Outcomes of COVID-19 among Patients on In-Center Hemodialysis: An Experience from the Epicenter in South Korea

 , , ,
, , ,  ,
, 

Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Laboratory Confirmation of SARS-CoV-2
2.3. Data Collection
2.4. Criteria for Quarantine Release and Discharge
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
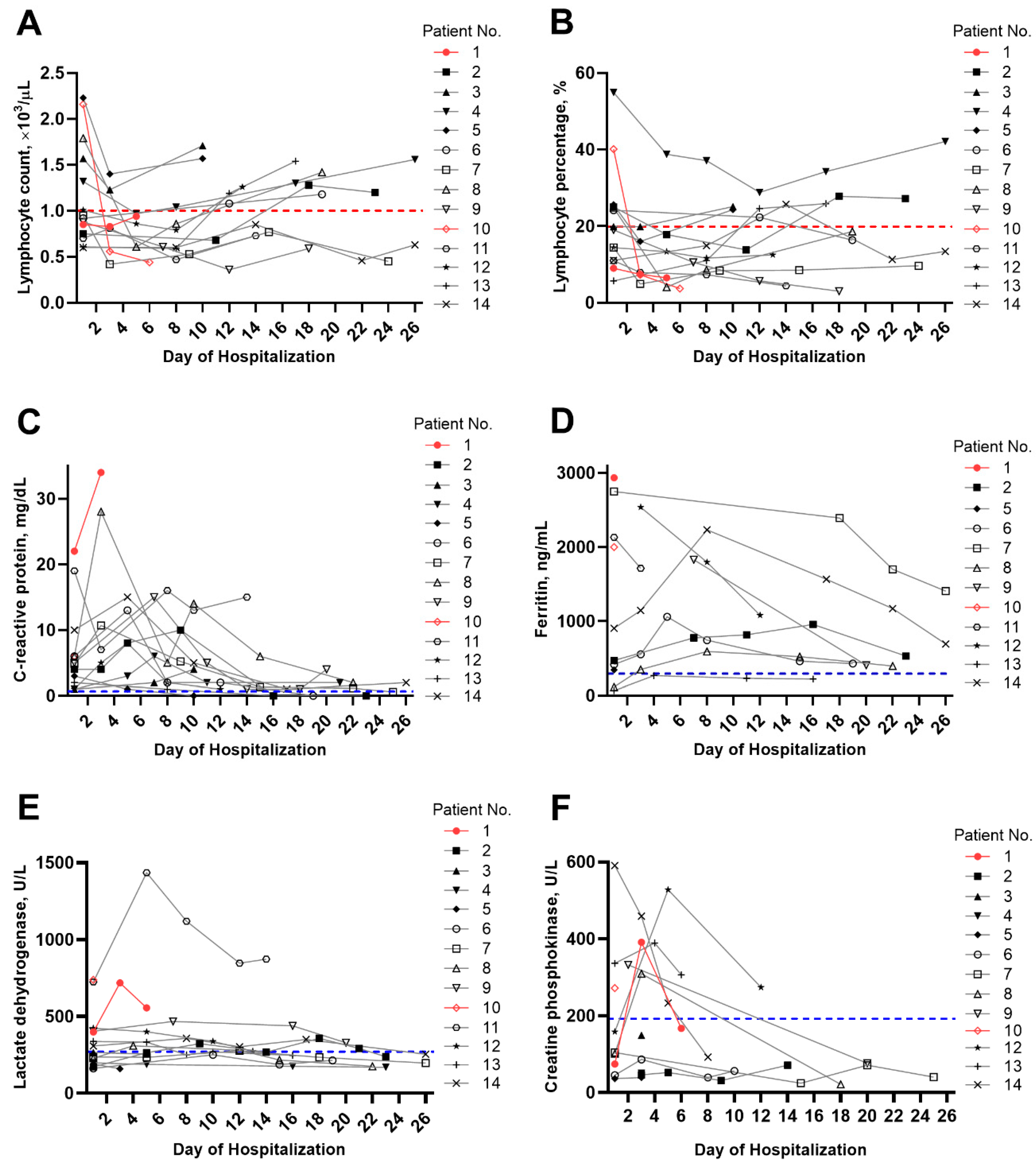
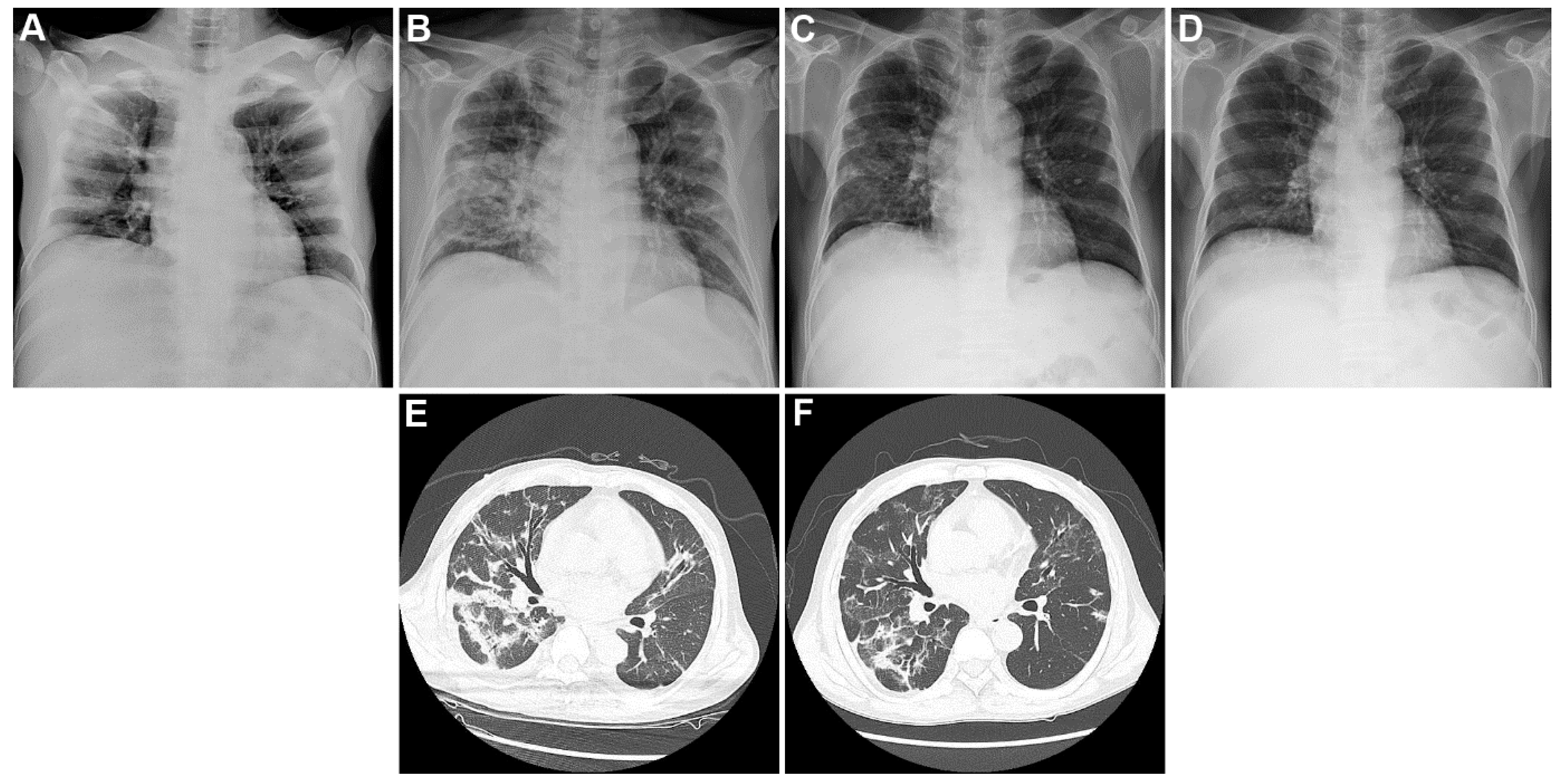
3.2. Clinical Findings
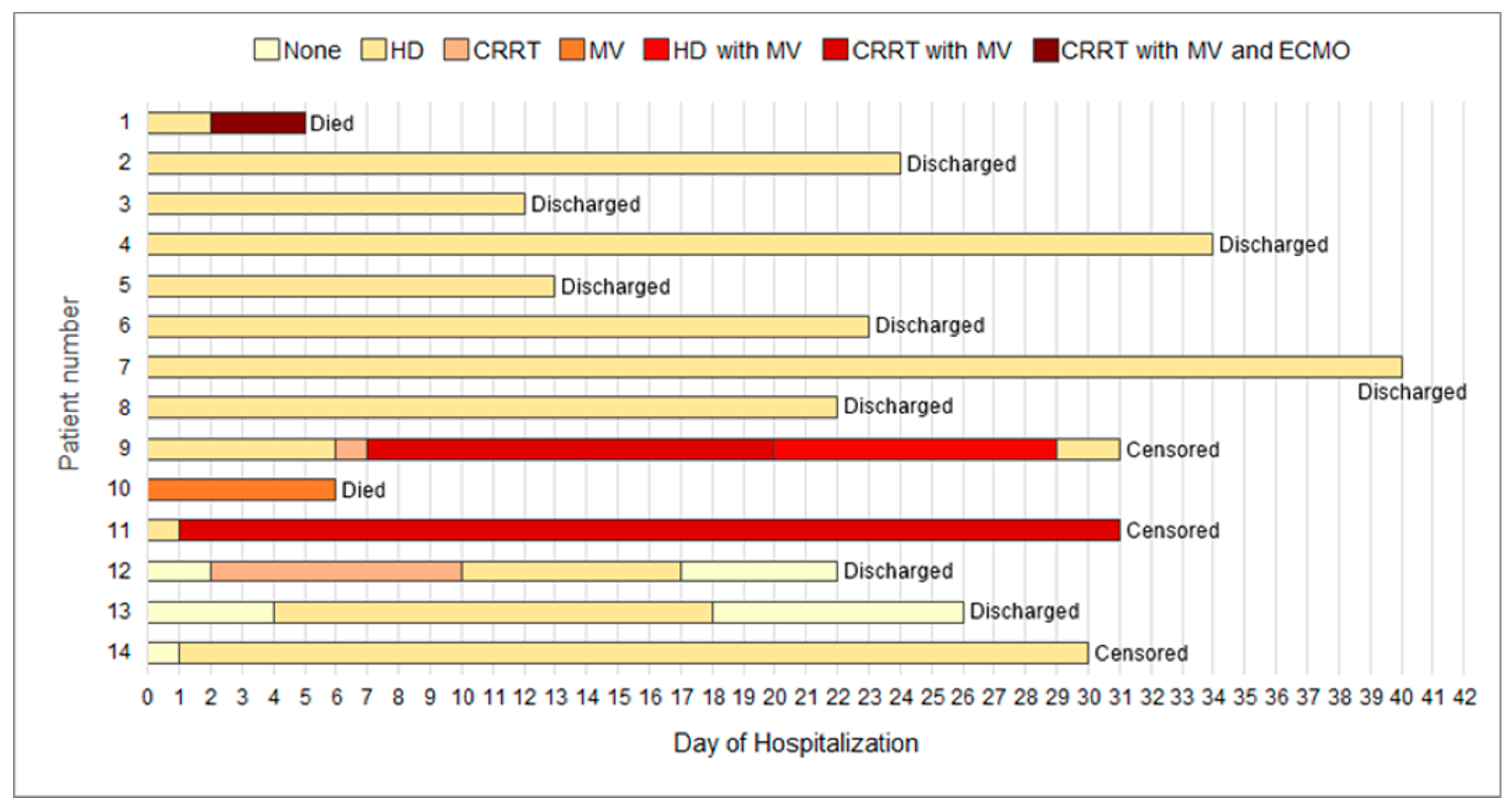
3.3. Treatments and Outcomes
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Hui, I.A.E.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; McHugh, T.D.; Memish, Z.A.; Drosten, C. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health-The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, B.E.; Ong, S.W.X.; Kalimuddin, S.; Low, J.G.; Tan, S.Y.; Loh, J.; Ng, O.T.; Marimuthu, K.; Ang, L.W.; Mak, T.M.; et al. Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore. JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korean Society of Infectious Diseases; Korean Society of Pediatric Infectious Diseases; Korean Society of Epidemiology; Korean Society for Antimicrobial Therapy; Korean Society for Healthcare-Associated Infection Control and Prevention; Korea Centers for Disease Control and Prevention. Report on the Epidemiological Features of Coronavirus Disease 2019 (COVID-19) Outbreak in the Republic of Korea from January 19 to March 2, 2020. J. Korean Med. Sci. 2020, 35, e112. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020. [Google Scholar] [CrossRef]
- Henry, B.M.; Lippi, G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int. Urol. Nephrol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Ikizler, T.A. COVID-19 and Dialysis Units: What Do We Know Now and What Should We Do? Am. J. Kidney Dis. 2020. [Google Scholar] [CrossRef]
