The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation † †

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
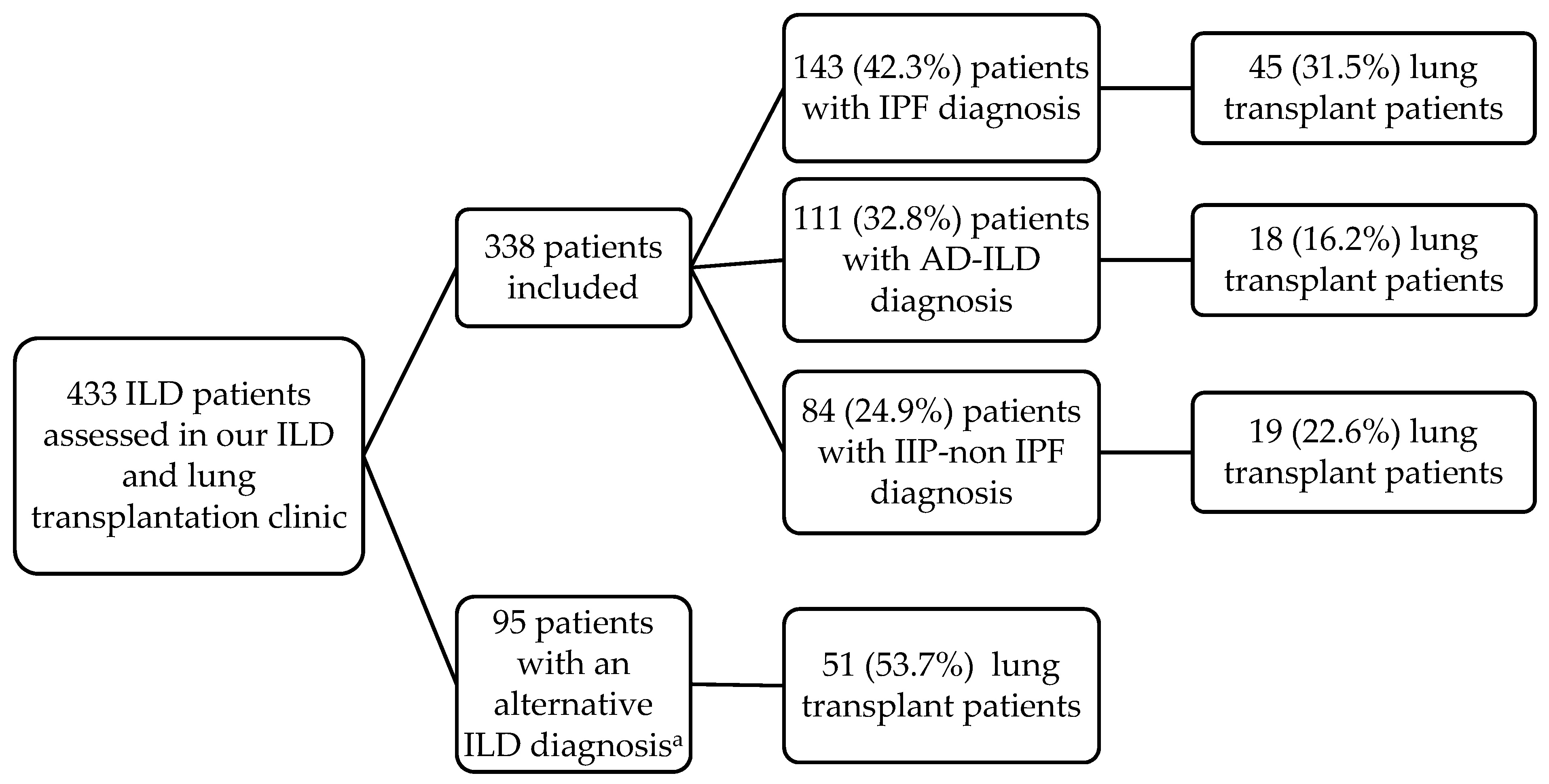
2.1. Patients
2.2. Methods
2.3. Descriptive Statistical Analysis
3. Results
3.1. Characteristics and Categories of ILD Patients According to Their Diagnosis
3.2. Spectrum of AD-ILD Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef]
- Cottin, V.; Hirani, N.A.; Hotchkin, D.L.; Nambiar, A.M.; Ogura, T.; Otaola, M.; Skowasch, D.; Park, J.S.; Poonyagariyagorn, H.K.; Wuyts, W.; et al. Presentation, diagnosis and clinical course of the spectrum of progressive-fibrosing interstitial lung diseases. Eur. Respir. Rev. 2018, 27, 180076. [Google Scholar] [CrossRef] [Green Version]
- Davidson, A.; Diamond, B. Autoimmune diseases. N. Engl. J. Med. 2001, 345, 340–350. [Google Scholar] [CrossRef]
- Goldblatt, F.; O’Neill, S.G. Clinical aspects of autoimmune rheumatic diseases. Lancet 2013, 382, 797–808. [Google Scholar] [CrossRef]
- Sociedad Española de Reumatología. Tratado SER de Diagnóstico y Tratamiento de Enfermedades Autoinmunes Sistémicas, 1st ed.; Elsevier: Madrid, Spain, 2018. [Google Scholar]
- Fischer, A.; du Bois, R. Interstitial lung disease in connective tissue disorders. Lancet 2012, 380, 689–698. [Google Scholar] [CrossRef]
- Mathai, S.C.; Danoff, S.K. Management of interstitial lung disease associated with connective tissue disease. BMJ 2016, 352, h6819. [Google Scholar] [CrossRef] [PubMed]
- Walker, U.A.; Tyndall, A.; Czirják, L.; Denton, C.; Farge-Bancel, D.; Kowal-Bielecka, O.; Müller-Ladner, U.; Bocelli-Tyndall, C.; Matucci-Cerinic, M. Clinical risk assessment of organ manifestations in systemic sclerosis: A report from the EULAR scleroderma trials and research group database. Ann. Rheum. Dis. 2007, 66, 754–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morisset, J.; Johnson, C.; Rich, E.; Collard, H.R.; Lee, J.S. Management of myositis-related interstitial lung disease. Chest 2016, 150, 1118–1128. [Google Scholar] [CrossRef]
- Marigliano, B.; Soriano, A.; Margiotta, D.; Vadacca, M.; Afeltra, A. Lung involvement in connective tissue diseases: A comprehensive review and a focus on rheumatoid arthritis. Autoimmun. Rev. 2013, 12, 1076–1084. [Google Scholar] [CrossRef]
- Atzeni, F.; Gerardi, M.C.; Barilaro, G.; Masala, I.F.; Benucci, M.; Sarzi-Puttini, P. Interstitial lung disease in systemic autoimmune rheumatic diseases: A comprehensive review. Expert Rev. Clin. Immunol. 2018, 14, 69–82. [Google Scholar] [CrossRef]
