Impaired Fibrinolysis in Patients with Isolated Aortic Stenosis is Associated with Enhanced Oxidative Stress

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Laboratory Investigations
2.2. Clot Permeability
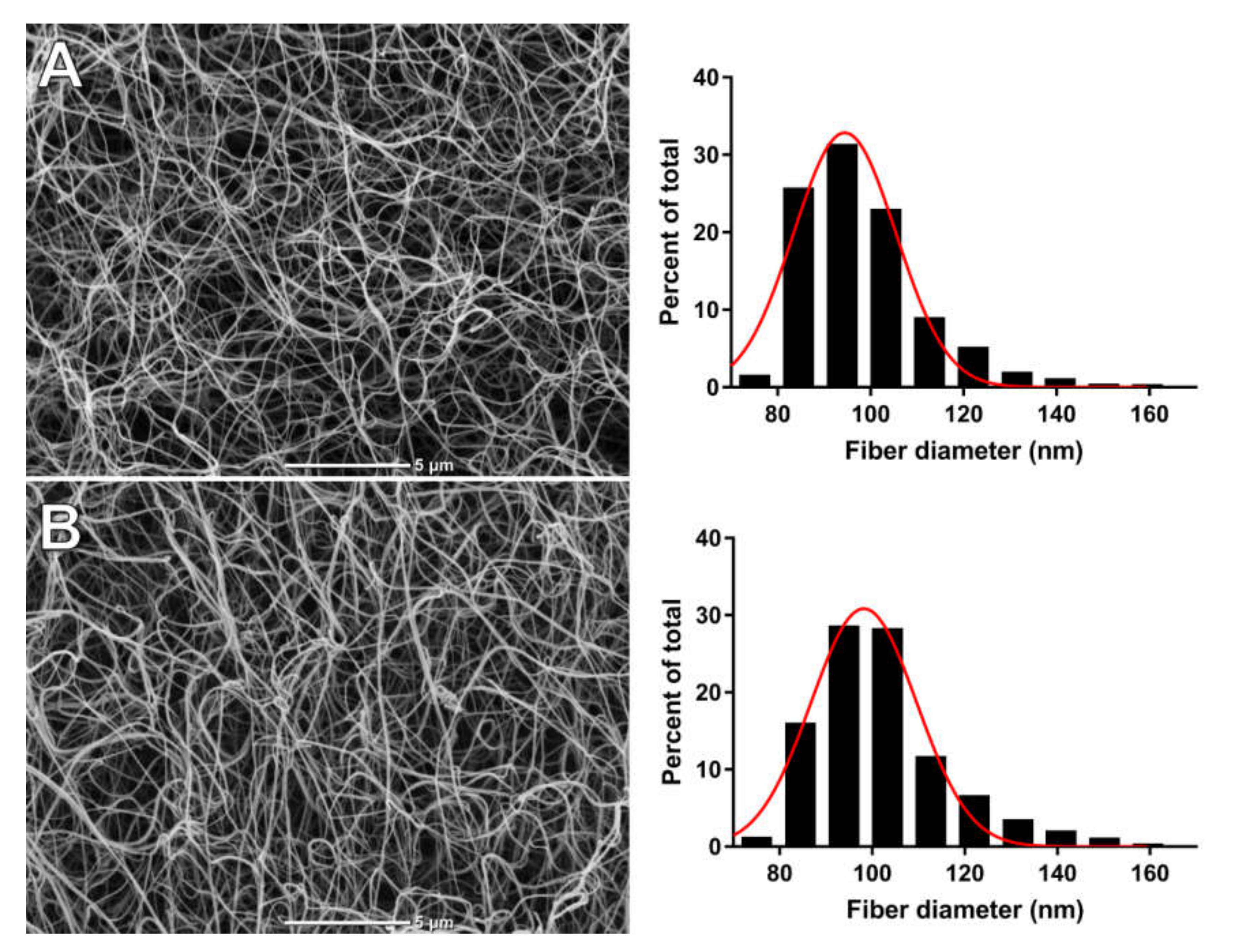
2.3. Scanning Electron Microscopy (SEM)
2.4. Plasma Clot Lysis Assays
2.5. Thrombin Generation
2.6. Plasma Carbonyl Content and Malondialdehyde Levels in Plasma
2.7. Statistical Analysis
3. Results
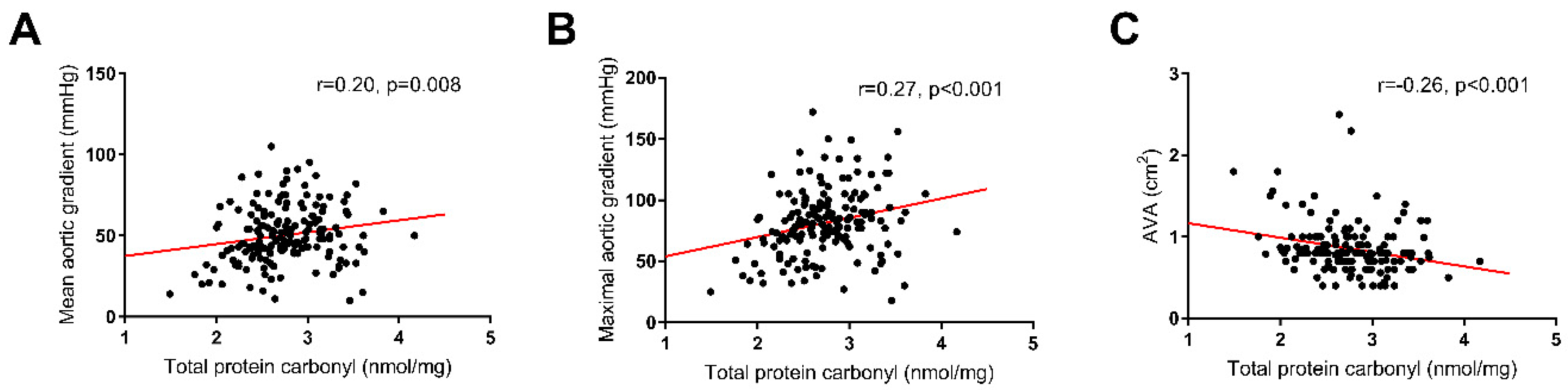
3.1. Oxidation and AS
3.2. Hypofibrinolysis in AS Patients
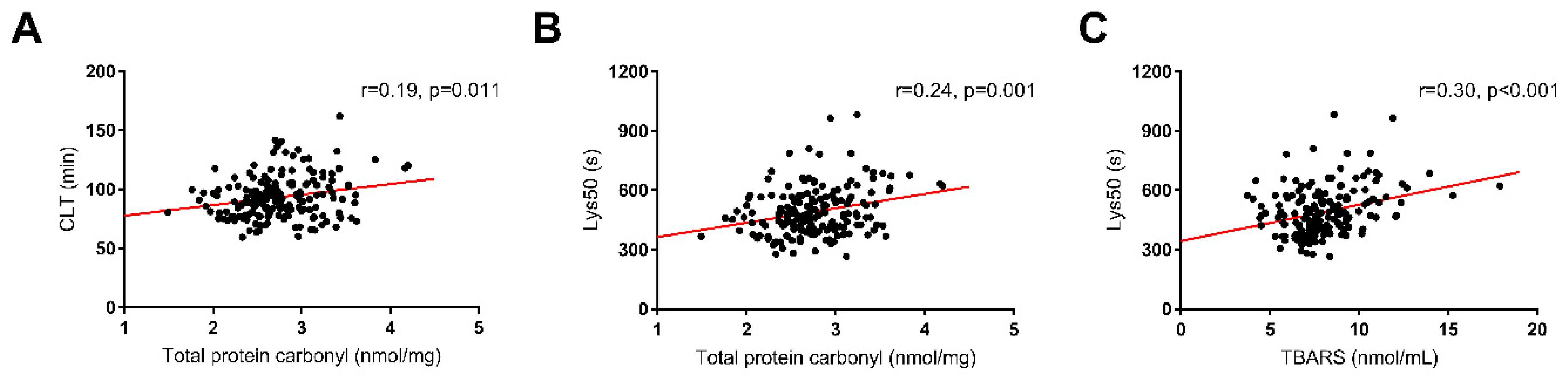
3.3. Determinants of Prolonged Fibrinolysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Eveborn, G.W.; Schirmer, H.; Heggelund, G.; Lunde, P.; Rasmussen, K. The evolving epidemiology of valvular aortic stenosis. the Tromsø study. Heart 2013, 99, 396–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindman, B.R.; Clavel, M.-A.; Mathieu, P.; Iung, B.; Lancellotti, P.; Otto, C.M.; Pibarot, P. Calcific aortic stenosis. Nat. Rev. Dis. Prim. 2016, 2, 16006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, J.D.; Chu, Y.; Brooks, R.M.; Richenbacher, W.E.; Peña-Silva, R.; Heistad, D.D. Dysregulation of Antioxidant Mechanisms Contributes to Increased Oxidative Stress in Calcific Aortic Valvular Stenosis in Humans. J. Am. Coll. Cardiol. 2008, 52, 843–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wada, S.; Sugioka, K.; Naruko, T.; Kato, Y.; Shibata, T.; Inoue, T.; Inaba, M.; Ohsawa, M.; Yoshiyama, M.; Ueda, M. Relationship between oxidative stress and aortic valve stenosis in humans: An immunohistochemical study. Osaka City Med. J. 2013, 59, 61–67. [Google Scholar]
- Zheng, K.H.; Tsimikas, S.; Pawade, T.; Kroon, J.; Jenkins, W.S.A.; Doris, M.K.; White, A.C.; Timmers, N.K.L.M.; Hjortnaes, J.; Rogers, M.A.; et al. Lipoprotein(a) and Oxidized Phospholipids Promote Valve Calcification in Patients With Aortic Stenosis. J. Am. Coll. Cardiol. 2019, 73, 2150–2162. [Google Scholar] [CrossRef]
- Pignatelli, P.; Menichelli, D.; Pastori, D.; Violi, F. Oxidative stress and cardiovascular disease: New insights. Kardiol. Pol. 2018, 713–722. [Google Scholar] [CrossRef] [Green Version]
