Is There a Bidirectional Association between Polycystic Ovarian Syndrome and Periodontitis? A Systematic Review and Meta-analysis






Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Focused Question and Eligibility Criteria
- “Does PCOS have an effect on the healthy periodontium?”
- “Does PCOS influence periodontal clinical characteristics of Periodontitis?
- “Does Periodontitis influence clinical characteristics of PCOS?”
- Female patients without PD (Patients-P); PCOS (Exposure-I); No PCOS (Comparison-C); periodontal probing depth (PPD), clinical attachment loss (CAL), bleeding on probing (BoP) levels (Outcome-O)
- Female patients with PD (Patients-P); PCOS (Exposure-I); No PCOS (Comparison-C); PPD, CAL, BoP levels (Outcome-O)
- Female patients with PD (Patients-P); PCOS (Exposure-I); No PCOS (Comparison-C); endocrine outcomes (Ferriman–Gallwey score, free androgen index, dehydroepiandrosterone sulfate (DHEAS), free testosterone and total testosterone levels); glycemic (fasting blood insulin, fasting blood glucose, homeostatic model assessment (HOMA-IR)); and physical (waist-to-hip ratio (WHR)) outcomes - O
2.3. Search Strategy
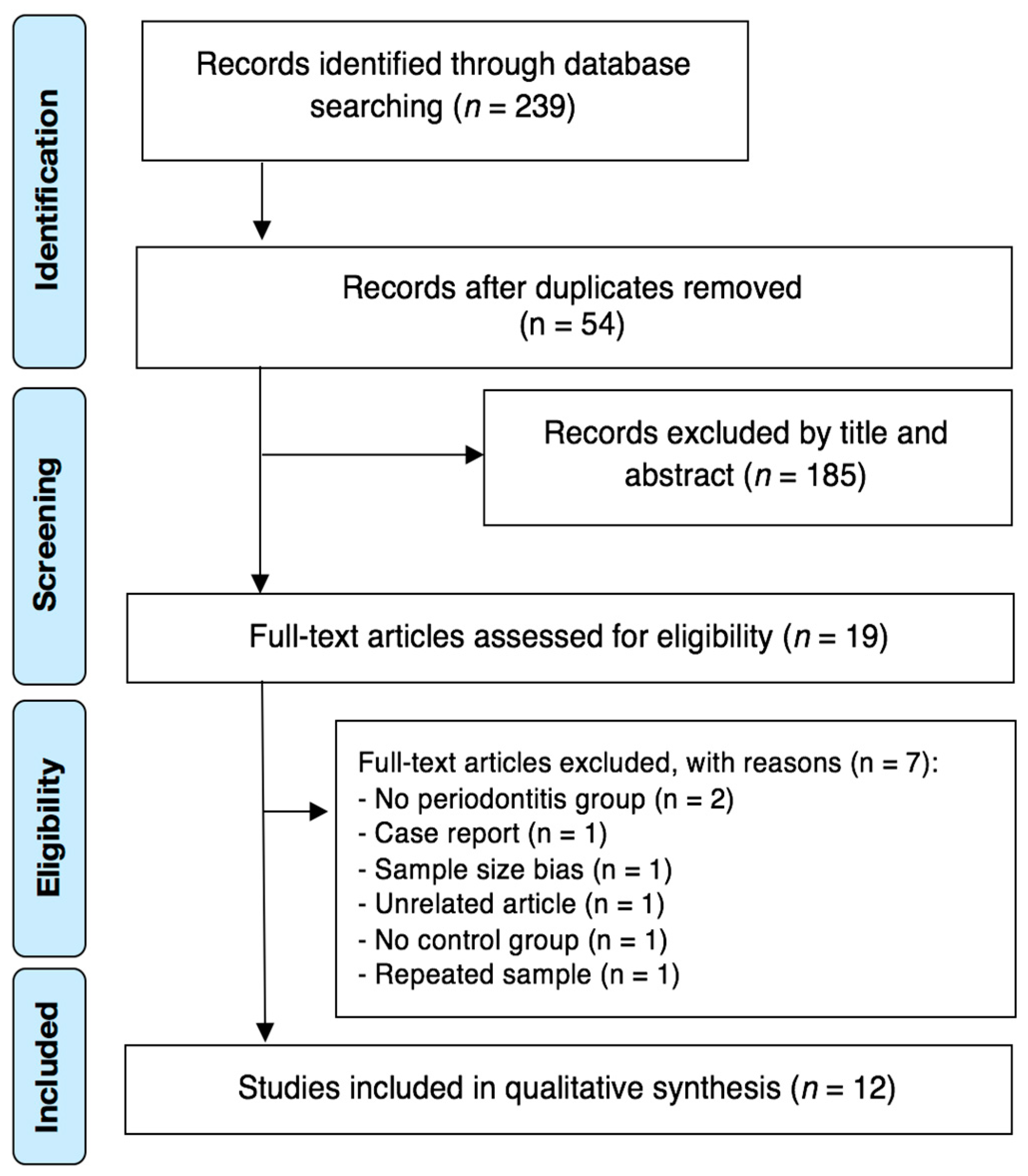
2.4. Study Processs
2.5. Risk of Bias (RoB) in Individual Studies
2.6. Statistical Analysis
2.7. Strength of Recommendation
3. Results
3.1. Characteristics of Included Studies
3.2. Methodological Quality
3.3. Methodological Quality
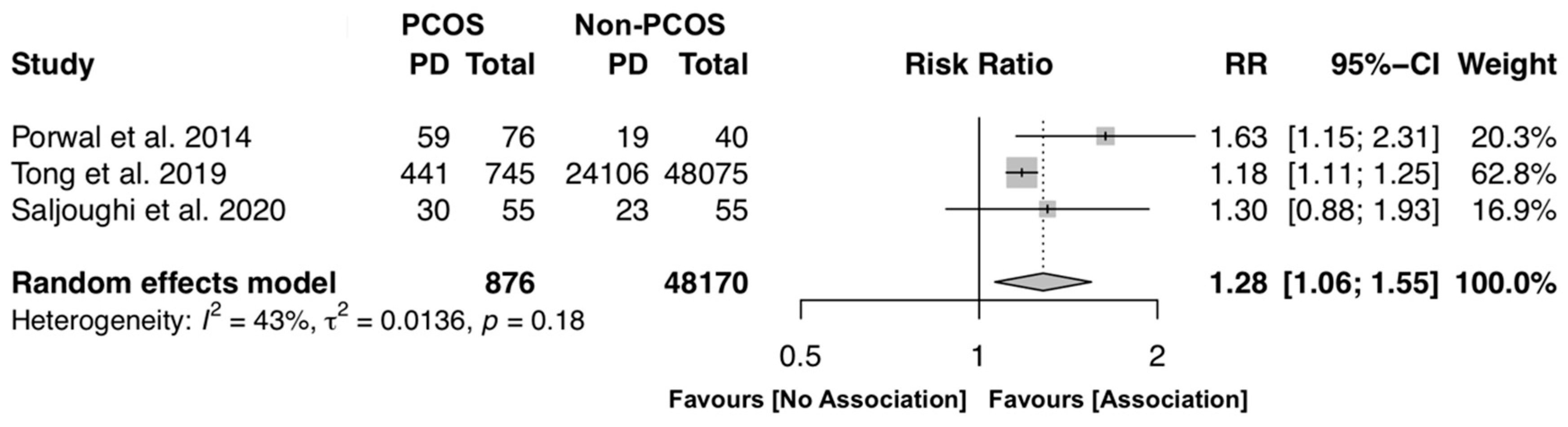
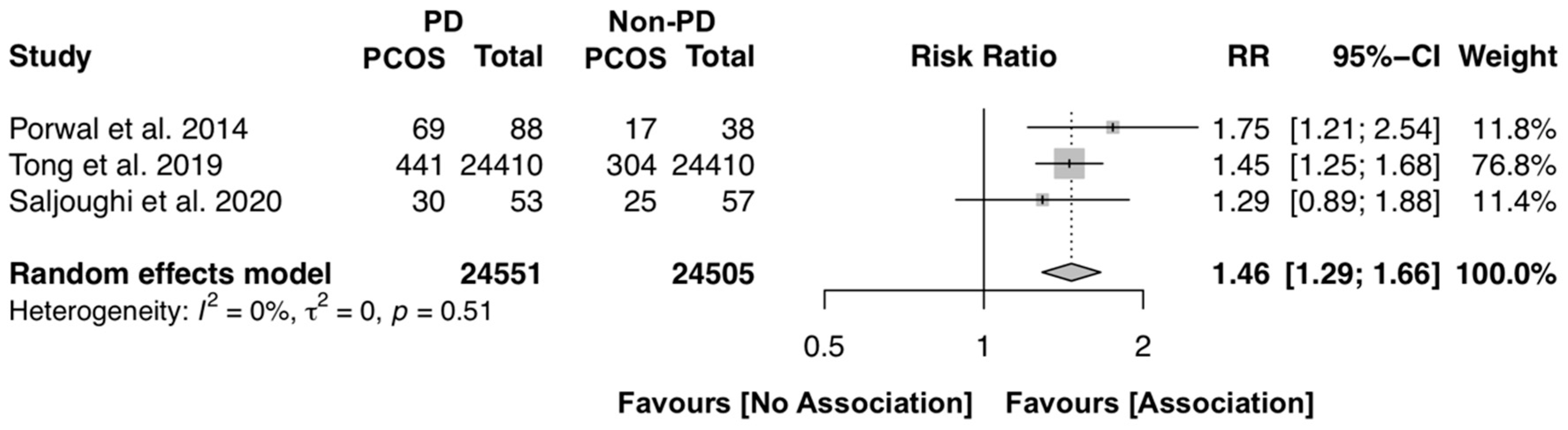
3.3.1. Bidirectional Association between Polycystic Ovarian Syndrome and Periodontitis
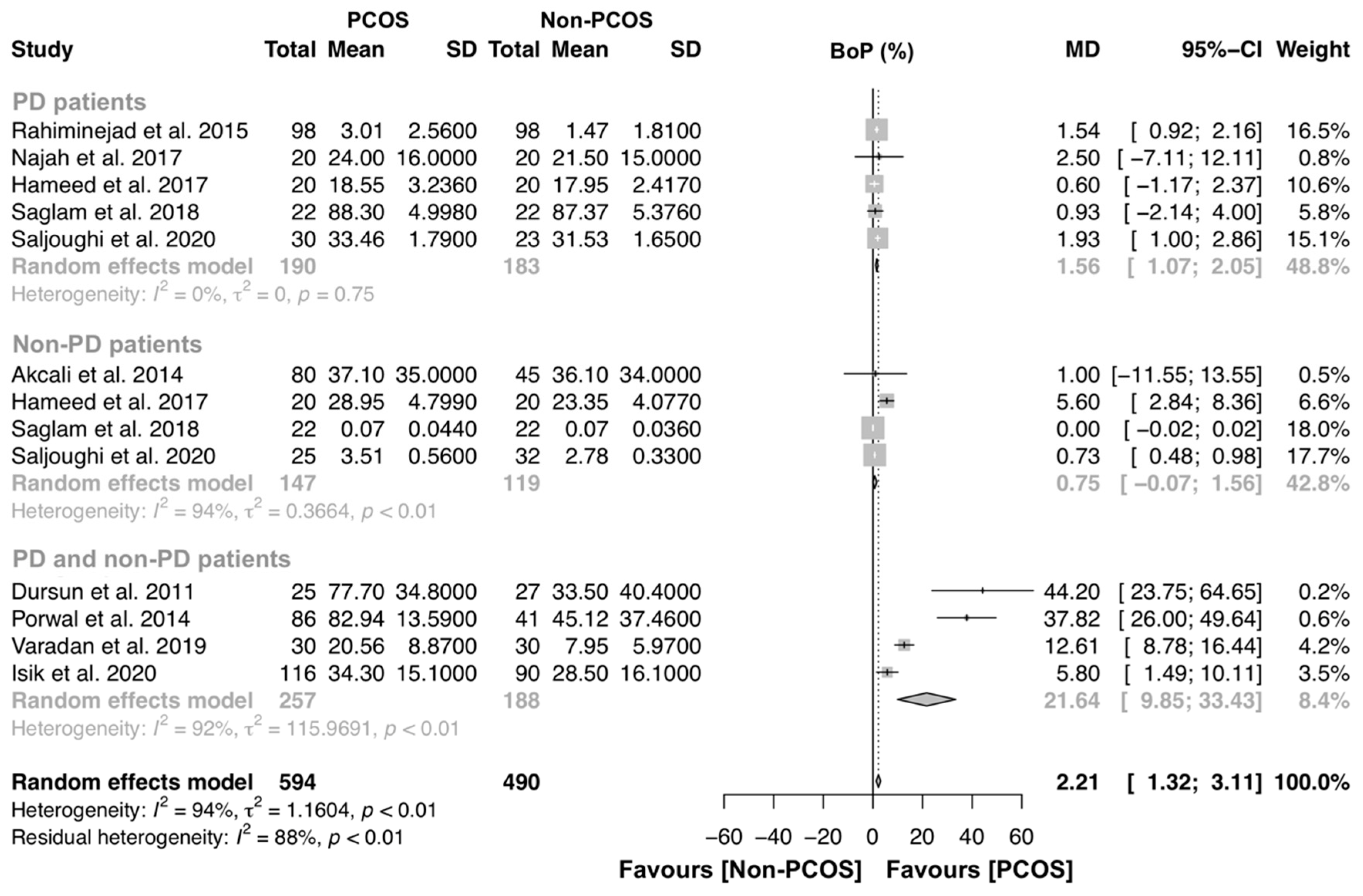
3.3.2. PCOS Effect on the Gingival Inflammation
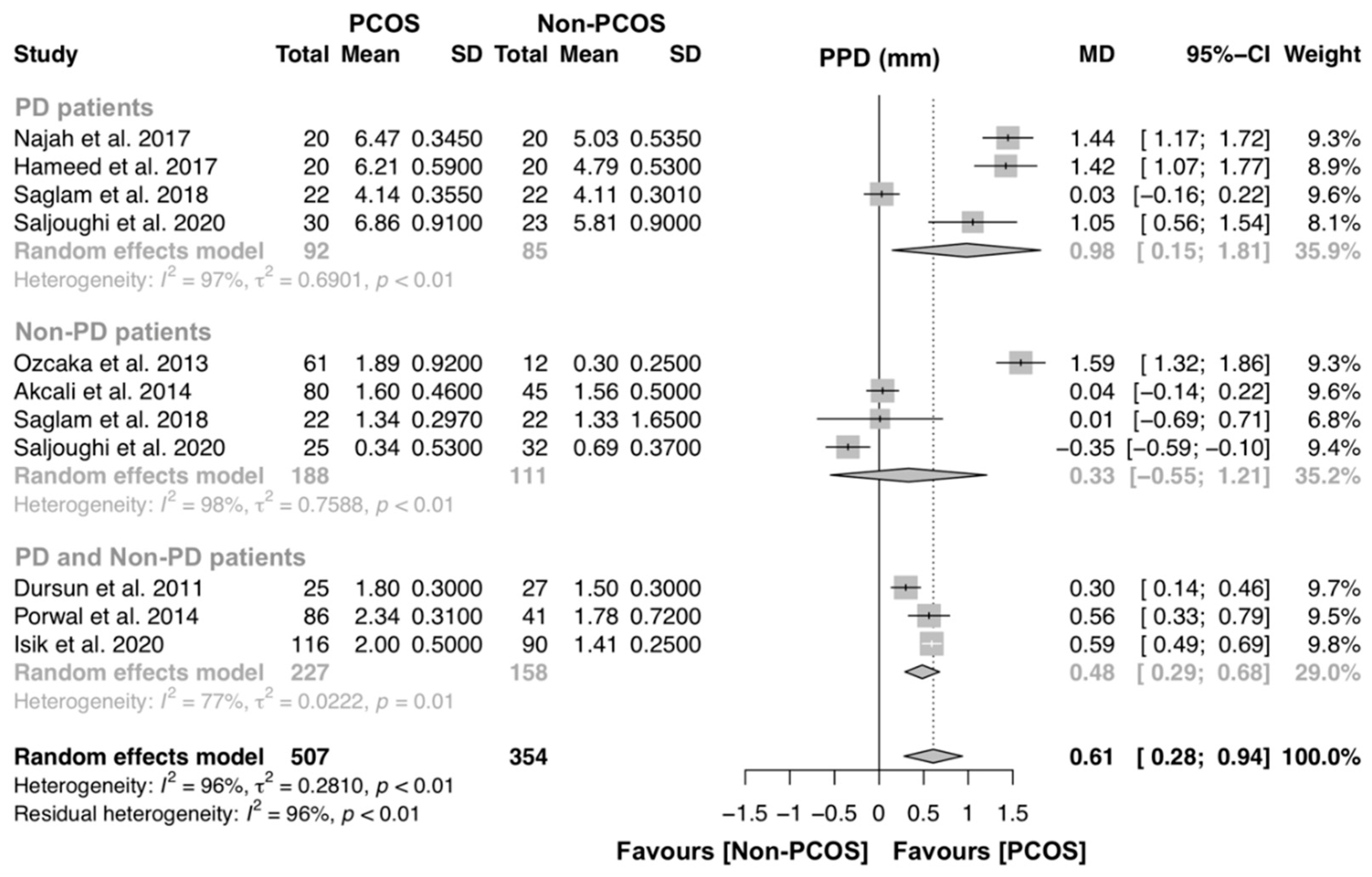
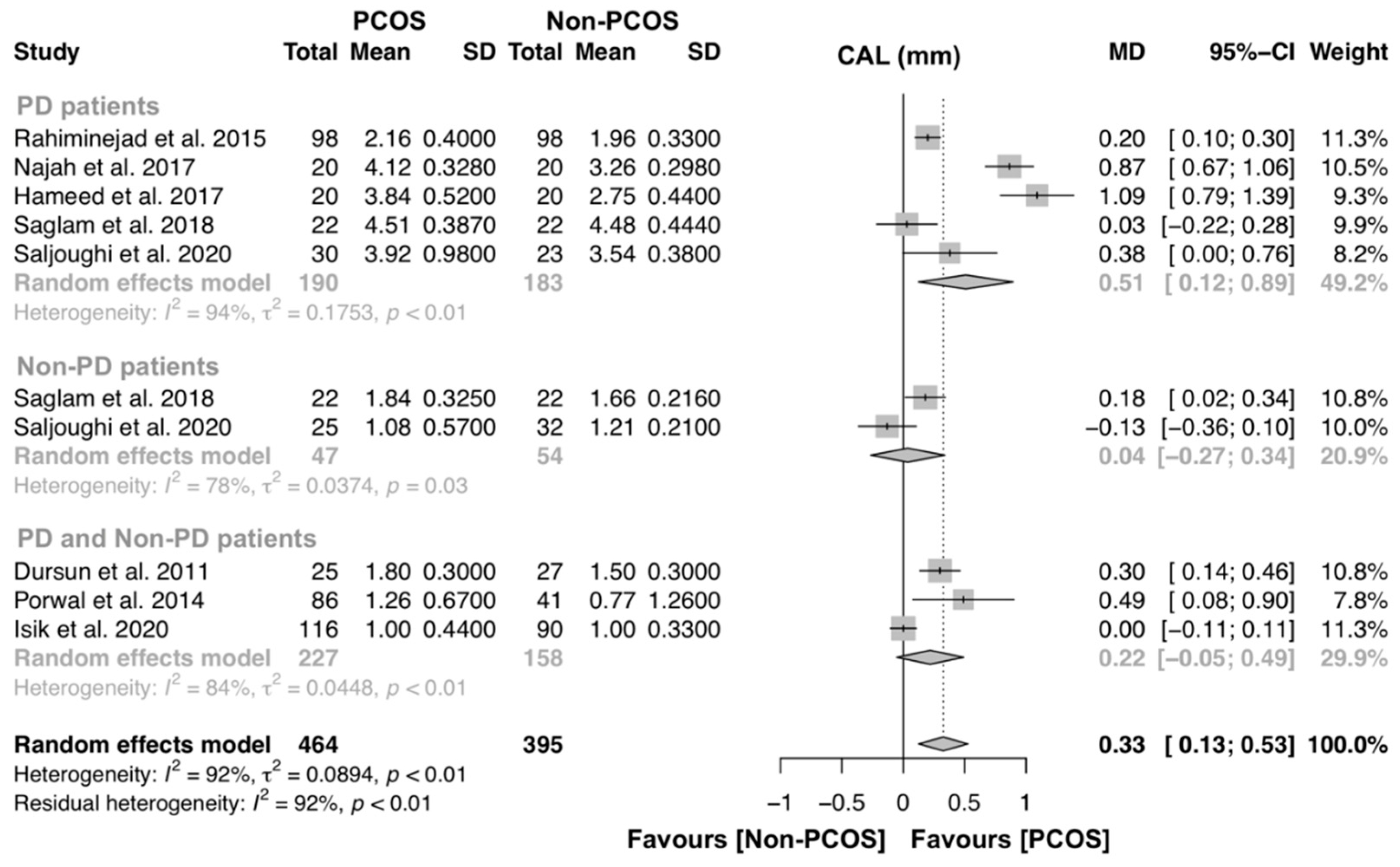
3.3.3. PCOS effect on Periodontal Structure Loss
3.3.4. Additional Analyses
4. Discussion
4.1. Summary of Main Findings and Quality of The Evidence
4.2. Strengths and Potential Limitations
4.3. Interpretation and Clinical Implications
4.4. Research Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Azziz, R. PCOS in 2015: New insights into the genetics of polycystic ovary syndrome. Nat. Rev. Endocrinol. 2016, 12, 74. [Google Scholar] [CrossRef] [PubMed]
- Dumesic, D.A.; Oberfield, S.E.; Stener-Victorin, E.; Marshall, J.C.; Laven, J.S.; Legro, R.S. Scientific statement on the diagnostic criteria, epidemiology, pathophysiology, and molecular genetics of polycystic ovary syndrome. Endocr. Rev. 2015, 36, 487–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwood, E.A.; Huddleston, H.G. Insulin resistance in polycystic ovary syndrome: Concept versus cutoff. Fertil. Steril. 2019, 112, 827–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hull, M.G.R. Epidemiology of infertility and polycystic ovarian disease: Endocrinological and demographic studies. Gynecol. Endocrinol. 1987, 1, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, L.; Saul, S.R.; Copperman, A.B.; Hammerstad, S.S.; Yi, Z.; Zhang, W.; Tomer, Y.; Kase, N. Intrauterine reprogramming of the polycystic ovary syndrome: Evidence from a pilot study of cord blood global methylation analysis. Front. Endocrinol. (Lausanne) 2017, 8, 352. [Google Scholar] [CrossRef] [Green Version]
