Clinical Characteristics and Associated Risk Factors of Prediabetes in the Southwestern Region of Korea from 2010–2019



Abstract
:1. Introduction
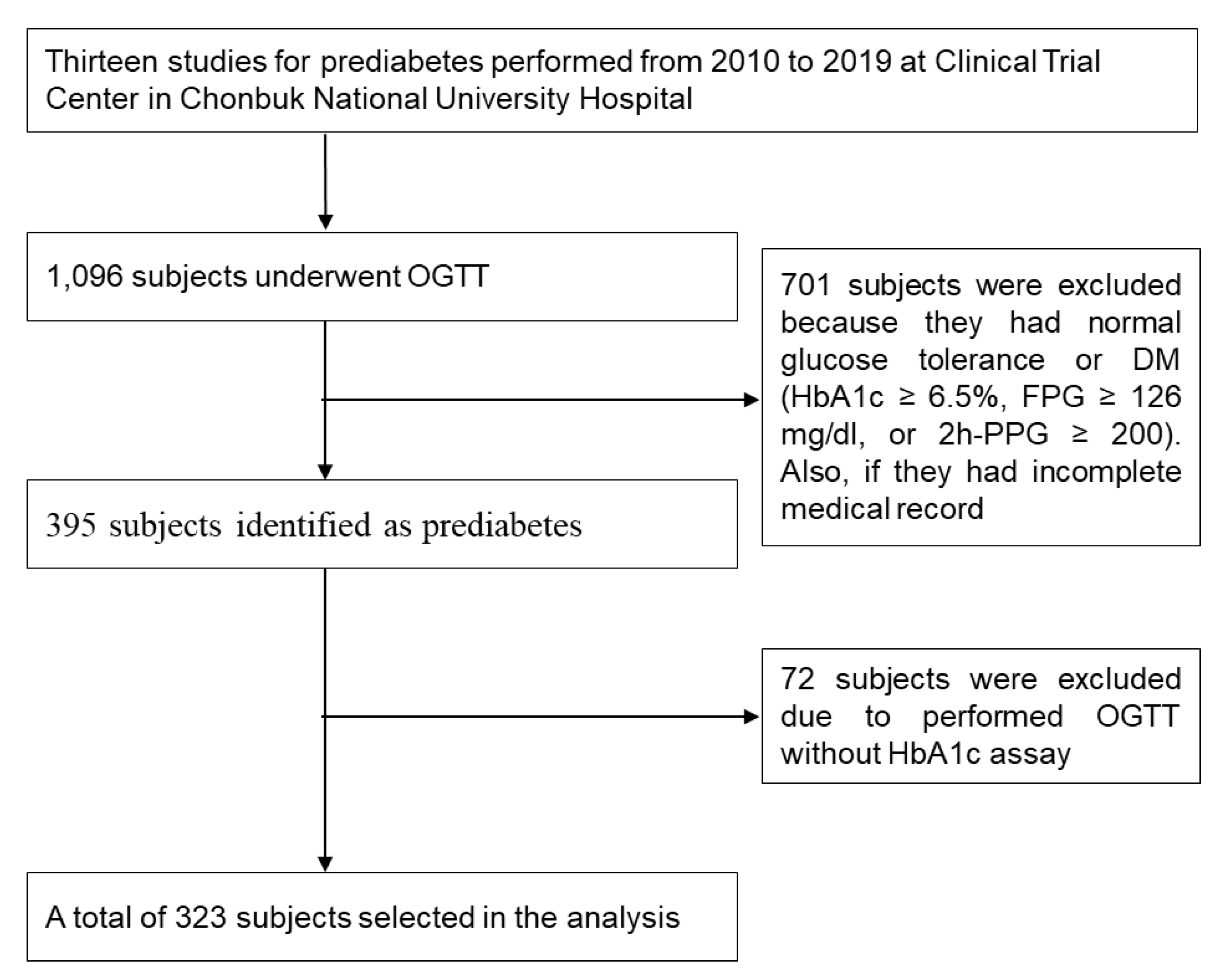
2. Subjects and Methods
2.1. Data Collection
2.2. Definitions
2.3. Assays and Calculations
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Subjects According to Prediabetes Subtypes
3.2. Glucose Parameters in the Subjects Defined by Prediabetes Subtypes
3.3. Biochemical Characteristics of the Subjects Defined by Prediabetes Subtypes
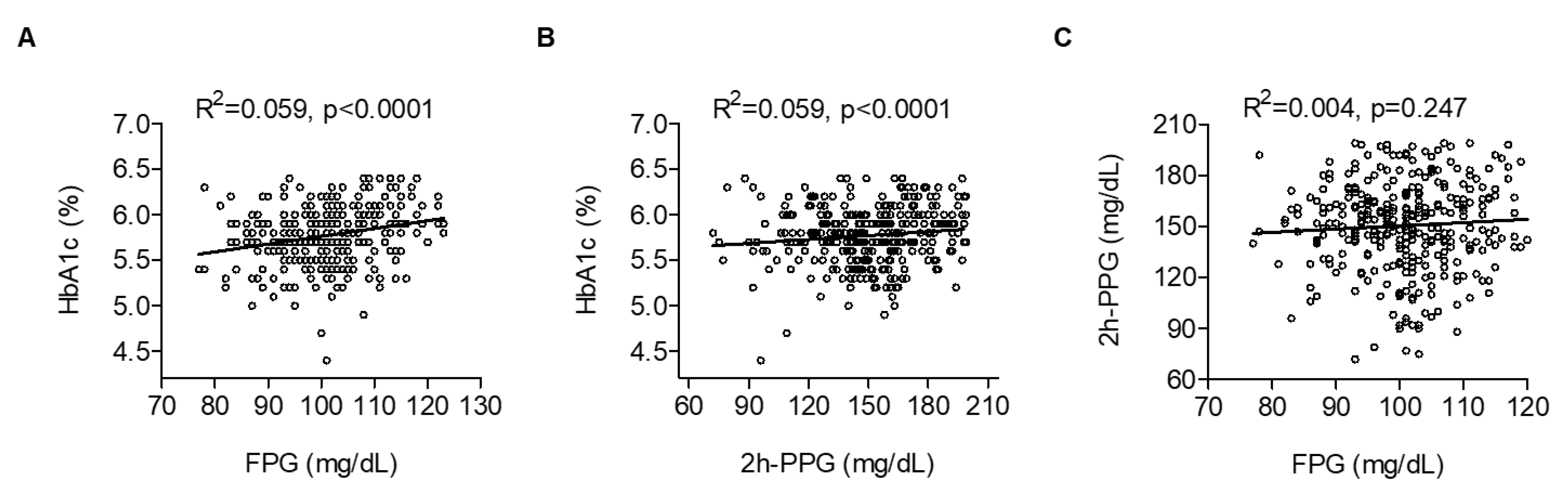
3.4. Risk Factors of FPG, 2h-PPG and HbA1c Levels in Subjects with Prediabetes
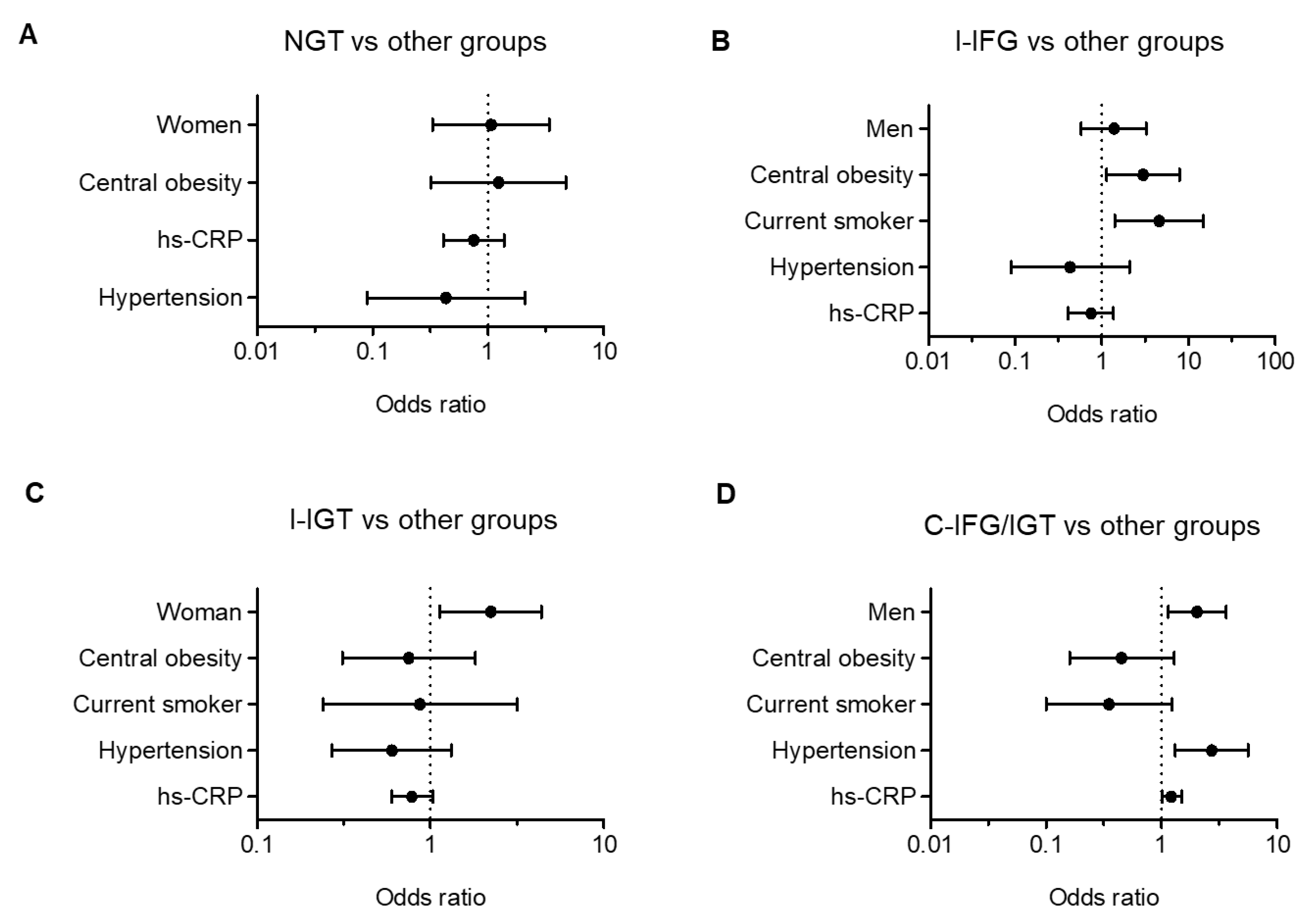
3.5. Risk Factors Associated with Prediabetes Subtypes
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Tabak, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimaki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul-Ghani, M.A.; Tripathy, D.; DeFronzo, R.A. Contributions of beta-cell dysfunction and insulin resistance to the pathogenesis of impaired glucose tolerance and impaired fasting glucose. Diabetes Care 2006, 29, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Korean Centers for Disease Control and Prevention. Evidence-Based Guideline for Type 2 Diabetes in Primary Care. Available online: www.digitalcpg.kr (accessed on 7 April 2020).
- Hostalek, U. Global epidemiology of prediabetes—Present and future perspectives. Clin. Diabetes Endocrinol. 2019, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, J.; Lindstrom, J.; Eriksson, J.G.; Valle, T.T.; Hamalainen, H.; Ilanne-Parikka, P.; Keinanen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Chiasson, J.L.; Josse, R.G.; Gomis, R.; Hanefeld, M.; Karasik, A.; Laakso, M.; Group, S.-N.T.R. Acarbose for prevention of type 2 diabetes mellitus: The STOP-NIDDM randomised trial. Lancet 2002, 359, 2072–2077. [Google Scholar] [CrossRef]
- Gillies, C.L.; Abrams, K.R.; Lambert, P.C.; Cooper, N.J.; Sutton, A.J.; Hsu, R.T.; Khunti, K. Pharmacological and lifestyle interventions to prevent or delay type 2 diabetes in people with impaired glucose tolerance: Systematic review and meta-analysis. BMJ 2007, 334, 299. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Gao, P.; Zhang, M.; Huang, Z.; Zhang, D.; Deng, Q.; Li, Y.; Zhao, Z.; Qin, X.; Jin, D.; et al. Prevalence and Ethnic Pattern of Diabetes and Prediabetes in China in 2013. JAMA 2017, 317, 2515–2523. [Google Scholar] [CrossRef]
