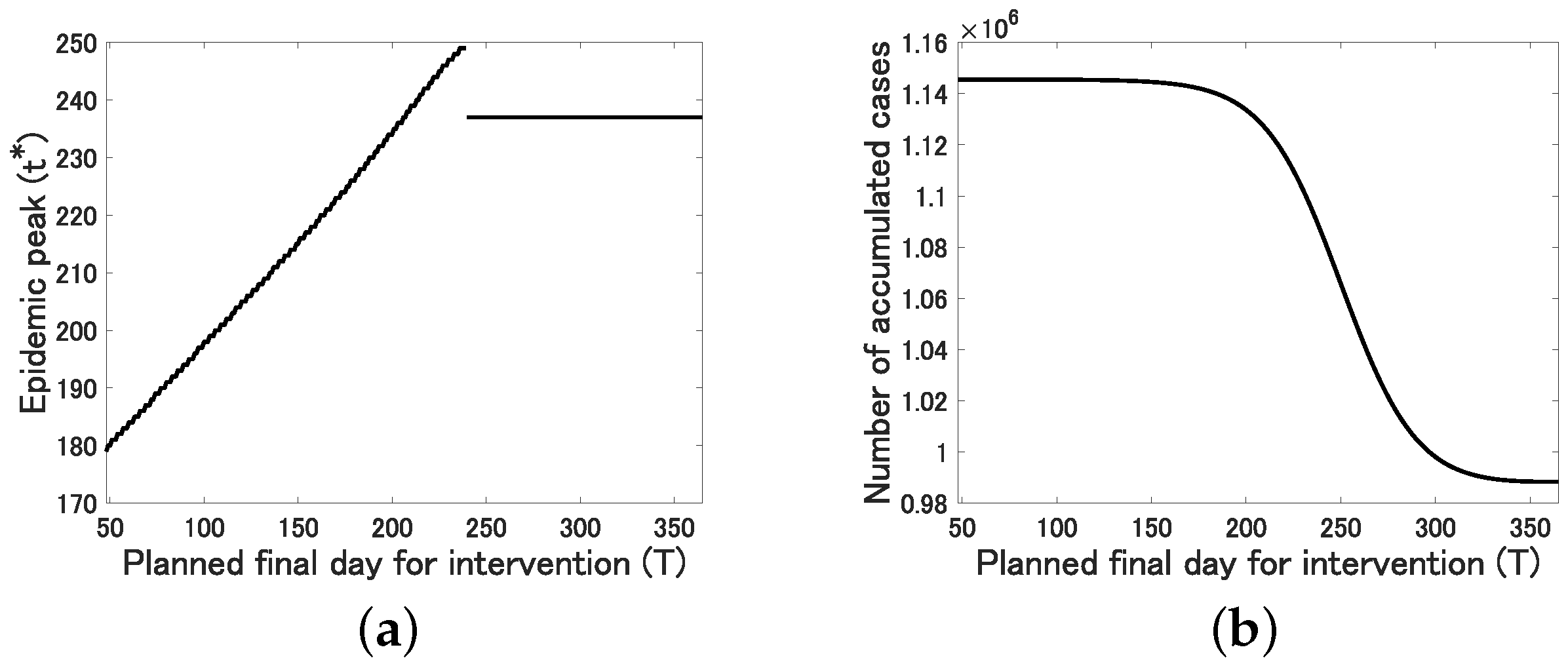
3.2. Possible Effect of Intervention
4. Discussion
- The essential epidemic size, which is characterized by , would not be affected by the identification rate p in a realistic parameter range –, in particular, .
- The intervention exactly has a positive effect on the delay of the epidemic peak, which would contribute to improve the medical environment utilizing the extra time period.
- Intervention over a relatively long period is needed to effectively reduce the final epidemic size.
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/index.html (accessed on 23 February 2020).
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 5 March 2020).
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Jankem, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. New Eng. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHK World Japan. Japan Sets up Emergency Measures for Coronavirus. Available online: https://www3.nhk.or.jp/nhkworld/en/news/20200213_07/ (accessed on 17 February 2020).
- Inaba, H. Age-Structured Populatin Dynamics in Demography and Epidemiology; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Linton, N.M.; Kobayashi, T.; Yang, Y.; Hayashi, K.; Akhmetzhanov, A.R.; Jung, S.; Yuan, B.; Kinoshita, R.; Nishiura, H. Incubation period and other epidemiological characteristics of 2019 novel coronavirus infections with right truncation: A statistical analysis of publicly available case data. J. Clin. Med. 2020, 9, 538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.; Qiu, Y.; Yan, H.; Huang, Y.; Zhu, Y.; Chen, S.X. Tracking and predicting COVID-19 epidemic in China mainland. medRxive 2020. [Google Scholar] [CrossRef] [Green Version]
- Statistics Bureau Japan. Population Estimates Monthly Report January. Available online: https://web.archive.org/web/20190623053923/http://www.stat.go.jp/english/data/jinsui/tsuki/index.html (accessed on 5 March 2020).