- Macut, D.; Bjekić-Macut, J.; Rahelić, D.; Doknić, M. Insulin and the polycystic ovary syndrome. Diabetes Res. Clin. Pract. 2017, 130, 163–170. [Google Scholar] [CrossRef]
- McCartney, C.R.; Marshall, J.C. Polycystic ovary syndrome. N. Engl. J. Med. 2016, 375, 54–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, R.J.; Dewailly, D.; Legro, R.S.; Hickey, T.E. Polycystic ovary syndrome. Lancet 2007, 370, 685–697. [Google Scholar] [CrossRef] [Green Version]
- Kellesarian, S.V.; Malignaggi, V.R.; Kellesarian, T.V.; Al-Kheraif, A.A.; Alwageet, M.M.; Malmstrom, H.; Romanos, G.E.; Javed, F. Association between periodontal disease and polycystic ovary syndrome: A systematic review. Int. J. Impot. Res. 2017, 29, 89–95. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, 162–170. [Google Scholar] [CrossRef]
- Darveau, R.P. Periodontitis: A polymicrobial disruption of host homeostasis. Nat. Rev. Microbiol. 2010, 8, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Dawson, D.; Emecen-Huja, P.; Nagarajan, R.; Howard, K.; Grady, M.E.; Thompson, K.; Peyyala, R.; Al-Attar, A.; Lethbridge, K.; et al. The periodontal war: Microbes and immunity. Periodontology 2000 2017, 75, 52–115. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Schuster, J.L.; Stevens, J.; Dawson, D.; Kryscio, R.J.; Lin, Y.; Thomas, M.V.; Miller, C.S. Patterns of salivary analytes provide diagnostic capacity for distinguishing chronic adult periodontitis from health. J. Clin. Immunol. 2013, 33, 271–279. [Google Scholar] [CrossRef]
- Dursun, E.; Akaln, F.A.; Güncü, G.N.; Çnar, N.; Aksoy, D.Y.; Tözüm, T.F.; Kilinc, K.; Yildiz, B.O. Periodontal disease in polycystic ovary syndrome. Fertil. Steril. 2011, 95, 320–323. [Google Scholar] [CrossRef]
- Porwal, S.; Tewari, S.; Sharma, R.K.; Singhal, S.R.; Narula, S.C. Periodontal Status and High-Sensitivity C-Reactive Protein Levels in Polycystic Ovary Syndrome with and Without Medical Treatment. J. Periodontol. 2014, 85, 1380–1389. [Google Scholar] [CrossRef] [PubMed]
- Rahiminejad, M.E.; Moaddab, A.; Zaryoun, H.; Rabiee, S.; Moaddab, A.; Khodadoustan, A. Comparison of prevalence of periodontal disease in women with polycystic ovary syndrome and healthy controls. Dent. Res. J. (Isfahan) 2015, 12, 507–512. [Google Scholar]
- Saglam, E.; Canakcı, C.F.; Sebin, S.O.; Saruhan, N.; Ingec, M.; Canakcı, H.; Sezer, U. Evaluation of Oxidative Status in Patients With Chronic Periodontitis and Polycystic Ovary Syndrome: A Cross-Sectional Study. J. Periodontol. 2018, 89, 76–84. [Google Scholar] [CrossRef]
- Tong, C.; Wang, Y.H.; Yu, H.C.; Chang, Y.C. Increased Risk of Polycystic Ovary Syndrome in Taiwanese Women with Chronic Periodontitis: A Nationwide Population-Based Retrospective Cohort Study. J. Women’s Health 2019, 28, 1436–1441. [Google Scholar] [CrossRef]
