Always Online? Internet Addiction and Social Impairment in Psoriasis across Germany

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Recruitment
2.2. Questionnaire
2.3. Statistical Analyses
3. Results
3.1. Social Impairment
3.2. Internet Addiction
3.3. Depression, Smoking, and Drinking
4. Discussion
4.1. Social Impairment
4.2. Internet Addiction
4.3. Depression, Smoking, and Alcohol Dependency
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Total (n = 460) | Gender | p-Value | Age | p-Value | Psoriasis is Preventing Leisure Activities | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female (n = 287) | Male (n = 173) | <46 years (n = 222) | ≥46 years (n = 238) | Never or Rarely (n = 130) | Sometimes, Frequently, or Always (n = 330) | ||||||
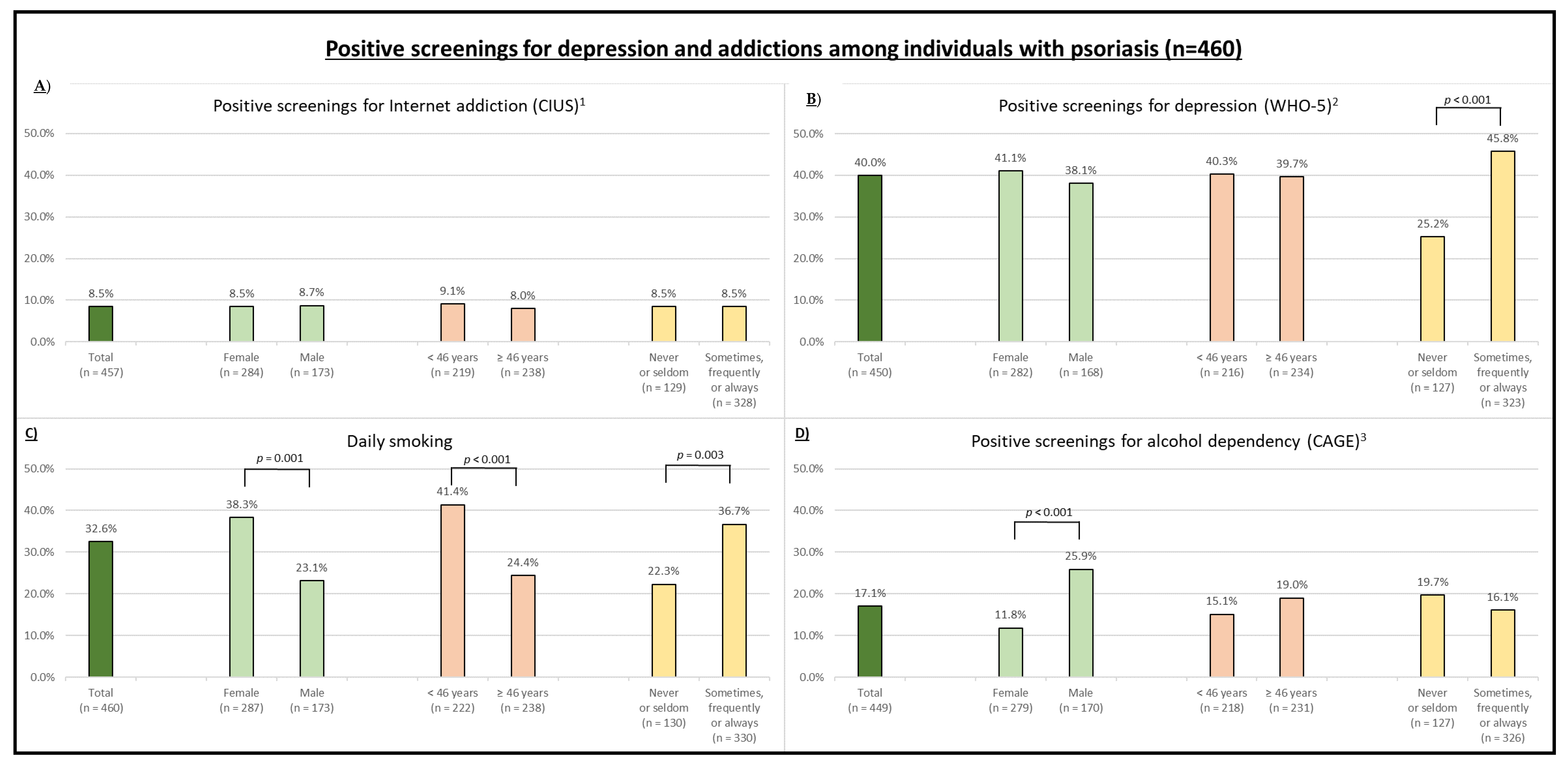
| Internet addiction 3; n (%) | Yes | 39 (8.5%) | 24 (8.5%) | 15 (8.7%) | 0.935 | 20 (9.1%) | 19 (8.0%) | 0.660 | 11 (8.5%) | 28 (8.5%) | 0.997 |
| No | 418 (91.5%) | 260 (91.5%) | 158 (91.3%) | 199 (90.9%) | 219 (92.0%) | 118 (91.5%) | 300 (91.5%) | ||||
| missing | 3 | 3 | 0 | 3 | 0 | 1 | 2 | ||||
| Depression 1; n (%) | Yes | 180 (40.0%) | 116 (41.1%) | 64 (38.1%) | 0.524 | 87 (40.3%) | 93 (39.7%) | 0.908 | 32 (25.2%) | 148 (45.8%) | <0.001 |
| No | 270 (60.0%) | 166 (58.9%) | 104 (61.9%) | 129 (59.7%) | 141 (60.3%) | 95 (74.8%) | 175 (54.2%) | ||||
| missing | 10 | 5 | 5 | 6 | 4 | 3 | 7 | ||||
| Alcohol dependency 2; n (%) | Yes | 77 (17.1%) | 33 (11.8%) | 44 (25.9%) | <0.001 | 33 (15.1%) | 44 (19.0%) | 0.272 | 25 (19.7%) | 52 (16.1%) | 0.371 |
| No | 372 (82.9%) | 246 (88.2%) | 126 (74.1%) | 185 (84.9%) | 187 (81.0%) | 102 (80.3%) | 270 (83.9%) | ||||
| missing | 11 | 8 | 3 | 4 | 7 | 7 | 4 | ||||
| Smoking daily; n (%) | Yes | 150 (32.6%) | 110 (38.3%) | 40 (23.1%) | 0.001 | 92 (41.4%) | 58 (24.4%) | <0.001 | 29 (22.3%) | 121 (36.7%) | 0.003 |
| No | 310 (67.4%) | 177 (61.7%) | 133 (76.9%) | 130 (58.6%) | 180 (75.6%) | 101 (77.7%) | 209 (63.3%) | ||||
| missing | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| Dependent Variable | Independent Variables (Reference) | Crude OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|---|
| Internet addiction 1 | Age | 0.98 (0.96–1.01) | - |
| Gender (male) | 0.97 (0.50–1.91) | - | |
| Duration of psoriasis | 0.97 (0.95–1.00) | 0.97 (0.95–1.00) | |
| Currently in medical care (yes) | 0.99 (0.46–2.17) | - | |
| Severity at the time of study participation (mild) | - | - | |
| moderate | 1.34 (0.56–3.24) | - | |
| severe | 1.29 (0.46–3.60) | - | |
| Severity in general (mild) | - | - | |
| moderate | 0.54 (0.19–1.53) | - | |
| severe | 0.61 (0.20–1.80) | - | |
| Social impairment (never or rarely) | 1.00 (0.48–2.08) | - | |
