Antiplatelet Antibodies Do Not Predict the Response to Intravenous Immunoglobulins during Immune Thrombocytopenia

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
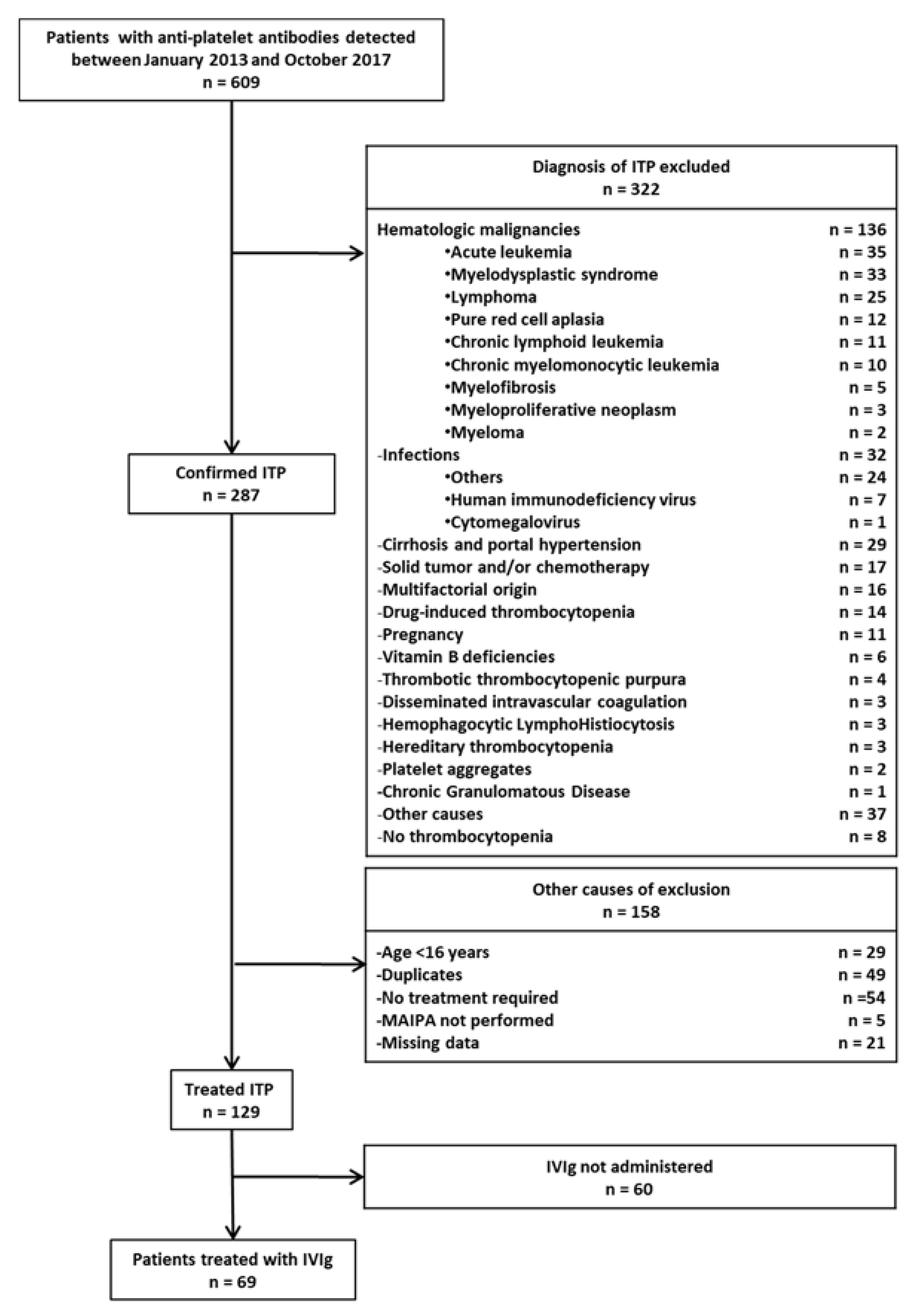
3.1. Patient Characteristics
3.2. Response to IVIg According to the Presence of Anti-GPIb/IX Antibodies
3.3. Predictive Factors of Response to IVIg
3.4. Response to Splenectomy According to the Presence of Anti-GPIb/IX Antibodies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Audia, S.; Mahevas, M.; Samson, M.; Godeau, B.; Bonnotte, B. Pathogenesis of immune thrombocytopenia. Autoimmun. Rev. 2017, 16, 620–632. [Google Scholar] [CrossRef]
- Zufferey, A.; Kapur, R.; Semple, J.W. Pathogenesis and therapeutic mechanisms in immune thrombocytopenia (ITP). J. Clin. Med. 2017, 6, 16. [Google Scholar] [CrossRef]
- Grozovsky, R.; Begonja, A.J.; Liu, K.; Visner, G.; Hartwig, J.H.; Falet, H.; Hoffmeister, K.M. The Ashwell-Morell receptor regulates hepatic thrombopoietin production via JAK2-STAT3 signaling. Nat. Med. 2015, 21, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; van der Wal, D.E.; Zhu, G.; Xu, M.; Yougbare, I.; Ma, L.; Vadasz, B.; Carrim, N.; Grozovsky, R.; Ruan, M.; et al. Desialylation is a mechanism of Fc-independent platelet clearance and a therapeutic target in immune thrombocytopenia. Nat. Commun. 2015, 6, 7737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrbensky, J.R.; Moore, J.E.; Arnold, D.M.; Smith, J.W.; Kelton, J.G.; Nazy, I. The sensitivity and specificity of platelet autoantibody testing in immune thrombocytopenia: A systematic review and meta-analysis of a diagnostic test. J. Thromb. Haemost. 2019. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, D.; Canoui-Poitrine, F.; Croisille, L.; Lee, K.; Roudot-Thoraval, F.; Languille, L.; Khellaf, M.; Michel, M.; Godeau, B.; Bierling, P. Antiplatelet antibodies detected by the MAIPA assay in newly diagnosed immune thrombocytopenia are associated with chronic outcome and higher risk of bleeding. Ann. Hematol. 2014, 93, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Zhu, L.; Tao, L.; Bao, J.; Yang, M.; Simpson, E.K.; Li, C.; van der Wal, D.E.; Chen, P.; Spring, C.M.; et al. Relative efficacy of steroid therapy in immune thrombocytopenia mediated by anti-platelet GPIIbIIIa versus GPIbalpha antibodies. Am. J. Hematol. 2012, 87, 206–208. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.; Ma, S.H.; Liu, J.; Hou, Y.; Liu, X.M.; Niu, T.; Xu, R.R.; Guo, C.S.; Wang, X.M.; Cheng, Y.F.; et al. Association of autoantibody specificity and response to intravenous immunoglobulin G therapy in immune thrombocytopenia: A multicenter cohort study. J. Thromb. Haemost. 2014, 12, 497–504. [Google Scholar] [CrossRef]