- Varadan, M.; Gopalkrishna, P.; Bhat, P.V.; Kamath, S.U.; Krithishree, S.; Thriveni, K.G.; Kumar, S. Influence of polycystic ovary syndrome on the periodontal health of Indian women visiting a secondary health care centre. Clin. Oral Investig. 2019, 23, 3249–3255. [Google Scholar] [CrossRef]
- Varghese, A.; Balu, P.; Saravanakumar, R.; Muthu, J.; Vineela, K. Salivary interleukin-6 levels among polycystic ovary syndrome patients with and without chronic periodontitis—A comparative study. Contemp. Clin. Dent. 2019, 10, 498–501. [Google Scholar] [PubMed]
- Saljoughi, F.; Nasri, K.; Bayani, M. Gingival crevicular fluid levels of visfatin in patients with chronic periodontitis and polycystic ovary syndrome. Obstet. Gynecol. Sci. 2020, 63, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Işık, Y.; Telatar, G.Y.; Neşelioğlu, S.; Biçer, C.; Gürlek, B. Evaluation of periodontal status in different phenotypes of polycystic ovary syndrome in untreated patients of early reproductive age: A case-control study. J. Obstet. Gynaecol. Res. 2020, 46, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Tewari, S.; Narula, S.C.; Singhal, S.R.; Sharma, R.K. Effect of Non-Surgical Periodontal Therapy Along with Myo-Inositol on High-Sensitivity C-Reactive Protein and Insulin Resistance in Women With Polycystic Ovary Syndrome and Chronic Periodontitis: A Randomized Controlled Trial. J. Periodontol. 2017, 88, 999–1011. [Google Scholar]
- Márquez-Arrico, C.F.; Silvestre-Rangil, J.; Gutiérrez-Castillo, L.; Martinez-Herrera, M.; Silvestre, F.J.; Rocha, M. Association between periodontal disease and polycystic ovary syndrome: A systematic review. J. Clin. Med. 2020, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Farrok, F.; Ng, K.T.; Nuzaim, M.; Koh, W.J.; Teoh, W.Y. Association of Periodontal Disease and Polycystic Ovarian Syndrome: A Systematic Review and Meta-analysis with Trial Sequential Analysis. Open Dent. J. 2019, 13, 478–487. [Google Scholar] [CrossRef] [Green Version]
- Higgins, P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, 4th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- OpenGrey. Available online: http://www.opengrey.eu (accessed on 1 June 2020).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Schwarzer, G.; Carpenter, J.R.; Rücker, G. Meta-Analysis with R; Springer: Cham, Switzerland, 2015; ISBN 9783319214153. [Google Scholar]
- Schwarzer, G. meta: An R Package for Meta-Analysis. R News 2007, 7, 40–45. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Newman, M.G.; Weyant, R.; Hujoel, P. JEBDP Improves Grading System and Adopts Strength of Recommendation Taxonomy Grading (SORT) for Guidelines and Systematic Reviews. J. Evid. Based. Dent. Pract. 2007, 7, 147–150. [Google Scholar] [CrossRef]