- Shin, J.Y. Trends in the prevalence and management of diabetes in Korea: 2007–2017. Epidemiol. Health 2019, 41, e2019029. [Google Scholar] [CrossRef] [Green Version]
- Yokota, N.; Miyakoshi, T.; Sato, Y.; Nakasone, Y.; Yamashita, K.; Imai, T.; Hirabayashi, K.; Koike, H.; Yamauchi, K.; Aizawa, T. Predictive models for conversion of prediabetes to diabetes. J. Diabetes Complic. 2017, 31, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Wolever, T.M.; Jenkins, D.J.; Jenkins, A.L.; Josse, R.G. The glycemic index: Methodology and clinical implications. Am. J. Clin. Nutr. 1991, 54, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, A.; Nambi, S.S.; Mather, K.; Baron, A.D.; Follmann, D.A.; Sullivan, G.; Quon, M.J. Quantitative insulin sensitivity check index: A simple, accurate method for assessing insulin sensitivity in humans. J. Clin. Endocrinol. Metab. 2000, 85, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Xiao, X.; Sun, C.; Tian, S.; Sun, Z.; Gao, Y.; Li, Y.; Cheng, J.; Lv, Y.; Li, M.; et al. Ideal glycated hemoglobin cut-off points for screening diabetes and prediabetes in a Chinese population. J. Diabetes Investig. 2016, 7, 695–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oka, R.; Yagi, K.; Sakurai, M.; Nakamura, K.; Moriuchi, T.; Miyamoto, S.; Nohara, A.; Kawashiri, M.A.; Takeda, Y.; Yamagishi, M. Insulin secretion and insulin sensitivity on the oral glucose tolerance test (OGTT) in middle-aged Japanese. Endocr. J. 2012, 59, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Hua, L.; Liu, W.F.; Song, H.L.; Dai, X.W.; Yang, J.K. The prevalence of glucose metabolism disturbances in Chinese Muslims and possible risk factors: A study from northwest China. Arq. Bras. Endocrinol. Metabol. 2014, 58, 715–723. [Google Scholar] [CrossRef] [Green Version]
- Faerch, K.; Borch-Johnsen, K.; Holst, J.J.; Vaag, A. Pathophysiology and aetiology of impaired fasting glycaemia and impaired glucose tolerance: Does it matter for prevention and treatment of type 2 diabetes? Diabetologia 2009, 52, 1714–1723. [Google Scholar] [CrossRef] [Green Version]
