Return to Sport after Anatomic and Reverse Total Shoulder Arthroplasty in Elderly Patients: A Systematic Review and Meta-Analysis

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Study Outcomes
2.3. Search Methods for Identification of Studies
2.4. Data Collection
2.5. Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
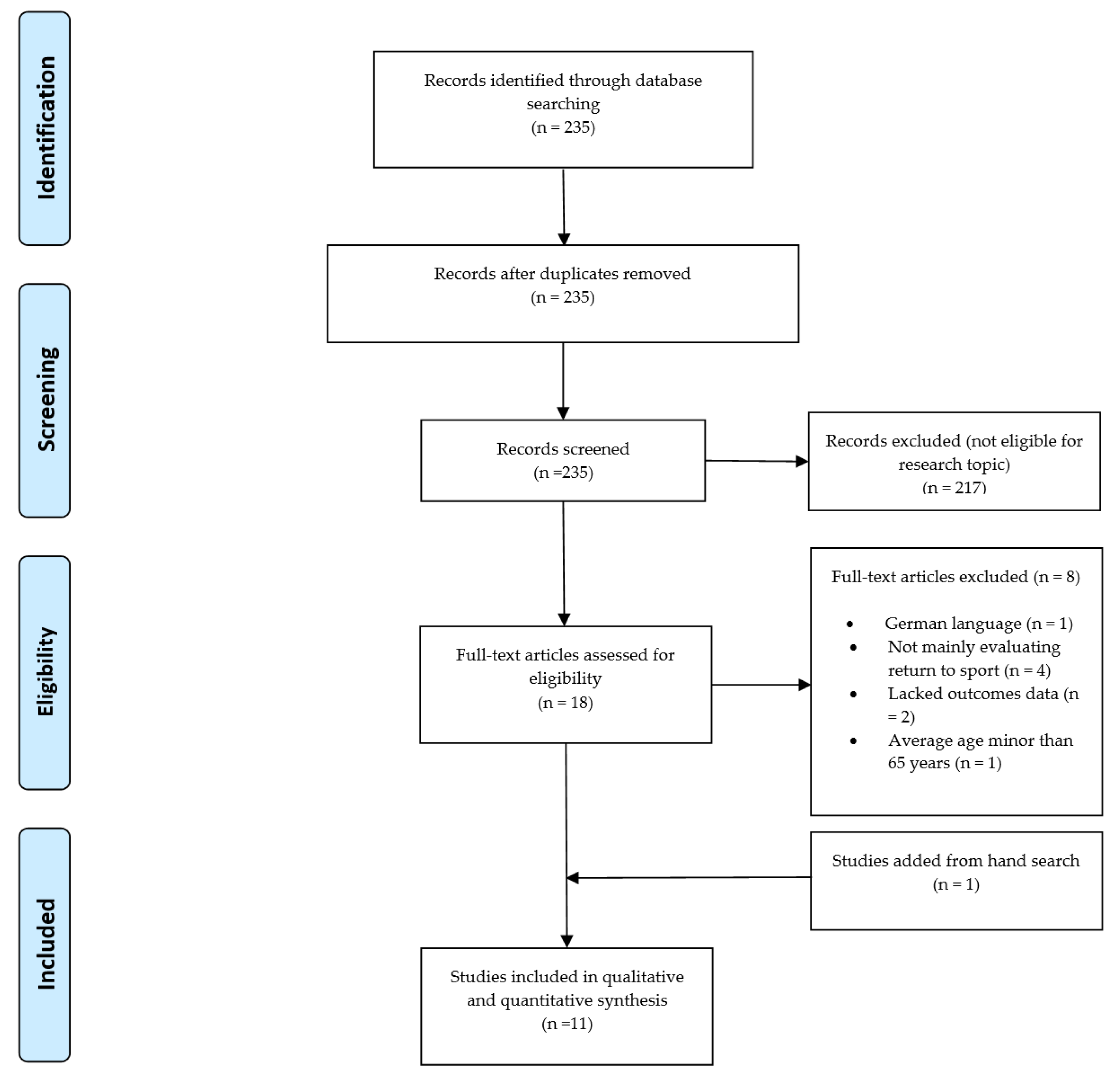
3.1. Study Selection
3.2. Study Characteristics and Demographic Details
3.3. Methodological Evaluation
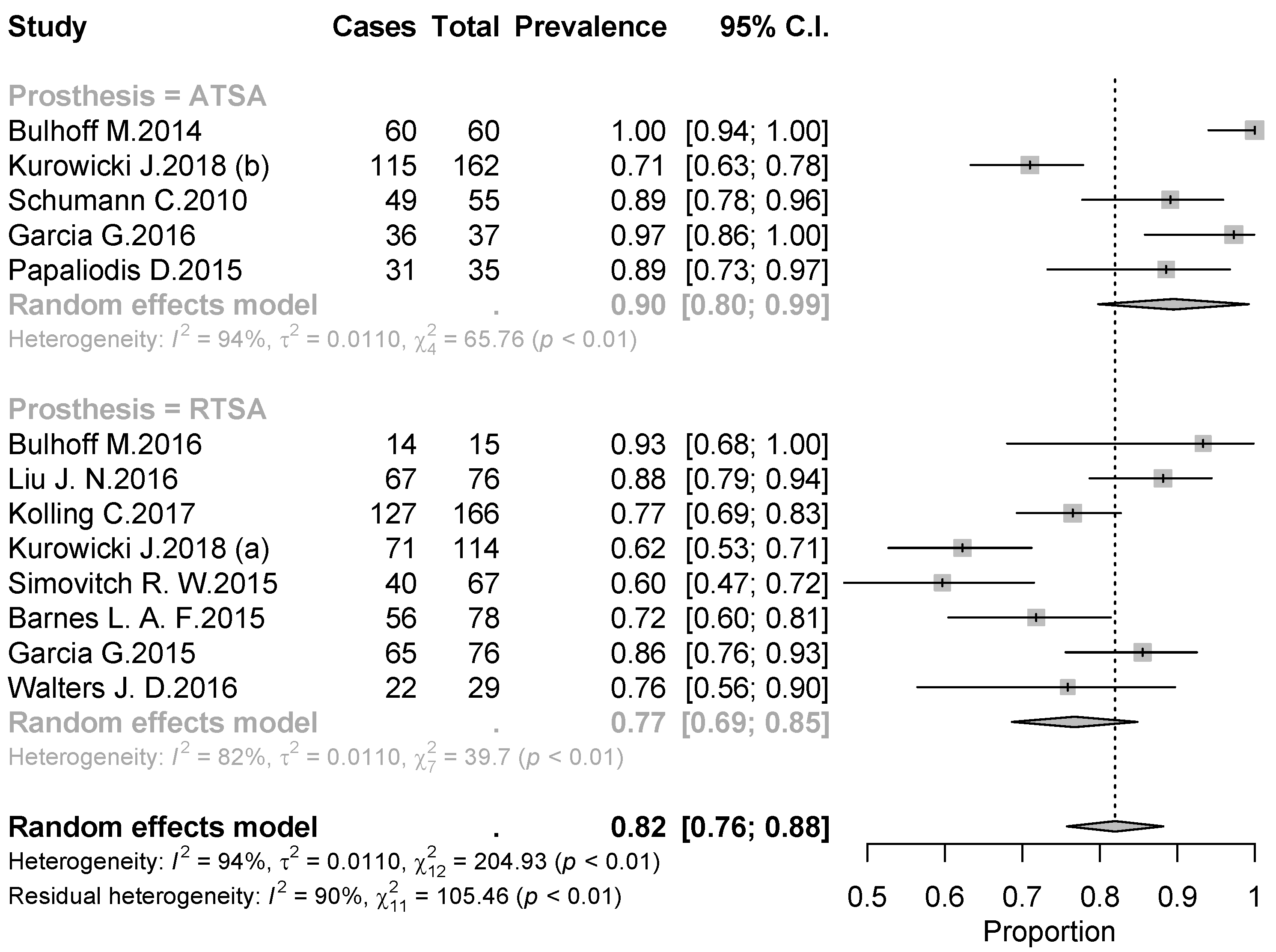
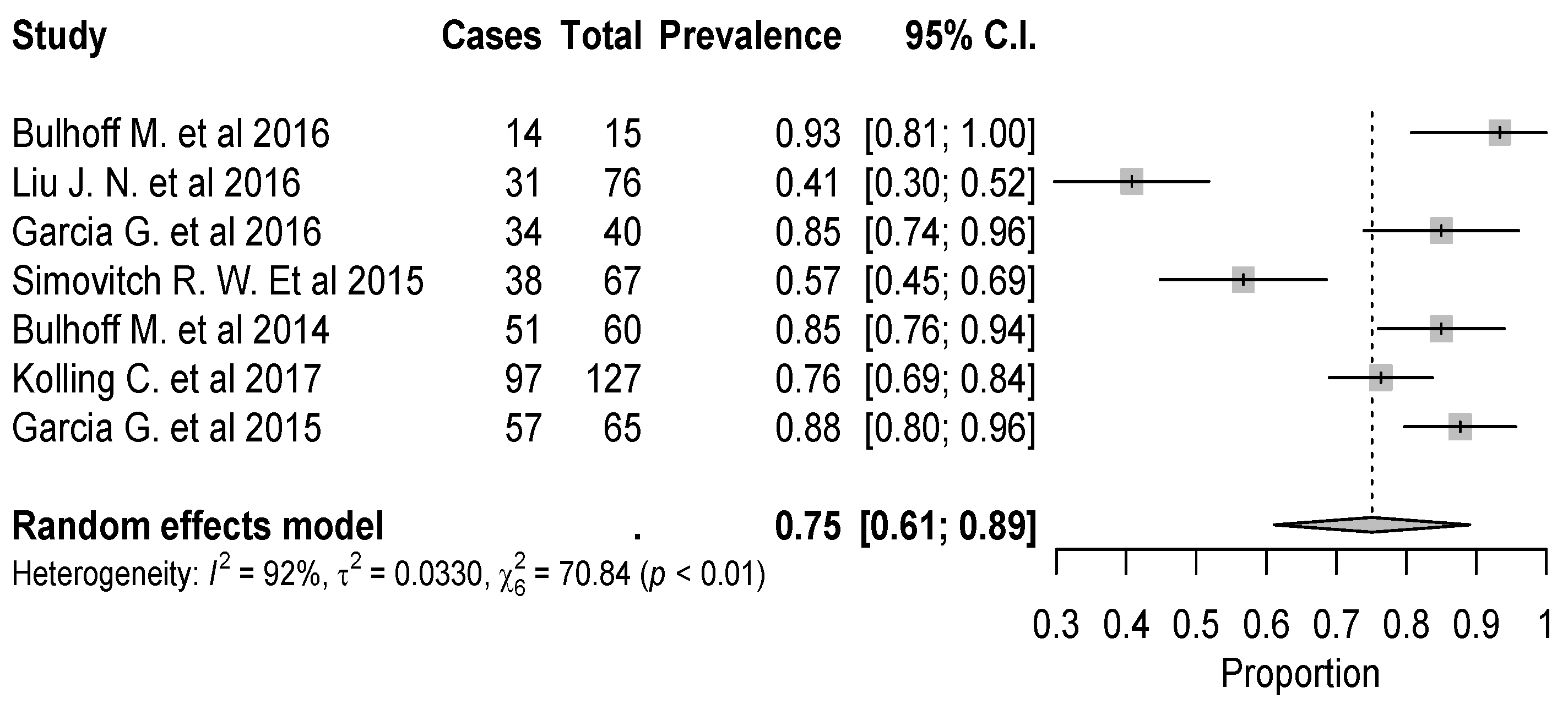
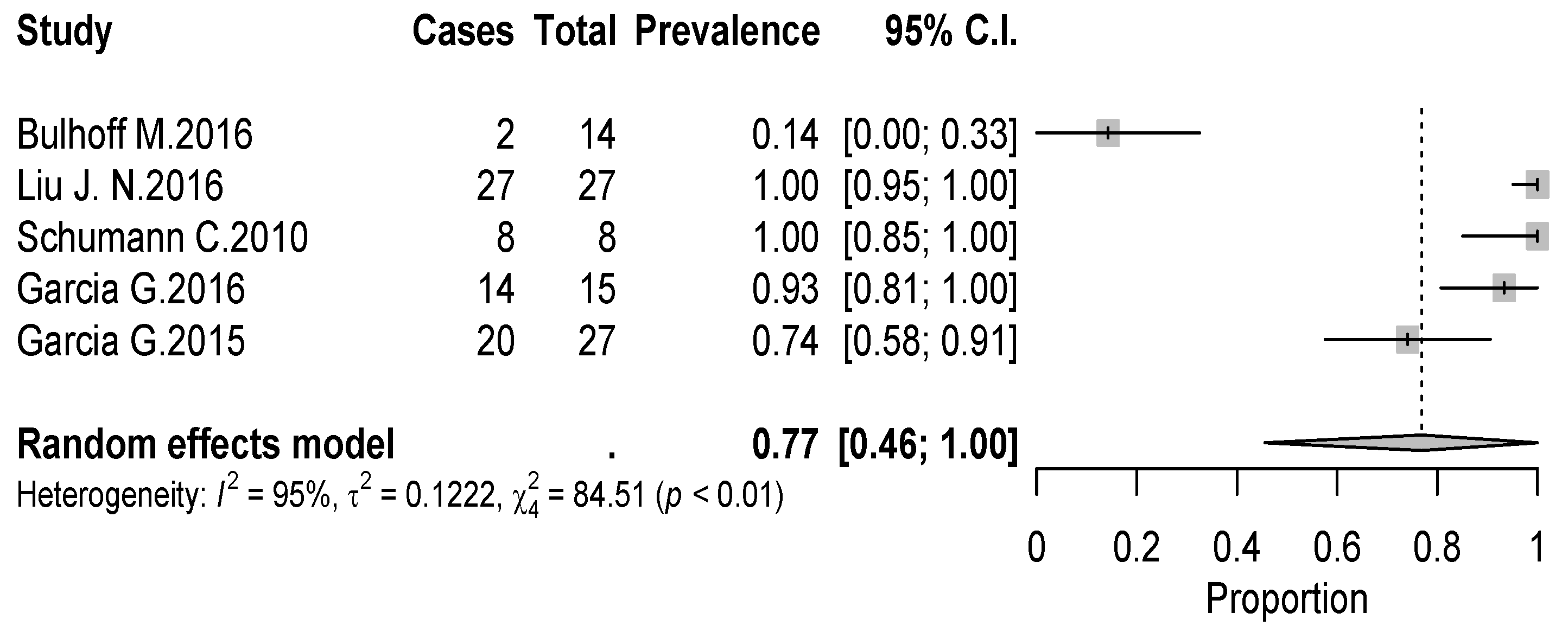
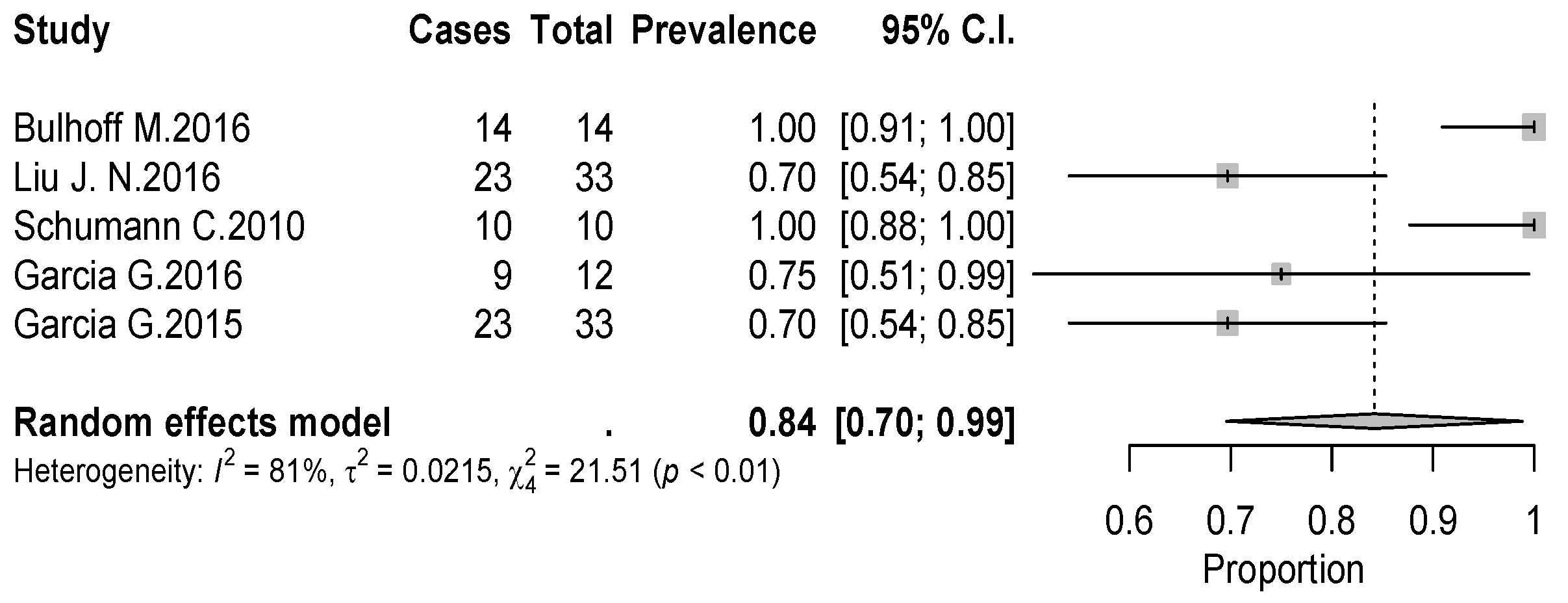
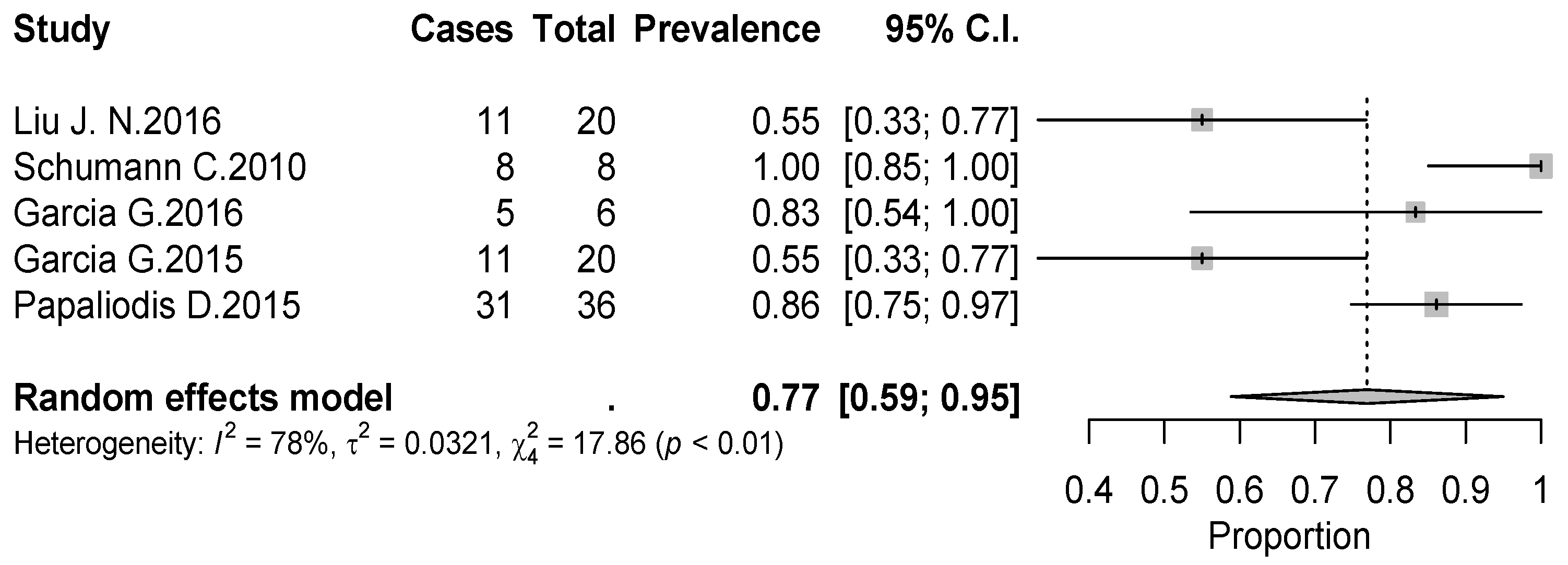
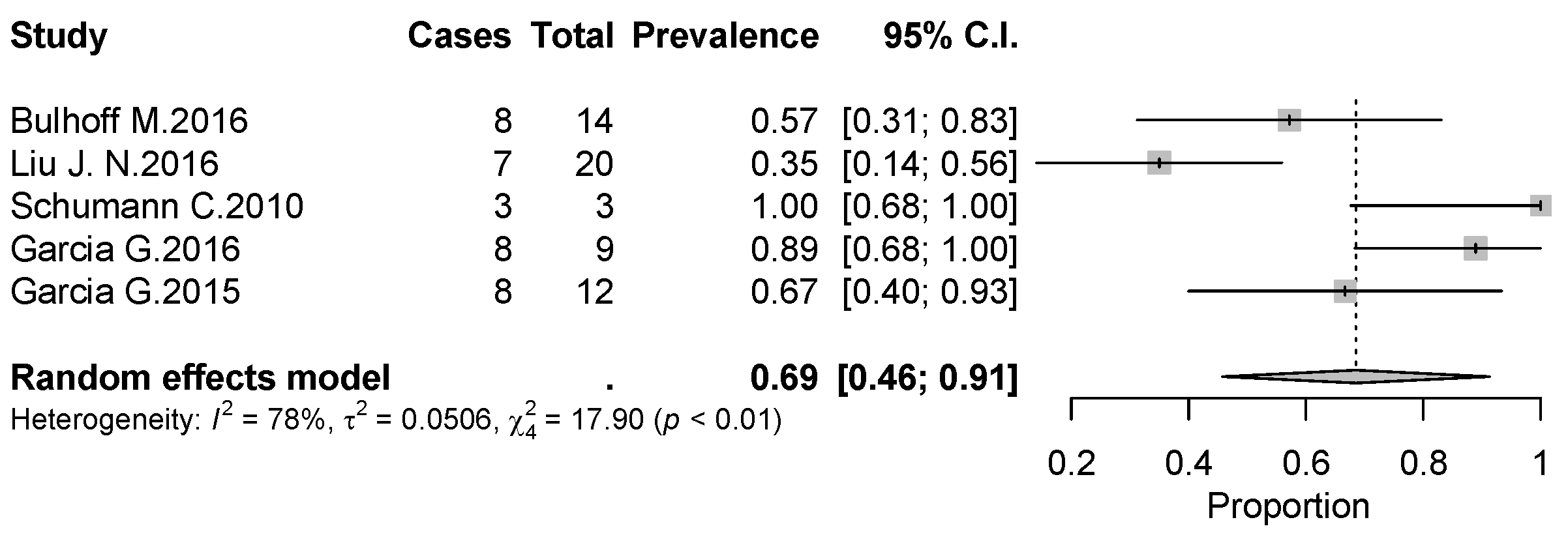
3.4. Return to Sport
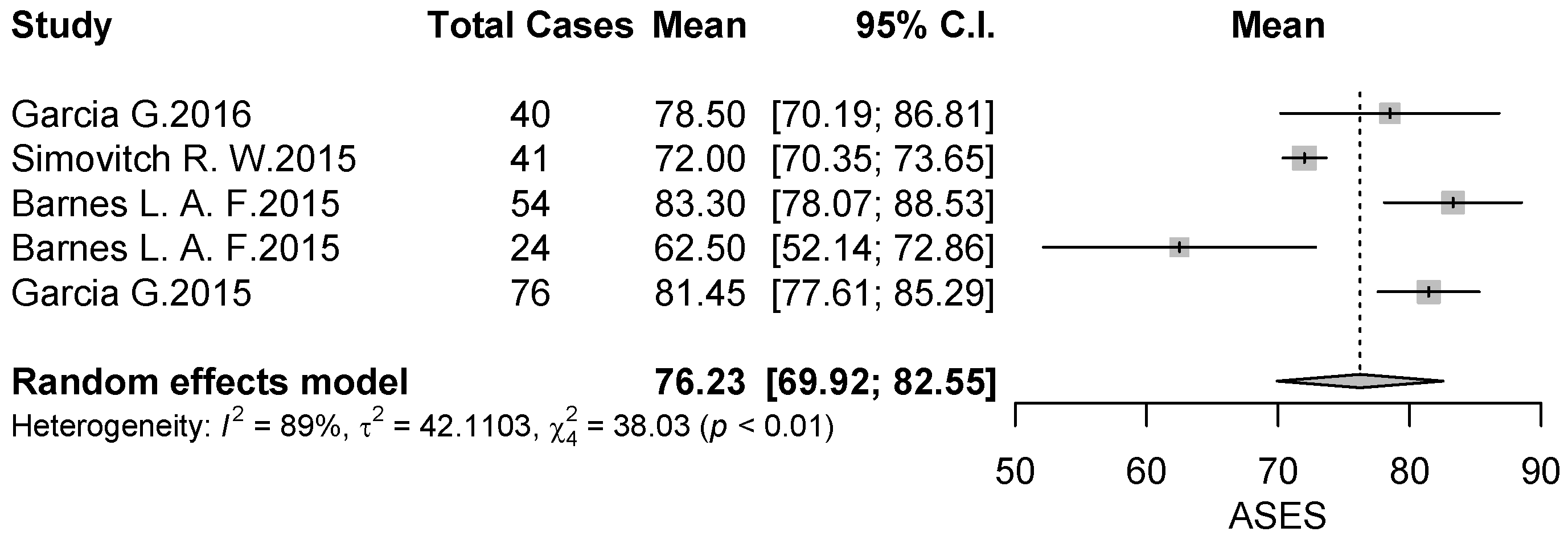
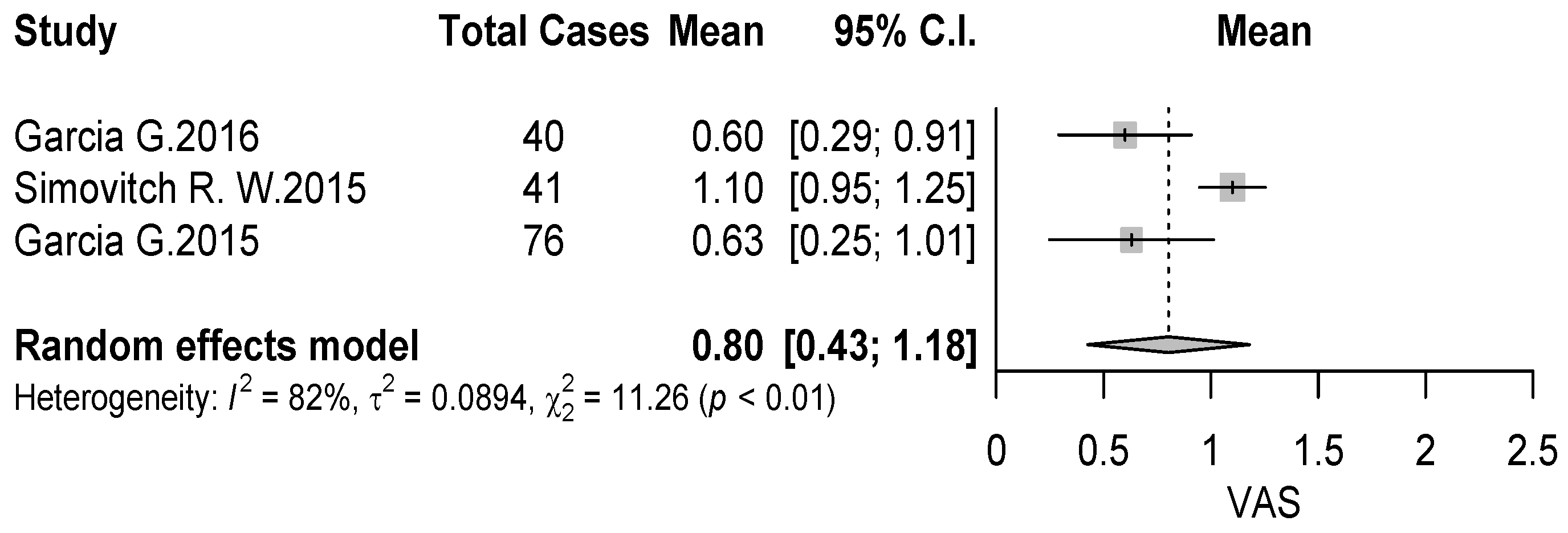
3.5. Clinical Outcome Data
3.6. Rehabilitation Protocols
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Deshmukh, A.V.; Koris, M.; Zurakowski, D.; Thornhill, T.S. Total shoulder arthroplasty: Long-term survivorship, functional outcome, and quality of life. J. Shoulder Elbow Surg. 2005, 14, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Westermann, R.W.; Pugely, A.J.; Martin, C.T.; Gao, Y.; Wolf, B.R.; Hettrich, C.M. Reverse Shoulder Arthroplasty in the United States: A Comparison of National Volume, Patient Demographics, Complications, and Surgical Indications. Iowa Orthop. J. 2015, 35, 1–7. [Google Scholar] [PubMed]
- Chalmers, P.N.; Keener, J.D. Expanding roles for reverse shoulder arthroplasty. Curr. Rev. Musculoskelet. Med. 2016, 9, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Waldstein, W.; Kolbitsch, P.; Koller, U.; Boettner, F.; Windhager, R. Sport and physical activity following unicompartmental knee arthroplasty: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 717–728. [Google Scholar] [CrossRef] [Green Version]
- Mont, M.A.; LaPorte, D.M.; Mullick, T.; Silberstein, C.E.; Hungerford, D.S. Tennis after total hip arthroplasty. Am. J. Sports Med. 1999, 27, 60–64. [Google Scholar] [CrossRef]
- Huch, K.; Müller, K.A.; Stürmer, T.; Brenner, H.; Puhl, W.; Günther, K.P. Sports activities 5 years after total knee or hip arthroplasty: The Ulm Osteoarthritis Study. Ann. Rheum. Dis. 2005, 64, 1715–1720. [Google Scholar] [CrossRef]
