Prognostic Value of Early Intermittent Electroencephalography in Patients after Extracorporeal Cardiopulmonary Resuscitation

 ,
,
Abstract
:1. Introduction
2. Methods
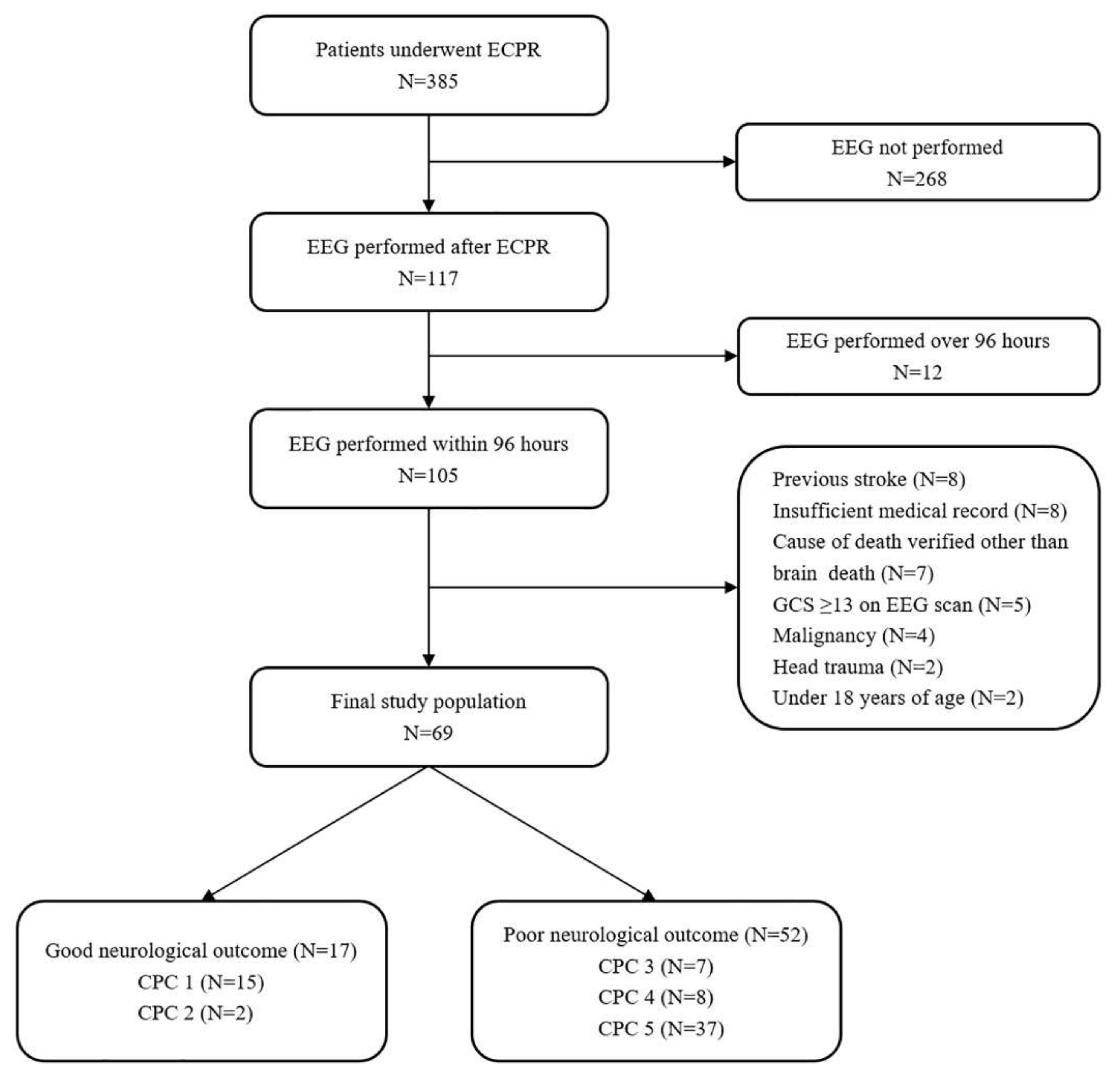
2.1. Study Population and Design
2.2. Endpoints and Definitions
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics and Clinical Outcomes
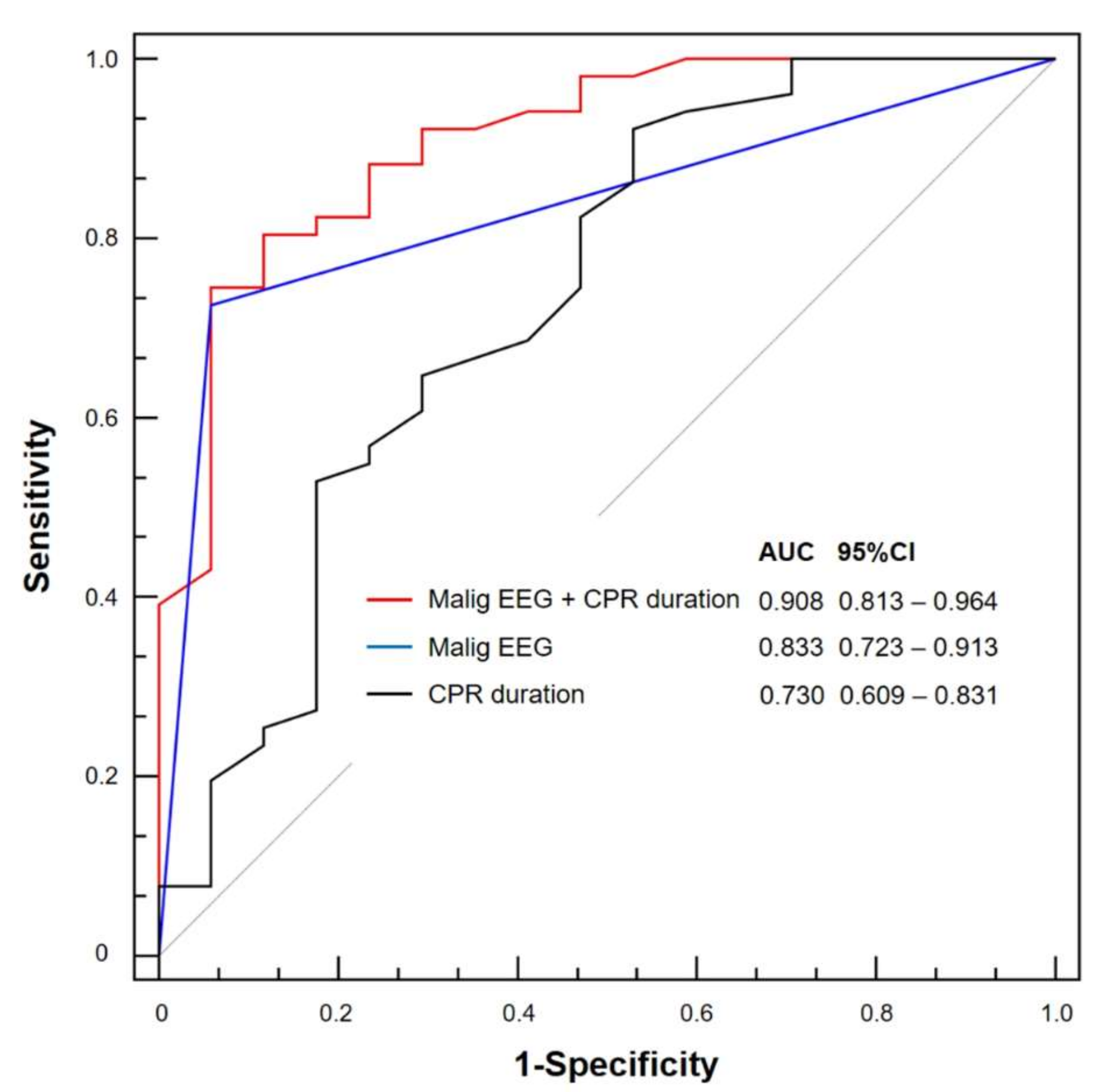
3.2. Relationship between EEG and Neurologic Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data and Materials
Consent for Publication
References
- Ryu, J.A.; Chung, C.R.; Cho, Y.H.; Sung, K.; Suh, G.Y.; Park, T.K.; Song, Y.B.; Hahn, J.Y.; Choi, J.H.; Gwon, H.C.; et al. The association of findings on brain computed tomography with neurologic outcomes following extracorporeal cardiopulmonary resuscitation. Crit. Care 2017, 21, 15. [Google Scholar] [CrossRef] [Green Version]
- Ryu, J.A.; Chung, C.R.; Cho, Y.H.; Sung, K.; Jeon, K.; Suh, G.Y.; Park, T.K.; Lee, J.M.; Song, Y.B.; Hahn, J.Y.; et al. Neurologic Outcomes in Patients Who Undergo Extracorporeal Cardiopulmonary Resuscitation. Ann. Thorac. Surg. 2019, 108, 749–755. [Google Scholar] [CrossRef]
- Sondag, L.; Ruijter, B.J.; Tjepkema-Cloostermans, M.C.; Beishuizen, A.; Bosch, F.H.; van Til, J.A.; van Putten, M.; Hofmeijer, J. Early EEG for outcome prediction of postanoxic coma: Prospective cohort study with cost-minimization analysis. Crit. Care 2017, 21, 111. [Google Scholar] [CrossRef] [Green Version]
- Ryu, J.A.; Cho, Y.H.; Sung, K.; Choi, S.H.; Yang, J.H.; Choi, J.H.; Lee, D.S.; Yang, J.H. Predictors of neurological outcomes after successful extracorporeal cardiopulmonary resuscitation. BMC Anesthesiol. 2015, 15, 26. [Google Scholar] [CrossRef] [Green Version]
- Ahn, C.; Kim, W.; Cho, Y.; Choi, K.S.; Jang, B.H.; Lim, T.H. Efficacy of extracorporeal cardiopulmonary resuscitation compared to conventional cardiopulmonary resuscitation for adult cardiac arrest patients: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 34208. [Google Scholar] [CrossRef]