- Najah, A.; Salman, S.A.; Akram, H.M.; Ahmed, M.A.A.; Ameer, L.A.A.; Khairi, A.W.A. Measurement of serum Superoxide dismutase levels in women with polycystic ovarian syndrome and chronic periodontitis. J. Baghdad Coll. Dent. 2017, 29, 76–81. [Google Scholar] [CrossRef]
- Hameed, D.J.; Ahmend, M.A.-A. Evaluation of Serum Homocysteine and Nitric Oxide Levels in Women with Polycystic Ovarian Syndrome and Periodontal Diseases. Tikrit J. Dent. Sci. 2017, 5, 57–65. [Google Scholar]
- Özçaka, Ö.; Buduneli, N.; Ceyhan, B.O.; Akcali, A.; Hannah, V.; Nile, C.; Lappin, D.F. Is Interleukin-17 Involved in the Interaction Between Polycystic Ovary Syndrome and Gingival Inflammation? J. Periodontol. 2013, 84, 1827–1837. [Google Scholar] [CrossRef] [PubMed]
- Akcalı, A.; Bostanci, N.; Özçaka, Ö.; Gümüş, P.; Öztürk-Ceyhan, B.; Tervahartiala, T.; Husu, H.; Buduneli, N.; Sorsa, T.; Belibasakis, G.N. Gingival Inflammation and Salivary or Serum Granulocyte-Secreted Enzymes in Patients with Polycystic Ovary Syndrome. J. Periodontol. 2017, 88, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Escobar-Morreale, H.F.; Luque-Ramírez, M.; González, F. Circulating inflammatory markers in polycystic ovary syndrome: A systematic review and metaanalysis. Fertil. Steril. 2011, 95, 1048–1058. [Google Scholar] [CrossRef] [Green Version]
- Özçaka, Ö.; Ceyhan, B.Ö.; Akcali, A.; Biçakci, N.; Lappin, D.F.; Buduneli, N. Is There an Interaction Between Polycystic Ovary Syndrome and Gingival Inflammation? J. Periodontol. 2012, 83, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontology 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [Green Version]
- D’Aiuto, F.; Gkranias, N.; Bhowruth, D.; Khan, T.; Orlandi, M.; Suvan, J.; Masi, S.; Tsakos, G.; Hurel, S.; Hingorani, A.D.; et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: A 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 954–965. [Google Scholar] [CrossRef]
- The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, 149–161. [Google Scholar] [CrossRef] [Green Version]
- Botelho, J.; Machado, V.; Proença, L.; Mendes, J.J. The 2018 periodontitis case definition improves accuracy performance of full-mouth partial diagnostic protocols. Sci. Rep. 2020, in press. [Google Scholar] [CrossRef]
- Graetz, C.; Mann, L.; Krois, J.; Sälzer, S.; Kahl, M.; Springer, C.; Schwendicke, F. Comparison of periodontitis patients’ classification in the 2018 versus 1999 classification. J. Clin. Periodontol. 2019, 46, 908–917. [Google Scholar] [CrossRef]
- Rosenfield, R.L.; Ehrmann, D.A. The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr. Rev. 2016, 37, 467–520. [Google Scholar] [CrossRef]
- Legro, R.S.; Dodson, W.C.; Kris-Etherton, P.M.; Kunselman, A.R.; Stetter, C.M.; Williams, N.I.; Gnatuk, C.L.; Estes, S.J.; Fleming, J.; Allison, K.C.; et al. Randomized controlled trial of preconception interventions in infertile women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2015, 100, 4048–4058. [Google Scholar] [CrossRef] [PubMed]