- Demer, L.; Tintut, Y. The roles of lipid oxidation products and receptor activator of nuclear factor-κB signaling in atherosclerotic calcification. Circ. Res. 2011, 108, 1482–1493. [Google Scholar] [CrossRef]
- Capoulade, R.; Chan, K.L.; Yeang, C.; Mathieu, P.; Bossé, Y.; Dumesnil, J.G.; Tam, J.W.; Teo, K.K.; Mahmut, A.; Yang, X.; et al. Oxidized phospholipids, lipoprotein(a), and progression of calcific aortic valve stenosis. J. Am. Coll. Cardiol. 2015, 66, 1236–1246. [Google Scholar] [CrossRef] [Green Version]
- Goyal, T.; Mitra, S.; Khaidakov, M.; Wang, X.; Singla, S.; Ding, Z.; Liu, S.; Mehta, J.L. Current Concepts of the Role of Oxidized LDL Receptors in Atherosclerosis. Curr. Atheroscler. Rep. 2012, 14, 150–159. [Google Scholar] [CrossRef]
- Rosenfeld, M.A.; Bychkova, A.V.; Shchegolikhin, A.N.; Leonova, V.B.; Biryukova, M.I.; Kostanova, E.A. Ozone-induced oxidative modification of plasma fibrin-stabilizing factor. Biochim. Biophys. Acta Proteins Proteom. 2013, 1834, 2470–2479. [Google Scholar] [CrossRef] [PubMed]
- Hopps, E.; Caimi, G. Protein oxidation in metabolic syndrome. Clin. Investig. Med. 2013, 36, E1–E8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becatti, M.; Marcucci, R.; Bruschi, G.; Taddei, N.; Bani, D.; Gori, A.M.; Giusti, B.; Gensini, G.F.; Abbate, R.; Fiorillo, C. Oxidative modification of fibrinogen is associated with altered function and structure in the subacute phase of myocardial infarction. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1355–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryk, A.; Konieczynska, M.; Rostoff, P.; Broniatowska, E.; Hohendorff, J.; Malecki, M.; Undas, A. Plasma Protein Oxidation as a Determinant of Impaired Fibrinolysis in Type 2 Diabetes. Thromb. Haemost. 2019, 119, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Natorska, J.; Marek, G.; Hlawaty, M.; Sobczyk, D.; Sadowski, J.; Tracz, W.; Undas, A. Evidence for tissue factor expression in aortic valves in patients with aortic stenosis. Pol. Arch. Intern. Med. 2009, 119, 636–642. [Google Scholar] [CrossRef]
- Natorska, J.; Marek, G.; Hlawaty, M.; Sadowski, J.; Tracz, W.; Undas, A. Fibrin presence within aortic valves in patients with aortic stenosis: Association with in vivo thrombin generation and fibrin clot properties. Thromb. Haemost. 2011, 105, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Natorska, J.; Wypasek, E.; Grudzień, G.; Sadowski, J.; Undas, A. Impaired fibrinolysis is associated with the severity of aortic stenosis in humans. J. Thromb. Haemost. 2013, 11, 733–740. [Google Scholar] [CrossRef]