- Go, R.S.; Johnston, K.L.; Bruden, K.C. The association between platelet autoantibody specificity and response to intravenous immunoglobulin G in the treatment of patients with immune thrombocytopenia. Haematologica 2007, 92, 283–284. [Google Scholar] [CrossRef] [Green Version]
- Feng, R.; Liu, X.; Zhao, Y.; Zhu, Y.; Peng, J.; Hou, M.; Chen, C. GPIIb/IIIa autoantibody predicts better rituximab response in ITP. Br. J. Haematol. 2017, 182, 305–307. [Google Scholar] [CrossRef] [Green Version]
- Khellaf, M.; Michel, M.; Schaeffer, A.; Bierling, P.; Godeau, B. Assessment of a therapeutic strategy for adults with severe autoimmune thrombocytopenic purpura based on a bleeding score rather than platelet count. Haematologica 2005, 90, 829–832. [Google Scholar] [PubMed]
- Provan, D.; Arnold, D.M.; Bussel, J.B.; Chong, B.H.; Cooper, N.; Gernsheimer, T.; Ghanima, W.; Godeau, B.; Gonzalez-Lopez, T.J.; Grainger, J.; et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019, 3, 3780–3817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwab, I.; Lux, A.; Nimmerjahn, F. Pathways responsible for human autoantibody and therapeutic intravenous IgG activity in humanized mice. Cell Rep. 2015, 13, 610–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webster, M.L.; Sayeh, E.; Crow, M.; Chen, P.; Nieswandt, B.; Freedman, J.; Ni, H. Relative efficacy of intravenous immunoglobulin G in ameliorating thrombocytopenia induced by antiplatelet GPIIbIIIa versus GPIbalpha antibodies. Blood 2006, 108, 943–946. [Google Scholar] [CrossRef] [Green Version]
- Godeau, B.; Chevret, S.; Varet, B.; Lefrere, F.; Zini, J.M.; Bassompierre, F.; Cheze, S.; Legouffe, E.; Hulin, C.; Grange, M.J.; et al. Intravenous immunoglobulin or high-dose methylprednisolone, with or without oral prednisone, for adults with untreated severe autoimmune thrombocytopenic purpura: A randomised, multicentre trial. Lancet 2002, 359, 23–29. [Google Scholar] [CrossRef]
- Kiefel, V.; Santoso, S.; Weisheit, M.; Mueller-Eckhardt, C. Monoclonal antibody—Specific immobilization of platelet antigens (MAIPA): A new tool for the identification of platelet-reactive antibodies. Blood 1987, 70, 1722–1726. [Google Scholar] [CrossRef] [Green Version]
- Moulis, G.; Palmaro, A.; Montastruc, J.L.; Godeau, B.; Lapeyre-Mestre, M.; Sailler, L. Epidemiology of incident immune thrombocytopenia: A nationwide population-based study in France. Blood 2014. [Google Scholar] [CrossRef] [Green Version]