- Turkmen, S.; Ahangari, A.; Bäckstrom, T. Roux-en-Y Gastric Bypass Surgery in Patients with Polycystic Ovary Syndrome and Metabolic Syndrome. Obes. Surg. 2016, 26, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Brewer, H.B.; Cleeman, J.I.; Smith, S.C.; Lenfant, C. Definition of Metabolic Syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference on Scientific Issues Related to Definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunaif, A.; Segal, K.R.; Futterweit, W.; Dobrjansky, A. Profound peripheral insulin resistance, independent of obesity, in polycystic ovary syndrome. Diabetes 1989, 38, 1165–1174. [Google Scholar] [CrossRef]
- Lewy, V.D.; Danadian, K.; Witchel, S.F.; Arslanian, S. Early metabolic abnormalities in adolescent girls with polycystic ovarian syndrome. J. Pediatr. 2001, 138, 38–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeUgarte, C.M.; Bartolucci, A.A.; Azziz, R. Prevalence of insulin resistance in the polycystic ovary syndrome using the homeostasis model assessment. Fertil. Steril. 2005, 83, 1454–1460. [Google Scholar] [CrossRef]
- Stepto, N.K.; Cassar, S.; Joham, A.E.; Hutchison, S.K.; Harrison, C.L.; Goldstein, R.F.; Teede, H.J. Women with polycystic ovary syndrome have intrinsic insulin resistance on euglycaemic-hyperinsulaemic clamp. Hum. Reprod. 2013, 28, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin resistance and the polycystic ovary syndrome revisited: An update on mechanisms and implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef] [PubMed]
- Dumesic, D.A.; Abbott, D.H.; Sanchita, S.; Chazenbalk, G.D. Endocrine–metabolic dysfunction in polycystic ovary syndrome: An evolutionary perspective. Curr. Opin. Endocr. Metab. Res. 2020, 12, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, M.; Porneki, A.D.; Skov, V.; Burns, J.S.; Beck-Nielsen, H.; Glintborg, D.; Gaster, M. Insulin resistance is not conserved in myotubes established from women with PCOS. PLoS ONE 2010, 5. [Google Scholar] [CrossRef] [PubMed]
- Rosenfield, R.L. Polycystic ovary syndrome and insulin-resistant hyperinsulinemia. J. Am. Acad. Dermatol. 2001, 45, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Tosi, F.; Di Sarra, D.; Kaufman, J.M.; Bonin, C.; Moretta, R.; Bonora, E.; Zanolin, E.; Moghetti, P. Total body fat and central fat mass independently predict insulin resistance but not hyperandrogenemia in women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2015, 100, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Nestler, J.E.; Jakubowicz, D.J.; De Vargas, A.F.; Brik, C.; Quintero, N.; Medina, F. Insulin stimulates testosterone biosynthesis by human thecal cells from women with polycystic ovary syndrome by activating its own receptor and using inositolglycan mediators as the signal transduction system. J. Clin. Endocrinol. Metab. 1998, 83, 2001–2005. [Google Scholar]
- Ben-Shlomo, I. The polycystic ovary syndrome: What does insulin resistance have to do with it? Reprod. Biomed. Online 2003, 6, 36–42. [Google Scholar] [CrossRef]
