Knowledge of Rare Respiratory Diseases among Paediatricians and Medical School Students

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Statistical Analysis
3. Results
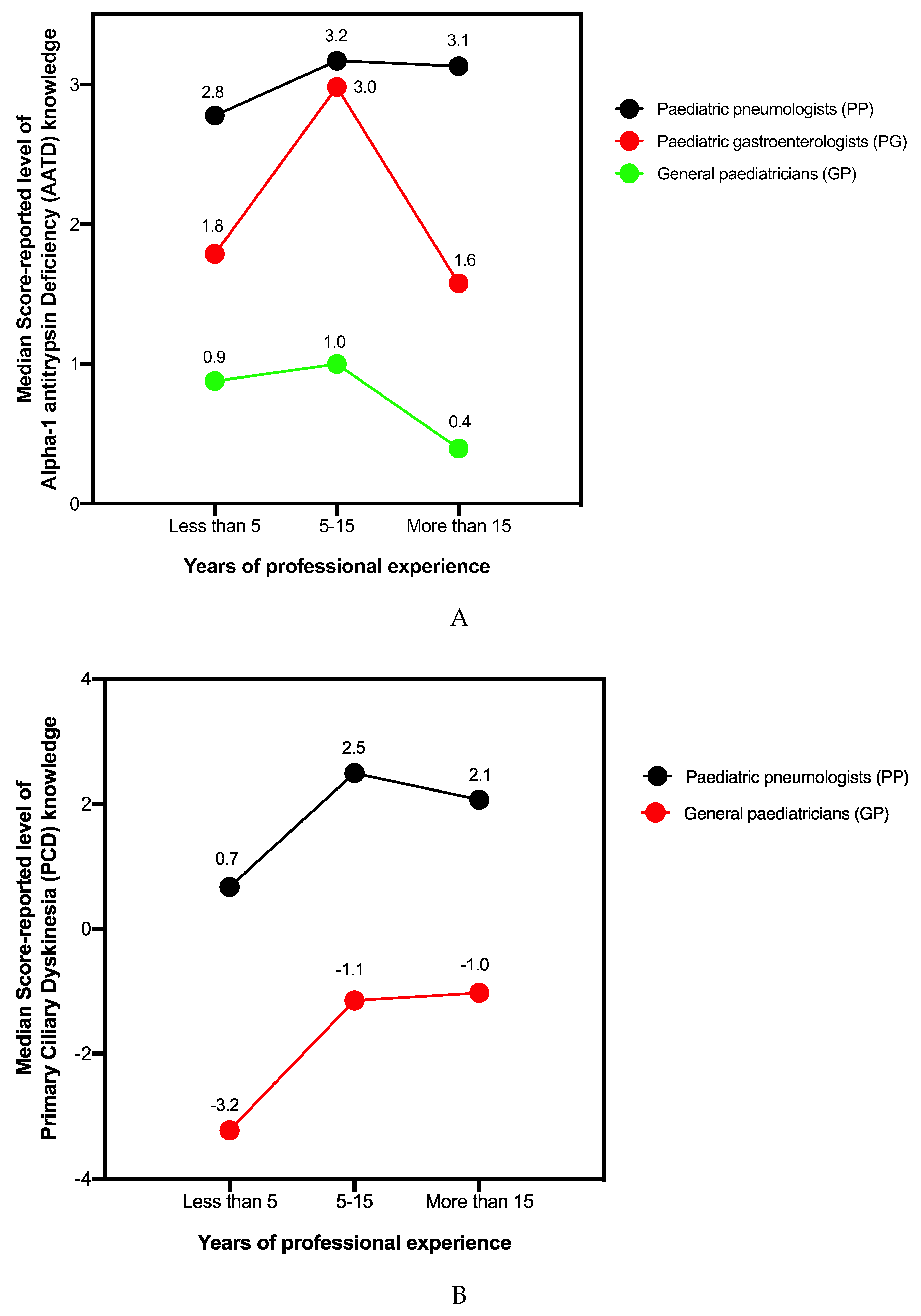
3.1. AATD Knowledge
3.2. PCD Knowledge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Torres-Durán, M.; Lopez-Campos, J.L.; Barrecheguren, M.; Miravitlles, M.; Martinez-Delgado, B.; Castillo, S.; Escribano, A.; Baloira, A.; Navarro-Garcia, M.M.; Pellicer, D.; et al. Alpha-1 antitrypsin deficiency: Outstanding questions and future directions. Orphanet J. Rare Dis. 2018, 13, 114. [Google Scholar] [CrossRef] [Green Version]
- Miravitlles, M.; Dirksen, A.; Ferrarotti, I.; Koblizek, V.; Lange, P.; Mahadeva, R.; McElvaney, N.G.; Parr, D.; Piitulainen, E.; Roche, N.; et al. European Respiratory Society statement: Diagnosis and treatment of pulmonary disease in alpha1-antitrypsin deficiency. Eur. Respir. J. 2017, 30, 50. [Google Scholar] [CrossRef] [Green Version]
- Greulich, T.; Vogelmeier, C.F. Alpha-1-antitrypsin deficiency: Increasing awareness and improving diagnosis. Ther. Adv. Respir. Dis. 2016, 10, 72–84. [Google Scholar] [CrossRef] [Green Version]
- Stoller, J.K.; Aboussouan, L.S. A Review of 1-Antitrypsin Deficiency. Am. J. Respir. Crit. Care Med. 2012, 185, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Greulich, T.; Ottaviani, S.; Bals, R.; Lepper, P.M.; Vogelmeier, C.; Luisetti, M.; Ferrarotti, I. Alpha1-antitrypsin deficiency—Diagnostic testing and disease awareness in Germany and Italy. Respir. Med. 2013, 107, 1400–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reula, A.; Lucas, J.S.; Moreno-Galdó, A.; Romero, T.; Milara, X.; Carda, C.; Mata-Roig, M.; Escribano, A.; Dasi, F.; Armengot-Carceller, M. New insights in primary ciliary dyskinesia. Expert Opin. Orphan Drugs 2017, 5, 537–548. [Google Scholar] [CrossRef] [Green Version]
- Lobo, J.; Zariwala, M.A.; Noone, P.G. Primary ciliary dyskinesia. Semin. Respir. Crit. Care Med. 2015, 36, 169–179. [Google Scholar] [CrossRef] [Green Version]
- Knowles, M.R.; Daniels, L.A.; Davis, S.D.; Zariwala, M.A.; Leigh, M.W. Primary ciliary dyskinesia: Recent advances in diagnostics, genetics, and characterization of clinical disease. Am. J. Respir. Crit. Care Med. 2013, 188, 913–922. [Google Scholar] [CrossRef] [Green Version]