- Brighton, T.A.; Evans, S.; Castaldi, P.A.; Chesterman, C.N.; Chong, B.H. Prospective evaluation of the clinical usefulness of an antigen-specific assay (MAIPA) in idiopathic thrombocytopenic purpura and other immune thrombocytopenias. Blood 1996, 88, 194–201. [Google Scholar] [CrossRef] [Green Version]
- Meyer, O.; Agaylan, A.; Bombard, S.; Kiesewetter, H.; Salama, A. A novel antigen-specific capture assay for the detection of platelet antibodies and HPA-1a phenotyping. Vox Sang. 2006, 91, 324–330. [Google Scholar] [CrossRef]
- Najaoui, A.; Bakchoul, T.; Stoy, J.; Bein, G.; Rummel, M.J.; Santoso, S.; Sachs, U.J. Autoantibody-mediated complement activation on platelets is a common finding in patients with immune thrombocytopenic purpura (ITP). Eur. J. Haematol. 2012, 88, 167–174. [Google Scholar] [CrossRef]
- Panzer, S.; Hocker, L.; Rieger, M.; Vormittag, R.; Koren, D.; Dunkler, D.; Pabinger, I. Agonist-inducible platelet activation in chronic idiopathic autoimmune thrombocytopenia. Eur. J. Haematol. 2007, 79, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Porcelijn, L.; Huiskes, E.; Oldert, G.; Schipperus, M.; Zwaginga, J.J.; de Haas, M. Detection of platelet autoantibodies to identify immune thrombocytopenia: State of the art. Br. J. Haematol. 2018, 182, 423–426. [Google Scholar] [CrossRef] [PubMed]
- Al-Samkari, H.; Rosovsky, R.P.; Karp Leaf, R.S.; Smith, D.B.; Goodarzi, K.; Fogerty, A.E.; Sykes, D.B.; Kuter, D.J. A modern reassessment of glycoprotein-specific direct platelet autoantibody testing in immune thrombocytopenia. Blood Adv. 2020, 4, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, D.M.; Santoso, S.; Greinacher, A. Recommendations for the implementation of platelet autoantibody testing in clinical trials of immune thrombocytopenia. J. Thromb. Haemost. 2012, 10, 695–697. [Google Scholar] [CrossRef] [Green Version]
- Romero-Guzman, L.T.; Lopez-Karpovitch, X.; Paredes, R.; Barrales-Benitez, O.; Piedras, J. Detection of platelet-associated immunoglobulins by flow cytometry for the diagnosis of immune thrombocytopenia: A prospective study and critical review. Haematologica 2000, 85, 627–631. [Google Scholar]
- Quach, M.E.; Dragovich, M.A.; Chen, W.; Syed, A.K.; Cao, W.; Liang, X.; Deng, W.; De Meyer, S.F.; Zhu, G.; Peng, J.; et al. Fc-independent immune thrombocytopenia via mechanomolecular signaling in platelets. Blood 2018, 131, 787–796. [Google Scholar] [CrossRef] [Green Version]
- Tao, L.; Zeng, Q.; Li, J.; Xu, M.; Wang, J.; Pan, Y.; Wang, H.; Tao, Q.; Chen, Y.; Peng, J.; et al. Platelet desialylation correlates with efficacy of first-line therapies for immune thrombocytopenia. J. Hematol. Oncol. 2017, 10, 46. [Google Scholar] [CrossRef] [Green Version]