- Natorska, J.; Undas, A. Blood coagulation and fibrinolysis in aortic valve stenosis: Links with inflammation and calcification. Thromb. Haemost. 2015, 114, 217–227. [Google Scholar] [CrossRef]
- Mourino-Alvarez, L.; Baldan-Martin, M.; Gonzalez-Calero, L.; Martinez-Laborde, C.; Sastre-Oliva, T.; Moreno-Luna, R.; Lopez-Almodovar, L.F.; Sanchez, P.L.; Fernandez-Aviles, F.; Vivanco, F.; et al. Patients with calcific aortic stenosis exhibit systemic molecular evidence of ischemia, enhanced coagulation, oxidative stress and impaired cholesterol transport. Int. J. Cardiol. 2016, 225, 99–106. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; Bonis, M.D.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Munoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Kardiol. Pol. 2018, 76, 1–62. [Google Scholar] [CrossRef] [Green Version]
- Undas, A.; Podolec, P.; Zawilska, K.; Pieculewicz, M.; Jedliński, I.; Stgpień, E.; Konarska-Kuszewska, E.; Wȩglarz, P.; Duszyńska, M.; Hanschke, E.; et al. Altered fibrin clot structure/function in patients with cryptogenic ischemic stroke. Stroke 2009, 40, 1499–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ząbczyk, M.; Majewski, J.; Karkowski, G.; Malinowski, K.P.; Undas, A. Vitamin K antagonists favourably modulate fibrin clot properties in patients with atrial fibrillation as early as after 3 days of treatment: Relation to coagulation factors and thrombin generation. Thromb. Res. 2015, 136, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Pieters, M.; Philippou, H.; Undas, A.; de Lange, Z.; Rijken, D.C.; Mutch, N.J. An international study on the feasibility of a standardized combined plasma clot turbidity and lysis assay: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 1007–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, A.M.; Cymbalista, C.M.; Spector, T.D.; Grant, P.J. Heritability of Clot Formation, Morphology, and Lysis. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2783–2789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wajih, N.; Basu, S.; Ucer, K.B.; Rigal, F.; Shakya, A.; Rahbar, E.; Vachharajani, V.; Guthold, M.; Gladwin, M.T.; Smith, L.M.; et al. Erythrocytic bioactivation of nitrite and its potentiation by far-red light. Redox Biol. 2019, 20, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Ząbczyk, M.; Natorska, J.; Janion-Sadowska, A.; Malinowski, K.P.; Janion, M.; Undas, A. Elevated Lactate Levels in Acute Pulmonary Embolism Are Associated with Prothrombotic Fibrin Clot Properties: Contribution of NETs Formation. J. Clin. Med. 2020, 9, 953. [Google Scholar] [CrossRef] [Green Version]
- Ilich, A.; Noubouossie, D.F.; Henderson, M.; Ellsworth, P.; Betbadal, K.F.; Campello, E.; Meeks, S.; Dunn, A.; Park, M.S.; Pawlinski, R.; et al. Development and application of global assays of hyper- and hypofibrinolysis. Res. Pract. Thromb. Haemost. 2019, 4, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Sumaya, W.; Wallentin, L.; James, S.K.; Siegbahn, A.; Gabrysch, K.; Bertilsson, M.; Himmelmann, A.; Ajjan, R.A.; Storey, R.F. Fibrin clot properties independently predict adverse clinical outcome following acute coronary syndrome: A PLATO substudy. Eur. Heart J. 2018, 39, 1078–1085. [Google Scholar] [CrossRef] [Green Version]
- Abdul, S.; Leebeek, F.W.G.; Rijken, D.C.; De Willige, S.U. Natural heterogeneity of α2-antiplasmin: Functional and clinical consequences. Blood 2016, 127, 538–545. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, M.E.; Lisman, T.; De Groot, P.G.; Meijers, J.C.M.; Le Cessie, S.; Doggen, C.J.M.; Rosendaal, F.R. Venous thrombosis risk associated with plasma hypofibrinolysis is explained by elevated plasma levels of TAFI and PAI-1. Blood 2010, 116, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Lisman, T. Decreased Plasma Fibrinolytic Potential As a Risk for Venous and Arterial Thrombosis. Semin. Thromb. Hemost. 2016, 43, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Houng, A.; Reed, G.L. Releasing the Brakes on the Fibrinolytic System in Pulmonary Emboli: Unique Effects of Plasminogen Activation and α2-Antiplasmin Inactivation. Circulation 2017, 135, 1011–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urano, T.; Suzuki, Y. Thrombolytic Therapy Targeting Alpha 2-Antiplasmin. Circulation 2017, 135, 1021–1023. [Google Scholar] [CrossRef] [PubMed]