- de Vegt, F.; Dekker, J.M.; Jager, A.; Hienkens, E.; Kostense, P.J.; Stehouwer, C.D.; Nijpels, G.; Bouter, L.M.; Heine, R.J. Relation of impaired fasting and postload glucose with incident type 2 diabetes in a Dutch population: The Hoorn Study. JAMA 2001, 285, 2109–2113. [Google Scholar] [CrossRef]
- Engberg, S.; Vistisen, D.; Lau, C.; Glumer, C.; Jorgensen, T.; Pedersen, O.; Borch-Johnsen, K. Progression to impaired glucose regulation and diabetes in the population-based Inter99 study. Diabetes Care 2009, 32, 606–611. [Google Scholar] [CrossRef] [Green Version]
- Han, S.J.; Kim, H.J.; Kim, D.J.; Lee, K.W.; Cho, N.H. Incidence and predictors of type 2 diabetes among Koreans: A 12-year follow up of the Korean Genome and Epidemiology Study. Diabetes Res. Clin. Pract. 2017, 123, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Roh, W.G.; Shin, H.C.; Choi, J.H.; Lee, Y.J.; Kim, K. Alcohol consumption and higher incidence of impaired fasting glucose or type 2 diabetes in obese Korean men. Alcohol 2009, 43, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Van’t Riet, E.; Alssema, M.; Rijkelijkhuizen, J.M.; Kostense, P.J.; Nijpels, G.; Dekker, J.M. Relationship between A1C and glucose levels in the general Dutch population: The new Hoorn study. Diabetes Care 2010, 33, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, F.; Moellering, D.R.; Garvey, W.T. Use of HbA1c for diagnoses of diabetes and prediabetes: Comparison with diagnoses based on fasting and 2-hr glucose values and effects of gender, race, and age. Metab. Syndr. Relat. Disord. 2014, 12, 258–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosmanov, A.R.; Wan, J. Low positive predictive value of hemoglobin A1c for diagnosis of prediabetes in clinical practice. Am. J. Med. Sci. 2014, 348, 191–194. [Google Scholar] [CrossRef]
- Kawakami, N.; Takatsuka, N.; Shimizu, H.; Ishibashi, H. Effects of smoking on the incidence of non-insulin-dependent diabetes mellitus. Replication and extension in a Japanese cohort of male employees. Am. J. Epidemiol. 1997, 145, 103–109. [Google Scholar] [CrossRef]
