Nomogram Predicting the Likelihood of Parametrial Involvement in Early-Stage Cervical Cancer: Avoiding Unjustified Radical Hysterectomies

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
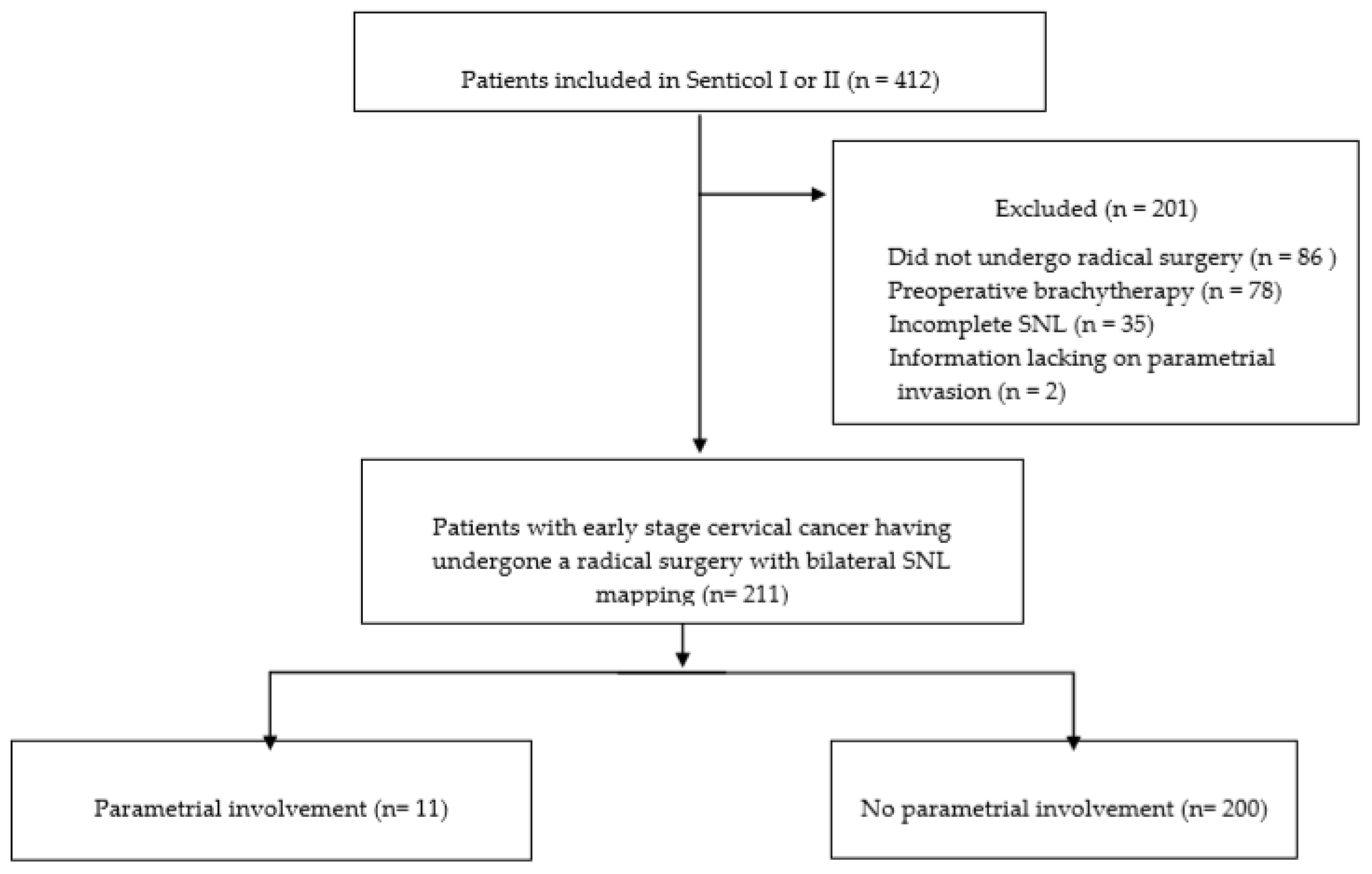
2.1. Population and Data Analysis
2.2. Statistical Analysis
2.3. Development of the Model
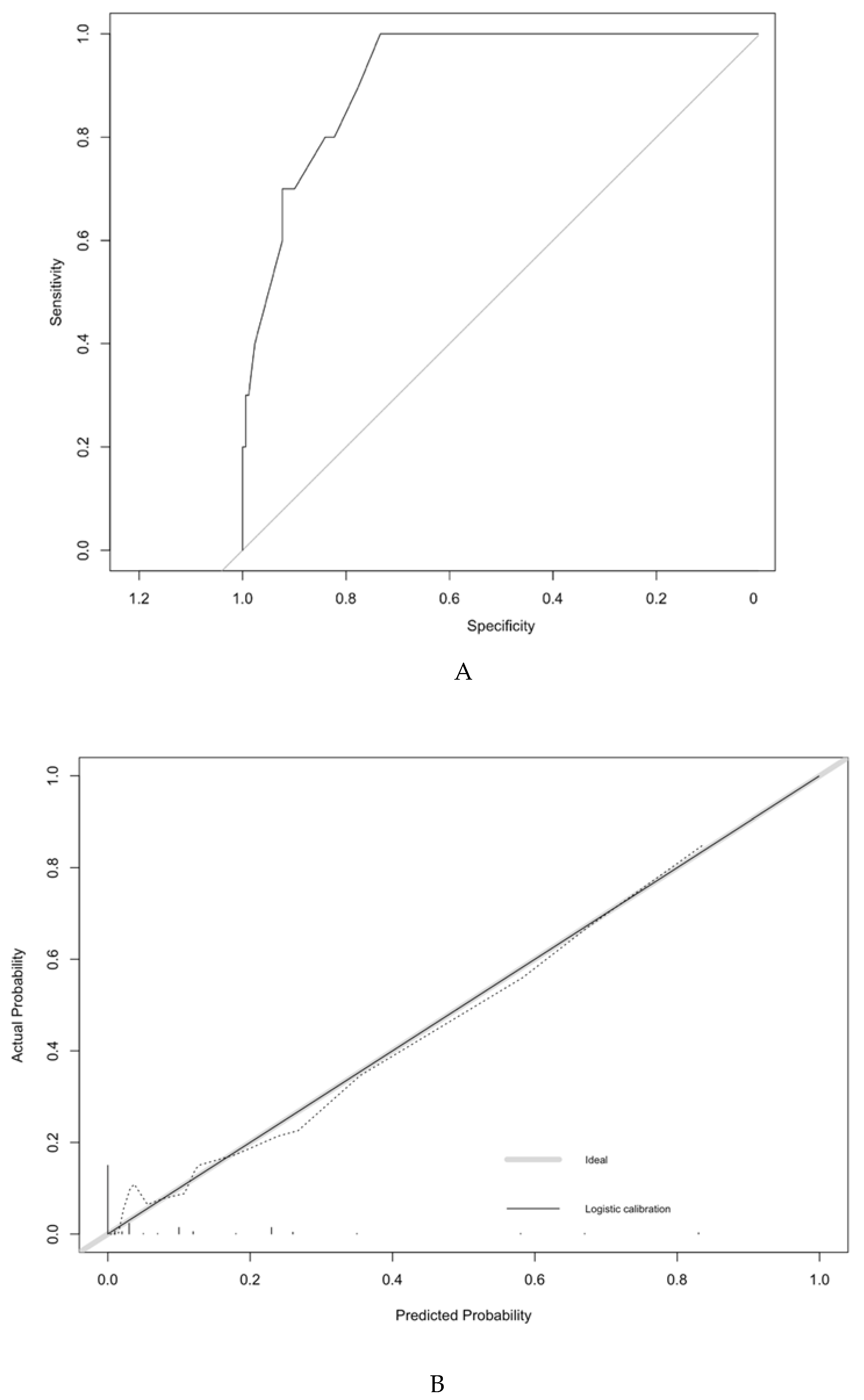
2.4. Accuracy of the Model
2.5. Validation of the Model
2.6. Optimal Threshold of the Model
3. Results
3.1. Population Characteristics
3.2. Likelihood of a Parametrial Involvement
3.3. Development of the Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Covens, A.; Rosen, B.; Murphy, J.; Laframboise, S.; DePetrillo, A.D.; Lickrish, G.; Colgan, T.; Chapman, W.; Shaw, P. How important is removal of the parametrium at surgery for carcinoma of the cervix? Gynecol. Oncol. 2002, 84, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Jung, D.C.; Kim, M.K.; Kang, S.; Seo, S.S.; Cho, J.Y.; Park, N.H.; Song, Y.S.; Park, S.Y.; Kang, S.B.; Kim, J.W. Identification of a patient group at low risk for parametrial invasion in early-stage cervical cancer. Gynecol. Oncol. 2010, 119, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Kong, T.W.; Kim, J.; Son, J.H.; Kang, S.W.; Paek, J.; Chun, M.; Chang, S.J.; Ryu, H.S. Preoperative nomogram for prediction of microscopic parametrial infiltration in patients with FIGO stage IB cervical cancer treated with radical hysterectomy. Gynecol. Oncol. 2016, 142, 109–114. [Google Scholar] [CrossRef]
- Dabi, Y.; Willecocq, C.; Ballester, M.; Carcopino, X.; Bendifallah, S.; Ouldamer, L.; Lavoue, V.; Canlorbe, G.; Raimond, E.; Coutant, C.; et al. Identification of a low risk population for parametrial invasion in patients with early-stage cervical cancer. J. Transl. Med. 2018, 14, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonneau, C.; Cortez, A.; Lis, R.; Mirshahi, M.; Fauconnier, A.; Ballester, M.; Daraï, E.; Touboul, C. Lymphatic and nerve distribution throughout the parametrium. Gynecol. Oncol. 2013, 131, 708–713. [Google Scholar] [CrossRef]
