Temperament and Character Profile and Its Clinical Correlates in Male Patients with Dual Schizophrenia



Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Sociodemographic and Clinical Variables
2.3.2. Temperament and Character Assessment
2.4. Data Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics
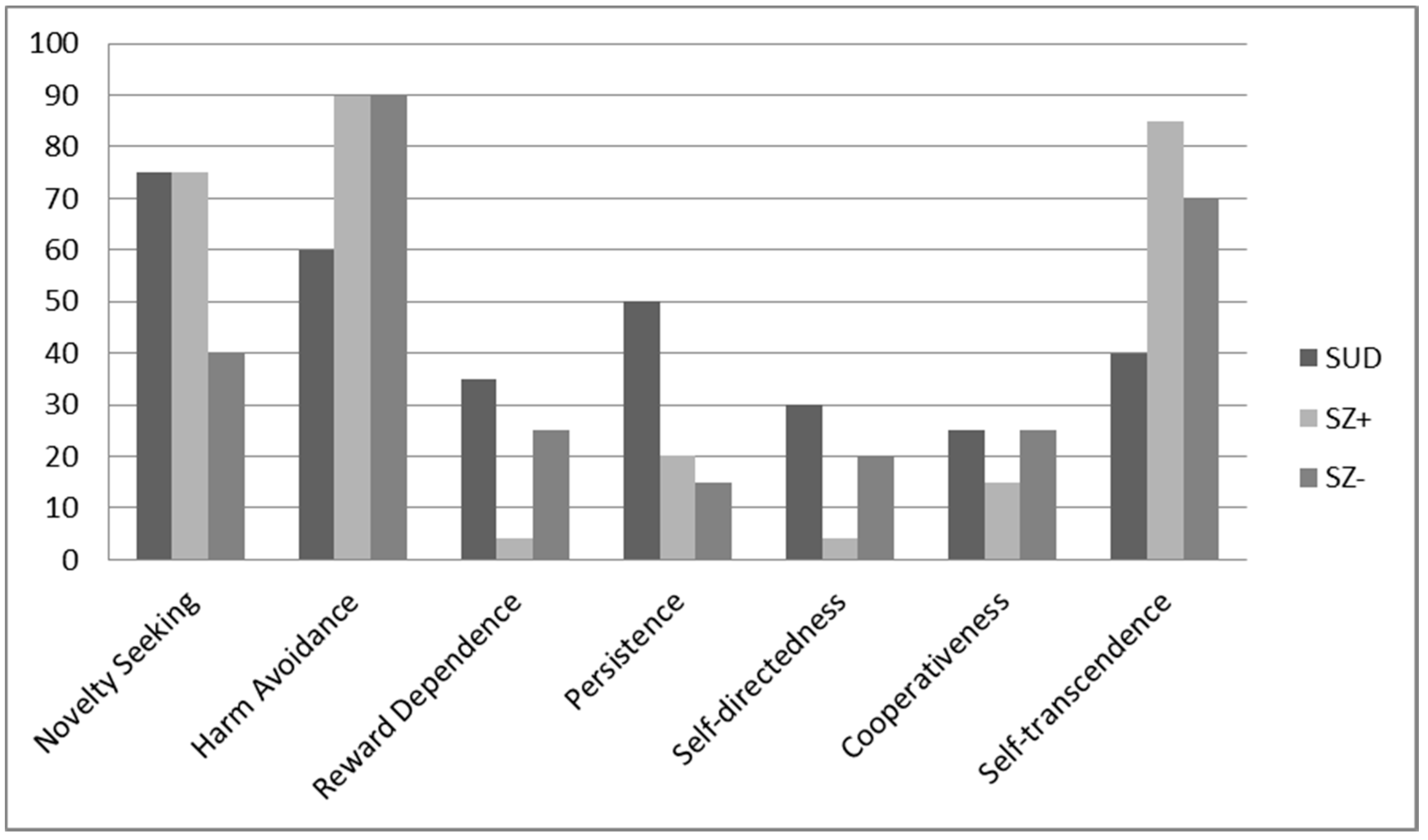
3.2. Personality Dimensions
3.3. Clinical Variates Associated with Personality Dimensions
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Andersen, A.M.; Bienvenu, O.J. Personality and psychopathology. Int. Rev. Psychiatry 2011, 23, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Szerman, N.; Peris, L. Precision Psychiatry and Dual Disorders. J. Dual Diagn. 2019, 14, 237–246. [Google Scholar] [CrossRef] [PubMed]
- European Monitoring Centre for Drug and Addiction (EMCDDA). Informe Europeo Sobre Drogas: Tendencias y Novedades; Oficina de Publicaciones de la Unión Europea: Luxemburgo, 2018; ISBN 978-92-9497-318-4. [Google Scholar] [CrossRef]
- Hunt, G.E.; Large, M.M.; Cleary, M.; Lai, H.M.X.; Saunders, J.B. Prevalence of comorbid substance use in schizophrenia spectrum disorders in community and clinical settings, 1990–2017: Systematic review and meta-analysis. Drug Alcohol Depend. 2018, 191, 234–258. [Google Scholar] [CrossRef] [PubMed]
- European Monitoring Centre for Drug and Addiction (EMCDDA). European Drug Report 2015: Comorbidity of Substance Use and Mental Disorders in Europe; Publications Office of the European Union: Luxembourg, 2019; ISBN 978-92-9168-834-0. [Google Scholar] [CrossRef]
- Green, A.I.; Khokhar, J.Y. Addiction and schizophrenia: A translational perspective. Schizophr. Res. 2018, 194, 1–3. [Google Scholar] [CrossRef]
- Sánchez-Peña, J.F.; Alvarez-Cotoli, P.; Rodríguez-Solano, J.J. Psychiatric disorders associated with alcoholism: 2 year follow-up of treatment. Actas Esp. Psiquiatr. 2012, 40, 129–135. [Google Scholar]
- Jiménez-Castro, L.; Raventós-Vorst, H.; Escamilla, M. Substance use disorder and schizophrenia: Prevalence and sociodemographic characteristics in the Latin American population. Actas Esp. Psiquiatr. 2010, 39, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Marquez-Arrico, J.E.; Adan, A. Personality in patients with substance use disorders according to the co-occurring severe mental illness: A study using the alternative five factor model. Pers. Individ. Differ. 2016, 97, 76–81. [Google Scholar] [CrossRef]
- Schmidt, L.M.; Hesse, M.; Lykke, J. The impact of substance use disorders on the course of schizophrenia-A 15-year follow-up study. Dual diagnosis over 15 years. Schizophr. Res. 2011, 130, 228–233. [Google Scholar] [CrossRef]