- Rimm, E.B.; Chan, J.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C. Prospective study of cigarette smoking, alcohol use, and the risk of diabetes in men. BMJ 1995, 310, 555–559. [Google Scholar] [CrossRef] [Green Version]
- Dagogo-Jack, S. Pitfalls in the use of HbA1c as a diagnostic test: The ethnic conundrum. Nat. Rev. Endocrinol. 2010, 6, 589–593. [Google Scholar] [CrossRef]
- Kahan, B.C.; Rehal, S.; Cro, S. Risk of selection bias in randomised trials. Trials 2015, 16, 405. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| NGT | I-IFG | I-IGT | C-IFG/IGT | Total | p-Value † | |
|---|---|---|---|---|---|---|
| Total | 27 (8.4) | 67 (20.7) | 107 (33.1) | 122 (37.8) | 323 (100) | <0.0001 |
| Men, n (%) | 8 (29.6) | 43 (64.2) | 38 (35.5) | 70 (57.4) | 159 (49.2) | <0.0001 |
| Women, n (%) | 19 (70.4) | 24 (35.8) | 69 (64.5) | 52 (42.6) | 164 (50.8) | <0.0001 |
| Age (years) | 51.4 ± 8.6 | 51.0 ± 9.3 | 53.0±9.4 | 51.1 ± 9.3 | 51.7 ± 9.3 | 0.410 |
| ≤39 years, n (%) | 3 (11.1) | 8 (11.9) | 10 (9.3) | 13 (10.7) | 34 (10.5) | 0.937 |
| 40–49 years, n (%) | 7 (25.9) | 18 (26.9) | 22 (20.6) | 29 (23.8) | 76 (23.5) | |
| 50–59 years, n (%) | 12 (44.4) | 29 (43.3) | 47 (43.9) | 58 (47.5) | 146 (45.2) | |
| ≥60 years, n (%) | 5 (18.5) | 12 (17.9) | 28 (26.2) | 22 (18.0) | 67 (20.7) | |
| BMI (kg/m2) | 24.3 ± 2.6 | 25.3 ± 2.6 | 24.7 ± 2.4 | 25.3 ± 2.4 | 25.0 ± 2.5 | 0.084 |
| Normal weight, n (%) | 10 (37.0) | 15 (22.4) | 26 (24.3) | 20 (16.4) | 71 (22.0) | 0.364 |
| Overweight, n (%) | 7 (25.9) | 18 (26.9) | 32 (29.9) | 40 (32.8) | 97 (30.0) | |
| Obese, n (%) | 10 (37.0) | 34 (50.7) | 49 (45.8) | 62 (50.8) | 155 (48.0) | |
| Waist–hip ratio | ||||||
| Men | 0.93 ± 0.03 | 0.92 ± 0.05 | 0.92 ± 0.05 | 0.94 ± 0.05 | 0.93 ± 0.05 | 0.226 |
| Women | 0.88 ± 0.07 | 0.91 ± 0.05 | 0.91 ± 0.05 | 0.92 ± 0.04 | 0.91 ± 0.05 | 0.153 |
| Central obesity, n (%) | 16 (59.3) | 36 (53.7) | 80 (74.8) | 88 (72.1) | 220 (68.1) | 0.049 |
| Current smoker, n (%) | 0 (0.0) | 7 (10.4) | 6 (5.6) | 7 (5.7) | 20 (6.2) | 0.085 |
| Current drinker, n (%) | 5 (18.5) | 25 (37.3) | 40 (37.4) | 62 (50.8) | 132 (40.9) | 0.001 |
| Alcohol consumption (unit/weeks) | 4.66 ± 1.37 | 8.1 ± 7.4 | 6.3 ± 6.9 | 7.3 ± 6.8 | 7.1 ± 6.8 | 0.623 |