- Magnussen, R.A.; Mallon, W.J.; Willems, W.J.; Moorman, C.T. Long-term activity restrictions after shoulder arthroplasty: An international survey of experienced shoulder surgeons. J. Shoulder Elbow Surg. 2011, 20, 281–289. [Google Scholar] [CrossRef]
- Wolff, A.L.; Rosenzweig, L. Anatomical and biomechanical framework for shoulder arthroplasty rehabilitation. J. Hand Ther. 2017, 30, 167–174. [Google Scholar] [CrossRef]
- Bade, M.J.; Struessel, T.; Dayton, M.; Foran, J.; Kim, R.H.; Miner, T.; Wolfe, P.; Kohrt, W.M.; Dennis, D.; Stevens-Lapsley, J.E. Early High-Intensity Versus Low-Intensity Rehabilitation After Total Knee Arthroplasty: A Randomized Controlled Trial. Arthritis Care Res. (Hoboken) 2017, 69, 1360–1368. [Google Scholar] [CrossRef]
- Nassar, I.; Fahey, J.; Mitchell, D. Rapid recovery following hip and knee arthroplasty using local infiltration analgesia: Length of stay, rehabilitation protocol and cost savings. ANZ J. Surg. 2020, 90, 355–359. [Google Scholar] [CrossRef]
- Hughes, M.; Neer, C.S. Glenohumeral joint replacement and postoperative rehabilitation. Phys. Ther. 1975, 55, 850–858. [Google Scholar] [CrossRef]
- Mulieri, P.J.; Holcomb, J.O.; Dunning, P.; Pliner, M.; Bogle, R.K.; Pupello, D.; Frankle, M.A. Is a formal physical therapy program necessary after total shoulder arthroplasty for osteoarthritis? J. Shoulder Elbow Surg. 2010, 19, 570–579. [Google Scholar] [CrossRef]
- Uschok, S.; Herrmann, S.; Pauly, S.; Perka, C.; Greiner, S. Reverse shoulder arthroplasty: The role of physical therapy on the clinical outcome in the mid-term to long-term follow-up. Arch. Orthop. Trauma Surg. 2018, 138, 1347–1352. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Bülhoff, M.; Sowa, B.; Bruckner, T.; Zeifang, F.; Raiss, P. Activity levels after reverse shoulder arthroplasty. Arch. Orthop. Trauma Surg. 2016, 136, 1189–1193. [Google Scholar] [CrossRef]
- Bülhoff, M.; Sattler, P.; Bruckner, T.; Loew, M.; Zeifang, F.; Raiss, P. Do patients return to sports and work after total shoulder replacement surgery? Am. J. Sports Med. 2015, 43, 423–427. [Google Scholar] [CrossRef]
- Liu, J.N.; Garcia, G.H.; Mahony, G.; Wu, H.H.; Dines, D.M.; Warren, R.F.; Gulotta, L.V. Sports after shoulder arthroplasty: A comparative analysis of hemiarthroplasty and reverse total shoulder replacement. J. Shoulder Elbow Surg. 2016, 25, 920–926. [Google Scholar] [CrossRef]