- Torrens, M.; Mestre-Pintó, J.I.; Montanari, L.; Vicente, J.; Domingo-Salvany, A. Patología dual: Una perspectiva europea. Adicciones 2017, 29, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Lynn Starr, H.; Bermak, J.; Mao, L.; Rodriguez, S.; Alphs, L. Comparison of long-acting and oral antipsychotic treatment effects in patients with schizophrenia, comorbid substance abuse, and a history of recent incarceration: An exploratory analysis of the PRIDE study. Schizophr. Res. 2018, 194, 39–46. [Google Scholar] [CrossRef]
- Donoghue, K.; Doody, G.A.; Murray, R.M.; Jones, P.B.; Morgan, C.; Dazzan, P.; Hart, J.; Mazzoncini, R.; MacCabe, J.H. Cannabis use, gender and age of onset of schizophrenia: Data from the ÆSOP study. Psychiatry Res. 2014, 215, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Arias, F.; Szerman, N.; Vega, P.; Mesías, B.; Basurte, I. Psicosis y drogas. Estudio Madrid sobre prevalencia de patología dual. Rev. Patol. Dual 2015, 2, 4. [Google Scholar] [CrossRef]
- Benaiges, I.; Serra-Grabulosa, J.M.; Prat, G.; Adan, A. Neuropsychological functioning and age-related changes in schizophrenia and/or cocaine dependence. Psychopharmacol. Biol. Psychiatry 2013, 40, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Togay, B.; Noyan, H.; Tasdelen, R.; Ucok, A. Clinical variables associated with suicide attempts in schizophrenia before and after the first episode. Psychiatry Res. 2015, 229, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Haddock, G.; Eisner, E.; Davies, G.; Coupe, N.; Barrowclough, C. Psychotic symptoms, self-harm and violence in individuals with schizophrenia and substance misuse problems. Schizophr. Res. 2013, 151, 215–220. [Google Scholar] [CrossRef]
- Rubio, G.; Torrens, M.; Calatayud, M.; Haro, G. Modelos Asistenciales en Patología Dual. In Tratado Sobre Patología Dual. Reintegrando la Salud Mental; Haro, G., Bobes, J., Casas, M., Didia, J., Rubio, G., Eds.; MRA Editors: Barcelona, Spain, 2010; pp. 655–668. [Google Scholar]
- Long, E.C.; Aggen, S.H.; Neale, M.C.; Knudsen, G.P.; Krueger, R.F.; South, S.C.; Czajkowski, N.; Nesvåg, R.; Ystrom, E.; Torvik, F.A.; et al. The association between personality disorders with alcohol use and misuse: A population-based twin study. Drug Alcohol Depend. 2017, 174, 171–180. [Google Scholar] [CrossRef] [Green Version]
- Trull, T.J.; Freeman, L.K.; Vebares, T.J.; Choate, A.M.; Helle, A.C.; Wycoff, A.M. Borderline personality disorder and substance use disorders: An updated review. Borderline Personal. Disord. Emot. Dysregulation 2018, 5. [Google Scholar] [CrossRef] [Green Version]
- Santens, E.; Claes, L.; Dierckx, E.; Luyckx, K.; Peuskens, H.; Dom, G. Personality profiles in substance use disorders: Do they differ in clinical symptomatology, personality disorders and coping? Pers. Individ. Differ. 2018, 131, 61–66. [Google Scholar] [CrossRef]
- Zilberman, N.; Yadid, G.; Efrati, Y.; Neumark, Y.; Rassovsky, Y. Personality profiles of substance and behavioral addictions. Addict. Behav. 2018, 82, 174–181. [Google Scholar] [CrossRef]