- Kuehni, C.E.; Frischer, T.; Strippoli, M.P.F.; Maurer, E.; Bush, A.; Nielsen, K.G.; Escribano, A.; Lucase, J.S.A.; Yiallouros, P.; Omran, H.; et al. Factors influencing age at diagnosis of primary ciliary dyskinesia in European children. Eur. Respir. J. 2010, 36, 1248–1258. [Google Scholar] [CrossRef] [Green Version]
- Casas, F.; Blanco, I.; Martínez, M.T.; Bustamante, A.; Miravitlles, M.; Cadenas, S.; Hernández, J.M.; Lázaro, L.; Rodríguez, E.; Rodríguez-Frías, F.; et al. Actualización sobre indicaciones de búsqueda activa de casos y tratamiento con alfa-1 antitripsina por vía intravenosa en pacientes con enfermedad pulmonar obstructiva crónica asociada a déficit de alfa-1 antitripsina. Arch. Bronconeumol. 2015, 51, 185–192. [Google Scholar] [CrossRef]
- Siri, D.; Farah, H.; Hogarth, D.K. Distinguishing alpha1-antitrypsin deficiency from asthma. Ann. Allergy Asthma Immunol. 2013, 111, 458–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolk, J.; Seersholm, N.; Kalsheker, N. Alpha1-antitrypsin deficiency: Current perspective on research, diagnosis, and management. Int. J. Chron. Obstruct. Pulmon. Dis. 2006, 1, 151–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolk, J. Case detection of α1-antitrypsin deficiency: Does it help the patient or the doctor? Eur. Respir. J. 2005, 26, 561–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanash, H.A.; Nilsson, P.M.; Nilsson, J.Å.; Piitulainen, E. Clinical course and prognosis of never-smokers with severe alpha-1-antitrypsin deficiency (PiZZ). Thorax 2008, 63, 1091–1095. [Google Scholar] [CrossRef] [Green Version]
- Teckman, J.H. Liver disease in alpha-1 antitrypsin deficiency: Current understanding and future therapy. COPD J. Chronic Obstr. Pulm. Dis. 2013, 10, 35–43. [Google Scholar] [CrossRef]
- Bush, A.; Chodhari, R.; Collins, N.; Copeland, F.; Hall, P.; Harcourt, J.; Hariri, M.; Hogg, C.; Lucas, J.; Mitchison, H.M.; et al. Primary ciliary dyskinesia: Current state of the art. Arch. Dis. Child. 2007, 92, 1136–1140. [Google Scholar] [CrossRef]
- Barbato, A.; Frischer, T.; Kuehni, C.E.; Snijders, D.; Azevedo, I.; Baktai, G.; Bartoloni, L.; Eber, E.; Escribano, A.; Haarman, E.; et al. Primary ciliary dyskinesia: A consensus statement on diagnostic and treatment approaches in children. Eur. Respir. J. 2009, 34, 1264–1276. [Google Scholar] [CrossRef] [Green Version]