- Garcia, G.H.; Liu, J.N.; Mahony, G.T.; Sinatro, A.; Wu, H.H.; Craig, E.V.; Warren, R.F.; Dines, D.M.; Gulotta, L.V. Hemiarthroplasty Versus Total Shoulder Arthroplasty for Shoulder Osteoarthritis: A Matched Comparison of Return to Sports. Am. J. Sports Med. 2016, 44, 1417–1422. [Google Scholar] [CrossRef]
- Garcia, G.H.; Taylor, S.A.; DePalma, B.J.; Mahony, G.T.; Grawe, B.M.; Nguyen, J.; Dines, J.S.; Dines, D.M.; Warren, R.F.; Craig, E.V.; et al. Patient Activity Levels After Reverse Total Shoulder Arthroplasty: What Are Patients Doing? Am. J. Sports Med. 2015, 43, 2816–2821. [Google Scholar] [CrossRef]
- Schumann, K.; Flury, M.P.; Schwyzer, H.K.; Simmen, B.R.; Drerup, S.; Goldhahn, J. Sports activity after anatomical total shoulder arthroplasty. Am. J. Sports Med. 2010, 38, 2097–2105. [Google Scholar] [CrossRef]
- Simovitch, R.W.; Gerard, B.K.; Brees, J.A.; Fullick, R.; Kearse, J.C. Outcomes of reverse total shoulder arthroplasty in a senior athletic population. J. Shoulder Elbow Surg. 2015, 24, 1481–1485. [Google Scholar] [CrossRef]
- Fink Barnes, L.A.; Grantham, W.J.; Meadows, M.C.; Bigliani, L.U.; Levine, W.N.; Ahmad, C.S. Sports activity after reverse total shoulder arthroplasty with minimum 2-year follow-up. Am. J. Orthop. (Belle Mead NJ) 2015, 44, 68–72. [Google Scholar]
- Papaliodis, D.; Richardson, N.; Tartaglione, J.; Roberts, T.; Whipple, R.; Zanaros, G. Impact of Total Shoulder Arthroplasty on Golfing Activity. Clin. J. Sport Med. 2015, 25, 338–340. [Google Scholar] [CrossRef]
- Kolling, C.; Borovac, M.; Audigé, L.; Mueller, A.M.; Schwyzer, H.K. Return to sports after reverse shoulder arthroplasty-the Swiss perspective. Int. Orthop. 2018, 42, 1129–1135. [Google Scholar] [CrossRef]
- Kurowicki, J.; Rosas, S.; Law, T.Y.; Levy, J.C. Participation in Work and Sport Following Reverse and Total Shoulder Arthroplasty. Am. J. Orthop. (Belle Mead NJ) 2018, 47. [Google Scholar] [CrossRef] [Green Version]
- Flurin, P.H.; Roche, C.P.; Wright, T.W.; Marczuk, Y.; Zuckerman, J.D. A Comparison and Correlation of Clinical Outcome Metrics in Anatomic and Reverse Total Shoulder Arthroplasty. Bull. Hosp. Jt. Dis. 2015, 73 (Suppl. 1), S118–S123. [Google Scholar]
- Eichinger, J.K.; Miller, L.R.; Hartshorn, T.; Li, X.; Warner, J.J.; Higgins, L.D. Evaluation of satisfaction and durability after hemiarthroplasty and total shoulder arthroplasty in a cohort of patients aged 50 years or younger: An analysis of discordance of patient satisfaction and implant survival. J. Shoulder Elbow Surg. 2016, 25, 772–780. [Google Scholar] [CrossRef]