- Compton, M.T.; Bakeman, R.; Alolayan, Y.; Balducci, P.M.; Bernardini, F.; Broussard, B.; Crisafio, A.; Cristofaro, S.; Amar, P.; Johnson, S.; et al. Personality domains, duration of untreated psychosis, functioning, and symptom severity in first-episode psychosis. Schizophr. Res. 2015, 168, 113–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridgewell, C.; Blackford, J.U.; McHugo, M.; Heckers, S. Personality traits predicting quality of life and overall functioning in schizophrenia. Schizophr. Res. 2017, 182, 19–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Mondragón, S.; Adan, A. Personality in male patients with substance use disorder and/or severe mental illness. Psychiatry Res. 2015, 228, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Marquez-Arrico, J.E.; Río-Martínez, L.; Navarro, J.F.; Prat, G.; Adan, A. Personality profile and clinical correlates of patients with substance use disorder with and without comorbid depression under treatment. Front. Psychiatry 2019, 10, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roncero, C.; Barral, C.; Grau-López, L.; Bos-Cucuruli, E.; Casas, M. Patología dual en esquizofrenia. Protoc. Interv. Patol. Dual 2016, 1–56. [Google Scholar]
- Cloninger, C.R.; Svrakic, D.M.; Przybeck, T.R. A psychobiological model of temperament and character. Arch. Gen. Psychiatry 1993, 50, 975–990. [Google Scholar] [CrossRef] [PubMed]
- Galindo, L.; Pastoriza, F.; Bergé, D.; Mané, A.; Picado, M.; Bulbena, A.; Robledo, P.; Pérez, V.; Vilarroya, O.; Cloninger, C.R. Association between neurological soft signs, temperament and character in patients with schizophrenia and non-psychotic relatives. PeerJ 2016. [Google Scholar] [CrossRef] [Green Version]
- Marquez-Arrico, J.E.; López-Vera, S.; Prat, G.; Adan, A. Temperament and character dimensions in male patients with substance use disorders: Differences relating to psychiatric comorbidity. Psychiatry Res. 2016, 237, 1–8. [Google Scholar] [CrossRef]
- Miskovic, M.; Ravanic, D.; Bankovic, D.; Zivlak-Radulovic, N.; Banjac, V.; Dragisic, T. The risk model of developing schizophrenia based on temperament and character. Psychiatr. Danub. 2018, 30, 57–63. [Google Scholar] [CrossRef]
- Khemiri, L.; Kuja-Halkola, R.; Larsson, H.; Jayaram-Lindström, N. Genetic overlap between impulsivity and alcohol dependence: A large-scale national twin study. Psychol. Med. 2016, 46, 1091–1102. [Google Scholar] [CrossRef]
- Hamdan-Mansour, A.M.; Mahmoud, K.F.; Al Shibi, A.N.; Arabiat, D.H. Impulsivity and sensation-seeking personality traits as predictors of substance use among University students. J. Psychosoc. Nurs. Ment. Health Serv. 2018, 56, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Benotsch, E.G.; Jeffers, A.J.; Snipes, D.J.; Martin, A.M.; Koester, S. The five factor model of personality and the non-medical use of prescription drugs: Associations in a young adult sample. Pers. Individ. Differ. 2013, 55, 852–855. [Google Scholar] [CrossRef]