- Sundgreen, C.; Larsen, F.S.; Herzog, T.M.; Knudsen, G.M.; Boesgaard, S.; Aldershvile, J. Autoregulation of cerebral blood flow in patients resuscitated from cardiac arrest. Stroke 2001, 32, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Park, S.B.; Yang, J.H.; Park, T.K.; Cho, Y.H.; Sung, K.; Chung, C.R.; Park, C.M.; Jeon, K.; Song, Y.B.; Hahn, J.Y.; et al. Developing a risk prediction model for survival to discharge in cardiac arrest patients who undergo extracorporeal membrane oxygenation. Int. J. Cardiol. 2014, 177, 1031–1035. [Google Scholar] [CrossRef]
- Westhall, E. Electroencephalography as a Prognostic Tool after Cardiac Arrest. Semin. Neurol. 2017, 37, 48–59. [Google Scholar] [CrossRef]
- Kang, M.J.; Lee, T.R.; Shin, T.G.; Sim, M.S.; Jo, I.J.; Song, K.J.; Jeong, Y.K. Survival and neurologic outcomes of out-of-hospital cardiac arrest patients who were transferred after return of spontaneous circulation for integrated post-cardiac arrest syndrome care: The another feasibility of the cardiac arrest center. J. Korean Med. Sci. 2014, 29, 1301–1307. [Google Scholar] [CrossRef] [Green Version]
- Cummins, R.O.; Chamberlain, D.A.; Abramson, N.S.; Allen, M.; Baskett, P.J.; Becker, L.; Bossaert, L.; Delooz, H.H.; Dick, W.F.; Eisenberg, M.S.; et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: The Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 1991, 84, 960–975. [Google Scholar]
- The Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef]
- Rittenberger, J.C.; Raina, K.; Holm, M.B.; Kim, Y.J.; Callaway, C.W. Association between Cerebral Performance Category, Modified Rankin Scale, and discharge disposition after cardiac arrest. Resuscitation 2011, 82, 1036–1040. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Jung, D.S.; Hwang, K.J.; Seo, J.H.; Na, G.Y.; Hong, S.B.; Joo, E.Y.; Seo, D.W. Can an exercise bicycle be safely used in the epilepsy monitoring unit?: An exercise method to provoke epileptic seizures and the related safety issues. Epilepsy Behav. 2015, 46, 79–83. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, L.J.; LaRoche, S.M.; Gaspard, N.; Gerard, E.; Svoronos, A.; Herman, S.T.; Mani, R.; Arif, H.; Jette, N.; Minazad, Y.; et al. American Clinical Neurophysiology Society’s Standardized Critical Care EEG Terminology: 2012 version. J. Clin. Neurophysiol. 2013, 30, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Westhall, E.; Rossetti, A.O.; van Rootselaar, A.F.; Wesenberg Kjaer, T.; Horn, J.; Ullen, S.; Friberg, H.; Nielsen, N.; Rosen, I.; Aneman, A.; et al. Standardized EEG interpretation accurately predicts prognosis after cardiac arrest. Neurology 2016, 86, 1482–1490. [Google Scholar] [CrossRef]
- Cummins, R.O.; Chamberlain, D.; Hazinski, M.F.; Nadkarni, V.; Kloeck, W.; Kramer, E.; Becker, L.; Robertson, C.; Koster, R.; Zaritsky, A.; et al. Recommended guidelines for reviewing, reporting, and conducting research on in-hospital resuscitation: The in-hospital ‘Utstein style’. American Heart Association. Circulation 1997, 95, 2213–2239. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Amorim, E.; Rittenberger, J.C.; Baldwin, M.E.; Callaway, C.W.; Popescu, A. Malignant EEG patterns in cardiac arrest patients treated with targeted temperature management who survive to hospital discharge. Resuscitation 2015, 90, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.H.; Park, K.N.; Shon, Y.M.; Kim, Y.M.; Kim, H.J.; Youn, C.S.; Kim, S.H.; Choi, S.P.; Kim, S.C. Continuous Amplitude-Integrated Electroencephalographic Monitoring Is a Useful Prognostic Tool for Hypothermia-Treated Cardiac Arrest Patients. Circulation 2015, 132, 1094–1103. [Google Scholar] [CrossRef]