| Depression 2 | Age | 0.99 (0.98–1.01) | - |
| Gender (male) | 1.14 (0.77–1.68) | - | |
| Duration of psoriasis | 0.98 (0.97–1.00) | 0.98 (0.97–1.00) | |
| Currently in medical care (yes) | 1.32 (0.84–2.09) | - | |
| Severity at the time of study participation (mild) | - | - | |
| moderate | 1.53 (0.92–2.52) | 1.34 (0.80–2.25) | |
| severe | 2.77 (1.55–4.94) | 2.13 (1.16–3.91) | |
| Severity in general (mild) | - | - | |
| moderate | 1.11 (0.53–2.31) | - | |
| severe | 2.08 (0.98–4.43) | - | |
| Social impairment (never or rarely) | 2.51 (1.59–3.96) | 2.12 (1.32–3.42) | |
| Daily smoking | Age | 0.96 (0.95–0.98) | 0.96 (0.95–0.98) |
| Gender (male) | 2.07 (1.35–3.16) | 2.13 (1.36–3.34) | |
| Duration of psoriasis | 0.98 (0.96–0.99) | - | |
| Currently in medical care (yes) | 0.96 (0.60–1.52) | - | |
| Severity at the time of study participation (mild) | - | - | |
| moderate | 1.36 (0.81–2.26) | - | |
| severe | 1.71 (0.95–3.09) | - | |
| Severity in general (mild) | - | - | |
| moderate | 2.97 (1.12–7.89) | 3.40 (1.24–9.31) | |
| severe | 3.99 (1.48–10.78) | 4.58 (1.62–12.96) | |
| Social impairment (never or rarely) | 2.02 (1.26–3.23) | 1.77 (1.07–2.94) | |
| Alcohol dependency 3 | Age | 1.01 (0.99–1.03) | - |
| Gender (male) | 0.34 (0.23–0.63) | 0.34 (0.23–0.63) | |
| Duration of psoriasis | 1.01 (1.00–1.03) | - | |
| Currently in medical care (yes) | 1.08 (0.60–1.94) | - | |
| Severity at the time of study participation (mild) | - | - | |
| moderate | 1.71 (0.88–3.31) | - | |
| severe | 1.10 (0.49–2.48) | - | |
| Severity in general (mild) | - | - | |
| moderate | 2.76 (0.82–9.37) | - | |
| severe | 1.86 (0.53–6.57) | - | |
| Social impairment (never or rarely) | 0.79 (0.46–1.33) | - |
References
- Young, K.S. The evolution of Internet addiction. Addict. Behav. 2017, 64, 229–230. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; International Version; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Rumpf, H.-J.; Vermulst, A.A.; Bischof, A.; Kastirke, N.; Gürtler, D.; Bischof, G.; Meerkerk, G.-J.; John, U.; Meyer, C. Occurence of internet addiction in a general population sample: A latent class analysis. Eur. Addict. Res. 2014, 20, 159–166. [Google Scholar] [CrossRef]
- Wartberg, L.; Kriston, L.; Kammerl, R.; Petersen, K.-U.; Thomasius, R. Prevalence of pathological internet use in a representative German sample of adolescents: Results of a latent profile analysis. Psychopathology 2015, 48, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Schielein, M.C.; Tizek, L.; Knobloch, L.; Maaßen, D.; Biedermann, T.; Zink, A. Psoriasis and addictions: Assessing mental health in a cross-sectional study across Germany. under review.