- Shacter, E.; Williams, J.A.; Lim, M.; Levine, R.L. Differential susceptibility of plasma proteins to oxidative modification: Examination by western blot immunoassay. Free Radic. Biol. Med. 1994, 17, 429–437. [Google Scholar] [CrossRef]
- Martinez, M.; Weisel, J.W.; Ischiropoulos, H. Functional impact of oxidative posttranslational modifications on fibrinogen and fibrin clots. Free Radic. Biol. Med. 2013, 65, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Wolberg, A.S. Thrombin generation and fibrin clot structure. Blood Rev. 2007, 21, 131–142. [Google Scholar] [CrossRef]
- Colombo, G.; Clerici, M.; Garavaglia, M.E.; Giustarini, D.; Rossi, R.; Milzani, A.; Dalle-Donne, I. A step-by-step protocol for assaying protein carbonylation in biological samples. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2016, 1019, 178–190. [Google Scholar] [CrossRef]
- Trevisan, M.; Browne, R.; Ram, M.; Muti, P.; Freudenheim, J.; Carosella, A.M.; Armstrong, D. Correlates of Markers of Oxidative Status in the General Population. Am. J. Epidemiol. 2001, 154, 348–356. [Google Scholar] [CrossRef]
- Undas, A.; Szułdrzynski, K.; Stepien, E.; Zalewski, J.; Godlewski, J.; Tracz, W.; Pasowicz, M.; Zmudka, K. Reduced clot permeability and susceptibility to lysis in patients with acute coronary syndrome: Effects of inflammation and oxidative stress. Atherosclerosis 2008, 196, 551–557. [Google Scholar] [CrossRef]
- Li, H.; Horke, S.; Förstermann, U. Vascular oxidative stress, nitric oxide and atherosclerosis. Atherosclerosis 2014, 237, 208–219. [Google Scholar] [CrossRef]
- Kearney, K.; Tomlinson, D.; Smith, K.; Ajjan, R. Hypofibrinolysis in diabetes: A therapeutic target for the reduction of cardiovascular risk. Cardiovasc. Diabetol. 2017, 16, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabet, H.Y.; Edwards, W.D.; Tazelaar, H.D.; Daly, R.C. Congenitally bicuspid aortic valves: A surgical pathology study of 542 cases (1991 through 1996) and a literature review of 2715 additional cases. Mayo Clin. Proc. 1999, 74, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Ajjan, R.A.; Gamlen, T.; Standeven, K.F.; Mughal, S.; Hess, K.; Smith, K.A.; Dunn, E.J.; Anwar, M.M.; Rabbani, N.; Thornalley, P.J.; et al. Diabetes is associated with posttranslational modifications in plasminogen resulting in reduced plasmin generation and enzyme-specific activity. Blood 2013, 122, 134–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total Cohort (n = 173) | CLT ≥ 104 min (n = 43) | CLT < 104 min (n = 130) | p-Value |