- Mittoo, S.; Gelber, A.C.; Christopher-Stine, L.; Horton, M.R.; Lechtzin, N.; Danoff, S.K. Ascertainment of collagen vascular disease in patients presenting with interstitial lung disease. Respir. Med. 2009, 103, 1152–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, A.; Antoniou, K.M.; Brown, K.K.; Cadranel, J.; Corte, T.J.; du Bois, R.M.; Lee, J.S.; Leslie, K.O.; Lynch, D.A.; Matteson, E.L.; et al. An official European Respiratory Society/American Thoracic Society research statement: Interstitial pneumonia with autoimmune features. Eur. Respir. J. 2015, 46, 976–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, B.; Raghu, G. Interstitial pneumonia with autoimmune features: The new consensus-based definition for this cohort of patients should be broadened. Eur. Respir. J. 2016, 47, 1293–1295. [Google Scholar] [CrossRef] [PubMed]
- Cavagna, L.; Gonzalez Gay, M.A.; Allanore, Y.; Matucci-Cerinic, M. Interstitial pneumonia with autoimmune features: A new classification still on the move. Eur. Respir. Rev. 2018, 27, 180047. [Google Scholar] [CrossRef] [PubMed]
- Sambataro, G.; Sambataro, D.; Torrisi, S.E.; Vancheri, A.; Pavone, M.; Rosso, R.; Schisano, M.; Crimi, C.; Pignataro, F.; Fischer, A.; et al. State of the art in interstitial pneumonia with autoimmune features: A systematic review on retrospective studies and suggestions for further advances. Eur. Respir. Rev. 2018, 27, 170139. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Kim, D.S.; Park, I.N.; Jang, S.J.; Kitaichi, M.; Nicholson, A.G.; Colby, T.V. Prognosis of fibrotic interstitial pneumonia: Idiopathic versus collagen vascular disease-related subtypes. Am. J. Respir. Crit. Care Med. 2007, 175, 705–711. [Google Scholar] [CrossRef]
- Navaratnam, V.; Ali, N.; Smith, C.J.; McKeever, T.; Fogarty, A.; Hubbard, R.B. Does the presence of connective tissue disease modify survival in patients with pulmonary fibrosis? Respir. Med. 2011, 105, 1925–1930. [Google Scholar] [CrossRef] [Green Version]
- Castelino, F.V.; Goldberg, H.; Dellaripa, P.F. The impact of rheumatological evaluation in the management of patients with interstitial lung disease. Rheumatology 2011, 50, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.F.; Flaherty, K.R.; Lasky, J.A.; et al. An Official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef]
- Furini, F.; Carnevale, A.; Casoni, G.L.; Guerrini, G.; Cavagna, L.; Govoni, M.; Sciré, C.A. The role of the multidisciplinary evaluation of interstitial lung diseases: Systematic literature review of the current evidence and future perspectives. Front. Med. 2019, 6, 246. [Google Scholar] [CrossRef] [Green Version]