- Michalek, I.M.; Loring, B.; John, S.M. A systematic review of worldwide epidemiology of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Tizek, L.; Schielein, M.C.; Seifert, F.; Biedermann, T.; Böhner, A.; Zink, A. Skin diseases are more common than we think: Screening results of an unreferred population at the Munich Oktoberfest. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Greb, J.E.; Goldminz, A.M.; Elder, J.T.; Lebwohl, M.G.; Gladman, D.D.; Wu, J.J.; Mehta, N.N.; Finlay, A.Y.; Gottlieb, A.B. Psoriasis. Nat. Rev. Dis. Primers 2016, 2, 16082. [Google Scholar] [CrossRef]
- Schuster, B.; Ziehfreund, S.; Albrecht, H.; Spinner, C.D.; Biedermann, T.; Peifer, C.; Zink, A. Happiness in dermatology: A holistic evaluation of the mental burden of skin diseases. J. Eur. Acad. Dermatol. Venereol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Do, Y.K.; Lakhani, N.; Malhotra, R.; Halstater, B.; Theng, C.; Østbye, T. Association between psoriasis and leisure-time physical activity: Findings from the National Health and Nutrition Examination Survey. J. Dermatol. 2015, 42, 148–153. [Google Scholar] [CrossRef]
- Kouris, A.; Platsidaki, E.; Kouskoukis, C.; Christodoulou, C. Psychological parameters of psoriasis. Psychiatriki 2017, 28, 54–59. [Google Scholar] [CrossRef]
- Da Silva, N.; von Stülpnagel, C.; Langenbruch, A.; Danckworth, A.; Augustin, M.; Sommer, R. Disease burden and patient needs and benefits in anogenital psoriasis: Developmental specificities for person-centred healthcare of emerging adults and adults. J. Eur. Acad. Dermatol. Venereol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Schielein, M.C.; Tizek, L.; Schuster, B.; Ziehfreund, S.; Biedermann, T.; Zink, A. Genital psoriasis and associated factors of sexual avoidance—A people-centered cross-sectional study in Germany. Acta Derm Venerol. 2020. [Google Scholar] [CrossRef]
- Auker, L.; Cordingley, L.; Pye, D.R.; Griffiths, C.E.M.; Young, H.S. What are the barriers to physical activity in patients with chronic plaque psoriasis? Br. J. Dermatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Mrowietz, U.; Luck-Sikorski, C.; von Kiedrowski, R.; Schlette, S.; Radtke, M.A.; John, S.M.; Zink, A.; Suthakharan, N.; Sommer, R. Translating the WHA resolution in a member state: Towards a German programme on ’Destigmatization’ for individuals with visible chronic skin diseases. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2202–2208. [Google Scholar] [CrossRef]
- Topp, J.; Andrees, V.; Weinberger, N.A.; Schäfer, I.; Sommer, R.; Mrowietz, U.; Luck-Sikorski, C.; Augustin, M. Strategies to reduce stigma related to visible chronic skin diseases: A systematic review. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2029–2038. [Google Scholar] [CrossRef]