- Bloomberg. Japan’s Hokkaido may Have 940 Infected, Researcher Says. Available online: https://www.bloomberg.com/news/articles/2020-03-03/japan-s-hokkaido-could-have-up-to-940-infected-researcher-says (accessed on 5 March 2020).
- Diekmann, O.; Heesterbeek, J.A.P.; Metz, J.A.J. On the definition and the computation of the basic reproduction ratio R0 in models for infectious diseases in heterogeneous populations. J. Math. Biol. 1990, 28, 365–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Driessche, P.; Watmough, J. Reproduction numbers and sub-threshold endemic equilibria for compartmental models of disease transmission. Math. Biosci. 2002, 180, 29–48. [Google Scholar] [CrossRef]
- Capaldi, A.; Behrend, S.; Berman, B.; Smith, J.; Wright, J.; Lloyd, A.L. Parameter estimation and uncertainty quantification for an epidemic model. Math. Biosci. Eng. 2012, 9, 553–576. [Google Scholar] [PubMed]
- The Japan Times. Nearly All Prefectures in Japan Shut Schools Amid Coronavirus Outbreak. Available online: https://www.japantimes.co.jp/news/2020/03/02/national/japan-prefectures-shut-schools-covid-19/#.XmIKE0BuKUk (accessed on 6 March 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and imoprtant lessons from the coronavirus disease 2019 (COVID-19) outbreak in China. J. Am. Med. Assoc. 2020. [Google Scholar] [CrossRef] [PubMed]
- CNBC. It’s a ‘false hope’ Coronavirus will Disappear in the Summer like the Flu, WHO Says. Available online: https://www.cnbc.com/2020/03/06/its-a-false-hope-coronavirus-will-disappear-in-the-summer-like-the-flu-who-says.html (accessed on 8 March 2020).
- Imai, N.; Cori, A.; Dorigatti, I.; Baguelin, M.; Connelly, C.A.; Riley, S.; Ferguson, N.M. Report 3: Transmissibility of 2019-nCoV; Imperial College London: London, UK, 2020. [Google Scholar]
- Liu, T.; Hu, J.; Kang, M.; Lin, L.; Zhong, H.; Xiao, J.; He, G.; Song, T.; Huang, Q.; Rong, Z.; et al. Transmission dynamics of 2019 novel coronavirus (2019-nCoV). bioRxive 2020. [Google Scholar] [CrossRef] [Green Version]
- Read, J.M.; Bridgen, J.R.E.; Cummings, D.A.T.; Ho, A.; Jewell, C.P. Novel coronavirus 2019-nCoV: Ealry estimation of epidemiological parameters and epidemic predictions. medRxive 2020. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.; Lin, Q.; Ran, J.; Musa, S.S.; Yang, G.; Wang, W.; Lou, Y.; Gao, D.; Yang, L.; He, D.; et al. Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: A data-driven analysis in the early phase of the outbreak. Int. J. Infect. Dis. 2020, 92, 214–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel. Med. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week | Number of Newly Reported Cases | Number of Accumulated Cases |
|---|---|---|
| 12 January–18 January | 1 | 1 |
| 19 January–25 January | 2 | 3 |
| 26 January–1 February | 14 | 17 |
| 2 February–8 February | 8 | 25 |
| 9 February–16 February | 28 | 53 |
| 17 February–23 February | 79 | 132 |
| 24 February–1 March | 107 | 239 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuniya, T. Prediction of the Epidemic Peak of Coronavirus Disease in Japan, 2020. J. Clin. Med. 2020, 9, 789. https://doi.org/10.3390/jcm9030789
Kuniya T. Prediction of the Epidemic Peak of Coronavirus Disease in Japan, 2020. Journal of Clinical Medicine. 2020; 9(3):789. https://doi.org/10.3390/jcm9030789
Chicago/Turabian StyleKuniya, Toshikazu. 2020. "Prediction of the Epidemic Peak of Coronavirus Disease in Japan, 2020" Journal of Clinical Medicine 9, no. 3: 789. https://doi.org/10.3390/jcm9030789
APA StyleKuniya, T. (2020). Prediction of the Epidemic Peak of Coronavirus Disease in Japan, 2020. Journal of Clinical Medicine, 9(3), 789. https://doi.org/10.3390/jcm9030789