- Golant, A.; Christoforou, D.; Zuckerman, J.D.; Kwon, Y.W. Return to sports after shoulder arthroplasty: A survey of surgeons’ preferences. J. Shoulder Elbow Surg. 2012, 21, 554–560. [Google Scholar] [CrossRef]
- Healy, W.L.; Iorio, R.; Lemos, M.J. Athletic activity after joint replacement. Am. J. Sports Med. 2001, 29, 377–388. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year of Publication | Study Design | LOE | N° of Shoulders (N° of Patients) | Dominant/Not Dominant | Mean Age (Years) | Type of Implant | Mean Follow-Up (Years) | MINORS Score |
|---|---|---|---|---|---|---|---|---|---|
| Bulhoff et al. [17] | 2015 | CS | IV | 170 (154) | 103/51 | 72 | ATSA | 6.2 | 7/16 |
| Bulhoff et al. [16] | 2016 | CS | IV | 38 (38) | 29/9 | Group A: 76.2; Group B: 78.4 | RTSA | 4.8 | 14/24 |
| Liu et al. [18] | 2016 | RS | III | 102 (102) | 58/44 | 72.3 | RTSA | 2.6 | 14/24 |
| Kolling et al. [25] | 2017 | RS | III | 271 (271) | 203/68 | 77.1 | RTSA | 2.9 | 7/16 |
| Schumann et al. [21] | 2010 | CS | IV | 100 (100) | 60/40 | 66.2 | ATSA | 2.8 | 8/16 |
| Garcia et al. [19] | 2016 | PS | III | 40 (40) | 26/14 | 66.3 | ATSA | 5.1 | 9/16 |
| Papaliodis et al. [24] | 2015 | CS | IV | 36 (35) | NR | 67.2 | ATSA | 3.2 | 8/16 |
| Simovitch et al. [22] | 2015 | CS | IV | 67 (67) | NR | 73 | RTSA | 3.6 | 10/16 |
| Barnes et al. [23] | 2015 | RS | III | 78 (78) | 48/30 | 75.3 | RTSA | 4.8 | 11/16 |
| Garcia et al. [20] | 2015 | RS | III | 76 (76) | 46/30 | 74.8 | RTSA | 2.6 | 16/24 |
| Kurowicki et al. [26] | 2018 | RS | IV | 276 (276) | NR | RTSA: 75 ATSA: 69 | RTSA ATSA | 2.4 | 14/24 |
| Study | Sports | Number of Patient Practicing Sport (%) | Number of Evaluated Patients | Rate of Return to Sport for Single Sport (%) | Overall Rate of Return to Sport (%) |
|---|---|---|---|---|---|
| Schumann et al. [21] | Swimming | 10 (20.4%) | 55 | NR | 49 (89%) |
| Golf | 8 (16.3%) | ||||
| Cycling | 8 (16.3%) | ||||
| Fitness | 8 (16.3%) | ||||
| Other | 21 (30.7%) | ||||
| Papaliodis et al. [24] | Golf | 35 (100%) | 35 | NR | 31 (88.57%) |
| Garcia et al., 2015 [20] | Fitness | 27 | 76 (some patients practiced more than 1 sport) | 22 (81.5%) | 65 (85.5%) |
| Swimming | 33 | 22 (66.7%) | |||
| Golf | 20 | 10 (50%) | |||
| Cycling | 10 | 5 (50%) | |||