|---|---|---|---|---|
| Age, years | 67.0 (59.0–72.5) | 67 (57–71) | 67 (59–74) | 0.40 |
| Male, n (%) | 84 (48.6) | 13 (30.2) | 71 (54.6) | 0.006 |
| BMI, kg/m2 | 27.4 (24.6–30.8) | 30.8 (26.6–32.7) | 26.4 (24.1–29.7) | <0.001 |
| Current smoking, n (%) | 36 (20.8) | 8 (18.6) | 28 (21.5) | 0.68 |
| Comorbidities, n (%) | ||||
| Obesity | 55 (31.8) | 25 (58.1) | 30 (23.1) | <0.001 |
| Hyperlipidemia | 35 (20.2) | 15 (34.9) | 20 (15.4) | 0.009 |
| Arterial hypertension | 132 (76.3) | 36 (85.7) | 96 (76.2) | 0.19 |
| Chronic kidney disease | 31 (17.9) | 11 (25.6) | 12 (15.4) | 0.18 |
| Chronic obstructive pulmonary disease | 9 (5.2) | 2 (4.8) | 7 (5.6) | 1.00 |
| Medication, n (%) | ||||
| Aspirin | 91 (52.6) | 23 (57.5) | 68 (56.2) | 0.89 |
| Statin | 118 (74.2) | 28 (70.0) | 90 (75.6) | 0.48 |
| Beta-blocker | 109 (63.0) | 27 (69.2) | 82 (68.3) | 0.92 |
| ACE inhibitor | 82 (47.4) | 26 (65.0) | 56 (47.5) | 0.056 |
| Echocardiographic parameters | ||||
| Ejection fraction, % | 60 (55–65) | 60 (55–65) | 60 (55–65) | 0.73 |
| Mean aortic gradient, mmHg | 50.3 ± 17.7 | 60.0 ± 18.8 | 47.1 ± 16.2 | <0.001 |
| Max aortic gradient, mmHg | 81.4 ± 27.3 | 96.7 ± 29.8 | 76.5 ± 24.7 | <0.001 |
| Aortic valve area, cm2 | 0.8 (0.7–1.0) | 0.8 (0.6–1.0) | 0.8 (0.7–1.0) | 0.14 |
| Routine laboratory investigations | ||||
| Glucose, mmol/L | 5.4 (5.0–5.8) | 5.4 (5.1–5.8) | 5.4 (4.9–5.7) | 0.26 |
| Creatinine, µmol/L | 79 (67–92) | 82 (66–99) | 78 (67–88) | 0.23 |
| Total cholesterol, mmol/L | 4.23 (3.72–5.06) | 4.45 (3.96–5.59) | 4.18 (3.60–4.92) | 0.007 |
| LDL-C, mmol/L | 2.41 (1.94–3.24) | 2.63 (1.96–3.73) | 2.28 (1.93–3.17) | 0.11 |
| HDL-C, mmol/L | 1.40 (1.17–1.76) | 1.41 (1.08–1.79) | 1.38 (1.18–1.75) | 0.87 |
| Triglycerides, mmol/L | 1.16 (0.87–1.68) | 1.57 (1.16–1.98) | 1.03 (0.78–1.52) | <0.001 |
| Lipoprotein (a), mg/dL | 11.9 (4.0–58.2) | 16.6 (4.8–91.4) | 11.2 (3.6–51.0) | 0.11 |
| CRP, mg/L | 1.35 (0.90–2.88) | 1.52 (1.00–3.00) | 1.35 (0.90–2.84) | 0.77 |
| Oxidative stress markers | ||||
| TBARS, nmol/mL | 7.76 (6.78–9.03) | 7.94 (7.19–9.35) | 7.66 (6.63–8.94) | 0.11 |
| Plasma PC, nmol/mg | 2.76 ± 0.45 | 2.97 ± 0.45 | 2.69 ± 0.43 | <0.001 |
