Prognostic Value of Tumor Size in Resected Stage IIIA-N2 Non-Small-Cell Lung Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Surgical Technique
2.3. Histopathological Evaluation
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinicopathologic Characteristics
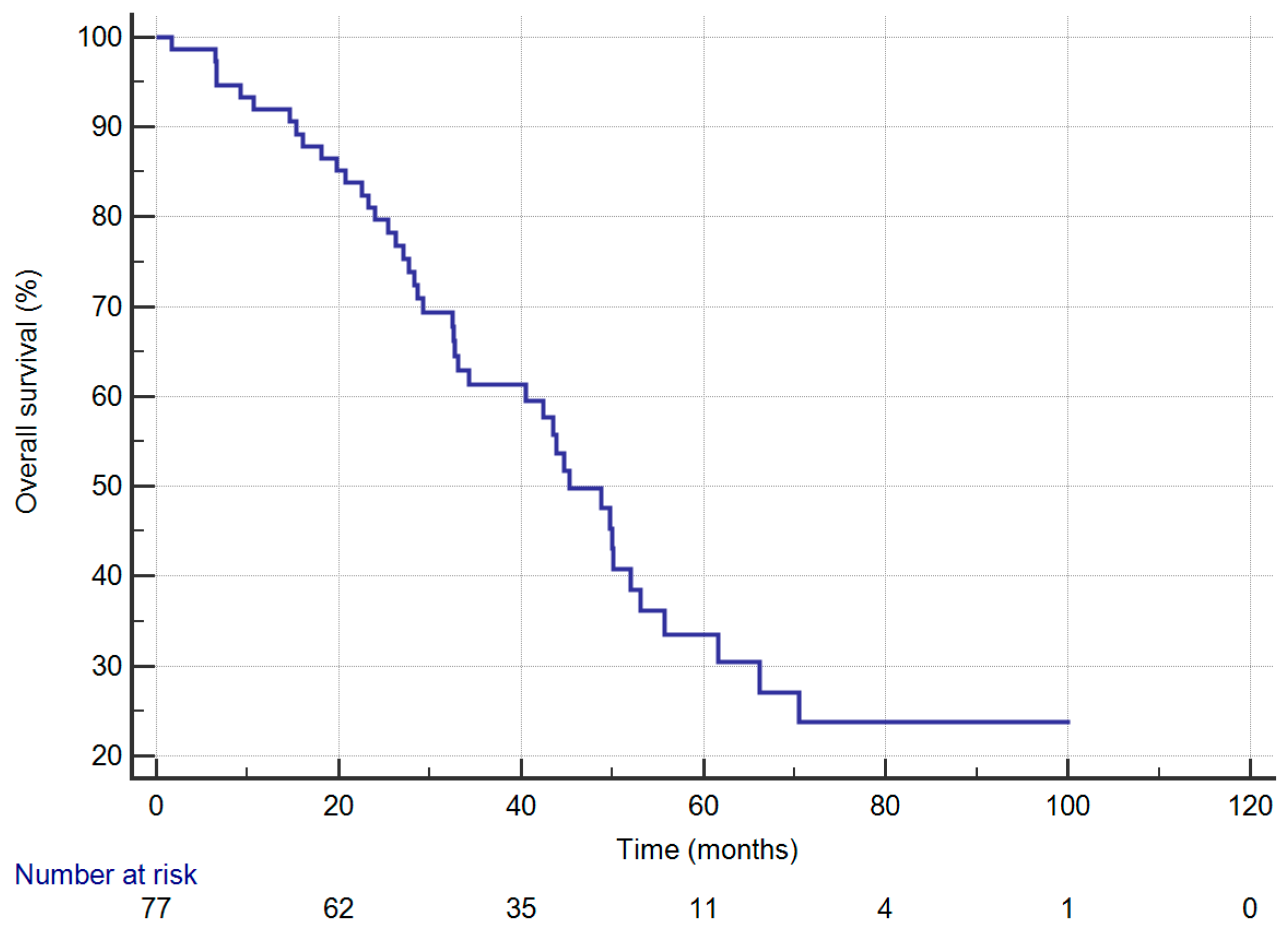
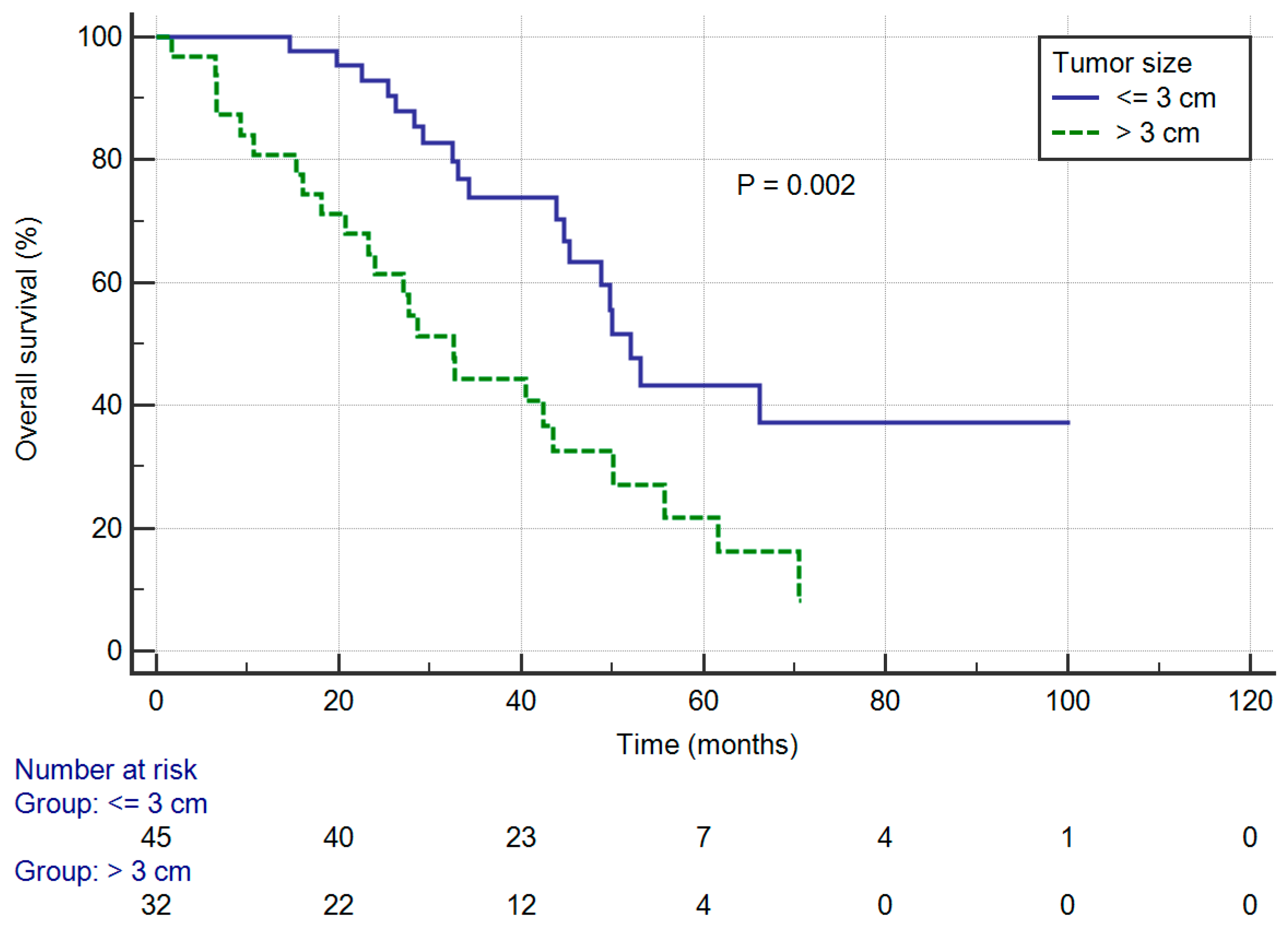
3.2. Overall Survival
3.3. Disease-Free Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, B.Y.; Huang, J.Y.; Cheng, C.Y.; Lin, C.H.; Ko, J.; Liaw, Y.P. Lung cancer and prognosis in taiwan: A population-based cancer registry. J. Thorac. Oncol. 2013, 8, 1128–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.J.N.C.I. SEER Cancer Statistics Review, 1975–2016; National Cancer Institute: Bethesda, MD, USA, 2019.