- Mikolasch, T.A.; Garthwaite, H.S.; Porter, J.C. Update in diagnosis and management of interstitial lung disease. Clin. Med. 2017, 17, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Weill, D.; Benden, C.; Corris, P.A.; Dark, J.H.; Davis, R.D.; Keshavjee, S.; Lederer, D.J.; Mulligan, M.J.; Patterson, G.A.; Singer, L.G.; et al. A consensus document for the selection of lung transplant candidates: 2014--an update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2015, 34, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O. III.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef]
- Lundberg, I.E.; Tjärnlund, A.; Bottai, M.; Werth, V.P.; Pilkington, C.; Visser, M.; Alfredsson, L.; Amato, A.A.; Barohn, R.J.; Liang, M.H.; et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann. Rheum. Dis. 2017, 76, 1955–1964. [Google Scholar] [CrossRef]
- Fries, J.F.; Hunder, G.G.; Bloch, D.A.; Michel, B.A.; Arend, W.P.; Calabrese, L.H.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; Lightfoot, R.W., Jr.; et al. The American College of Rheumatology 1990 criteria for the classification of vasculitis. Summary. Arthritis Rheum. 1990, 33, 1135–1136. [Google Scholar] [CrossRef]
- Lynch, D.A.; Sverzellati, N.; Travis, W.D.; Brown, K.K.; Colby, T.V.; Galvin, J.R.; Goldin, J.G.; Hansell, D.M.; Inoue, Y.; Johkoh, T.; et al. Diagnostic criteria for idiopathic pulmonary fibrosis: A Fleischner Society White Paper. Lancet Respir. Med. 2018, 6, 138–153. [Google Scholar] [CrossRef]
- Tirelli, C.; Morandi, V.; Valentini, A.; La Carrubba, C.; Dore, R.; Zanframundo, G.; Morbini, P.; Grignaschi, S.; Franconeri, A.; Oggionni, T.; et al. Multidisciplinary Approach in the Early Detection of Undiagnosed Connective Tissue Diseases in Patients with Interstitial Lung Disease: A Retrospective Cohort Study. Front. Med. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Skolnik, K.; Ryerson, C.J. Unclassifiable interstitial lung disease: A review. Respirology 2016, 21, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Ortona, E.; Pierdominici, M.; Maselli, A.; Veroni, C.; Aloisi, F.; Shoenfeld, Y. Sex-based differences in autoimmune diseases. Ann. Ist. Super. Sanita 2016, 52, 205–212. [Google Scholar] [PubMed]
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef] [Green Version]
- Barnes, J.; Mayes, M.D. Epidemiology of systemic sclerosis: Incidence, prevalence, survival, risk factors, malignancy, and environmental triggers. Curr. Opin. Rheumatol. 2012, 24, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.; Nasser, M.; Ahmad, K.; Cottin, V. Interstitial Pneumonia with Autoimmune Features (IPAF). Front. Med. 2019, 6, 209. [Google Scholar] [CrossRef] [PubMed]