- Ersche, K.D.; Turton, A.J.; Chamberlain, S.R.; Müller, U.; Bullmore, E.T.; Robbins, T.W. Cognitive dysfunction and anxious-impulsive personality traits are endophenotypes for drug dependence. Am. J. Psychiatry 2012, 169, 926–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valero, S.; Daigre, C.; Rodríguez-Cintas, L.; Barral, C.; Gomà-I-Freixanet, M.; Ferrer, M.; Casas, M.; Roncero, C. Neuroticism and impulsivity: Their hierarchical organization in the personality characterization of drug-dependent patients from a decision tree learning perspective. Compr. Psychiatry 2014, 55, 1227–1233. [Google Scholar] [CrossRef]
- Arenas, M.C.; Aguilar, M.A.; Montagud-Romero, S.; Mateos-García, A.; Navarro-Francés, C.I.; Miñarro, J.; Rodríguez-Arias, M. Influence of the Novelty-Seeking Endophenotype on the Rewarding Effects of Psychostimulant Drugs in Animal Models. Curr. Neuropharmacol. 2015, 14, 87–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedrero Pérez, E.J.; Rojo Mota, G. Diferencias de personalidad entre adictos a sustancias y población general. Estudio con el TCI-R de casos clínicos con controles emparejados. Adicciones 2008, 20, 251–261. [Google Scholar] [CrossRef] [Green Version]
- Evren, C.; Durkaya, M.; Evren, B.; Dalbudak, E.; Cetin, R. Relationship of relapse with impulsivity, novelty seeking and craving in male alcohol-dependent inpatients. Drug Alcohol Rev. 2012, 31, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.; Goudriaan, A.E.; Verdejo-Garcia, A.; Dom, G.; Roeyers, H.; Vanderplasschen, W. Impulsive choice predicts short-term relapse in substance-dependent individuals attending an in-patient detoxification programme. Psychol. Med. 2015, 45, 2083–2093. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Cintas, L.; Daigre, C.; Grau-López, L.; Barral, C.; Pérez-Pazos, J.; Voltes, N.; Braquehais, M.D.; Casas, M.; Roncero, C. Impulsivity and addiction severity in cocaine and opioid dependent patients. Addict. Behav. 2016, 58, 104–109. [Google Scholar] [CrossRef]
- Staiger, P.K.; Dawe, S.; Richardson, B.; Hall, K.; Kambouropoulos, N. Modifying the risk associated with an impulsive temperament: A prospective study of drug dependence treatment. Addict. Behav. 2014, 39, 1676–1681. [Google Scholar] [CrossRef]
- Dvorak, R.D.; Lamis, D.A.; Malone, P.S. Alcohol use, depressive symptoms, and impulsivity as risk factors for suicide proneness among college students. J. Affect. Disord. 2013, 149, 326–334. [Google Scholar] [CrossRef] [Green Version]