| SBP (mmHg) | 119.2 ± 12.5 | 123.1 ± 12.5 | 123.0 ± 13.4 | 125.1 ± 12.9 | 123.5 ± 13.0 | 0.163 |
| DBP (mmHg) | 76.74 ± 10.23 | 77.9 ± 9.2 | 78.0 ± 9.5 | 80.8 ± 9.2 | 78.9 ± 9.4 | 0.043 a |
| Pulse (BPM) | 72.78 ± 7.56 | 70.8 ± 9.9 | 70.3 ± 9.1 | 70.4 ± 8.1 | 70.7 ± 8.8 | 0.604 |
| NGT | I-IFG | I-IGT | C-IFG/IGT | p-Value † | p-Value ‡ | |
|---|---|---|---|---|---|---|
| OGTT | ||||||
| FPG (mg/dL) | 92.1 ± 5.1 | 105.4 ± 5.0 | 92.8 ± 5.1 | 107.8 ± 6.1 | <0.0001 | <0.0001 a |
| 0.5h-PPG (mg/dL) | 152.1 ± 28.7 | 176.1 ± 27.6 | 163.7 ± 21.8 | 183.0 ± 23.5 | <0.0001 | <0.0001 b |
| 1h-PPG (mg/dL) | 157.2 ± 35.3 | 181.3 ± 37.8 | 181.0 ± 27.6 | 201.5 ± 35.3 | <0.0001 | <0.0001 c |
| 1.5h-PPG (mg/dL) | 139.2 ± 28.3 | 151.6 ± 28.3 | 173.5 ± 28.8 | 189.6 ± 33.6 | <0.0001 | <0.0001 d |
| 2h-PPG (mg/dL) | 118.0 ± 16.4 | 118.3 ± 16.7 | 162.1 ± 15.5 | 165.3 ± 17.3 | <0.0001 | <0.0001 e |
| iAUC0–2h (h*mg/dL) | 93.6 ± 36.1 | 100.7 ± 37.1 | 137.3 ± 33.0 | 140.5 ± 39.3 | <0.0001 | <0.0001 f |
| Cmax (mg/dL) | 171.0 ± 23.5 | 190.9 ± 30.6 | 189.9 ± 21.2 | 209.9 ± 28.9 | <0.0001 | <0.0001 g |
| Tmax (min) | 60 [30–90] | 60 [30–90] | 60 [30–120] | 60 [30–120] | <0.0001 | <0.0001 h |
| FI (μU/mL) | 6.4 ± 2.6 | 8.0 ± 5.6 | 7.2 ± 4.3 | 8.7 ± 5.2 | 0.041 | 0.019 i |
| HOMA-IR | 1.5 ± 0.6 | 2.1 ± 1.5 | 1.7 ± 1.0 | 2.3 ± 1.4 | <0.0001 | <0.0001 j |
| HOMA-β (%) | 79.0 ± 29.0 | 68.6 ± 47.5 | 89.6 ± 53.5 | 71.3 ± 42.7 | 0.009 | 0.025 k |
| QUICKI § | 0.37 ± 0.03 | 0.36 ± 0.06 | 0.37 ± 0.06 | 0.35 ± 0.03 | 0.001 | 0.001 l |
| C-peptide (ng/mL) | 1.8 ± 0.4 | 2.1 ± 0.9 | 1.9 ± 0.6 | 2.1 ± 0.7 | 0.070 | 0.055 |
| HbA1c (%) | 5.9 ± 0.2 | 5.8 ± 0.4 | 5.7 ± 0.3 | 5.8 ± 0.3 | <0.0001 | <0.0001 m |
| NGT | I-IFG | I-IGT | C-IFG/IGT | p-Value † | p-Value ‡ | |
|---|---|---|---|---|---|---|
| CHOL (mg/dL) | 194.2 ± 30.4 | 191.2 ± 32.3 | 197.3 ± 34.3 | 201.2 ± 30.7 | 0.272 | 0.220 |
| TG (mg/dL) | 116.2 ± 64.1 | 136.4 ± 78.2 | 141.3 ± 70.0 | 149.2 ± 74.4 | 0.191 | 0.194 |
| HDL-C (mg/dL) | 53.9 ± 10.8 | 50.4 ± 10.2 | 48.0 ± 10.6 | 48.0 ± 10.2 | 0.028 | 0.030 a |
| LDL-C (mg/dL) | 117.8 ± 29.7 | 114.9 ± 28.1 | 120.8 ± 32.7 | 125.4 ± 29.7 | 0.179 | 0.158 |