- Scirè, C.A.; Gonzalez-Gay, M.A.; Selva-O’Callaghan, A.; Cavagna, L. Clinical spectrum time course of interstitial pneumonia with autoimmune features in patients positive for antisynthetase antibodies. Respir. Med. 2017, 132, 265–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sebastiani, M.; Cassone, G.; De Pasquale, L.; Cerri, S.; Della Casa, G.; Vacchi, C.; Luppi, F.; Salvarani, C.; Manfredi, A. Interstitial pneumonia with autoimmune features: A single center prospective follow-up study. Autoimmun. Rev. 2020, 19, 102451. [Google Scholar] [CrossRef] [PubMed]
- Ghrairi, N.; Aouadi, S.; Elhechmi, Y.Z.; Ben Saad, S.; Ben, A., I; Yalaoui, S. Antinuclear antibodies in interstitial lung disease: Prevalence and clinical significance. Tunis. Med. 2019, 97, 1240–1245. [Google Scholar]
- Solomon, J.J.; Brown, K.K. Rheumatoid arthritis-associated interstitial lung disease. Open Access Rheumatol. 2012, 4, 21–31. [Google Scholar]
- Klareskog, L.; Stolt, P.; Lundberg, K.; Källberg, H.; Bengtsson, C.; Grunewald, J.; Rönnelid, J.; Harris, H.E.; Ulfgren, A.K.; Rantapää-Dahlqvist, S. A new model for an etiology of rheumatoid arthritis: Smoking may trigger HLA-DR (shared epitope)-restricted immune reactions to autoantigens modified by citrullination. Arthritis Rheum. 2006, 54, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Steen, V.D. Autoantibodies in systemic sclerosis. Semin. Arthritis Rheum. 2005, 35, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Hesselstrand, R.; Scheja, A.; Shen, G.Q.; Wiik, A.; Akesson, A. The association of antinuclear antibodies with organ involvement and survival in systemic sclerosis. Rheumatology 2003, 42, 534–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann-Vold, A.M.; Midtvedt, Ø.; Tennøe, A.H.; Garen, T.; Lund, M.B.; Aaløkken, T.M.; Andreassen, A.K.; Elhage, F.; Brunborg, C.; Taraldsrud, E.; et al. Cardiopulmonary Disease Development in Anti-RNA Polymerase III-positive Systemic Sclerosis: Comparative Analyses from an Unselected, Prospective Patient Cohort. J. Rheumatol. 2017, 44, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, J.A.; Stainer, A.; Barnett, J.L.; Renzoni, E.A. Systemic Sclerosis Associated Interstitial Lung Disease: A Comprehensive Overview. Semin. Respir. Crit. Care Med. 2019, 40, 208–226. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Serrano, J.; Herrera-Bringas, D.; Mejía, M.; Rivero, H.; Mateos-Toledo, H.; Figueroa, J.E. Prognostic factors in a cohort of antisynthetase syndrome (ASS): Serologic profile is associated with mortality in patients with interstitial lung disease (ILD). Clin. Rheumatol. 2015, 34, 1563–1569. [Google Scholar] [CrossRef]
- Bartoloni, E.; Gonzalez-Gay, M.A.; Scirè, C.; Castaneda, S.; Gerli, R.; Lopez-Longo, F.J.; Martinez-Barrio, J.; Govoni, M.; Furini, F.; Pina, T.; et al. Clinical follow-up predictors of disease pattern change in anti-Jo1 positive anti-synthetase syndrome: Results from a multicenter, international and retrospective study. Autoimmun. Rev. 2017, 16, 253–257. [Google Scholar] [CrossRef]