- Ávila-Escribano, J.J.; Sánchez-Barba, M.; Álvarez-Pedrero, A.; López-Villarreal, A.; Recio-Pérez, J.; Rodríguez-Rodilla, M.; Fraile-García, E. Capacidad de predicción del inventario de temperamento y carácter de cloninger (TCI-R) en la evolución de los trastornos por uso de alcohol. Adicciones 2016, 28, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Hershberger, A.R.; Um, M.; Cyders, M.A. The relationship between the UPPS-P impulsive personality traits and substance use psychotherapy outcomes: A meta-analysis. Drug Alcohol Depend. 2017, 178, 408–416. [Google Scholar] [CrossRef]
- Andó, B.; Rózsa, S.; Kurgyis, E.; Szkaliczki, A.; Demeter, I.; Szikszay, P.; Demetrovics, Z.; Janka, Z.; Álmos, P.Z. Direct and indirect symptom severity indicators of alcohol dependence and the personality concept of the biosocial model. Subst. Use Misuse 2014, 49, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, R.; Muscatello, M.R.A.; Bruno, A.; Bilardi, F.; De Stefano, C.; Felletti, E.; Isgrò, S.; Micalizzi, V.; Micò, U.; Romeo, A.; et al. Temperament and character dimensions in opiate addicts: Comparing subjects who completed inpatient treatment in therapeutic communities vs. incompleters. Am. J. Drug Alcohol Abuse 2007, 33, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Fresán, A.; León-Ortiz, P.; Robles-García, R.; Azcárraga, M.; Guizar, D.; Reyes-Madrigal, F.; Tovilla-Zárate, C.A.; de la Fuente-Sandoval, C. Personality features in ultra-high risk for psychosis: A comparative study with schizophrenia and control subjects using the Temperament and Character Inventory-Revised (TCI-R). J. Psychiatr. Res. 2015, 61, 168–173. [Google Scholar] [CrossRef]
- Albayrak, Y.; Ekinci, O.; Çayköylü, A. Temperament and character personality profile in relation to suicide attempts in patients with schizophrenia. Compr. Psychiatry 2012, 53, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Vrbova, K.; Prasko, J.; Ociskova, M.; Holubova, M.; Kantor, K.; Kolek, A.; Grambal, A.; Slepecky, M. Suicidality, self-stigma, social anxiety and personality traits in stabilized schizophrenia patients—A cross-sectional study. Neuropsychiatr. Dis. Treat. 2018, 14, 1415–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jetha, M.K.; Goldberg, J.O.; Schmidt, L.A. Temperament and its relation to social functioning in schizophrenia. Int. J. Soc. Psychiatry 2013, 59, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Zhornitsky, S.; Rizkallah, É.; Pampoulova, T.; Chiasson, J.P.; Lipp, O.; Stip, E.; Potvin, S. Sensation-seeking, social anhedonia, and impulsivity in substance use disorder patients with and without schizophrenia and in non-abusing schizophrenia patients. Psychiatry Res. 2012, 200, 237–241. [Google Scholar] [CrossRef]
- Reno, R.M. Personality characterizations of outpatients with schizophrenia, schizophrenia with substance abuse, and primary substance abuse. J. Nerv. Ment. Dis. 2004, 192, 672–681. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects—WMA—The World Medical Association. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 3 March 2020).