- Touboul, C.; Fauconnier, A.; Zareski, E.; Bouhanna, P.; Daraï, E. The lateral infraureteral parametrium: Myth or reality? Am. J. Obstet. Gynecol. 2008, 199, 242.e1–242.e6. [Google Scholar] [CrossRef]
- Rob, L.; Halaska, M.; Robova, H. Nerve-sparing and individually tailored surgery for cervical cancer. Lancet Oncol. 2010, 11, 292–301. [Google Scholar] [CrossRef]
- Sood, A.K.; Nygaard, I.; Shahin, M.S.; Sorosky, J.I.; Lutgendorf, S.K.; Rao, S.S.C. Anorectal dysfunction after surgical treatment for cervical cancer. J. Am. Coll Surg. 2002, 195, 513–519. [Google Scholar] [CrossRef]
- Selcuk, S.; Cam, C.; Asoglu, M.R.; Kucukbas, M.; Arinkan, A.; Cikman, M.S.; Karateke, A. Effect of simple and radical hysterectomy on quality of life-analysis of all aspects of pelvic floor dysfunction. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 198, 84–88. [Google Scholar] [CrossRef]
- Benedetti-Panici, P.; Maneschi, F.; D’Andrea, G.; Cutillo, G.; Rabitti, C.; Congiu, M.; Coronetta, F.; Capelli, A. Early cervical carcinoma: The natural history of lymph node involvement redefined on the basis of thorough parametrectomy and giant section study. Cancer 2000, 88, 2267–2274. [Google Scholar] [CrossRef]
- Roh, J.W.; Lee, D.O.; Suh, D.H.; Lim, M.C.; Seo, S.S.; Chung, J.; Lee, S.; Park, S.Y. Efficacy and oncologic safety of nerve-sparing radical hysterectomy for cervical cancer: A randomized controlled trial. J. Gynecol. Oncol. 2015, 26, 90–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raspagliesi, F.; Ditto, A.; Fontanelli, R.; Solima, E.; Hanozet, F.; Zanaboni, F.; Kusamura, S. Nerve-sparing radical hysterectomy: A surgical technique for preserving the autonomic hypogastric nerve. Gynecol. Oncol. 2004, 93, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Possover, M.; Quakernack, J.; Chiantera, V. The LANN technique to reduce postoperative functional morbidity in laparoscopic radical pelvic surgery. J. Am. Coll Surg. 2005, 201, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Querleu, D.; Morrow, C.P. Classification of radical hysterectomy. Lancet Oncol. 2008, 9, 297–303. [Google Scholar] [CrossRef]