- Koo, J.; Marangell, L.B.; Nakamura, M.; Armstrong, A.; Jeon, C.; Bhutani, T.; Wu, J.J. Depression and suicidality in psoriasis: Review of the literature including the cytokine theory of depression. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1999–2009. [Google Scholar] [CrossRef]
- Zink, A.; Herrmann, M.; Fischer, T.; Lauffer, F.; Garzorz-Stark, N.; Böhner, A.; Spinner, C.D.; Biedermann, T.; Eyerich, K. Addiction: An underestimated problem in psoriasis health care. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1308–1315. [Google Scholar] [CrossRef]
- Michalek, I.M.; Loring, B.; John, S.M. Global Report on Psoriasis; World Health Organization: Geneva, Switzerland, 2016; ISBN 9241565187. [Google Scholar]
- Armstrong, A.W.; Harskamp, C.T.; Dhillon, J.S.; Armstrong, E.J. Psoriasis and smoking: A systematic review and meta-analysis. Br. J. Dermatol. 2014, 170, 304–314. [Google Scholar] [CrossRef]
- Brenaut, E.; Horreau, C.; Pouplard, C.; Barnetche, T.; Paul, C.; Richard, M.-A.; Joly, P.; Le Maître, M.; Aractingi, S.; Aubin, F.; et al. Alcohol consumption and psoriasis: A systematic literature review. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 30–35. [Google Scholar] [CrossRef]
- Takahashi, H.; Iinuma, S.; Tsuji, H.; Honma, M.; Iizuka, H. Biologics are more potent than other treatment modalities for improvement of quality of life in psoriasis patients. J. Dermatol. 2014, 41, 686–689. [Google Scholar] [CrossRef]
- Maroti, M.; Ulff, E.; Wijma, B. Quality of life before and 6 weeks after treatment in a dermatological outpatient treatment unit. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 1081–1085. [Google Scholar] [CrossRef]
- Eissing, L.; Radtke, M.A.; Zander, N.; Augustin, M. Barriers to guideline-compliant psoriasis care: Analyses and concepts. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 569–575. [Google Scholar] [CrossRef]
- Schielein, M.C.; Tizek, L.; Rotter, M.; Konstantinow, A.; Biedermann, T.; Zink, A. Guideline-compliant prescription of biologicals and possible barriers in dermatological practices in Bavaria. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 978–984. [Google Scholar] [CrossRef] [PubMed]
- Schielein, M.C.; Tizek, L.; Seifert, F.; Biedermann, T.; Zink, A. Versorgung von chronisch entzündlichen Hauterkrankungen: Gehen Betroffene zum niedergelassenen Dermatologen? Hautarzt 2019, 70, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, K.; George, A.; Gilson, L. People-centred science: Strengthening the practice of health policy and systems research. Health Res. Policy Syst. 2014, 12, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starfield, B. Is patient-centered care the same as person-focused care? Perm. J. 2011, 15, 63–69. [Google Scholar] [CrossRef]