- Naicker, S.; Yang, C.W.; Hwang, S.J.; Liu, B.C.; Chen, J.H.; Jha, V. The Novel Coronavirus 2019 epidemic and kidneys. Kidney Int. 2020. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Wang, R.; Liao, C.; He, H.; Hu, C.; Wei, Z.; Hong, Z.; Zhang, C.; Liao, M.; Shui, H. COVID-19 in Hemodialysis Patients: A Report of 5 Cases. Am. J. Kidney Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ferrey, A.J.; Choi, G.; Hanna, R.M.; Chang, Y.; Tantisattamo, E.; Ivaturi, K.; Park, E.; Nguyen, L.; Wang, B.; Tonthat, S.; et al. A Case of Novel Coronavirus Disease 19 in a Chronic Hemodialysis Patient Presenting with Gastroenteritis and Developing Severe Pulmonary Disease. Am. J. Nephrol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goicoechea, M.; Cámara, L.A.S.; Macías, N.; de Morales, A.M.; Rojas, Á.G.; Bascuñana, A.; Arroyo, D.; Vega, A.; Abad, S.; Verde, E. COVID-19: Clinical course and outcomes of 36 maintenance hemodialysis patients from a single center in Spain. Kidney Int. 2020. [Google Scholar] [CrossRef] [PubMed]
- Dudreuilh, C.; Kumar, N.; Moxham, V.; Hemsley, C.; Goldenberg, S.; Moutzouris, D.-A. De-isolation of COVID-positive haemodialysis patients in the outpatient setting: A single centre experience. Kidney Int. 2020. [Google Scholar] [CrossRef]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Piva, S.; Latronico, N.; et al. Management of Patients On Dialysis And With Kidney Transplant During SARS-COV-2 (COVID-19) Pandemic In Brescia, Italy. Kidney Int. Rep. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Diao, B.; Lv, X.; Zhu, J.; Liang, W.; Liu, L.; Bu, W.; Cheng, H.; Zhang, S.; Shi, M. 2019 novel coronavirus disease in hemodialysis (HD) patients: Report from one HD center in Wuhan, China. MedRxiv 2020. (pre-published). [Google Scholar]