| Bulhoff et al., 2015 [17] | Swimming | 60 (57%) | 105 | 60 (57%) | 60 (100%) |
| Fitness including lower limb | 42 (27%) | ||||
| Skiing | 31 (30%) | ||||
| Gardening | 29 (28%) | ||||
| Bowling/skittles | 18 (17%) | ||||
| Tennis | 15 (14%) | ||||
| Handball | 6 (4%) | ||||
| Athletics | 4 (3%) | ||||
| Volleyball | 3 (2%) | ||||
| Golf | 2 (1%) | ||||
| Other | 26 (25%) | ||||
| Bulhoff et al., 2016 [16] | Swimming | 15 (71%) | 22 | 14 (100%) | 14 (93%) |
| Fitness including lower limb | 8 (57%) | ||||
| Skiing | 7 (50%) | ||||
| Gardening | 8 (57%) | ||||
| Bowling | 7 (50%) | ||||
| Tennis | 8 (57%) | ||||
| Handball | 2 (14%) | ||||
| Kolling et al. [25] | Calisthenics | 166 | 305 | 28 (17%) | 127 (77%) |
| Hiking | 28 (17%) | ||||
| Swimming | 26 (16%) | ||||
| Alpine skiing | 13 (8%) | ||||
| Tennis | 12 (7%) | ||||
| Others | 58 (35%) | ||||
| Liu et al. [18] | Single tennis | 12 (12.2%) | 102 | 4 (33%) | 87 (85.9%) |
| Double tennis | 18 (18.3%) | 3 (16.6%) | |||
| Baseball | 1 (1.02%) | 1 (100%) | |||
| Swimming | 33 (33.66%) | 23 (70%) | |||
| Fitness | 27 (27.54%) | 27 (100%) | |||
| Golf | 20 (20.4%) | 11 (55%) | |||
| Cycling | 12 (12.2%) | 8 (67%) | |||
| Fishing | 4 (4.8%) | 1 (25%) | |||
| Rowing | 1 (1.02%) | 1 (100%) | |||
| Running | 7 (7.14%) | 5 (71.4%) | |||
| Skiing | 7 (7.14%) | 2 (29%) | |||
| Dancing | 2 (2.04%) | 1 (50%) | |||
| Horseback riding | 2 (2.04%) | 1 (50%) | |||
| Basketball | 1 (1.02%) | 1 (100%) | |||
| Simovitch et al. [22] | Golf | 67 (26%) | 255 | 50 (75%) | 64 (95%) |
| Swimming | 19 (29%) | ||||
| Water aerobics | 16 (24%) | ||||
| Deep sea fishing | 14 (21%) | ||||
| Firearm sports | 14 (21%) | ||||
| Weight lifting | 12 (18%) | ||||
| Softball | 7 (11%) | ||||
| Tennis | 7 (11%) | ||||
| Table tennis | 5 (7%) | ||||
| Scuba diving | 5 (7%) | ||||
| Racquetball | 3 (5%) | ||||
| Surfing | 1 (2%) | ||||
| Water skiing | 1 (2%) | ||||
| Garcia 2016 et al. [19] | Golf | 6 (8.3%) | 72 | 5 (83.3%) | 65 (90.27%) |
| Swimming | 12 (16%) | 9 (75%) | |||
| Baseball | 1 (1.4%) | 1 (100%) | |||
| Basketball | 1 (1.4%) | 1 (100%) | |||
| Nature sports | 7 (9.7%) | 7 (100%) | |||
| Fitness | 15 (21%) | 14 (93%) | |||
| Single tennis | 5 (7%) | 4 (80%) | |||
| Running | 14 (19.4%) | 13 (92.9%) | |||
| Cycling | 5 (7%) | 5 (100%) | |||
| Softball | 2 (2.7%) | 2 (100%) | |||