- Arafa, A.E.; Anzengruber, F.; Mostafa, A.M.; Navarini, A.A. Perspectives of online surveys in dermatology. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 511–520. [Google Scholar] [CrossRef]
- Tizek, L.; Schielein, M.; Rüth, M.; Ständer, S.; Pereira, M.P.; Eberlein, B.; Biedermann, T.; Zink, A. Influence of Climate on Google Internet Searches for Pruritus Across 16 German Cities: Retrospective Analysis. J. Med. Internet Res. 2019, 21, e13739. [Google Scholar] [CrossRef] [Green Version]
- Tizek, L.; Schielein, M.C.; Rüth, M.; Szeimies, R.-M.; Philipp-Dormston, W.G.; Braun, S.A.; Hecker, C.; Eberlein, B.; Biedermann, T.; Zink, A. Interest in Skin Cancer in Urban Populations: A Retrospective Analysis of Google Search Terms in Nine Large German Cities. Acta Derm. Venereol. 2019, 99, 797–804. [Google Scholar] [CrossRef] [Green Version]
- Zink, A.; Schuster, B.; Rüth, M.; Pereira, M.P.; Philipp-Dormston, W.G.; Biedermann, T.; Ständer, S. Medical needs and major complaints related to pruritus in Germany: A 4-year retrospective analysis using Google AdWords Keyword Planner. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Schuster, B.; Ziehfreund, S.; Biedermann, T.; Zink, A. Psoriasis 2.0: Facebook as a source of disease-related information for patients with psoriasis. J. Dtsch. Dermatol. Ges. 2020. [Google Scholar] [CrossRef] [Green Version]
- Wartberg, L.; Petersen, K.-U.; Kammerl, R.; Rosenkranz, M.; Thomasius, R. Psychometric validation of a German version of the compulsive Internet use scale. Cyberpsychology Behav. Soc. Netw. 2014, 17, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Guertler, D.; Rumpf, H.-J.; Bischof, A.; Kastirke, N.; Petersen, K.U.; John, U.; Meyer, C. Assessment of problematic internet use by the Compulsive Internet Use Scale and the Internet Addiction Test: A sample of problematic and pathological gamblers. Eur. Addict. Res. 2014, 20, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Wellbeing Measures in Primary Health Care: The DepCare Project. Available online: http://www.euro.who.int/__data/assets/pdf_file/0016/130750/E60246.pdf (accessed on 7 April 2020).
- Löwe, B.; Spitzer, R.L.; Gräfe, K.; Kroenke, K.; Quenter, A.; Zipfel, S.; Buchholz, C.; Witte, S.; Herzog, W. Comparative validity of three screening questionnaires for DSM-IV depressive disorders and physicians’ diagnoses. J. Affect. Disord. 2004, 78, 131–140. [Google Scholar] [CrossRef]