- Park, H.; Kim, D.; Yoo, K.; Kim, Y.; Lee, S.; Yoon, H.; Kim, D.; Kim, S.; Kim, M.; Jung, Y.; et al. Korean clinical practice guidelines for preventing transmission of coronavirus disease 2019 (COVID-19) in hemodialysis facilities. Kidney Res. Clin. Pract. 2020. [Google Scholar] [CrossRef]
- Jaillon, S.; Berthenet, K.; Garlanda, C. Sexual Dimorphism in Innate Immunity. Clin. Rev. Allergy Immunol. 2019, 56, 308–321. [Google Scholar] [CrossRef]
- Ahmed, S.B.; Ramesh, S. Sex hormones in women with kidney disease. Nephrol. Dial. Transplant. 2016, 31, 1787–1795. [Google Scholar] [CrossRef] [Green Version]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C.; et al. Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am. J. Gastroenterol. 2020. [Google Scholar] [CrossRef]
- Laird, E.; Rhodes, J.; Kenny, R. Vitamin D and Inflammation: Potential Implications for Severity of Covid-19. Ir. Med. J. 2020, 113, 81. [Google Scholar]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 33. [Google Scholar] [CrossRef] [PubMed]
- Delevaux, I.; Andre, M.; Colombier, M.; Albuisson, E.; Meylheuc, F.; Begue, R.J.; Piette, J.C.; Aumaitre, O. Can procalcitonin measurement help in differentiating between bacterial infection and other kinds of inflammatory processes? Ann. Rheum. Dis. 2003, 62, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Plebani, M. Procalcitonin in patients with severe coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chim. Acta 2020, 505, 190–191. [Google Scholar] [CrossRef] [PubMed]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Patients (n = 14) |