- Heitink-Polle, K.M.J.; Uiterwaal, C.; Porcelijn, L.; Tamminga, R.Y.J.; Smiers, F.J.; van Woerden, N.L.; Wesseling, J.; Vidarsson, G.; Laarhoven, A.G.; de Haas, M.; et al. Intravenous immunoglobulin vs observation in childhood immune thrombocytopenia: A randomized controlled trial. Blood 2018, 132, 883–891. [Google Scholar] [CrossRef]
- Kojouri, K.; Vesely, S.K.; Terrell, D.R.; George, J.N. Splenectomy for adult patients with idiopathic thrombocytopenic purpura: A systematic review to assess long-term platelet count responses, prediction of response, and surgical complications. Blood 2004, 104, 2623–2634. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Antiplatelet Antibodies | Anti-GPIb/IX+ | Anti-GPIb/IX- | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | Anti-GPIIb/IIIa+ | Anti-GPIIb/IIIa- | Total | Anti-GPIIb/IIIa+ | Anti-GPIIb/IIIa- | Total | ||||
| Anti-GPIa/IIa+ | Anti-GPIa/IIa- | Anti-GPIa/IIa- | Anti-GPIa/IIa+ | Anti-GPIa/IIa- | Anti-GPIa/IIa- | |||||
| Clinical characteristics | ||||||||||
| Population, n | 69 | 10 | 6 | 1 | 17 | 2 | 15 | 35 | 52 | |
| Sex ratio (Female/Male) | 37/32 | 3/2 | 1/2 | 0 | 8/9 | 2 | 7/8 | 4/3 | 29/23 | 0.6 |
| Age at diagnosis (years), median (IQR) | 60.3 (29.8–73.6) | 56.0 (30.0–70.0) | 77.4 (57.0–82.1) | 77.9 (NA) | 68.0 (41.8–75.5) | 37.9 (27.8–48.1) | 65.4 (31.1–74.8) | 60.3 (36.0–67.0) | 59.3 (29.8–73.5) | 0.6 |
| Primitive ITP (%) | 48 (69.6) | 6 (60) | 4 (66.67) | 1 (100) | 11 (64.7) | 1 (50) | 9 (60) | 26 (66.7) | 37 (71.2) | 0.8 |
| ITP course: | ||||||||||
| - Newly diagnosed, n (%) - persistent, n (%) - chronic, n (%) | 43 (62.3) 3 (4.3) 23 (33.3) | 8 (80) 0 (0) 2 (20) | 6 (100) 0 (0) 0 (0) | 0 (0) 0 (0) 1 (100) | 14 (82.4) 0 (0) 3 (17.65) | 0 (0) 1 (50) 1 (50) | 9 (60) 0 (0) 6 (40.0) | 20 (57.1) 2 (5.7) 13 (37.1) | 29 (55.7) 3 (5.8) 20 (38.46) | 0.1 0.6 0.2 |
| Age at IVIg initiation (years), median (IQR) | 62.7 (41.8–76.4) | 56.0 (33.6–69.5) | 77.4 (57.0–82.1) | 85.2 (NA) | 66 (41.8–75.5) | 40.7 (31.64–49.8) | 68.1 (43.4–75.5) | 62.7 (39.4–79.5) | 62.5 (40.7–76.5) | 1.0 |
| Platelet count (G/L), median (IQR) | ||||||||||
| At diagnosis | 7 (5–18) | 5.5 (5.0–8.5) | 9.0 (7.0–9.8) | 50 (NA) | 7 (5–9) | 9 (7–11) | 9.5 (5.0–45.0) | 7.0 (5.0–20.3) | 7 (5–22) | 0.2 |
| At day 1 | 7 (4–14) | 5.0 (3.5–8.5) | 8.0 (5.5–9.8) | 60 (NA) | 7.0 (5–10) | 7.5 (7.3–7.8) | 11.0 (5.0–15.5) | 7.5 (3–16.8) | 8.0 (4–16.5) | 0.7 |
| At day 3 | 38 (11–59) | 17 (10.3–33.3) | 56.0 (51.5–70.3) | 78 (NA) | 51 (17–66.5) | 25.5 (22.8–28.3) | 36.0 (12.5–83.5) | 40.0 (8.0–59.0) | 37 (10–59) | 0.6 |
| At day 5 | 46.5 (18.8–91.3) | 45 (31–49) | 105.0 (90.5–165.5) | NA | 49 (38–97) | NA | 49.5 (19.8–89.0) | 24 (12–66.5) | 37 (13.5–79) | 0.1 |