- Mittal, V.; Shah, A. Situs Inversus Totalis: The Association of Kartagener’s Syndrome with Diffuse Bronchiolitis and Azoospermia. Arch. Bronconeumol. 2012, 48, 179–182. [Google Scholar] [CrossRef]
- Magnin, M.L.; Cros, P.; Beydon, N.; Mahloul, M.; Tamalet, A.; Escudier, E.; Clément, A.; le Pointe, H.D.; Blanchon, S. Longitudinal lung function and structural changes in children with primary ciliary dyskinesia. Pediatr. Pulmonol. 2012, 47, 816–825. [Google Scholar]
- Armengot, M.; Bonet, M.; Carda, C.; Gómez, M.J.; Milara, J.; Mata, M.; Cortijo, J. Development and Validation of a Method of Cilia Motility Analysis for the Early Diagnosis of Primary Ciliary Dyskinesia. Acta Otorrinolaringol. 2012, 63, 1–8. [Google Scholar] [CrossRef]
- Carlén, B.; Stenram, U. Primary ciliary dyskinesia: A review. Ultrastruct. Pathol. 2005, 29, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Armengot, M.; Milara, J.; Mata, M.; Carda, C.; Cortijo, J. Cilia motility and structure in primary and secondary ciliary dyskinesia. Am. J. Rhinol. Allergy 2010, 24, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Taliercio, R.M.; Chatburn, R.L.; Stoller, J.K. Knowledge of alpha-1 antitrypsin deficiency among internal medicine house officers and respiratory therapists: Results of a survey. Respir. Care 2010, 55, 322–327. [Google Scholar] [PubMed]
- Esquinas, C.; Barrecheguren, M.; Sucena, M.; Rodriguez, E.; Fernandez, S.; Miravitlles, M. Practice and knowledge about diagnosis and treatment of alpha-1 antitrypsin deficiency in Spain and Portugal. BMC Pulm. Med. 2016. [Google Scholar] [CrossRef] [Green Version]
- European, Respiratory Society, and American Thoracic Society. American Thoracic Society/European Respiratory Society statement: Standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am. J. Respir. Crit. Care Med. 2003, 168, 818–900. [Google Scholar] [CrossRef]
- University of Valencia. School of Medicine Degree Programme. Available online: https://www.uv.es/uvweb/undergraduate-degree-medicine/en/what-can-study-/degree-programme/degree-programme/degree-medicine-1285938467926/Titulacio.html?id=1285847387054&p2=2 (accessed on 19 March 2020).