|---|---|
| Age | |
| Mean age (range), years | 63.5 ± 14.5 (40.0–88.0) |
| Distribution, n (%) | |
| <50 years | 2 (14.3) |
| 50–64 years | 8 (57.1) |
| 65–79 years | 1 (7.1) |
| ≥80 years | 3 (21.4) |
| Sex, n (%) | |
| Male/Female | 6 (42.9)/8 (57.1) |
| Mean duration of dialysis (range), years | 4.7 ± 5.3 (0–21.0) |
| Cause of ESRD, n (%) | |
| Diabetes mellitus | 7 (50.0) |
| Hypertension | 2 (14.3) |
| Others | 5 (35.7) |
| Body mass index, kg/m2 | 23.6 ± 4.3 |
| Comorbidities, n (%) | |
| Cardiovascular disease | 2 (14.2) |
| Cerebrovascular disease | 3 (21.4) |
| Chronic obstructive pulmonary disease | 0 |
| Diabetes mellitus | 7 (50.0) |
| Hypertension | 11 (78.6) |
| Cancer | 2 (14.3) |
| Charlson Comorbidity Index | 5.6 ± 1.8 |
| History of contacts with patient with COVID-19, n (%) | 4 (28.6) |
| Symptoms | |
| Cough | 7 (50.0) |
| Sputum | 3 (21.4) |
| Dyspnea | 5 (35.7) |
| Sore throat | 1 (7.1) |
| Rhinorrhea | 2 (14.3) |
| Myalgia | 2 (14.3) |
| Fatigue | 4 (28.6) |
| Nausea, vomiting, or diarrhea | 2 (14.3) |
| Mean duration from symptom onset to diagnosis, days | 2.6 ± 2.3 |
| Mean duration from symptom onset to admission, days | 3.5 ± 2.8 |
| Parameter | Patients (n = 14) |
|---|---|
| Vital signs | |
| Systolic blood pressure, mmHg | 136.5 ± 24.7 |
| Diastolic blood pressure, mmHg | 76.8 ± 15.6 |
| Heart rate >100 beats per min, n (%) | 2 (14.3) |
| Respiratory rate ≥20 breaths per min, n (%) | 5 (35.7) |
| Body temperature ≥ 38 °C, n (%) | 3 (21.4) |
| Laboratory results (normal range) | |
| White blood cell count, ×103/µL (4.0–10.0) | 5.8 ± 2.1 |
| Lymphocyte count, ×103/µL (1.0–4.5) | 1.1 ± 0.5 |
| Hemoglobin, g/dL (13.0–18.0) | 10.5 ± 1.4 |
| Platelet count, ×103/µL (130–400) | 162.1 ± 74.0 |