- Goya, T.; Asamura, H.; Yoshimura, H.; Kato, H.; Shimokata, K.; Tsuchiya, R.; Sohara, Y.; Miya, T.; Miyaoka, E. Prognosis of 6644 resected non-small cell lung cancers in Japan: A Japanese lung cancer registry study. Lung Cancer 2005, 50, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Aisner, D.L.; Wood, D.E.; Akerley, W.; Bauman, J.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; Dilling, T.J.; Dobelbower, M.; et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 5.2018. J. Natl. Compr. Canc. Netw. 2018, 16, 807–821. [Google Scholar] [CrossRef] [Green Version]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, 1–21. [Google Scholar] [CrossRef]
- Sui, X.; Jiang, W.; Chen, H.; Yang, F.; Wang, J.; Wang, Q. Validation of the Stage Groupings in the Eighth Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2017, 12, 1679–1686. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Wang, S.; Zhou, Y.; Lai, S.; Xiao, G.; Gazdar, A.; Xie, Y. Evaluation of the 7(th) and 8(th) editions of the AJCC/UICC TNM staging systems for lung cancer in a large North American cohort. Oncotarget 2017, 8, 66784–66795. [Google Scholar] [CrossRef]
- Rocco, G.; Nason, K.; Brunelli, A.; Varela, G.; Waddell, T.; Jones, D.R. Management of stage IIIA (N2) non-small cell lung cancer: A transatlantic perspective. J. Thorac. Cardiovasc. Surg. 2016, 151, 1235–1238. [Google Scholar] [CrossRef] [Green Version]
- Veeramachaneni, N.K.; Feins, R.H.; Stephenson, B.J.; Edwards, L.J.; Fernandez, F.G. Management of stage IIIA non-small cell lung cancer by thoracic surgeons in North America. Ann. Thorac. Surg. 2012, 94, 922–926, discussion 926–928. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R. The role of surgery in patients with clinical n2 disease. Thorac. Surg. Clin. 2013, 23, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Boffa, D.; Fernandez, F.G.; Kim, S.; Kosinski, A.; Onaitis, M.W.; Cowper, P.; Jacobs, J.P.; Wright, C.D.; Putnam, J.B.; Furnary, A.P. Surgically Managed Clinical Stage IIIA-Clinical N2 Lung Cancer in The Society of Thoracic Surgeons Database. Ann. Thorac. Surg. 2017, 104, 395–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, C.; Yoon, S.; Lee, D.H.; Park, S.I.; Kim, D.K.; Kim, Y.H.; Kim, H.R.; Choi, S.H.; Kim, W.S.; Choi, C.M.; et al. Prognostic Significance of the Number of Metastatic pN2 Lymph Nodes in Stage IIIA-N2 Non-Small-Cell Lung Cancer After Curative Resection. Clin. Lung Cancer 2015, 16, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Garelli, E.; Renaud, S.; Falcoz, P.E.; Weingertner, N.; Olland, A.; Santelmo, N.; Massard, G. Microscopic N2 disease exhibits a better prognosis in resected non-small-cell lung cancer. Eur. J. Cardiothorac. Surg. 2016, 50, 322–328. [Google Scholar] [CrossRef] [Green Version]
- Cerfolio, R.J.; Bryant, A.S. Survival of patients with unsuspected N2 (stage IIIA) nonsmall-cell lung cancer. Ann. Thorac. Surg. 2008, 86, 362–366, discussion 366–367. [Google Scholar] [CrossRef]