- Mayfield, D.; McLeod, G.; Hall, P. The CAGE questionnaire: Validation of a new alcoholism screening instrument. Am. J. Psychiatry 1974, 131, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, S.; Kopec, J.A. The CAGE questionnaire for alcohol misuse: A review of reliability and validity studies. Clin. Investig. Med. 2007, 30, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Ramsay, B.; O’Reagan, M. A survey of the social and psychological effects of psoriasis. Br. J. Dermatol. 1988, 118, 195–201. [Google Scholar] [CrossRef]
- Patruno, C.; Napolitano, M.; Balato, N.; Ayala, F.; Megna, M.; Patrì, A.; Cirillo, T.; Balato, A. Psoriasis and skin pain: Instrumental and biological evaluations. Acta Derm. Venereol. 2015, 95, 432–438. [Google Scholar] [CrossRef]
- Eichenberg, C.; Schott, M.; Decker, O.; Sindelar, B. Attachment Style and Internet Addiction: An Online Survey. J. Med. Internet Res. 2017, 19, e170. [Google Scholar] [CrossRef]
- Megna, M.; Gisonni, P.; Napolitano, M.; Dell’Aversano Orabona, G.; Patruno, C.; Ayala, F.; Balato, N. The Effect of Smartphone Addiction on Hand Joints in Psoriatic Patients: An Ultrasound-Based Study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 73–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atzendorf, J.; Rauschert, C.; Seitz, N.-N.; Lochbühler, K.; Kraus, L. The Use of Alcohol, Tobacco, Illegal Drugs and Medicines. Dtsch. Arztebl. Int. 2019, 116, 577–584. [Google Scholar] [CrossRef] [PubMed]


| Total (n = 460) | Psoriasis is Preventing Leisure Activities | p-Value | ||
|---|---|---|---|---|
| Never or Rarely (n = 130) | Sometimes, Frequently, or Always (n = 330) | |||
| Age (years) | ||||
| (Mean, SD) | 45.9 ± 13.7 | 46.7 ± 14.1 | 45.6 ± 13.6 | 0.426 |
| Age group <46 | 222 (48.3%) | 62 (47.7%) | 160 (48.5%) | 0.878 |
| Age group ≥46 | 238 (51.7%) | 68 (52.3%) | 170 (51.5%) | |
| Gender; n (%) | ||||
| Female | 287 (62.4%) | 86 (66.2%) | 201 (60.9%) | 0.296 |
| Male | 173 (37.6%) | 44 (33.8%) | 129 (39.1%) | |
| Duration of psoriasis (years) | ||||
| (Mean, SD) | 21.0 ± 14.7 | 21.9 ± 15.1 | 20.7 ± 14.6 | 0.416 |
| Currently in medical care; n (%) | ||||
| Yes | 355 (77.2%) | 95 (73.1%) | 260 (78.8%) | 0.189 |
| No | 105 (22.8%) | 35 (26.9%) | 70 (21.2%) | |
| Severity at the time of study participation; n (%) | ||||
| Mild | 102 (22.2%) | 47 (36.2%) | 55 (16.7%) | <0.001 |
| Moderate | 253 (55.0%) | 74 (56.9%) | 179 (54.2%) | |
| Severe | 105 (22.8%) | 9 (6.9%) | 96 (29.1%) | |
| Severity in general; n (%) | ||||
| Mild | 37 (8.0%) | 22 (16.9%) | 15 (4.5%) | <0.001 |
| Moderate | 259 (56.3%) | 83 (63.8%) | 176 (53.3%) | |
| Severe | 164 (35.7%) | 25 (19.2%) | 139 (42.1%) | |
| Severity at study participation compared to severity in general; n (%) | ||||