| C-reactive protein, mg/dL (<0.5) | 6.1 (3.0–8.8) |
| Ferritin, ng/mL (n = 9; 30–400) | 472.0 (292.4–1693.2) |
| Procalcitonin, ng/mL (n = 9; <0.05) | 0.6 (0.3–1.0) |
| Albumin, g/dL (3.5–5.2) | 3.3 ± 0.7 |
| Alanine aminotransferase, U/L (<41) | 14.5 (11.5–18.0) |
| Aspartate aminotransferase, U/L (<40) | 19.0 (16.0–33.8) |
| Lactate dehydrogenase, U/L (135–250) | 264.5 (196.0–401.0) |
| Creatine phosphokinase, U/L (n = 10; 26–192) | 210.4 ± 188.8 |
| Lactic acid, mmol/L (n = 8; 0.5–1.6) | 1.3 (1.1–2.2) |
| Prothrombin time, sec (n = 12; 10–14) | 13.1 (13.0–13.9) |
| Activated partial thromboplastin time, s (n = 12; 20–35) | 37.8 (36.3–40.9) |
| D-dimer, µg/mL (n = 7; <0.5) | 1.7 (1.0–3.8) |
| Chest radiography findings, n (%) | |
| Clear | 4 (28.6) |
| Unilateral infiltration | 3 (21.4) |
| Bilateral infiltration | 7 (50.0) |
| Pleural effusion | 2 (14.3) |
| Patients (n = 14) | |
|---|---|
| Treatment, n (%) | |
| Low-flow oxygen therapy | 4 (28.6) |
| High-flow oxygen therapy | 2 (14.3) |
| Invasive mechanical ventilation | 4 (28.6) |
| ECMO | 1 (7.1) |
| CRRT | 4 (28.6) |
| Lopinavir and ritonavir | 14 (100.0) |
| Hydroxychloroquine | 7 (50.0) |
| Others | |
| Antibiotics treatment | 13 (92.9) |
| Antifungal treatment | 2 (14.3) |
| Glucocorticoids | 3 (21.4) |
| Intravenous immunoglobulin therapy | 1 (7.1) |
| Vasopressors | 4 (28.6) |
| Events during hemodialysis, n (%) | |
| Hypotension | 3 (21.4) |
| Dialysis vascular access occlusion | 3 (21.4) |
| Arrhythmia | 1 (7.1) |
| Patients (n = 14) | |
|---|---|
| Outcomes | |
| Median length of stay (IQR), days | |
| In hospital | 22.0 (14.0–30.0) |
| In ICU (n = 5) | 6.0 (5.0–27.0) |
| Median duration of positive results following COVID-19 test (IQR), days | 21.0 (12.0–30.0) |