- Samaniego, E.A.; Mlynash, M.; Caulfield, A.F.; Eyngorn, I.; Wijman, C.A. Sedation confounds outcome prediction in cardiac arrest survivors treated with hypothermia. Neurocrit. Care 2011, 15, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Young, G.B. Clinical practice. Neurologic prognosis after cardiac arrest. N. Engl. J. Med. 2009, 361, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Stecker, M.M.; Cheung, A.T.; Pochettino, A.; Kent, G.P.; Patterson, T.; Weiss, S.J.; Bavaria, J.E. Deep hypothermic circulatory arrest: I. Effects of cooling on electroencephalogram and evoked potentials. Ann. Thorac. Surg. 2001, 71, 14–21. [Google Scholar] [CrossRef]
- Sekhon, M.S.; Ainslie, P.N.; Griesdale, D.E. Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: A “two-hit” model. Crit. Care 2017, 21, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandroni, C.; Cariou, A.; Cavallaro, F.; Cronberg, T.; Friberg, H.; Hoedemaekers, C.; Horn, J.; Nolan, J.P.; Rossetti, A.O.; Soar, J. Prognostication in comatose survivors of cardiac arrest: An advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine. Resuscitation 2014, 85, 1779–1789. [Google Scholar] [CrossRef]
- Taccone, F.; Cronberg, T.; Friberg, H.; Greer, D.; Horn, J.; Oddo, M.; Scolletta, S.; Vincent, J.L. How to assess prognosis after cardiac arrest and therapeutic hypothermia. Crit Care 2014, 18, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongiovanni, F.; Romagnosi, F.; Barbella, G.; Di Rocco, A.; Rossetti, A.O.; Taccone, F.S.; Sandroni, C.; Oddo, M. Standardized EEG analysis to reduce the uncertainty of outcome prognostication after cardiac arrest. Intensive Care Med. 2020, 46, 963–972. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Favorable Neurological Outcome (n = 17) | Poor Neurological Outcome (n = 52) | p Value | |
|---|---|---|---|
| Age (y)—median (IQR) | 51.0 (36.0–73.0) | 57.5 (50.0–69.5) | 0.460 |
| Gender, male—no. of patients (%) | 15 (88.2) | 37 (71.2) | 0.206 |
| Body mass index (kg/m2)—median (IQR) | 23.5 (21.3–27.7) | 25.2 (22.2–28.7) | 0.354 |