- Querleu, D.; Cibula, D.; Abu-Rustum, N.R. 2017 Update on the Querleu-Morrow Classification of Radical Hysterectomy. Ann. Surg. Oncol. 2017, 24, 3406–3412. [Google Scholar] [CrossRef] [PubMed]
- Recommendations | ESGO Gynae-Oncology Guidelines. Available online: https://guidelines.esgo.org/cervical-cancer/guidelines/recommendations/ (accessed on 6 January 2020).
- Wright, J.D.; Grigsby, P.W.; Brooks, R.; Powell, M.A.; Gibb, R.K.; Gao, F.; Rader, J.S.; Mutch, D.G. Utility of parametrectomy for early stage cervical cancer treated with radical hysterectomy. Cancer 2007, 110, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Frumovitz, M.; Sun, C.C.; Schmeler, K.M.; Deavers, M.T.; Dos Reis, R.; Levenback, C.F.; Ramirez, P.T. Parametrial involvement in radical hysterectomy specimens for women with early-stage cervical cancer. Obstet. Gynecol. 2009, 114, 93–99. [Google Scholar] [CrossRef]
- Yamazaki, H.; Todo, Y.; Okamoto, K.; Yamashiro, K.; Kato, H. Pretreatment risk factors for parametrial involvement in FIGO stage IB1 cervical cancer. J. Gynecol. Oncol. 2015, 26, 255–261. [Google Scholar] [CrossRef]
- Daraï, E.; Lavoué, V.; Rouzier, R.; Coutant, C.; Barranger, E.; Bats, A.-S. Contribution of the sentinel node procedure to tailoring the radicality of hysterectomy for cervical cancer. Gynecol. Oncol. 2007, 106, 251–256. [Google Scholar] [CrossRef]
- Bats, A.S.; Buénerd, A.; Querleu, D.; Leblanc, E.; Daraï, E.; Morice, P.; Marret, H.; Gillaizeau, F.; Mathevet, P.; Lécuru, F. Diagnostic value of intraoperative examination of sentinel lymph node in early cervical cancer: A prospective, multicenter study. Gynecol. Oncol. 2011, 123, 230–235. [Google Scholar] [CrossRef]
- Chung, H.H.; Kang, S.B.; Cho, J.Y.; Kim, J.W.; Park, N.H.; Song, Y.S.; Kim, S.H.; Lee, H.P. Can preoperative MRI accurately evaluate nodal and parametrial invasion in early stage cervical cancer? Jpn. J. Clin. Oncol. 2007, 37, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Sahdev, A.; Sohaib, S.A.; Wenaden, A.E.T.; Shepherd, J.H.; Reznek, R.H. The performance of magnetic resonance imaging in early cervical carcinoma: A long-term experience. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2007, 17, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Bipat, S.; Glas, A.S.; van der Velden, J.; Zwinderman, A.H.; Bossuyt, P.M.M.; Stoker, J. Computed tomography and magnetic resonance imaging in staging of uterine cervical carcinoma: A systematic review. Gynecol. Oncol. 2003, 91, 59–66. [Google Scholar] [CrossRef]
- Moro, F.; Gui, B.; Arciuolo, D.; Bertoldo, V.; Borzi, R.; Romeo, P.; Petta, F.; Cambi, F.; Pasciuto, T.; Zannoni, G.F.; et al. Fusion imaging of ultrasound and MRI in the assessment of locally advanced cervical cancer: A prospective study. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2020, 30, 456–465. [Google Scholar] [CrossRef]
- Harrell, F.E.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiol. Camb. Mass. 2005, 16, 73–81. [Google Scholar] [CrossRef]
- Pluta, M.; Rob, L.; Charvat, M.; Chmel, R.; Halaska, M., Jr.; Skapa, P.; Robova, H. Less radical surgery than radical hysterectomy in early stage cervical cancer: A pilot study. Gynecol. Oncol. 2009, 113, 181–184. [Google Scholar] [CrossRef]
- Strnad, P.; Robova, H.; Skapa, P.; Pluta, M.; Hrehorcak, M.; Halaska, M.; Rob, L. A prospective study of sentinel lymph node status and parametrial involvement in patients with small tumour volume cervical cancer. Gynecol. Oncol. 2008, 109, 280–284. [Google Scholar] [CrossRef]
- Bidus, M.A.; Caffrey, A.S.; You, W.B.; Amezcua, C.A.; Chernofsky, M.R.; Barner, R.; Seidman, J.; Rose, G.S. Cervical biopsy and excision procedure specimens lack sufficient predictive value for lymph-vascular space invasion seen at hysterectomy for cervical cancer. Am. J. Obstet. Gynecol. 2008, 199, 151.e1–151.e4. [Google Scholar]