| Double tennis | 4 (5.5%) | 4 (100%) | |||
| Barnes et al. [23] | High intensity activities (hunting, golf, skiing …) | NR | 78 | 18 (23.1%) | 100% |
| Moderate intensity activities (swimming, bowling …) | 38 (48.7%) | ||||
| Low intensity activities (riding bike, walking, dancing …) | 22 (28.2%) | ||||
| Kirowicki et al. [26] | Golf | RTSA: 16 (22%) ATSA: 31 (27%) | RTSA: 71 ATSA 115 | NR | RTSA 71/114 (62%); ATSA 115/162 (70%) |
| Swimming | RTSA: 13 (18%) ATSA: 19 (16%) | ||||
| Walking | RTSA: 16 (22%) ATSA: 18 (15%) | ||||
| Gym exercises | RTSA: 8 (11%) ATSA: 24 (20%) | ||||
| Racquet sport | RTSA: 4 (5%) ATSA: 13 (11%) | ||||
| Group fitness | RTSA: 5 (7%) ATSA: 10 (8%) | ||||
| Fishing and target shooting | RTSA: 5 (7%) ATSA: 4 (3%) | ||||
| Adventure sport | RTSA: 1 (1%) ATSA: 9 (8%) |
| Authors | Implant | Outcomes | Complication (Number) | Main Conclusion | |
|---|---|---|---|---|---|
| Preoperative | Postoperative | ||||
| Bulhoff et al. [17] | ATSA | NR | NR |
| |
| Bulhoff et al. [16] | RTSA | NR | aseptic loosening of glenoid component (1), dislocation (2) | Patients with glenohumeral osteoarthritis and rotator cuff disease being active prior to RSA surgery are able to successfully return to their level of sports participation afterwards. | |
| Liu et al. [18] | RTSA | ASES SCORE (overall mean change) +39 | None | Despite traditional sport restrictions placed on RTSA, patients undergoing RTSA can return to sports at rates higher than those undergoing HHA, with fewer postoperative complaints. | |
| VAS (overall mean reduction) −5.64 | |||||
| Kolling et al. [25] | RTSA | NR | NR |
| |
| Schumann et al. [21] | ATSA | CONSTANT SCORE (mean ± SD) | NR |
| |
| NR | GI: 70.8 ± 13.8; GII: 77.2 ± 10.6; GIII: 69.3 ± 9.7 | ||||
| SF-36 (mean ± SD) | |||||
| NR | Physical component: GI 41.0 ± 11.2; GII: 46.2 ± 9.0; GIII: 42.2 ± 10.6; Mental component GI: 55.6 ± 9.3; GII 55.7 ± 6.4; GIII: 47.7 ± 12.9 | ||||
| DASH SCORE (mean ± SD) | |||||
| NR | GI: 76.6 ± 19.3; GII: 83.4 ± 12.7; GIII: 69.6 ± 18.6 | ||||
| SPADI SCORE (mean ± SD) | |||||
| NR | GI: 78.6 ± 20.5; GII: 83.7 ± 16.5; GIII: 68.7 ± 19.2 | ||||
| Garcia et al. [19] | ATSA | ASES SCORE (mean) | NR |
| |
| 34.0 | 78.5 | ||||
| VAS (mean) | |||||
| 6.1 | 0.6 | ||||
| Papaliodis et al. [24] | ATSA | VAS (mean average improvement) 4.3 | NR |
| |