- Munir, I.; Yen, H.W.; Geller, D.H.; Torbati, D.; Bierden, R.M.; Weitsman, S.R.; Agarwal, S.K.; Magoffin, D.A. Insulin Augmentation of 17α-Hydroxylase Activity Is Mediated by Phosphatidyl Inositol 3-Kinase but Not Extracellular Signal-Regulated Kinase-1/ 2 in Human Ovarian Theca Cells. Endocrinology 2004, 145, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.; Chen, S.-W.; Su, W.-L.; Zhu, H.-Y.; Ouyang, S.-Y.; Cao, Y.-T.; Jiang, S.-Y. Sex Hormones Enhance Gingival Inflammation without Affecting IL-1 β and TNF-α in Periodontally Healthy Women during Pregnancy. Mediat. Inflamm. 2016. [Google Scholar] [CrossRef] [Green Version]
- Franks, S. Diagnosis of polycystic ovarian syndrome: In defense of the Rotterdam criteria. J. Clin. Endocrinol. Metab. 2006, 91, 786–789. [Google Scholar] [CrossRef] [Green Version]
- Nibali, L.; Tatarakis, N.; Needleman, I.; Tu, Y.K.; D’Aiuto, F.; Rizzo, M.; Donos, N. Association between metabolic syndrome and periodontitis: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2013, 98, 913–920. [Google Scholar] [CrossRef] [Green Version]
- Daudt, L.D.; Musskopf, M.L.; Mendez, M.; Remonti, L.L.R.; Leitão, C.B.; Gross, J.L.; Weidlich, P.; Oppermann, R.V. Association between metabolic syndrome and periodontitis: A systematic review and meta-analysis. Braz. Oral Res. 2018, 32, e35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, G.W. Bidirectional Interrelationships Between Diabetes and Periodontal Diseases: An Epidemiologic Perspective. Ann. Periodontol. 2001, 6, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Lalla, E.; Papapanou, P.N. Diabetes mellitus and periodontitis: A tale of two common interrelated diseases. Nat. Rev. Endocrinol. 2011, 7, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Grossi, S.G. Treatment of periodontal disease and control of diabetes: An assessment of the evidence and need for future research. Ann. Periodontol. 2001, 6, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Kocher, T.; König, J.; Borgnakke, W.S.; Pink, C.; Meisel, P. Periodontal complications of hyperglycemia/diabetes mellitus: Epidemiologic complexity and clinical challenge. Periodontology 2000 2018, 78, 59–97. [Google Scholar] [CrossRef] [PubMed]
- Borgnakke, W.; Ylostalo, P.; Taylor, G.; Genco, R. Effect of periodontal disease on diabetes: Systematic review of epidemiologic observational evidence. J. Clin. Periodontol. 2013, 40, S135–S152. [Google Scholar] [CrossRef]
- Demmer, R.; Desvraieux, M.; Holtfreter, B.; Jacobs, D.; Wallaschofski, H.; Nauck, M.; Volzke, H.; Kocher, T. Periodontal Status and A1c Change. Diabetes Care 2010, 33, 1037–1043. [Google Scholar] [CrossRef] [Green Version]
- Demmer, R.T.; Squillaro, A.; Papapanou, P.N.; Rosenbaum, M.; Friedewald, W.T.; Jacobs, D.R.; Desvarieux, M. Periodontal infection, systemic inflammation, and insulin resistance: Results from the continuous National Health and Nutrition Examination Survey (NHANES) 1999–2004. Diabetes Care 2012, 35, 2235–2242. [Google Scholar] [CrossRef] [Green Version]