- Stegeman, M.; Louwen, M.; van der Velden, J.; ten Kate, F.J.W.; den Bakker, M.A.; Burger, C.W.; Ansink, A.C. The incidence of parametrial tumor involvement in select patients with early cervix cancer is too low to justify parametrectomy. Gynecol. Oncol. 2007, 105, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Alcázar, J.L.; García, E.; Machuca, M.; Quintana, R.; Escrig, J.; Chacón, E.; Mínguez, J.A.; Chiva, L. Magnetic resonance imaging and ultrasound for assessing parametrial infiltration in cervical cancer. A systematic review and meta-analysis. Med. Ultrason. 2020, 22, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Kinney, W.K.; Hodge, D.O.; Egorshin, E.V.; Ballard, D.J.; Podratz, K.C. Identification of a low-risk subset of patients with stage IB invasive squamous cancer of the cervix possibly suited to less radical surgical treatment. Gynecol. Oncol. 1995, 57, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Jiamset, I.; Hanprasertpong, J. Risk Factors for Parametrial Involvement in Early-Stage Cervical Cancer and Identification of Patients Suitable for Less Radical Surgery. Oncol. Res. Treat. 2016, 39, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.-C.; Tai, Y.-J.; Chen, Y.-L.; Chiang, Y.-C.; Chen, C.-A.; Cheng, W.-F. Factors predicting parametrial invasion in patients with early-stage cervical carcinomas. PLoS ONE 2018, 13, e0204950. [Google Scholar] [CrossRef]
- Landoni, F.; Maneo, A.; Cormio, G.; Perego, P.; Milani, R.; Caruso, O.; Mangioni, C. Class II versus class III radical hysterectomy in stage IB-IIA cervical cancer: A prospective randomized study. Gynecol. Oncol. 2001, 80, 3–12. [Google Scholar] [CrossRef]
- Balaya, V.; Lécuru, F.; Magaud, L.; Ngô, C.; Huchon, C.; Bats, A.S.; Mathevet, P. Perioperative morbidity of radical trachelectomy with lymphadenectomy in early-stage cervical cancer: A French prospective multicentric cohort. J. Gynecol. Oncol. 2019, 30, e34. [Google Scholar] [CrossRef] [Green Version]
- Dedden, S.J.; Geomini, P.M.A.J.; Huirne, J.A.F.; Bongers, M.Y. Vaginal and Laparoscopic hysterectomy as an outpatient procedure: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 216, 212–223. [Google Scholar] [CrossRef]
- Radical Versus Simple Hysterectomy and Pelvic Node Dissection With Low-risk Early Stage Cervical Cancer-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT01658930 (accessed on 6 January 2020).