| Medical history—no. of patients (%) | |||
| Hypertension | 3 (17.6) | 26 (50.0) | 0.039 |
| Diabetes mellitus | 3 (17.6) | 20 (38.5) | 0.199 |
| Current smoker | 6 (35.3) | 11 (21.2) | 0.331 |
| Previous myocardial infarction | 2 (11.8) | 12 (23.1) | 0.491 |
| Malignancy | 1 (5.9) | 11 (21.2) | 0.269 |
| Dyslipidemia | 2 (11.8) | 10 (19.2) | 0.716 |
| Target temperature management—no. of patients (%) | 9 (52.9) | 21 (40.4) | 0.532 |
| Type of cardiac arrest—no. of patients (%) | 0.581 | ||
| Out of hospital cardiac arrest | 4 (23.5) | 18 (34.6) | |
| In-hospital cardiac arrest | 13 (76.5) | 34 (65.4) | |
| Bystander witnessed cardiac arrest—no. of patients (%) | 17 (100) | 50 (96.2) | 0.999 |
| Bystander performed CPR—no. of patients (%) | 16 (94.1) | 48 (92.3) | 0.999 |
| First monitored rhythm—no. of patients (%) | 0.167 | ||
| Asystole | 1 (5.9) | 11 (21.2) | |
| Pulseless electrical activity | 6 (35.3) | 23 (44.2) | |
| Shockable rhythm (VT or VF) | 10 (58.8) | 18 (34.6) | |
| Defibrillation—no. of patients (%) | 12 (70.6) | 30 (57.7) | 0.510 |
| CPR duration (min)—median (IQR) | 19.0 (8.0–28.0) | 31.0 (21.0–40.5) | 0.005 |
| Location of ECMO insertion—no. of patients (%) | 0.177 | ||
| Emergency room | 9 (52.9) | 24 (46.2) | |
| Intensive care unit | 4 (23.5) | 23 (44.2) | |
| Cath room | 4 (23.5) | 4 (7.7) | |
| Operation room | 0 (0) | 1 (1.9) | |
| Cardiac cause of arrest—no. of patients (%) | 0.999 | ||
| Ischemic | 7 (41.2) | 19 (45.2) | |
| Non-ischemic | 10 (58.8) | 23 (54.8) |
| Favorable Neurological Outcome (n = 17) | Poor Neurological Outcome (n = 52) | p Value | |
|---|---|---|---|
| Interval between ECPR and EEG scan—no. of patients (%) | 0.671 | ||
| 0–12 h | 2 (11.8) | 10 (19.2) | |
| 12–24 h | 4 (23.5) | 10 (19.2) | |
| 24–48 h | 5 (29.4) | 20 (38.5) | |
| 48–96 h | 6 (35.3) | 12 (23.1) | |
| Reasons of EEG scan no. of patients (%) | 0.724 | ||