- Koromantzos, P.A.; Makrilakis, K.; Dereka, X.; Katsilambros, N.; Vrotsos, I.A.; Madianos, P.N. A randomized, controlled trial on the effect of non-surgical periodontal therapy in patients with type 2 diabetes. Part I: Effect on periodontal status and glycaemic control. J. Clin. Periodontol. 2011, 38, 142–147. [Google Scholar] [CrossRef]
- Kaur, P.K.; Narula, S.C.; Rajput, R.; Sharma, R.K.; Tewari, S. Periodontal and glycemic effects of nonsurgical periodontal therapy in patients with type 2 diabetes stratified by baseline HbA1c. J. Oral Sci. 2015, 57, 201–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engebretson, S.; Kocher, T. Evidence that periodontal treatment improves diabetes outcomes: A systematic review and meta-analysis. J. Clin. Periodontol. 2013, 40, S153–S163. [Google Scholar] [CrossRef] [PubMed]
- Gay, I.C.; Tran, D.T.; Cavender, A.C.; Weltman, R.; Chang, J.; Luckenbach, E.; Tribble, G.D. The effect of periodontal therapy on glycaemic control in a Hispanic population with type 2 diabetes: A randomized controlled trial. J. Clin. Periodontol. 2014, 41, 673–680. [Google Scholar] [CrossRef] [Green Version]
- Chapple, I.L.C.; Genco, R. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef] [PubMed]
- Teeuw, W.J.; Gerdes, V.E.A.; Loos, B.G. Effect of periodontal treatment on glycemic control of diabetic patients: A systematic review and meta-analysis. Diabetes Care 2010, 33, 421–427. [Google Scholar] [CrossRef] [Green Version]
- Liew, A.K.C.; Punnanithinont, N.; Lee, Y.C.; Yang, J. Effect of non-surgical periodontal treatment on HbA1c: A meta-analysis of randomized controlled trials. Aust. Dent. J. 2013, 58, 350–357. [Google Scholar] [CrossRef]
- Sgolastra, F.; Severino, M.; Pietropaoli, D.; Gatto, R.; Monaco, A. Effectiveness of Periodontal Treatment to Improve Metabolic Control in Patients with Chronic Periodontitis and Type 2 Diabetes: A Meta-Analysis of Randomized Clinical Trials. J. Periodontol. 2013, 84, 958–973. [Google Scholar] [CrossRef] [PubMed]
- Simpson, T.C.; Weldon, J.C.; Worthington, H.V.; Needleman, I.; Wild, S.H.; Moles, D.R.; Stevenson, B.; Furness, S.; Iheozor-Ejiofor, Z. Treatment of periodontal disease for glycaemic control in people with diabetes. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Country | Funding | Number of Subjects | PCOS | PCOS–PD | PD | H | Mean Age ± SD (PCOS/PCOS–PD/PD/H) | Exclusion Criteria | PD Diagnostic Criteria | PCOS Criteria |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Porwal et al. (2014) | India | None | 126 | 85 | 0 | 0 | 41 | 23.50 ± 2.67/NA/NA/22.9 ± 4.7 | Thyroid dysfunction, hyperprolactinemia, and androgen-secreting tumors to avoid misdiagnosis of PCOS; chronic inflammatory disease; smoking and alcohol habits; Systemic ATB within 3 months; periodontal treatment within 6 months; and AgP diagnosis | Page and Eke 2012 | Rotterdam Criteria |