- Cibula, D.; McCluggage, W.G. Sentinel lymph node (SLN) concept in cervical cancer: Current limitations and unanswered questions. Gynecol. Oncol. 2019, 152, 202–207. [Google Scholar] [CrossRef]
- Rychlik, A.; Angeles, M.A.; Migliorelli, F.; Croce, S.; Mery, E.; Martinez, A.; Ferron, G.; Guyon, F.; Querleu, D. Frozen section examination of sentinel lymph nodes can be used as a decisional tool in the surgical management of early cervical cancer. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2020, 30, 358–363. [Google Scholar] [CrossRef]
- Martínez, A.; Mery, E.; Filleron, T.; Boileau, L.; Ferron, G.; Querleu, D. Accuracy of intraoperative pathological examination of SLN in cervical cancer. Gynecol. Oncol. 2013, 130, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Guani, B.; Dorez, M.; Magaud, L.; Buenerd, A.; Lecuru, F.; Mathevet, P. Impact of micrometastasis or isolated tumor cells on recurrence and survival in patients with early cervical cancer: SENTICOL Trial. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2019, 29, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Abu-Rustum, N.R.; Dusek, L.; Zikán, M.; Zaal, A.; Sevcik, L.; Kenter, G.G.; Querleu, D.; Jach, R.; Bats, A.S.; et al. Prognostic significance of low volume sentinel lymph node disease in early-stage cervical cancer. Gynecol. Oncol. 2012, 124, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, R.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Predictive Variable | Total Population n = 211 | Group without Parametrial Invasion n = 200 | Group with Parametrial Invasion n = 11 | p | |||
|---|---|---|---|---|---|---|---|
| n or Mean ± SD | (%) or (Range) | n or Mean ± SD | (%) or (Range) | n or Mean ± SD | (%) or (Range) | ||
| Age (years) | |||||||
| Mean ± SD | 43.2 ± 11.6 | (22–85) | 43.1 ± 11.6 | (22–85) | 45.4 ± 12.4 | (31–77) | 0.52 |
| <50 | 165 | 78.2 | 156 | 78 | 9 | 81.8 | 0.42 |
| 50–70 | 39 | 18.5 | 38 | 19 | 1 | 9.1 | |
| >70 | 7 | 3.3 | 6 | 3 | 1 | 9.1 | |
| BMI (kg/m2) | |||||||
| Mean ± SD | 23.5 ± 5.1 | (14.6–42.2) | 23.3 ± 4.9 | (14.6–41.4) | 27.1 ± 7.8 | (18–42.2) | 0.02 |
| <18.5 | 18 | 8.5 | 17 | 8.5 | 1 | 9.1 | 0.43 |
| 18.5–25 | 139 | 65.9 | 133 | 66.5 | 6 | 54.5 | |
| <25–30 | 29 | 13.7 | 28 | 14.0 | 1 | 9.1 | |
| >30 | 25 | 11.8 | 22 | 11.0 | 3 | 27.3 | |
| Parity | |||||||
| 0 | 50 | 23.7 | 48 | 24.0 | 2 | 18.2 | 0.66 |
| ≥1 | 161 | 76.3 | 152 | 76.0 | 9 | 81.8 | |