| Simovitch et al. [22] | RTSA | CONSTANT SCORE (mean ± SD) | type II acromion stress fracture (1); postoperative infection (1), postoperative dislocation (1) |
| |
| 25 ± 1.9 | 84 ± 1.7 | ||||
| ASES SCORE (mean ± SD) | |||||
| 31 ± 1.9 | 72 ± 4.5 | ||||
| ROM (mean ± SD) | |||||
| Flexion: 78 ± 16; Abduction: 67 ± 14.6; External rotation: 26 ± 5.2 | Flexion: 152 ± 12; Abduction: 148 ± 11.6; External rotation: 44 ± 5.7 | ||||
| VAS (mean ± SD) | |||||
| 7.2 ± 0.5 | 1.1 ± 0.5 | ||||
| SSV (mean ± SD) | |||||
| 27 ± 4.3 | 90 ± 4 | ||||
| Barnes et al. [23] | RTSA | ASES SCORE (mean) | dislocation (3), aseptic loosening (1); dissociated glenosphere baseplates (1); deep infections (2); superficial infection (1) | RTSA results in good pain relief and motion, with a variety of postoperative overhead activities enjoyed by some patients who are not limited by comorbidities. | |
| NR | 77.5 | ||||
| ROM (mean) | |||||
| NR | active forward elevation: 140°, active external rotation: 48°, active internal rotation: S1 | ||||
| VAS (mean) | |||||
| NR | 2.3 | ||||
| Kurowicki et al. [26] | RTSA ATSA | ASES SCORE (mean) | NR |
| |
| NR | RTSA: 77.14 ATSA: 83.03 | ||||
| Garcia et al. [20] | RTSA | ASES SCORE (mean ± SD) | None |
| |
| 34.3 ± 17.2 | 81.45 ± 17.1 | ||||
| VAS (mean ± SD) | |||||
| 6.57 ± 2.4 | 0.63 ± 1.7 | ||||
| Authors | Rehabilitative Protocols | Surgical Approach |
|---|---|---|
| Bulhoff et al. [17] | 1. Abduction pillow (20°) and internal rotation (20°) for the first 4 weeks. 2. Day 1 to 6th week: daily actively assisted exercise with a physiotherapist. 3. From 6th week: active and free range of motion. | Deltopectoral approach with subscapularis repair |
| Bulhoff et al. [16] | NR | Deltopectoral approach with subscapularis repair |
| Liu et al. [18] | 1. Sling immobilization for the first 4 weeks. 2. From 2nd week: passive ROM at 2 weeks. 3. From 6th week: active ROM. 4. From 12th week: strengthening exercises and prior recreational activities and work were encouraged. Restriction: avoid contact sports | NR |
| Kolling et al. [25] | 1. Sling immobilization during the night for the first 4 weeks. 2. From day 1 to 2nd week: passive motion with only limited external rotation movements to protect the reinserted subscapularis tendon. 3. From 2nd to 5th week: active mobilization and water therapy to gain shoulder strength and coordination. 4. After 12th week: resume any prior sports activities including non-contact sports. | Deltopectoral approach with subscapularis repair |