- First, M.B.; Gibbon, M. The Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) and the Structured Clinical Interview for DSM-IV Axis II Disorders (SCID-II). In Comprehensive Handbook of Psychological Assessment, Vol. 2: Personality Assessment; John Wiley & Sons: Hoboken, NJ, USA, 2004; pp. 134–143. ISBN 0-471-41612-6. [Google Scholar]
- Hall, R.C.W. Global Assessment of Functioning: A Modified Scale. Psychosomatics 1995, 36, 267–275. [Google Scholar] [CrossRef]
- Peralta Martín, V.; Cuesta Zorita, M.J. Validation of positive and negative symptom scale (PANSS) in a sample of Spanish schizophrenic patients. Actas Luso. Esp. Neurol. Psiquiatr. Cienc. Afines 1994, 22, 171–177. [Google Scholar] [PubMed]
- Gálvez, B.P.; Fernández, L.G.; De Vicente Manzanaro, M.P.; Valenzuela, M.A.O.; Lafuente, M.L. Validación española del drug abuse screening test (DAST-20 y DAST-10). Health Addict./Salud y Drog. 2010, 10, 35–50. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez-Zotes, J.A.; Bayón, C.; Montserrat, C.; Valero, J.; Labad, A.; Cloninger, C.R.; Fernández-Aranda, F. Inventario del Temperamento y el Carácter-Revisado (TCI-R). Baremación y datos normativos en una muestra de población general. Actas Esp. Psiquiatr. 2004, 32, 8–15. [Google Scholar] [PubMed]
- Anusic, I.; Lucas, R.E.; Brent Donnellan, M. Cross-sectional age differences in personality: Evidence from nationally representative samples from Switzerland and the United States. J. Res. Pers. 2012, 46, 116–120. [Google Scholar] [CrossRef]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Adan, A.; Capella, M.D.M.; Prat, G.; Forero, D.A.; Lopez-Vera, S.; Navarro, J.F. Executive functioning in men with schizophrenia and substance use disorders. Influence of lifetime suicide attempts. PLoS ONE 2017, 12, 1–16. [Google Scholar] [CrossRef]
- del Capella, M.M.; Adan, A. The age of onset of substance use is related to the coping strategies to deal with treatment in men with substance use disorder. PeerJ 2017, 3660. [Google Scholar] [CrossRef] [Green Version]
- Prom-Wormley, E.C.; Ebejer, J.; Dick, D.M.; Bowers, M.S. The genetic epidemiology of substance use disorder: A review. Drug Alcohol Depend. 2017, 180, 241–259. [Google Scholar] [CrossRef] [Green Version]
- Belbasis, L.; Köhler, C.A.; Stefanis, N.; Stubbs, B.; van Os, J.; Vieta, E.; Seeman, M.V.; Arango, C.; Carvalho, A.F.; Evangelou, E. Risk factors and peripheral biomarkers for schizophrenia spectrum disorders: An umbrella review of meta-analyses. Acta Psychiatr. Scand. 2018, 137, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Ibarra-Lecue, I.; Mollinedo-Gajate, I.; Meana, J.J.; Callado, L.F.; Diez-Alarcia, R.; Urigüen, L. Chronic cannabis promotes pro-hallucinogenic signaling of 5-HT2A receptors through Akt/mTOR pathway. Neuropsychopharmacology 2018, 43, 2028–2035. [Google Scholar] [CrossRef] [PubMed]