- Decaluwe, H.; De Leyn, P.; Vansteenkiste, J.; Dooms, C.; Van Raemdonck, D.; Nafteux, P.; Coosemans, W.; Lerut, T. Surgical multimodality treatment for baseline resectable stage IIIA-N2 non-small cell lung cancer. Degree of mediastinal lymph node involvement and impact on survival. Eur. J. Cardiothorac. Surg. 2009, 36, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Yoshino, I.; Yoshida, S.; Miyaoka, E.; Asamura, H.; Nomori, H.; Fujii, Y.; Nakanishi, Y.; Eguchi, K.; Mori, M.; Sawabata, N.; et al. Surgical outcome of stage IIIA- cN2/pN2 non-small-cell lung cancer patients in Japanese lung cancer registry study in 2004. J. Thorac. Oncol. 2012, 7, 850–855. [Google Scholar] [CrossRef] [Green Version]
- Tsitsias, T.; Boulemden, A.; Ang, K.; Nakas, A.; Waller, D.A. The N2 paradox: Similar outcomes of pre- and postoperatively identified single-zone N2a positive non-small-cell lung cancer. Eur. J. Cardiothorac. Surg. 2014, 45, 882–887. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Zhou, W.; Zhang, H.; Zhao, M.; Chen, X. Feasibility and long-term efficacy of video-assisted thoracic surgery for unexpected pathologic N2 disease in non-small cell lung cancer. Ann. Thorac. Med. 2013, 8, 170–175. [Google Scholar] [CrossRef]
- Jimenez, M.F.; Varela, G.; Novoa, N.M.; Aranda, J.L. Results of surgery for non-small cell lung cancer with N2 involvement unsuspected before thoracotomy. Arch. Bronconeumol. 2008, 44, 65–69. [Google Scholar] [CrossRef]
- Robinson, C.G.; Patel, A.P.; Bradley, J.D.; DeWees, T.; Waqar, S.N.; Morgensztern, D.; Baggstrom, M.Q.; Govindan, R.; Bell, J.M.; Guthrie, T.J.; et al. Postoperative radiotherapy for pathologic N2 non-small-cell lung cancer treated with adjuvant chemotherapy: A review of the National Cancer Data Base. J. Clin. Oncol. 2015, 33, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.F.; Kumar, A.; Gulack, B.C.; Mulvihill, M.S.; Hartwig, M.G.; Wang, X.; D’Amico, T.A.; Berry, M.F. Long-term outcomes after lobectomy for non-small cell lung cancer when unsuspected pN2 disease is found: A National Cancer Data Base analysis. J. Thorac. Cardiovasc. Surg. 2016, 151, 1380–1388. [Google Scholar] [CrossRef] [Green Version]
- Cerfolio, R.J.; Maniscalco, L.; Bryant, A.S. The treatment of patients with stage IIIA non-small cell lung cancer from N2 disease: Who returns to the surgical arena and who survives. Ann. Thorac. Surg. 2008, 86, 912–920, discussion 912–920. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.F.; Adil, S.M.; Anderson, K.L.; Meyerhoff, R.R.; Turley, R.S.; Hartwig, M.G.; Harpole, D.H., Jr.; Tong, B.C.; Onaitis, M.W.; D’Amico, T.A.; et al. Impact of patient selection and treatment strategies on outcomes after lobectomy for biopsy-proven stage IIIA pN2 non-small cell lung cancer. Eur. J. Cardiothorac. Surg. 2016, 49, 1607–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, F.; Chen, H.; Xiang, J.; Zhang, Y.; Zhou, J.; Hu, H.; Zhang, J.; Luo, X. Relationship between tumor size and disease stage in non-small cell lung cancer. BMC Cancer 2010, 10, 474. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.J.; Kim, S.R.; Kim, H.R.; Han, J.O.; Kim, Y.H.; Kim, D.K.; Park, S.I. Modern outcome and risk analysis of surgically resected occult N2 non-small cell lung cancer. Ann. Thorac. Surg. 2014, 97, 1920–1925. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, W.; Liang, H.; Yang, C.J.; D’Amico, T.; Ng, C.S.H.; Liu, C.C.; Petersen, R.H.; Rocco, G.; Brunelli, A.; et al. The Optimal Treatment for Stage IIIA-N2 Non-Small Cell Lung Cancer: A Network Meta-Analysis. Ann. Thorac. Surg. 2019, 107, 1866–1875. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age, Mean (SD), y | 59 (12.2) |
| Male, No. (%) | 35 (45.5) |
| Ever smoker, No. (%) | 29 (37.7) |
| Family History of Cancer, No. (%) Comorbidities, No. (%) Hypertension Cardiovascular Disease Chronic Obstructive Pulmonary DiseaseLiver Disease Chronic Kidney Disease Diabetes Mellitus | 14 (18.2) 24 (31.2) 8 (10.4) 6 (7.8) 6 (7.8) 4 (5.2) 10 (13.0) |
| Performance status, No. (%) ECOG 0 ECOG 1 | 39 (50.6) 38 (49.4) |
| Clinical N2, No. (%) | 35 (45.5) |
| Surgical Procedure, No. (%) Limited Resection Standard Resection | 8 (10.4) 69 (89.6) |
| Surgical Approach, No. (%) | |
| VATS | 41 (53.2) |
| Open Thoracotomy | 36 (46.8) |
| Tumor size, mean (SD), cm | 2.9 (1.0) |
| Tumor Size, No. (%) ≤3 cm 3–5 cm | 45 (58.4) 32 (41.6) |
| Histology, No. (%) Adenocarcinoma Squamous Cell Carcinoma Others | 62 (80.5) 9 (11.7) 6 (7.8) |
| Differentiation, No. (%) Well–moderate Poor Unknown | 48 (62.3) 27 (35.1) 2 (2.6) |
| CEA, Median (IQR), ng/mL | 4.0 (2.3–13.1) |
| Visceral Pleural Involvement, No. (%) | 35 (45.5) |
| Lymphovascular Permeation, No. (%) | 66 (85.7) |
| Perineural Invasion, No. (%) Number of Examined Lymph Nodes, Median (IQR) Number of Positive Lymph Nodes, Median (IQR) | 12 (15.6) 14 (9–20) 3 (1–6) |
| N2 Ratio, Median (IQR), % | 33.3 (13.8–50.0) |
| Tumor Location, No. (%) Central Location Lower Lobe Location | 44 (57.1) 31 (40.3) |
| Multiple N2 Station, No. (%) | 21 (27.3) |
| Induction therapy, No. (%) | 10 (13.0) |
| Adjuvant Therapy, No. (%) | 65 (84.4) |
| Postoperative Radiotherapy, No. (%) | 23 (29.9) |
| Parameter | Hazard Ratio (95% CI) | p-Value |
|---|---|---|
| Age (≥65 y versus <65) | 1.939 (1.050–3.582) | 0.034 |
| Gender (Male versus Female) | 1.084 (0.582–2.020) | 0.799 |
| Ever Smoker (Yes versus No) | 0.987 (0.526–1.851) | 0.967 |
| Family History of Cancer (Yes versus No) Hypertension (Yes versus No) Cardiovascular Disease (Yes versus No) Chronic Obstructive Pulmonary Disease (Yes versus No) Liver Disease (Yes versus No) Chronic Kidney Disease (Yes versus No) Diabetes Mellitus (Yes versus No) | 0.681 (0.302–1.532) 0.630 (0.310–1.279) 0.523 (0.161–1.692) 2.094 (0.741–5.916) 1.662 (0.698–3.960) 0.395 (0.054–2.877) 1.040 (0.438–2.469) | 0.352 0.201 0.279 0.163 0.251 0.359 0.930 |
| Performance Status (ECOG 1 versus ECOG 0) | 2.093 (1.133–3.867) | 0.018 |