| Coagulation | ||||
| Fibrinogen, g/L | 3.41 ± 0.73 | 3.5 ± 0.78 | 3.38 ± 0.71 | 0.36 |
| TF, pg/mL | 80.9 (64.5–92.8) | 82.4 (64.7–90.8) | 79.6 (64.3–93.7) | 0.69 |
| Prothrombin, % | 106.9 ± 15.9 | 112.64 ± 17.16 | 104.99 ± 15.10 | 0.006 |
| Fibrinolysis proteins | ||||
| Plasminogen, % | 97 (89–109) | 102 (92–116) | 95 (87–107) | 0.006 |
| α2-antiplasmin, % | 94.5 ± 7.3 | 98.12 ± 5.85 | 93.27 ± 7.40 | <0.001 |
| PAI-1, ng/mL | 11.5 (7.8–16.8) | 19.9 (13.7–22.4) | 10.0 (7.4–13.7) | <0.001 |
| TAFI, % | 81.8 ± 14.1 | 84.38 ± 15.39 | 84.38 ± 15.39 | 0.16 |
| Fibrin clot properties | ||||
| Ks (thrombin-based), 10−9 cm2 | 4.39 (3.47–5.59) | 4.03 (3.33–5.18) | 4.52 (3.50–5.94) | 0.14 |
| Ks (TF-based), 10−9 cm2 | 5.53 (4.57–6.76) | 5.42 (4.57–6.45) | 5.56 (4.60–6.88) | 0.36 |
| CLT, min | 91.5 (79.3–103.7) | 116.0 (107.6–126.0) | 85.5 (77.0–94.7) | <0.001 |
| Lys50, s | 472 (401–565) | 546 (416–634) | 463 (398–537) | 0.003 |
| Variable | Multivariate * | Multivariate ** (R2 = 0.54) | Multivariate *** (R2 = 0.55) | ||||
|---|---|---|---|---|---|---|---|
| β (95% CI) | R2 | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | |
| Mean aortic gradient | 0.29 (0.14–0.43) | 0.15 | <0.001 | 0.22 (0.11–0.33) | <0.001 | 0.13 (0.02–0.25) | 0.027 |
| Plasma PC | 11.03 (5.21–16.85) | 0.20 | <0.001 | 4.96 (0.25–9.69) | 0.039 | ||
| Prothrombin | 0.41 (0.26–0.57) | 0.21 | <0.001 | 0.24 (0.08–0.39) | 0.003 | ||
| α2-antiplasmin | 0.82 (0.47–1.17) | 0.18 | <0.001 | 0.59 (0.26–0.92) | <0.001 | 0.69 (0.38–1.00) | <0.001 |
| Plasminogen | 0.32 (0.15–0.49) | 0.15 | <0.001 | 0.23 (0.09–0.38) | 0.001 | ||
| PAI-1 | 1.39 (1.06–1.73) | 0.34 | <0.001 | 1.25 (0.98–1.52) | <0.001 | 1.22 (0.92–1.54) | <0.001 |
| Triglycerides | 7.11 (3.31–10.90) | 0.15 | <0.001 | 4.11 (1.17–7.05) | 0.006 | ||
| Lipoprotein(a) | 0.06 (−0.00–0.12) | 0.13 | 0.051 | 0.04 (0.00–0.09) | 0.045 | ||
| TAFI | 0.07 (−0.12–0.25) | 0.08 | 0.49 | −0.11 (−0.25–0.09) | 0.11 | ||
| Maximum aortic gradient | 0.17 (0.07–0.27) | 0.13 | <0.001 | ||||
| Fibrinogen | 4.52 (0.69–8.34) | 0.11 | 0.021 | ||||
| Ks | −2.10 (−3.66– −0.53) | 0.12 | 0.01 | ||||
| Total cholesterol | 5.08 (2.23–7.94) | 0.14 | <0.001 | ||||
| LDL-C | 3.18 (0.27–6.08) | 0.10 | 0.033 | ||||
| Variable | OR per | Univariate * | Multivariate ** | ||