- Jupp, B.; Dalley, J.W. Behavioral endophenotypes of drug addiction: Etiological insights from neuroimaging studies. Neuropharmacology 2014, 76, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Capella, M.D.M.; Benaiges, I.; Adan, A. Neuropsychological performance in polyconsumer men under treatment. Influence of age of onset of substance use. Sci. Rep. 2015, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.Y.; Kang, J.I.; Kim, S.J.; Lee, M.K.; Lee, E.; An, S.K. Temperament and character in individuals at ultra-high risk for psychosis and with first-episode schizophrenia: Associations with psychopathology, psychosocial functioning, and aspects of psychological health. Compr. Psychiatry 2013, 54, 1161–1168. [Google Scholar] [CrossRef]


{kind=link}
| Sociodemographic Variables | SUD (N = 55) | SZ+ (N = 55) | SZ- (N = 55) | Statistical Contrasts |
|---|---|---|---|---|
| Age | 35.78 ± 6.98 | 36.00 ± 8.19 | 39.07 ± 8.72 | F(2,162) = 2.91 |
| Civil status | χ2(2) = 9.75 * | |||
| Single | 58.2% | 76.4% | 83.6% | |
| Married/Stable partner | 25.5% | 12.7% | 9.1% | |
| Separated/Divorced | 16.4% | 10.9% | 7.3% | |
| Living arrangements | χ2(1) = 2.16 | |||
| Alone | 10.9% | 7.3% | 3.6% | |
| Accompanied | 89.1% | 92.7% | 96.4% | |
| Employment situation | χ2(4) = 62.19 *** | |||
| Working | 30.9% | 10.9% | 9.1% | |
| Unemployment compensation | 25.5% | 5.5% | 3.6% | |
| On sick leave | 16.4% | 7.3% | 0% | |
| Disability pension | 12.7% | 61.8% | 81.8% | |
| No income | 14.5% | 14.5% | 5.5% | |
| Years of schooling | 10.38 ± 2.20 | 9.62 ± 2.31 | 9.71 ± 2.15 | F(2,162) = 1.94 |
| Clinical Characteristics | SUD (N = 55) | SZ+ (N = 55) | SZ- (N = 55) | Statistical Contrasts |
|---|---|---|---|---|
| Family history of psychiatric disorders | 21.8% | 29.1% | 34.5% | χ2(1) = 2.20 |
| Family history of SUD | 29.1% | 21.8% | 7.3% | χ2(1) = 8.68 * |
| Suicide attempts | 0.42 ± 0.90 | 1.25 ± 1.82 | 0.69 ± 1.57 | F(2,162) = 4.56 * |
| GAF | 74.50 ± 10.06 | 63.13 ± 11.22 | 59.75 ± 10.15 | F(2,162) = 29.52 *** |
| Number of psychiatric medications | 0.93 ± 1.14 | 3.30 ± 1.68 | 3.22 ± 1.46 | F(2,162) = 47.81 *** |
| Typical antipsychotics | 0% | 22.2% | 25.5% | χ2(1) = 15.80 *** |
| Atypical antipsychotics | 3.6% | 96.3% | 94.5% | χ2(1) = 134.74 *** |
| CPZ equivalent dosage (mg) | 6.06 ± 32.13 | 350.55 ± 281.35 | 617.07 ± 522.12 | F(2,162) = 43.56 *** |
| Interdictor | 20% | 37% | χ2(1) = 3.89 * | |
| Medical disease comorbidity | 0.47 ± 0.69 | 0.53 ± 0.77 | 0.64 ± 0.80 | F(2,162) = 0.67 |
| Onset age of SZ | 23.35 ± 6.96 | 23.65 ± 6.71 | t(1,108) = 0.237 | |
| Duration of SZ (years) | 12.65 ± 8.01 | 15.42 ± 9.30 | t(1,108) = 1.67 | |
| PANSS scores | ||||
| Positive symptoms | 11.83 ± 5.70 | 10.30 ± 4.19 | t(1,108) = 1.46 | |
| Negative symptoms | 15.58 ± 7.39 | 14.18 ± 7.40 | t(1,108) = 0.89 | |
| General psychopathology | 31.10 ± 10.91 | 24.70 ± 9.01 | t(1,108) = 2.99 ** | |
| Onset age of SUD | 20.55 ± 7.24 | 17.60 ± 5.65 | t(1,108) = 2.38 * | |
| Duration of SUD (years) | 14.61 ± 8.94 | 17.85 ± 8.03 | t(1,108) = 2.00 * | |
| Number of substances used | 2.93 ± 1.61 | 3.62 ± 1.75 | t(1,108) = 2.16 * | |
| Main substance of dependence | χ2(4) = 6.66 | |||
| Cocaine | 12.7% | 10.9% | ||
| Alcohol | 9.1% | 12.7% | ||
| Alcohol + Cocaine | 27.3% | 9.1% | ||
| Polydrug use | 50.9% | 67.3% | ||
| Type of substances used a | ||||
| Cocaine | 89.10% | 92.70% | χ2(1) = 0.44 | |
| Alcohol | 80.00% | 76.0% | χ2(1) = 0.21 | |
| Cannabis | 52.70% | 76.40% | χ2(1) = 6.71 ** | |