| Schumann et al. [21] | NR | Deltopectoral approach with subscapularis repair |
| Garcia et al. [19] | NR | Deltopectoral approach |
| Papaliodis et al. [24] | NR | NR |
| Simovitch et al. [22] | 1. Abduction sling for the first 4 weeks. 2. From day 1 to 4th week: passive ROM and isometric exercises. 3. From 6th week: active ROM. 4. From 12th week: strengthening exercises. 5. From 16th week: return to sports. | Deltopectoral approach without subscapularis repair |
| Barnes et al. [23] | 1. Sling immobilization for the first 4 weeks (only wrist and elbow motion allowed) 2. From 4th week: active shoulder ROM. 3. From 8th week: strengthening exercises. | Deltopectoral approach with subscapularis repair |
| Garcia et al. [20] | NR Restriction: avoid contact sports. | NR |
| Kirowicki et al. [26] | NR | NR |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papalia, R.; Ciuffreda, M.; Albo, E.; De Andreis, C.; Diaz Balzani, L.A.; Alifano, A.M.; Fossati, C.; Macaluso, A.; Borzuola, R.; De Vincentis, A.; et al. Return to Sport after Anatomic and Reverse Total Shoulder Arthroplasty in Elderly Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1576. https://doi.org/10.3390/jcm9051576
Papalia R, Ciuffreda M, Albo E, De Andreis C, Diaz Balzani LA, Alifano AM, Fossati C, Macaluso A, Borzuola R, De Vincentis A, et al. Return to Sport after Anatomic and Reverse Total Shoulder Arthroplasty in Elderly Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(5):1576. https://doi.org/10.3390/jcm9051576
Chicago/Turabian StylePapalia, Rocco, Mauro Ciuffreda, Erika Albo, Chiara De Andreis, Lorenzo Alirio Diaz Balzani, Anna Maria Alifano, Chiara Fossati, Andrea Macaluso, Riccardo Borzuola, Antonio De Vincentis, and et al. 2020. "Return to Sport after Anatomic and Reverse Total Shoulder Arthroplasty in Elderly Patients: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 5: 1576. https://doi.org/10.3390/jcm9051576
APA StylePapalia, R., Ciuffreda, M., Albo, E., De Andreis, C., Diaz Balzani, L. A., Alifano, A. M., Fossati, C., Macaluso, A., Borzuola, R., De Vincentis, A., & Denaro, V. (2020). Return to Sport after Anatomic and Reverse Total Shoulder Arthroplasty in Elderly Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 9(5), 1576. https://doi.org/10.3390/jcm9051576