{kind=link}
| Demographic Data | Professional Experience | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Years of Clinical Practice | Healthcare Practice Type | AATD/PCD Patient Management | Awareness of Reference Units | |||||||||||
| Groups | Number of Surveys Completed | <5 | 5–15 | >15 | Primary Care (Clinic) | Private Hospital | Public Tertiary Hospital | District Hospital | Private Practice | Public Secondary Hospital | Yes | No | Yes | No |
| General paediatricians (GP) | A: 193 | 25.3% | 35.2% | 39.3% | 57.5% | 2.6% | 19.7% | 17.1% | 2.1% | 1.0% | 48.7% | 51.3% | 14.5% | 85.5% |
| B: 190 | 25.7% | 35.7% | 38.4% | 57.3% | 2.6% | 19.4% | 17.3% | 2.1% | 1.3% | 46.8% | 52.1% | 19.7% | 80.3% | |
| Paediatric pneumologists (PP) | A: 123 | 7.3% | 43.1% | 49.6% | -- | 3.2% | 64.2% | 24.4% | 2.4% | 5.7% | 52.0% | 48.0% | 30.0% | 70.0% |
| B: 123 | 7.4% | 43.0% | 49.6% | -- | 3.2% | 64.2% | 24.3% | 2.4% | 5.7% | 47.1% | 52.9% | 66.6% | 33.3% | |
| Paediatric gastroenterologists (PG) | A: 166 | 28.3% | 32.0% | 39.7% | -- | 8.4% | 63.2% | 26.5% | 1.2% | 0.6% | 66.9% | 33.1% | 22.9% | 77.1% |
| Medical students (MS) | A: 136 | -- | -- | -- | -- | -- | -- | -- | -- | -- | 32.3% | 67.7% | 9.5% | 90.4% |
| B: 135 | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | 8.9% | 91.1% | |
| Groups | Number of Correct Answers on the Clinical Manifestations of the Disease | Correct Answers about the Phenotype of the Disease | Number of Correct Answers about the Treatment of the Disease | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 0 | 1 | 2 | 3 | ||
| General paediatricians (GP) | 44.5% | 38.5% | 15.5% | 1.50% | 59.1% | 16.1% | 24.9% | 33.2% | 25.8% |
| Paediatric pneumologists (PP) | 12.2% | 47.9% | 37.4% | 2.4% | 93.5% | 9.8% | 26.8% | 38.2% | 25.2% |
| Paediatric gastroenterologists (PG) | 18.6% | 49.4% | 30.1% | 1.8% | 86.1% | 21.7% | 25.3% | 31.3% | 21.7% |
| Medical students (MS) | 77.9% | 19.8% | 1.4% | 0.7% | 35.3% | 32.4% | 23.5% | 29.4% | 14.7% |
| Groups | Correct clinical Manifestations | Correct Diagnostic Options | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| General paediatricians (GP) | 2.6% | 13.1% | 21.0% | 15.7% | 14.2% | 13.6% | 11.5% | 7.8% | 0.5% | 4.7% | 20.0% | 28.4% | 18.9% | 15.7% | 10.0% | 1.05% | -- | 0.5% | -- |
| Paediatric pneumologists (PP) | -- | 1.6% | 6.5% | 8.1% | 4.8% | 13.0% | 16.2% | 49.5% | -- | 1.6% | 8.1% | 21.9% | 24.3% | 25.5% | 8.9% | 8.1% | 3.5% | -- | -- |
| Medical students (MS) | 17.0% | 22.9% | 25.1% | 12.5% | 8.8% | 9.6% | 1.4% | 2.2% | 4.4% | 8.1% | 18.5% | 19.2% | 23.7% | 18.5% | 5.1% | 1.4% | 0.7% | -- | -- |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Requena-Fernández, M.Á.; Dasí, F.; Castillo, S.; Barajas-Cenobi, R.; Navarro-García, M.M.; Escribano, A. Knowledge of Rare Respiratory Diseases among Paediatricians and Medical School Students. J. Clin. Med. 2020, 9, 869. https://doi.org/10.3390/jcm9030869
Requena-Fernández MÁ, Dasí F, Castillo S, Barajas-Cenobi R, Navarro-García MM, Escribano A. Knowledge of Rare Respiratory Diseases among Paediatricians and Medical School Students. Journal of Clinical Medicine. 2020; 9(3):869. https://doi.org/10.3390/jcm9030869
Chicago/Turabian StyleRequena-Fernández, María Ángeles, Francisco Dasí, Silvia Castillo, Rafael Barajas-Cenobi, María Mercedes Navarro-García, and Amparo Escribano. 2020. "Knowledge of Rare Respiratory Diseases among Paediatricians and Medical School Students" Journal of Clinical Medicine 9, no. 3: 869. https://doi.org/10.3390/jcm9030869
APA StyleRequena-Fernández, M. Á., Dasí, F., Castillo, S., Barajas-Cenobi, R., Navarro-García, M. M., & Escribano, A. (2020). Knowledge of Rare Respiratory Diseases among Paediatricians and Medical School Students. Journal of Clinical Medicine, 9(3), 869. https://doi.org/10.3390/jcm9030869