| Worse | 60 (13.0%) | 12 (9.2%) | 48 (14.5%) | 0.225 |
| Equal | 249 (54.1%) | 77 (59.2%) | 172 (52.1%) | |
| Better | 151 (32.8%) | 41 (31.5%) | 110 (33.3%) | |
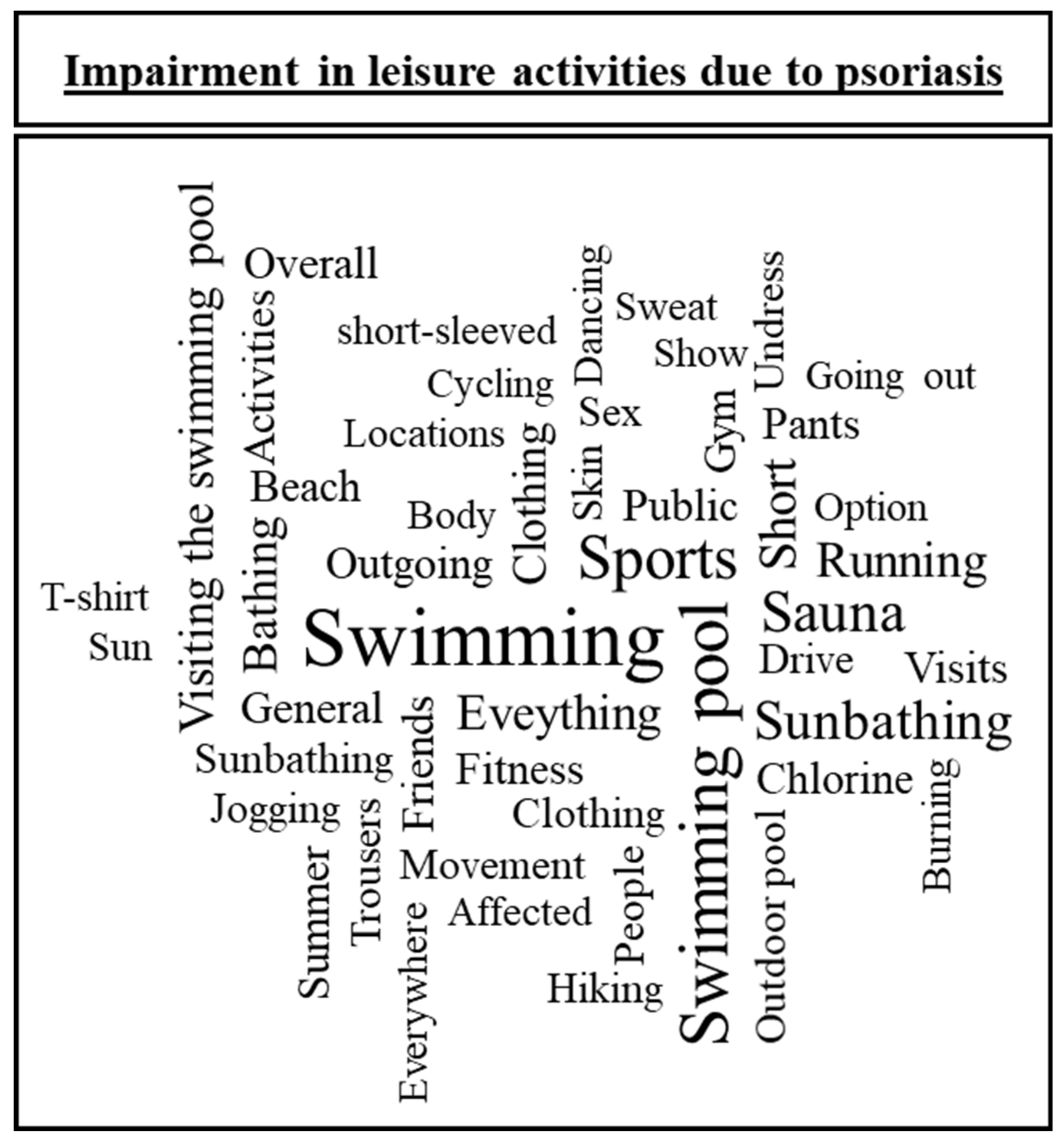
| Category | Count n (%) | Example | Participant (Gender, Age) |
|---|---|---|---|
| Swimming | 273 (67.2%) | “Sauna and swimming pool, but only because of the expected looks on the affected areas” | Woman, 32 years |
| “Swimming in public pools. The chlorine burns the skin”. | Man, 39 years | ||
| Sport | 93 (22.9%) | “I can’t go jogging anymore as my knees were destroyed by psoriatic arthritis”. | Man, 32 years |
| “Running” | Woman, 51 years | ||
| Stigmatization and appearance | 49 (12.1%) | “Whenever I can’t put on anything long enough to hide my disease in public” | Woman, 50 years |
| “Any activity requiring short clothing” | Woman, 21 years | ||
| Sauna | 32 (7.9%) | “Sauna, bathing” | Man, 73 years |
| “Sauna, swimming, nudism” | Woman, 57 years | ||
| Sunbathing | 30 (7.4%) | “Sunbathing at the lake” | Man, 57 years |
| “Sunbathing at the beach” | Man, 30 years | ||
| Movements and walking | 28 (6.9%) | “Going for a walk” | Woman, 52 years |
| “Roughhousing with my son” | Man, 34 years | ||
| Going out and meeting friends | 26 (6.4%) | “Any activity among people is unpleasant because the strong itching leads to scratching and leaving dandruff everywhere”. | Woman, 27 years |
| “Visiting restaurants with friends” | Man, 38 years | ||
| Other | 21 (5.2%) | “Everything you need hands for” | Woman, 67 years |
| “Living” | Man, 38 years |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schielein, M.C.; Tizek, L.; Schuster, B.; Ziehfreund, S.; Liebram, C.; Eyerich, K.; Zink, A. Always Online? Internet Addiction and Social Impairment in Psoriasis across Germany. J. Clin. Med. 2020, 9, 1818. https://doi.org/10.3390/jcm9061818
Schielein MC, Tizek L, Schuster B, Ziehfreund S, Liebram C, Eyerich K, Zink A. Always Online? Internet Addiction and Social Impairment in Psoriasis across Germany. Journal of Clinical Medicine. 2020; 9(6):1818. https://doi.org/10.3390/jcm9061818
Chicago/Turabian StyleSchielein, Maximilian Christian, Linda Tizek, Barbara Schuster, Stefanie Ziehfreund, Claudia Liebram, Kilian Eyerich, and Alexander Zink. 2020. "Always Online? Internet Addiction and Social Impairment in Psoriasis across Germany" Journal of Clinical Medicine 9, no. 6: 1818. https://doi.org/10.3390/jcm9061818
APA StyleSchielein, M. C., Tizek, L., Schuster, B., Ziehfreund, S., Liebram, C., Eyerich, K., & Zink, A. (2020). Always Online? Internet Addiction and Social Impairment in Psoriasis across Germany. Journal of Clinical Medicine, 9(6), 1818. https://doi.org/10.3390/jcm9061818