| CHOL/HDL | 3.75 ± 0.96 | 3.91 ± 0.85 | 4.29 ± 1.10 | 4.34 ± 0.97 | 0.004 | 0.005 b |
| LDL/HDL | 2.28 ± 0.76 | 2.37 ± 0.72 | 2.65 ± 0.93 | 2.69 ± 0.76 | 0.019 | 0.020 c |
| TG/HDL | 2.39 ± 1.91 | 2.83 ± 1.69 | 3.25 ± 1.99 | 3.39 ± 1.95 | 0.053 | 0.053 |
| ApoA1 (g/L) | 1.52 ± 0.23 | 1.47 ± 0.20 | 1.38 ± 0.20 | 1.38 ± 0.20 | 0.025 | 0.024 d |
| ApoB (g/L) | 1.12 ± 0.16 | 1.09 ± 0.23 | 1.06 ± 0.25 | 1.09 ± 0.22 | 0.813 | 0.735 |
| ApoB/ApoA1 | 0.75 ± 0.14 | 0.75 ± 0.18 | 0.80 ± 0.21 | 0.81 ± 0.20 | 0.451 | 0.360 |
| hs-CRP § (mg/L) | 0.53 ± 0.70 | 1.01 ± 1.91 | 0.75 ± 1.23 | 1.32 ± 2.50 | 0.434 | 0.415 |
| γ-GT (IU/L) | 21.0 ± 10.8 | 38.6 ± 30.2 | 26.5 ± 19.1 | 35.6 ± 26.0 | 0.001 | 0.156 |
| AST (IU/L) | 21.4 ± 4.5 | 24.2 ± 7.0 | 23.4 ± 6.3 | 24.2 ± 6.7 | 0.204 | 0.413 |
| ALT (IU/L) | 20.8 ± 7.5 | 24.9 ± 11.0 | 22.6 ± 8.7 | 26.0 ± 12.1 | 0.025 | 0.129 |
| Total bilirubin (mg/dL) | 0.75 ± 0.26 | 0.84 ± 0.32 | 0.85 ± 0.37 | 0.94 ± 0.43 | 0.201 | 0.257 |
| Variable | Simple Linear Regression | Multiple Regression | ||||
|---|---|---|---|---|---|---|
| Model 1 † | Model 2 ‡ | |||||
| r | p-Value | Β | p-Value | β | p-Value | |
| Age | −0.051 | 0.359 | - | - | - | - |
| BMI | 0.155 | 0.005 | −0.043 | 0.497 | −0.048 | 0.449 |
| WHR | 0.216 | <0.0001 | 0.162 | 0.005 | 0.169 | 0.005 |
| Alcohol consumption | 0.065 | 0.462 | - | - | - | - |
| SBP | 0.080 | 0.154 | - | - | - | - |
| DBP | 0.103 | 0.065 | - | - | - | - |
| Pulse | 0.003 | 0.964 | - | - | - | - |
| 2h-PPG | 0.065 | 0.247 | - | - | - | - |
| iAUC0–2h | 0.043 | 0.454 | - | - | - | - |
| Cmax | 0.426 | <0.0001 | 0.348 | <0.0001 | 0.346 | <0.0001 |
| Tmax | −0.096 | 0.095 | - | - | - | - |
| Fasting insulin a | 0.165 | 0.003 | - | - | - | - |
| HOMA-IR | 0.286 | <0.0001 | 0.223 | <0.0001 | 0.216 | 0.001 |
| HOMA-β | −0.233 | <0.0001 | - | - | - | - |
| QUICKI a,§ | −0.255 | <0.0001 | - | - | - | - |
| C-peptide a | 0.183 | 0.007 | - | - | - | - |
| HbA1c | 0.242 | <0.0001 | 0.227 | <0.0001 | 0.237 | <0.0001 |
| Total CHOL | 0.025 | 0.661 | - | - | - | - |
| TG | 0.044 | 0.451 | - | - | - | - |
| HDL-C | −0.027 | 0.646 | - | - | - | - |
| LDL-C | 0.019 | 0.741 | - | - | - | - |
| Apo B/Apo A1 | −0.019 | 0.809 | - | - | - | - |