- Cavagna, L.; Trallero-Araguás, E.; Meloni, F.; Cavazzana, I.; Rojas-Serrano, J.; Feist, E.; Zanframundo, G.; Morandi, V.; Meyer, A.; Pereira da Silva, J.A.; et al. Influence of Antisynthetase Antibodies Specificities on Antisynthetase Syndrome Clinical Spectrum Time Course. J. Clin. Med. 2019, 8, 2013. [Google Scholar] [CrossRef] [Green Version]
- Kinder, B.W.; Collard, H.R.; Koth, L.; Daikh, D.I.; Wolters, P.J.; Elicker, B.; Jones, K.D.; King, T.E., Jr. Idiopathic nonspecific interstitial pneumonia: Lung manifestation of undifferentiated connective tissue disease? Am. J. Respir. Crit. Care Med. 2007, 176, 691–697. [Google Scholar] [CrossRef] [Green Version]
- Spagnolo, P.; Lee, J.S.; Sverzellati, N.; Rossi, G.; Cottin, V. The Lung in Rheumatoid Arthritis: Focus on Interstitial Lung Disease. Arthritis Rheumatol. 2018, 70, 1544–1554. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.H.; Cox, C.W.; Montner, S.M.; Adegunsoye, A.; Oldham, J.M.; Husain, A.N.; Vij, R.; Noth, I.; Lynch, D.A.; Strek, M.E. CT Features of the Usual Interstitial Pneumonia Pattern: Differentiating Connective Tissue Disease-Associated Interstitial Lung Disease From Idiopathic Pulmonary Fibrosis. AJR Am. J. Roentgenol. 2018, 210, 307–313. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ILD Patients, n = 338 | AD-ILD, n = 111 | IPF, n = 143 | IIP-Non IPF, n = 84 | p-Value a | p-Value b | p-Value c | p-Value d | |
|---|---|---|---|---|---|---|---|---|
| Sex (women/men), n (%) | 108/230 (32.0/68.0) | 53/58 (47.7/52.3) | 24/119 (16.8/83.2) | 31/53 (36.9/63.1) | <0.001 | <0.001 | 0.13 | <0.001 |
| Age at ILD diagnosis, years, median [IQR] | 59 (52–64) | 57 (50–63) | 60 (55–64) | 58 (44–66) | 0.01 | 0.006 | 0.87 | 0.025 |
| Smoking ever, n (%) | 232 (68.6) | 69 (62.2) | 113 (79.0) | 50 (59.5) | 0.002 | 0.003 | 0.71 | 0.002 |
| Pulmonary function tests | ||||||||
| FEV1 (% predicted), mean ± SD | 76.4 ± 22.6 | 79.2 ± 24.7 | 77.5 ± 20.3 | 70.8 ± 22.8 | 0.029 | 0.56 | 0.018 | 0.024 |
| FVC (% predicted), mean ± SD | 77.6 ± 23.0 | 81.8 ± 25.0 | 77.4 ± 19.9 | 72.4 ± 24.3 | 0.018 | 0.12 | 0.009 | 0.09 |
| FEV1/FVC (% predicted), mean ± SD | 78.9 ± 9.6 | 77.9 ± 8.7 | 79.0 ± 9.2 | 80.0 ± 11.2 | 0.33 | 0.35 | 0.15 | 0.47 |
| DLCO (% predicted) mean ± SD | 36.7 ± 15.1 | 38.2 ± 14.7 | 34.9 ± 15.4 | 37.9 ± 14.9 | 0.28 | 0.15 | 0.92 | 0.25 |
| Actual lung transplant received, n (%) | 82 (24.3) | 18 (16.2) | 45 (31.5) | 19 (22.6) | 0.018 | 0.005 | 0.26 | 0.15 |
| Rheumatic autoimmune disease | n (%) |
| Rheumatoid arthritis | 30 (27.0) |
| Systemic sclerosis | 29 (26.1) |
| Interstitial pneumonia with autoimmune features | 20 (18.0) |