| Clinical N2 (Yes versus Unsuspected) | 0.963 (0.525–1.767) | 0.903 |
| Limited Resection (Yes versus Anatomical) | 1.453 (0.612–3.449) | 0.397 |
| VATS (Yes versus Open Thoracotomy) | 0.429 (0.223–0.824) | 0.011 |
| Tumor Size (≤3 versus 3–5) | 0.390 (0.213–0.715) | 0.002 |
| Histology (Adenocarcinoma versus Others) | 1.442 (0.689–3.018) | 0.332 |
| Differentiation (Poor versus Others) | 0.618 (0.311–1.226) | 0.168 |
| CEA (≥3 versus <3) | 1.593 (0.729–3.482) | 0.243 |
| Visceral Pleural Involvement (Yes versus No) | 1.359 (0.743–2.486) | 0.319 |
| Lymphovascular Permeation (Yes versus No) | 1.314 (0.513–3.352) | 0.567 |
| Perineural Invasion (Yes versus No) | 0.483 (0.173–1.354) | 0.166 |
| N2 Ratio (≥40% versus <40%) | 1.167 (0.632–2.154) | 0.622 |
| Central Location (Yes versus Peripheral) | 1.061 (0.576–1.955) | 0.848 |
| Lower Lobe Location (Yes versus Upper or Middle) | 1.408 (0.757–2.619) | 0.280 |
| Multiple N2 Station (Yes versus No) | 1.056 (0.550–2.028) | 0.870 |
| Induction Therapy (Yes versus No) | 0.793 (0.281–2.236) | 0.660 |
| Adjuvant Therapy (Yes versus No) | 1.147 (0.483–2.725) | 0.756 |
| Postoperative Radiotherapy (Yes versus No) | 0.551 (0.263–1.151) | 0.113 |
| Parameter | Hazard Ratio (95% CI) | p-Value |
|---|---|---|
| Age (≥65 y versus <65) | 1.576 (0.799–3.111) | 0.190 |
| Performance Status (ECOG 1 versus ECOG 0) | 1.669 (0.878–3.173) | 0.118 |
| VATS (Yes versus Open Thoracotomy) | 0.383 (0.178–0.824) | 0.014 |
| Tumor Size (≤3 versus 3–5) | 0.373 (0.194–0.714) | 0.003 |
| Differentiation (Poor versus Others) | 0.732 (0.358–1.499) | 0.394 |
| Perineural Invasion (Yes versus No) | 0.681 (0.229–2.023) | 0.489 |
| Postoperative Radiotherapy (Yes versus No) | 1.173 (0.501–2.745) | 0.713 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-Y.; Wu, B.-R.; Chen, C.-H.; Cheng, W.-C.; Chen, W.-C.; Liao, W.-C.; Chen, C.-Y.; Hsia, T.-C.; Tu, C.-Y. Prognostic Value of Tumor Size in Resected Stage IIIA-N2 Non-Small-Cell Lung Cancer. J. Clin. Med. 2020, 9, 1307. https://doi.org/10.3390/jcm9051307
Chen C-Y, Wu B-R, Chen C-H, Cheng W-C, Chen W-C, Liao W-C, Chen C-Y, Hsia T-C, Tu C-Y. Prognostic Value of Tumor Size in Resected Stage IIIA-N2 Non-Small-Cell Lung Cancer. Journal of Clinical Medicine. 2020; 9(5):1307. https://doi.org/10.3390/jcm9051307
Chicago/Turabian StyleChen, Chih-Yu, Bing-Ru Wu, Chia-Hung Chen, Wen-Chien Cheng, Wei-Chun Chen, Wei-Chih Liao, Chih-Yi Chen, Te-Chun Hsia, and Chih-Yen Tu. 2020. "Prognostic Value of Tumor Size in Resected Stage IIIA-N2 Non-Small-Cell Lung Cancer" Journal of Clinical Medicine 9, no. 5: 1307. https://doi.org/10.3390/jcm9051307
APA StyleChen, C. -Y., Wu, B. -R., Chen, C. -H., Cheng, W. -C., Chen, W. -C., Liao, W. -C., Chen, C. -Y., Hsia, T. -C., & Tu, C. -Y. (2020). Prognostic Value of Tumor Size in Resected Stage IIIA-N2 Non-Small-Cell Lung Cancer. Journal of Clinical Medicine, 9(5), 1307. https://doi.org/10.3390/jcm9051307