| Median duration of mechanical ventilation (IQR), days (n = 4) | 14.0 (4.0–28.0) |
| Median duration of ECMO, days (n = 1) | 3 |
| Median duration of CRRT (IQR), days (n = 4) | 8.5 (3.0–25.0) |
| Died in the hospital, n (%) | 2 (14.3) |
| Discharged from the hospital, n (%) | 9 (64.3) |
| Remained in the hospital, n (%) | 3 (21.4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, H.-Y.; Lim, J.-H.; Kang, S.H.; Kim, S.G.; Lee, Y.-H.; Lee, J.; Chang, H.-H.; Kim, S.-W.; Choi, J.-Y.; Cho, J.-H.; et al. Outcomes of COVID-19 among Patients on In-Center Hemodialysis: An Experience from the Epicenter in South Korea. J. Clin. Med. 2020, 9, 1688. https://doi.org/10.3390/jcm9061688
Jung H-Y, Lim J-H, Kang SH, Kim SG, Lee Y-H, Lee J, Chang H-H, Kim S-W, Choi J-Y, Cho J-H, et al. Outcomes of COVID-19 among Patients on In-Center Hemodialysis: An Experience from the Epicenter in South Korea. Journal of Clinical Medicine. 2020; 9(6):1688. https://doi.org/10.3390/jcm9061688
Chicago/Turabian StyleJung, Hee-Yeon, Jeong-Hoon Lim, Seok Hui Kang, Seong Gyu Kim, Yong-Hoon Lee, Jaehee Lee, Hyun-Ha Chang, Shin-Woo Kim, Ji-Young Choi, Jang-Hee Cho, and et al. 2020. "Outcomes of COVID-19 among Patients on In-Center Hemodialysis: An Experience from the Epicenter in South Korea" Journal of Clinical Medicine 9, no. 6: 1688. https://doi.org/10.3390/jcm9061688
APA StyleJung, H. -Y., Lim, J. -H., Kang, S. H., Kim, S. G., Lee, Y. -H., Lee, J., Chang, H. -H., Kim, S. -W., Choi, J. -Y., Cho, J. -H., Kim, C. -D., Kim, Y. -L., & Park, S. -H. (2020). Outcomes of COVID-19 among Patients on In-Center Hemodialysis: An Experience from the Epicenter in South Korea. Journal of Clinical Medicine, 9(6), 1688. https://doi.org/10.3390/jcm9061688