| Psychodysleptics | 27.30% | 40.00% | χ2(1) = 1.99 | |
| Opioids | 14.50% | 25.50% | χ2(1) = 2.05 | |
| Sedatives | 1.80% | 16.40% | χ2(1) = 7.04 ** | |
| Abstinence period (months) | 7.55 ± 2.61 | 6.57 ± 3.64 | t(1,108) = 1.62 | |
| Number of relapses | 0.82 ± 1.48 | 2.25 ± 2.97 | t(1,108) = 3.21 ** | |
| DAST-20 (severity of addiction) | 13.05 ± 3.47 | 13.44 ± 2.86 | t(1,108) = 0.54 |
| TCI-R Dimensions | SUD (N = 55) | SZ+ (N = 55) | SZ- (N = 55) | F(2,161) | ηp2 | Bonferroni Post-Hoc Analyses |
|---|---|---|---|---|---|---|
| Temperament | ||||||
| Novelty Seeking | 106.88 ± 1.86 | 106.06 ± 1.86 | 96.23 ± 1.88 | 9.86 *** | 0.11 | SUD,SZ+ > SZ- |
| Harm Avoidance | 95.27 ± 2.60 | 112.12 ± 2.60 | 111.18 ± 2.62 | 13.22 *** | 0.14 | SZ+,SZ- > SUD |
| Reward Dependence | 97.88 ± 2.14 | 91.50 ± 2.14 | 95.70 ± 2.16 | 2.31 | 0.03 | |
| Persistence | 113.48 ± 2.66 | 103.45 ± 2.65 | 99.38 ± 2.68 | 7.38 *** | 0.08 | SZ+,SZ -< SUD |
| Character | ||||||
| Self-directedness | 137.82 ± 3.08 | 116.54 ± 3.08 | 134.64 ± 3.11 | 13.90 *** | 0.15 | SZ+ < SZ-,SUD |
| Cooperativeness | 130.75 ± 2.44 | 123.24 ± 2.43 | 131.40 ± 2.46 | 3.46 | 0.04 | |
| Self-transcendence | 58.66 ± 2.20 | 77.26 ± 2.20 | 69.77 ± 2.22 | 18.19 *** | 0.18 | SZ+,SZ- > SUD |
| TCI-R Dimensions | SUD (N = 55) | SZ+ (N = 55) | SZ- (N = 55) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| R2 Adjusted | IV | β Standardized | R2 Adjusted | IV | β Standardized | R2 Adjusted | IV | β Standardized | |
| Temperament | |||||||||
| Novelty Seeking | 0.133 | Onset age of SUD | −0.386 ** | ||||||
| Harm Avoidance | 0.117 | PANSS_GP | 0.373 * | 0.091 | PANSS_P | 0.331* | |||
| Reward Dependence | 0.249 | GAF | 0.513 *** | 0.187 | GAFPANSS_N | 0.360 ** −0.285 * | |||
| Character | |||||||||
| Self-directedness | 0.313 | Abstinence period (months) | 0.370 * −0.332 * | 0.161 | PANSS_GP | −0.421 ** | |||
| PANSS_GP | |||||||||
| Cooperativeness | 0.282 | Number of relapses | −0.412 *** 0.343 ** 0.249 * | 0.228 | PANSS_GP | −0.494 *** | |||
| Duration of SZ (years) | |||||||||
| Age of SUD onset | |||||||||
| Self-transcendence | 0.084 | PANSS_P | 0.327 * | 0.117 | PANSS_GP | 0.441 *** | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Río-Martínez, L.; Marquez-Arrico, J.E.; Prat, G.; Adan, A. Temperament and Character Profile and Its Clinical Correlates in Male Patients with Dual Schizophrenia. J. Clin. Med. 2020, 9, 1876. https://doi.org/10.3390/jcm9061876
Río-Martínez L, Marquez-Arrico JE, Prat G, Adan A. Temperament and Character Profile and Its Clinical Correlates in Male Patients with Dual Schizophrenia. Journal of Clinical Medicine. 2020; 9(6):1876. https://doi.org/10.3390/jcm9061876
Chicago/Turabian StyleRío-Martínez, Laura, Julia E. Marquez-Arrico, Gemma Prat, and Ana Adan. 2020. "Temperament and Character Profile and Its Clinical Correlates in Male Patients with Dual Schizophrenia" Journal of Clinical Medicine 9, no. 6: 1876. https://doi.org/10.3390/jcm9061876
APA StyleRío-Martínez, L., Marquez-Arrico, J. E., Prat, G., & Adan, A. (2020). Temperament and Character Profile and Its Clinical Correlates in Male Patients with Dual Schizophrenia. Journal of Clinical Medicine, 9(6), 1876. https://doi.org/10.3390/jcm9061876