| hs-CRP § | 0.080 | 0.233 | - | - | - | - |
| γ-GT | 0.230 | <0.0001 | 0.045 | 0.436 | 0.048 | 0.415 |
| AST a | 0.116 | 0.037 | - | - | - | - |
| ALT a | 0.165 | 0.003 | - | - | - | - |
| Total bilirubin a | 0.129 | 0.074 | - | - | - | - |
| Variable | Simple Linear Regression | Multiple Regression | ||||
|---|---|---|---|---|---|---|
| Model 1 † | Model 2 ‡ | |||||
| r | p-Value | β | p-Value | β | p-Value | |
| Age | 0.070 | 0.211 | - | - | - | - |
| BMI | 0.047 | 0.406 | - | - | - | - |
| WHR | 0.116 | 0.059 | 0.089 | 0.072 | 0.099 | 0.048 |
| Alcohol consumption | 0.014 | 0.873 | - | - | ||
| SBP | 0.130 | 0.019 | 0.077 | 0.119 | 0.087 | 0.081 |
| DBP a | 0.132 | 0.017 | - | - | - | - |
| Pulse | −0.015 | 0.794 | - | - | - | - |
| FPG | 0.065 | 0.247 | - | - | - | - |
| iAUC0–2h | 0.580 | <0.0001 | 0.734 | <0.0001 | 0.705 | <0.0001 |
| Cmax | 0.376 | <0.0001 | −0.320 | <0.0001 | −0.282 | 0.003 |
| Tmax | 0.420 | <0.0001 | 0.258 | <0.0001 | 0.270 | <0.0001 |
| Fasting insulin | 0.052 | 0.354 | - | - | - | - |
| HOMA-IR | 0.058 | 0.297 | - | - | - | - |
| HOMA-β | 0.041 | 0.468 | - | - | - | - |
| QUICKI § | −0.073 | 0.192 | - | - | - | - |
| C-peptide | 0.037 | 0.594 | - | - | - | - |
| HbA1c | 0.119 | 0.032 | 0.042 | 0.395 | 0.023 | 0.678 |
| Total CHOL | 0.052 | 0.368 | - | - | - | - |
| TG | 0.086 | 0.139 | - | - | - | - |
| HDL-C | −0.120 | 0.038 | −0.050 | 0.302 | −0.049 | 0.313 |
| LDL-C | 0.081 | 0.162 | - | - | - | - |
| Apo B/Apo A1 | 0.020 | 0.794 | - | - | - | - |
| hs-CRP § | 0.070 | 0.295 | - | - | - | - |
| γ-GT | −0.037 | 0.534 | - | - | - | - |
| AST | 0.031 | 0.577 | - | - | - | - |
| ALT | 0.067 | 0.228 | - | - | - | - |
| Total bilirubin | −0.001 | 0.994 | - | - | - | - |
| Variable | Simple Linear Regression | Multiple Regression | ||||
|---|---|---|---|---|---|---|
| Model 1 † | Model 2 ‡ | |||||
| r | p-Value | β | p-Value | β | p-Value | |
| Age | 0.223 | <0.0001 | 0.130 | 0.009 | 0.127 | 0.010 |
| BMI | 0.064 | 0.254 | - | - | - | - |
| WHR | 0.018 | 0.771 | - | - | - | - |
| Alcohol consumption | −0.193 | 0.028 | −0.074 | 0.201 | −0.044 | 0.456 |
| SBP | −0.166 | 0.003 | −0.139 | 0.006 | −0.125 | 0.014 |
| DBP a | −0.145 | 0.009 | - | - | - | |