|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| CLT | |||||
| Mean aortic gradient | 1 mmHg | 1.05 (1.03–1.07) | <0.001 | 1.07 (1.03–1.11) | <0.001 |
| Plasma PC | 1 nmol/mg | 6.41 (2.58–17.83) | <0.001 | 5.93 (1.42–29.80) | 0.021 |
| α2-antiplasmin | 1 % | 1.10 (1.04–1.17) | 0.013 | 1.18 (1.08–1.30) | <0.001 |
| Plasminogen | 1% | 1.03 (1.00–1.06) | 0.027 | ||
| PAI-1 | 1 ng/mL | 1.17 (1.10–1.25) | <0.001 | 1.18 (1.09–1.28) | <0.001 |
| Triglycerides | 1 mmol/L | 2.89 (1.63–5.39) | <0.001 | 7.09 (2.75–22.06) | <0.001 |
| Lys50 | |||||
| Plasma PC | 1 nmol/mg | 5.83 (2.23–15.21) | <0.001 | 7.61 (2.44–23.70) | <0.001 |
| TBARS | 1 μM | 1.34 (1.11–1.63) | 0.003 | ||
| α2-antiplasmin | 1 % | 1.16 (1.08–1.25) | <0.001 | 1.11 (1.02–1.20) | 0.013 |
| Fibrinogen | 1 g/L | 3.09 (1.68–5.69) | <0.001 | 2.49 (1.16–5.37) | 0.020 |
| Prothrombin | 1 % | 1.07 (1.03–1.10) | <0.001 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siudut, J.; Natorska, J.; Wypasek, E.; Wiewiórka, Ł.; Ostrowska-Kaim, E.; Wiśniowska-Śmiałek, S.; Plens, K.; Legutko, J.; Undas, A. Impaired Fibrinolysis in Patients with Isolated Aortic Stenosis is Associated with Enhanced Oxidative Stress. J. Clin. Med. 2020, 9, 2002. https://doi.org/10.3390/jcm9062002
Siudut J, Natorska J, Wypasek E, Wiewiórka Ł, Ostrowska-Kaim E, Wiśniowska-Śmiałek S, Plens K, Legutko J, Undas A. Impaired Fibrinolysis in Patients with Isolated Aortic Stenosis is Associated with Enhanced Oxidative Stress. Journal of Clinical Medicine. 2020; 9(6):2002. https://doi.org/10.3390/jcm9062002
Chicago/Turabian StyleSiudut, Jakub, Joanna Natorska, Ewa Wypasek, Łukasz Wiewiórka, Elżbieta Ostrowska-Kaim, Sylwia Wiśniowska-Śmiałek, Krzysztof Plens, Jacek Legutko, and Anetta Undas. 2020. "Impaired Fibrinolysis in Patients with Isolated Aortic Stenosis is Associated with Enhanced Oxidative Stress" Journal of Clinical Medicine 9, no. 6: 2002. https://doi.org/10.3390/jcm9062002
APA StyleSiudut, J., Natorska, J., Wypasek, E., Wiewiórka, Ł., Ostrowska-Kaim, E., Wiśniowska-Śmiałek, S., Plens, K., Legutko, J., & Undas, A. (2020). Impaired Fibrinolysis in Patients with Isolated Aortic Stenosis is Associated with Enhanced Oxidative Stress. Journal of Clinical Medicine, 9(6), 2002. https://doi.org/10.3390/jcm9062002