| At day 7 | 43 (21–103) | 33.5 (25.5–48.8) | 196.0 (187.0–294.5) | NA | 47 (27.5–116.5) | 320 (NA) | 62.0 (34.3–98.3) | 36.0 (13.0–91.5) | 40.5 (18.3–100.5) | 0.6 |
| At day 10 | 32 (14–100) | 54 (20–100) | 24 (NA) | NA | 39 (21–88.5) | 191 (NA) | 77.0 (36.5–119.5) | 14 (10–43) | 32 (12–119.5) | 0.9 |
| Treatments | ||||||||||
| Steroids (%) | 60 (87.0) | 9 (90) | 6 (100) | 1 (100) | 16 (94.1) | 2 (100) | 12 (80) | 30 (85.7) | 44 (84.6) | 0.4 |
| IVIg total dose administered (g/kg), n (%) | NA | |||||||||
| 2 1.6 1.2 1 0.8 0.4 Not known | 34 (56.7) 5 (7.2) 3 (4.3) 20 (29) 1 (1.4) 2 (2.9) 4 (5.8) | 5 (50) 2 (20) 0 (0) 3 (30.0) 0 (0) 0 (0) 0 (0) | 2 (33.3) 0 (0) 0 (0) 3 (50) 0 (0) 0 (0) 1 (16.6) | 1 (100) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) | 8 (47.1) 2 (11.8) 0 (0) 6 (35.3) 0 (0) 0 (0) 1 (5.9) | 0 (0) 0 (0) 0 (0) 2 (100) 0 (0) 0 (0) 0 (0) | 8 (53.3) 0 (0) 2 (13.3) 4 (26.7) 0 (0) 1 (6.7) 0 (0) | 18 (51.4) 3 (8.6) 1 (2.9) 8 (22.9) 1 (2.9) 1 (2.9) 3 (8.6) | 26 (50) 3 (5.6) 3 (5.6) 14 (26.9) 1 (1.9) 2 (3.7) 3 (5.6) | |
| Anti-GPIb/IX | Anti-GPIIb/IIIa | Number of Patients n (%) | Response to IVIg n (%) |
|---|---|---|---|
| + | + | 16 (23.2) | 15 (93.8) |
| + | - | 1 (1.5) | 0 (0) |
| - | + | 17 (24.6) | 14 (82.4) |
| - | - | 35 (50.7) | 24 (68.6) |
| Total | 69 | 53 (76.8) |
| Subgroups | n | Anti-GPIb/IX+ | Anti-GPIb/IX- | p | ||
|---|---|---|---|---|---|---|
| Responders (n, %) | Non Responders (n, %) | Responders (n, %) | Non Responders (n, %) | |||
| 69 | 15 (88.2) | 2 (11.8) | 38 (73.1) | 14 (26.9) | 0.3 | |
| Age at diagnosis ≤ 30 years | 18 | 4 (100) | 0 (0) | 12 (85.7) | 2 (14.3) | 1.0 |
| Age at diagnosis ≤ 60 years | 33 | 7 (100) | 0 (0) | 21 (80.8) | 5 (19.2) | 0.6 |
| Age at IVIg initiation ≤ 40 years | 17 | 4 (100) | 0 (0) | 10 (76.9) | 3 (23.1) | 0.5 |
| Age at IVIg initiation ≤ 50 years | 24 | 5 (100) | 0 (0) | 16 (84.2) | 3 (15.8) | 1.0 |
| Age at IVIg initiation ≤ 60 years | 30 | 7 (100) | 0 (0) | 19 (82.6) | 4 (17.4) | 0.6 |
| Newly diagnosed ITP | 43 | 13 (92.9) | 1 (7.1) | 23 (79.3) | 6 (20.7) | 0.4 |
| Persistent ITP | 3 | 0 (0) | 0 (0) | 0 (0) | 3 (100) | NA |
| Chronic ITP | 23 | 2 (66.7) | 1 (33.3) | 15 (75) | 5 (25) | 1.0 |
| Anti-GPIIb/IIIa antibodies | 33 | 29 (93.8) | 1 (6.3) | 14 (82.4) | 3 (17.7) | 0.6 |
| Anti-GPIa/IIa antibodies | 12 | 9 (90) | 1 (10) | 1 (50) | 1 (50) | 0.3 |
| Male | 32 | 7 (77.8) | 2 (22.2) | 15 (65.2) | 8 (34.8) | 0.7 |
| Female | 37 | 8 (100) | 0 (0) | 23 (79.3) | 6 (20.7) | 0.3 |
| Primary ITP | 48 | 10 (90.1) | 1 (9.1) | 29 (78.4) | 8 (21.6) | 0.6 |
| Secondary ITP | 21 | 5 (83.3) | 1 (16.7) | 9 (60) | 6 (40) | 0.6 |
| Subgroups | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (CI 95%) | p | OR (CI 95%) | p | |