| Pulse | −0.044 | 0.428 | - | - | - | |
| FPG | 0.242 | <0.0001 | 0.287 | <0.0001 | 0.289 | <0.0001 |
| 2h-PPG | 0.119 | 0.032 | 0.029 | 0.606 | 0.014 | 0.809 |
| iAUC0–2h a | 0.191 | 0.001 | - | - | - | - |
| Cmax | 0.238 | <0.0001 | 0.182 | 0.002 | 0.187 | 0.001 |
| Tmax | 0.144 | 0.013 | 0.132 | 0.012 | 0.140 | 0.008 |
| Fasting insulin | 0.071 | 0.202 | - | - | - | - |
| HOMA-IR | 0.099 | 0.076 | - | - | - | - |
| HOMA-β | −0.011 | 0.840 | - | - | - | - |
| QUICKI § | −0.030 | 0.591 | - | - | - | - |
| C-peptide, | −0.030 | 0.660 | - | - | - | - |
| Total CHOL a | 0.160 | 0.006 | - | - | - | - |
| TG | −0.025 | 0.667 | - | - | - | - |
| HDL-C | 0.008 | 0.885 | - | - | - | - |
| LDL-C | 0.211 | <0.0001 | 0.143 | 0.004 | 0.133 | 0.007 |
| Apo A1 | 0.071 | 0.366 | ||||
| Apo B | 0.145 | 0.063 | ||||
| hs-CRP § | 0.117 | 0.036 | 0.043 | 0.378 | 0.055 | 0.252 |
| γ-GT | −0.194 | 0.001 | −0.048 | 0.683 | −0.041 | 0.474 |
| AST | 0.047 | 0.403 | - | - | - | - |
| ALT | 0.087 | 0.119 | - | - | - | - |
| Total bilirubin | −0.153 | 0.033 | 0.136 | 0.007 | 0.136 | 0.006 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, M.-R.; Jung, S.-J.; Bae, E.-J.; Park, B.-H.; Chae, S.-W. Clinical Characteristics and Associated Risk Factors of Prediabetes in the Southwestern Region of Korea from 2010–2019. J. Clin. Med. 2020, 9, 1114. https://doi.org/10.3390/jcm9041114
Oh M-R, Jung S-J, Bae E-J, Park B-H, Chae S-W. Clinical Characteristics and Associated Risk Factors of Prediabetes in the Southwestern Region of Korea from 2010–2019. Journal of Clinical Medicine. 2020; 9(4):1114. https://doi.org/10.3390/jcm9041114
Chicago/Turabian StyleOh, Mi-Ra, Su-Jin Jung, Eun-Ju Bae, Byung-Hyun Park, and Soo-Wan Chae. 2020. "Clinical Characteristics and Associated Risk Factors of Prediabetes in the Southwestern Region of Korea from 2010–2019" Journal of Clinical Medicine 9, no. 4: 1114. https://doi.org/10.3390/jcm9041114
APA StyleOh, M. -R., Jung, S. -J., Bae, E. -J., Park, B. -H., & Chae, S. -W. (2020). Clinical Characteristics and Associated Risk Factors of Prediabetes in the Southwestern Region of Korea from 2010–2019. Journal of Clinical Medicine, 9(4), 1114. https://doi.org/10.3390/jcm9041114