| For neurological outcome prediction or decreased mentality | 7 (41.2) | 26 (50.0) | |
| Seizure or abnormal movement | 10 (58.8) | 26 (50.0) | |
| Pupil reflex—no. of patients (%) | 0.199 | ||
| Both prompt | 13 (76.5) | 27 (51.9) | |
| One or both sluggish | 2 (11.8) | 8 (15.4) | |
| One or both fix | 2 (11.8) | 17 (32.7) | |
| Glasgow Coma Scale on EEG scan | 7.0 (3.0–9.0) | 3.0 (3.0–7.0) | 0.012 |
| Use of sedative or analgesic—no. of patients (%) | 15 (88.2) | 26 (50.0) | 0.012 |
| Bolus infusion | 4 (23.5) | 10 (19.2) | 0.734 |
| Continuous infusion | 15 (88.2) | 24 (46.2) | 0.006 |
| Remifentanil | 8 (47.1) | 13 (25.0) | |
| Midazolam | 7 (41.2) | 9 (17.3) | |
| Fentanyl | 6 (35.3) | 5 (9.6) | |
| Propofol | 4 (23.5) | 2 (3.8) | |
| Use of antiepileptic drug | 4 (23.5) | 13 (25.0) | 0.999 |
| Favorable Neurological Outcome (n = 17) | Poor Neurological Outcome (n = 52) | p Value | |
|---|---|---|---|
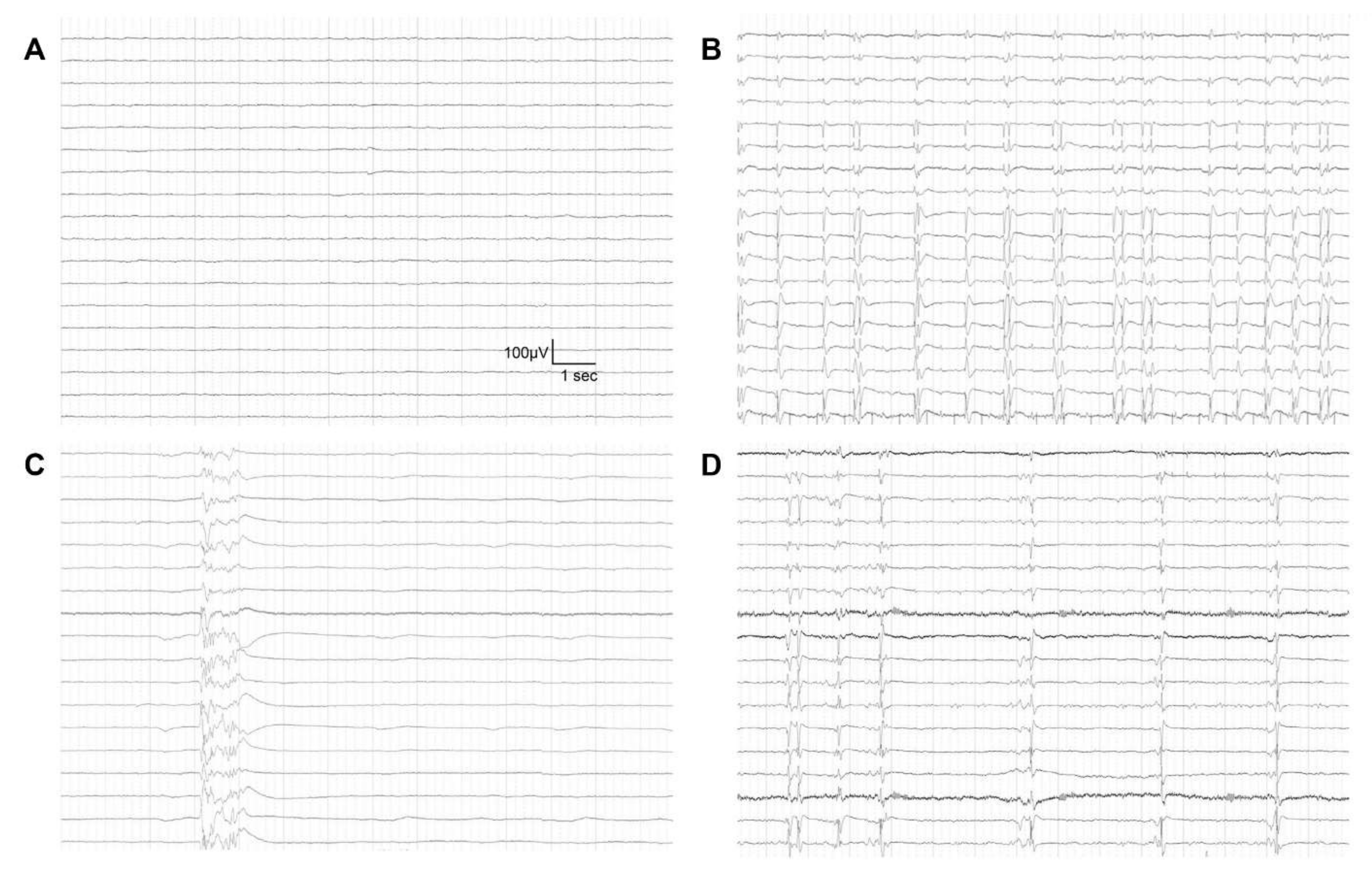
| EEG findings—no. of patients (%) | <0.001 | ||
| Benign EEG | 16 (94.1) | 14 (26.9) | |
| Malignant EEG | 1 (5.9) | 38 (73.1) | |
| Highly malignant EEG | |||
| Suppressed background without discharges | 0 (0) | 18 (34.6) | |
| Suppressed background with continuous periodic discharges | 0 (0) | 2 (3.8) | |
| Burst-suppression background with or without discharges | 0 (0) | 10 (19.2) | |
| Moderately malignant EEG | |||
| Malignant periodic or rhythmic patterns | 0 (0) | 6 (11.5) | |
| Malignant background | 0 (0) | 2 (3.8) | |
| Unreactive EEG | 1 (5.9) | 0 (0) | |
| EEG patterns according to time interval—no. of patients (%) | |||
| EEG performed within 24 h after ECPR | 0.001 | ||
| Benign EEG patterns | 6 (35.3) | 4 (7.7) | |
| Malignant EEG patterns | 0 (0) | 16 (30.8) | |
| EEG performed over 24 h after ECPR | 0.001 | ||
| Benign EEG patterns | 10 (58.8) | 10 (19.2) | |
| Malignant EEG patterns | 1 (5.9) | 22 (42.3) | |
| Accompanied clinical seizure—no. of patients (%) | 0.121 | ||