| Akcali et al. 2014 | Turkey | IADR | 125 | 80 | 0 | 0 | 45 | 25.6 ± 5.2/NA/NA/26.1 ± 4.7 | Hyperandrogenism, DM, hyperprolactemia, congenital adrenal hyperplasia, thyroid disorders, Cushing syndrome, HTA, hepatic or renal dysfunction; BMI > 30 kg/m2; CVD; medications (e.g., oral contraceptive agents, steroid hormones, insulin-sensitizing drugs and ATB or ant-inflammatory); periodontal status within the last 6 months | Armitage 1999 | Rotterdam Criteria |
| Hameed et al. 2017 | India | None | 80 | 20 | 20 | 20 | 20 | NA | Smoking habits; pregnant women; periodontal therapy at the previous 3 months; anti-inflammatory or ATB therapy during the last 3 months; contraceptives or hormonal drugs or medications for PCOS; systemic diseases (e.g., DM, HTA, CVD) which could affect periodontal health | AAP 1999 | Rotterdam Criteria |
| Saglam et al. 2017 | India | None | 88 | 22 | 22 | 22 | 22 | 27.6 ± 4.0/28.6 ± 4.5/28.2 ± 4.3/27.8 ± 3.9 | Cushing syndrome, non-classic congenital adrenal hyperplasia, hyperprolactinemia, thyroid dysfunction, and androgen-secreting tumors | Page and Eke 2012 | Rotterdam Criteria |
| Tong et al. 2019 | Taiwan | None | 48820 | 304 | 441 | 23969 | 24106 | NA | Endocrine disorders (e.g., Cushing syndrome, non-classic congenital adrenal hyperplasia, hyperprolactinemia, thyroid dysfunction and androgen-secreting tumors) | ICD-9-CM code: 523.4 | ICD-9-CM code: 256.4X |
| Saljoughi et al. 2020 | Iran | Arak University of Medical Sciences | 110 | 25 | 30 | 23 | 32 | 45.3 ± 3.0/45.2 ± 3.2/45.3 ± 3.1/45.5 ± 3.3 | Interfering drugs (e.g., ATB, oral contraceptives, antihypertensive, and DM drugs); infection in the last 6 months; systemic diseases (e.g., thyroid disorders, hyperprolactinemia, DM, HTA, malignancies, osteoporosis); obesity and overweight; smoking and alcohol habits, and pregnant women | Armitage 1999 | Rotterdam Criteria |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, V.; Escalda, C.; Proença, L.; Mendes, J.J.; Botelho, J. Is There a Bidirectional Association between Polycystic Ovarian Syndrome and Periodontitis? A Systematic Review and Meta-analysis. J. Clin. Med. 2020, 9, 1961. https://doi.org/10.3390/jcm9061961
Machado V, Escalda C, Proença L, Mendes JJ, Botelho J. Is There a Bidirectional Association between Polycystic Ovarian Syndrome and Periodontitis? A Systematic Review and Meta-analysis. Journal of Clinical Medicine. 2020; 9(6):1961. https://doi.org/10.3390/jcm9061961
Chicago/Turabian StyleMachado, Vanessa, Cláudia Escalda, Luís Proença, José João Mendes, and João Botelho. 2020. "Is There a Bidirectional Association between Polycystic Ovarian Syndrome and Periodontitis? A Systematic Review and Meta-analysis" Journal of Clinical Medicine 9, no. 6: 1961. https://doi.org/10.3390/jcm9061961
APA StyleMachado, V., Escalda, C., Proença, L., Mendes, J. J., & Botelho, J. (2020). Is There a Bidirectional Association between Polycystic Ovarian Syndrome and Periodontitis? A Systematic Review and Meta-analysis. Journal of Clinical Medicine, 9(6), 1961. https://doi.org/10.3390/jcm9061961