| Menopausal status | |||||||
| Yes | 52 | 24.6 | 49 | 24.5 | 3 | 27.3 | 0.83 |
| No | 159 | 75.4 | 151 | 75.5 | 8 | 72.7 | |
| Clinical FIGO stage | |||||||
| IA1 with emboli-IA2 | 24 | 11.5 | 24 | 12.1 | 0 | 0.0 | 0.63 |
| IB1 | 115 | 55.0 | 108 | 54.5 | 7 | 63.6 | |
| IB2 | 67 | 32.1 | 63 | 31.8 | 4 | 36.4 | |
| IIA1 | 3 | 1.4 | 3 | 1.5 | 0 | 0.0 | |
| Not specified | 2 | 2 | |||||
| Histology | |||||||
| Squamous cell carcinoma | 142 | 67.6 | 132 | 67.9 | 10 | 90.9 | 0.23 |
| Adenocarcinoma | 61 | 29.0 | 60 | 29.6 | 1 | 9.1 | |
| Other type | 7 | 3.3 | 7 | 2.6 | 0 | 0.0 | |
| Not specified | 1 | 1 | |||||
| Grade of differentiation | |||||||
| G1 | 65 | 43.3 | 63 | 44.7 | 2 | 22.2 | 0.41 |
| G2 | 58 | 38.7 | 53 | 37.6 | 5 | 55.6 | |
| G3 | 27 | 18.0 | 25 | 17.7 | 2 | 22.2 | |
| Not specified | 61 | 59 | 2 | 2 | |||
| Type of surgery | |||||||
| Radical Hysterectomy | 160 | 75.8 | 150 | 75.0 | 10 | 90.9 | 0.23 |
| Radical Trachelectomy | 51 | 24.2 | 50 | 25.0 | 1 | 9.1 | |
| Type of Lymph node staging | |||||||
| SLN biopsy alone | 65 | 30.8 | 64 | 32.0 | 1 | 9.1 | 0.11 |
| SLN biopsy + Pelvic lymphadenectomy | 146 | 69.2 | 136 | 68.0 | 10 | 90.9 | |
| Node status | |||||||
| Patients with positive SLN | |||||||
| Yes | 29 | 13.7 | 23 | 11.5 | 6 | 54.5 | <0.0001 |
| No | 182 | 86.3 | 177 | 88.5 | 5 | 45.5 | |
| SLN status | |||||||
| Macrometastasis | 8 | 3.8 | 5 | 2.5 | 3 | 27.3 | <0.0001 |
| Micrometastasis | 10 | 4.7 | 9 | 4.5 | 1 | 9.1 | |
| ITC | 11 | 5.2 | 9 | 4.5 | 2 | 18.2 | |
| Negative | 182 | 86.3 | 177 | 88.5 | 5 | 45.5 | |
| Final pathological exam | |||||||
| Tumor size | |||||||
| Mean (mm) ± SD | 10 ± 11.9 | (0–60) | 9 ± 11.1 | (0–60) | 28.5 ± 10.9 | (15–50) | <0.0001 |
| <20 mm | 158 | 76.7 | 156 | 80 | 2 | 18.2 | <0.0001 |
| ≥20 mm | 48 | 23.3 | 39 | 20 | 9 | 81.8 | |
| Not specified | 5 | 5 | |||||
| Deep stromal invasion | |||||||
| Mean (mm) ± SD | 5.6 ± 7.7 | (0–40) | 4.3 ± 7.8 | (0–40) | 17.6 ± 8.3 | (6–30) | <0.0001 |
| <10 mm | 136 | 75.1 | 134 | 78.4 | 2 | 20.0 | <0.0001 |
| ≥10 mm | 45 | 24.9 | 37 | 21.6 | 8 | 80.0 | |
| Not specified | 30 | 29 | 1 | ||||
| Lympho-vascular space invasion | |||||||
| Yes | 71 | 33.6 | 62 | 31.0 | 9 | 81.8 | 0.001 |
| No | 140 | 66.4 | 138 | 69.0 | 2 | 18.2 | |
| Vaginal invasion | |||||||
| Yes | 11 | 5.3 | 5 | 2.5 | 6 | 54.5 | <0.0001 |
| No | 198 | 94.7 | 193 | 97.5 | 5 | 45.5 | |
| Not specified | 2 | 2 | |||||
| Positive margin | |||||||