| Absence of clinical seizure | 7 (41.2) | 28 (53.8) | |
| Sporadic seizure or myoclonus | 10 (58.8) | 18 (34.6) | |
| Myoclonic status epilepticus | 0 (0) | 6 (11.5) |
| Adjusted OR (95% CI) | p Value | |
|---|---|---|
| Malignant EEG patterns | 36.43 (4.632–1013.711) | <0.001 |
| First monitored rhythm | ||
| Asystole | 1 | Reference |
| Pulseless electrical activity | 0.84 (0.046–11.674) | 0.894 |
| Shockable rhythm (VT or VF) | 0.19 (0.011–1.622) | 0.135 |
| CPR duration (min) | 1.06 (1.009–1.138) | 0.020 |
| Use of sedative or analgesic | 0.26 (0.023–1.845) | 0.188 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.O.; Ko, R.-E.; Chung, C.R.; Yang, J.H.; Park, T.K.; Cho, Y.H.; Sung, K.; Suh, G.Y.; Ryu, J.-A. Prognostic Value of Early Intermittent Electroencephalography in Patients after Extracorporeal Cardiopulmonary Resuscitation. J. Clin. Med. 2020, 9, 1745. https://doi.org/10.3390/jcm9061745
Kim YO, Ko R-E, Chung CR, Yang JH, Park TK, Cho YH, Sung K, Suh GY, Ryu J-A. Prognostic Value of Early Intermittent Electroencephalography in Patients after Extracorporeal Cardiopulmonary Resuscitation. Journal of Clinical Medicine. 2020; 9(6):1745. https://doi.org/10.3390/jcm9061745
Chicago/Turabian StyleKim, Yong Oh, Ryoung-Eun Ko, Chi Ryang Chung, Jeong Hoon Yang, Taek Kyu Park, Yang Hyun Cho, Kiick Sung, Gee Young Suh, and Jeong-Am Ryu. 2020. "Prognostic Value of Early Intermittent Electroencephalography in Patients after Extracorporeal Cardiopulmonary Resuscitation" Journal of Clinical Medicine 9, no. 6: 1745. https://doi.org/10.3390/jcm9061745
APA StyleKim, Y. O., Ko, R. -E., Chung, C. R., Yang, J. H., Park, T. K., Cho, Y. H., Sung, K., Suh, G. Y., & Ryu, J. -A. (2020). Prognostic Value of Early Intermittent Electroencephalography in Patients after Extracorporeal Cardiopulmonary Resuscitation. Journal of Clinical Medicine, 9(6), 1745. https://doi.org/10.3390/jcm9061745