| Anti-synthetase syndrome | 19 (17.1) |
| Others a | 13 (11.8) |
| Autoantibody profile b | n/N (%) |
| Rheumatoid factor | 31/79 (39.2) |
| Anti–citrullinated protein antibody | 25/59 (42.4) |
| Antinuclear antibody | 64/90 (71.1) |
| Anti-SSa (Ro) | 17/53 (32.1) |
| Anti-SSb (La) | 4/50 (8.0) |
| Anti-Scl 70 | 15/61 (24.6) |
| Myositis-associated antibodies c | 26/56 (46.4) |
| Others d | 15/67 (22.4) |
| High-resolution computed tomography pattern | n (%) |
| UIP pattern | 41 (37.3) |
| Probable UIP pattern | 16 (14.5) |
| Indeterminate for UIP pattern | 3 (2.7) |
| Features most consistent with an alternative diagnosis | |
| NSIP pattern | 43 (39.1) |
| Non-NSIP pattern | 7 (6.4) |
| RA-ILD n (%) | SSc-ILD n (%) | IPAF n (%) | Anti-Synthetase Syndrome n (%) | |
|---|---|---|---|---|
| UIP pattern | 18 (60.0) | 6 (21.5) | 8 (40.0) | 5 (26.3) |
| Probable UIP pattern | 2 (6.7) | 4 (14.3) | 4 (20.0) | 4 (21.1) |
| Indeterminate for UIP pattern | 1 (3.3) | 2 (7.1) | - | - |
| Features most consistent with an alternative diagnosis | ||||
| NSIP pattern | 8 (26.7) | 14 (50.0) | 5 (25.0) | 10 (52.6) |
| Non-NSIP pattern | 1 (3.3) | 2 (7.1) | 3 (15.0) | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atienza-Mateo, B.; Remuzgo-Martínez, S.; Mora Cuesta, V.M.; Iturbe-Fernández, D.; Fernández-Rozas, S.; Prieto-Peña, D.; Calderón-Goercke, M.; Corrales, A.; Blanco Rodríguez, G.; Gómez-Román, J.J.; et al. The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation †. J. Clin. Med. 2020, 9, 1606. https://doi.org/10.3390/jcm9061606
Atienza-Mateo B, Remuzgo-Martínez S, Mora Cuesta VM, Iturbe-Fernández D, Fernández-Rozas S, Prieto-Peña D, Calderón-Goercke M, Corrales A, Blanco Rodríguez G, Gómez-Román JJ, et al. The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation †. Journal of Clinical Medicine. 2020; 9(6):1606. https://doi.org/10.3390/jcm9061606
Chicago/Turabian StyleAtienza-Mateo, Belén, Sara Remuzgo-Martínez, Víctor Manuel Mora Cuesta, David Iturbe-Fernández, Sonia Fernández-Rozas, Diana Prieto-Peña, Mónica Calderón-Goercke, Alfonso Corrales, Gerardo Blanco Rodríguez, José Javier Gómez-Román, and et al. 2020. "The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation †" Journal of Clinical Medicine 9, no. 6: 1606. https://doi.org/10.3390/jcm9061606
APA StyleAtienza-Mateo, B., Remuzgo-Martínez, S., Mora Cuesta, V. M., Iturbe-Fernández, D., Fernández-Rozas, S., Prieto-Peña, D., Calderón-Goercke, M., Corrales, A., Blanco Rodríguez, G., Gómez-Román, J. J., González-Gay, M. Á., & Cifrián, J. M. (2020). The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation †. Journal of Clinical Medicine, 9(6), 1606. https://doi.org/10.3390/jcm9061606