| Yes | 10 | 4.8 | 6 | 3.0 | 4 | 36.4 | <0.0001 |
| No | 199 | 95.2 | 192 | 97.0 | 7 | 63.6 | |
| Not specified | 2 | 2 | |||||
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variable | Odds Ratio | IC 95% | p | ORa | IC 95% | p |
| Body mass index (kg/m2) | ||||||
| 1.1 | 1.01–1.22 | 0.03 | 1.11 | 0.98–1.27 | 0.11 | |
| Sentinel lymph node status | ||||||
| Negative | 1 | 1 | ||||
| ITC | 3.93 | 0.41–37.28 | 0.23 | 1.63 | 0.13–19.65 | 0.7 |
| Micrometastasis | 7.86 | 1.34–46.24 | 0.02 | 9.91 | 0.53–183.19 | 0.12 |
| Macrometastasis | 21.24 | 3.94–114.52 | <0.001 | 16.34 | 1.33–199.89 | 0.03 |
| Tumor size | ||||||
| <20 mm | 1 | 1 | ||||
| ≥20 mm | 18 | 3.74–86.68 | <0.001 | 6.55 | 0.81–53.31 | 0.08 |
| Deep stromal invasion | ||||||
| <10 mm | 1 | 1 | ||||
| ≥10 mm | 14.49 | 2.95–71.16 | <0.001 | 5.55 | 0.49–63.4 | 0.17 |
| Presence of lympho-vascular space involvement | ||||||
| No | 1 | 1 | ||||
| Yes | 10.02 | 2.10–47.72 | <0.001 | 2.25 | 0.33–15.23 | 0.41 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benoit, L.; Balaya, V.; Guani, B.; Bresset, A.; Magaud, L.; Bonsang-Kitzis, H.; Ngô, C.; Mathevet, P.; Lécuru, F. Nomogram Predicting the Likelihood of Parametrial Involvement in Early-Stage Cervical Cancer: Avoiding Unjustified Radical Hysterectomies. J. Clin. Med. 2020, 9, 2121. https://doi.org/10.3390/jcm9072121
Benoit L, Balaya V, Guani B, Bresset A, Magaud L, Bonsang-Kitzis H, Ngô C, Mathevet P, Lécuru F. Nomogram Predicting the Likelihood of Parametrial Involvement in Early-Stage Cervical Cancer: Avoiding Unjustified Radical Hysterectomies. Journal of Clinical Medicine. 2020; 9(7):2121. https://doi.org/10.3390/jcm9072121
Chicago/Turabian StyleBenoit, Louise, Vincent Balaya, Benedetta Guani, Arnaud Bresset, Laurent Magaud, Helene Bonsang-Kitzis, Charlotte Ngô, Patrice Mathevet, and Fabrice Lécuru. 2020. "Nomogram Predicting the Likelihood of Parametrial Involvement in Early-Stage Cervical Cancer: Avoiding Unjustified Radical Hysterectomies" Journal of Clinical Medicine 9, no. 7: 2121. https://doi.org/10.3390/jcm9072121
APA StyleBenoit, L., Balaya, V., Guani, B., Bresset, A., Magaud, L., Bonsang-Kitzis, H., Ngô, C., Mathevet, P., & Lécuru, F. (2020). Nomogram Predicting the Likelihood of Parametrial Involvement in Early-Stage Cervical Cancer: Avoiding Unjustified Radical Hysterectomies. Journal of Clinical Medicine, 9(7), 2121. https://doi.org/10.3390/jcm9072121