| Patients characteristics | ||||
| Men | 0.43 (0.11–1.54) | 0.16 | 0.27 (0.06–1.28) | 0.10 |
| Secondary ITP | 0.43 (0.13–1.78) | 0.22 | 0.1 (0.02–0.64) | 0.01 |
| Age at diagnosis ≤ 30 years | 2.99 (0.58–30.1) | 0.21 | ||
| Age at diagnosis ≤ 60 years | 2.43 (0.67–10.22) | 0.16 | ||
| Age at IVIg initiation ≤ 40 years | 1.55 (0.35–9.70) | 0.74 | ||
| Age at IVIg initiation ≤ 50 years | 2.80 (0.66–17.2) | 0.15 | 3.0 (0.5–17.2) | 0.21 |
| Age at IVIg initiation ≤ 60 years | 2.84 (0.74–13.7) | 0.15 | ||
| ITP course | ||||
| Newly diagnosed | 2.68 (0.75–10.09) | 0.14 | 5.4 (1.2–24.7) | 0.03 |
| Persistent | NA | 0.01 | ||
| Chronic | 0.79 (0.22–3.10) | 0.77 | ||
| Antiplatelet antibodies | ||||
| Anti-GPIIb/IIIa | 3.56 (0.92–17.14) | 0.05 | 4.82 (1.08–21.5) | 0.04 |
| Anti-GPIa/IIa | 1.62 (0.29–16.9) | 0.72 | ||
| Anti-GPIb/IX | 2.73 (0.52–27.6) | 0.32 | ||
| Anti-GPIb/IX | Anti-GPIIb/IIIa | Number of Patients n (%) | Response to Splenectomy n (%) |
|---|---|---|---|
| + | + | 3 (27.3) | 2 (66.6) |
| + | - | 0 (0) | NA |
| - | + | 5 (45.5) | 3 (60) |
| - | - | 3 (27.3) | 2 (66.6) |
| Total | 11 | 7 (63.4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogier, T.; Samson, M.; Mourey, G.; Falvo, N.; Magy-Bertrand, N.; Ouandji, S.; Picque, J.-B.; Greigert, H.; Mausservey, C.; Imbach, A.; et al. Antiplatelet Antibodies Do Not Predict the Response to Intravenous Immunoglobulins during Immune Thrombocytopenia. J. Clin. Med. 2020, 9, 1998. https://doi.org/10.3390/jcm9061998
Rogier T, Samson M, Mourey G, Falvo N, Magy-Bertrand N, Ouandji S, Picque J-B, Greigert H, Mausservey C, Imbach A, et al. Antiplatelet Antibodies Do Not Predict the Response to Intravenous Immunoglobulins during Immune Thrombocytopenia. Journal of Clinical Medicine. 2020; 9(6):1998. https://doi.org/10.3390/jcm9061998
Chicago/Turabian StyleRogier, Thomas, Maxime Samson, Guillaume Mourey, Nicolas Falvo, Nadine Magy-Bertrand, Sethi Ouandji, Jean-Baptiste Picque, Hélène Greigert, Christelle Mausservey, Arthur Imbach, and et al. 2020. "Antiplatelet Antibodies Do Not Predict the Response to Intravenous Immunoglobulins during Immune Thrombocytopenia" Journal of Clinical Medicine 9, no. 6: 1998. https://doi.org/10.3390/jcm9061998
APA StyleRogier, T., Samson, M., Mourey, G., Falvo, N., Magy-Bertrand, N., Ouandji, S., Picque, J. -B., Greigert, H., Mausservey, C., Imbach, A., Ghesquière, T., Voillat, L., Caillot, D., Deconinck, E., Bonnotte, B., & Audia, S. (2020). Antiplatelet Antibodies Do Not Predict the Response to Intravenous Immunoglobulins during Immune Thrombocytopenia. Journal of Clinical Medicine, 9(6), 1998. https://doi.org/10.3390/jcm9061998