Use of Guselkumab for the Treatment of Moderate-to-Severe Plaque Psoriasis: A 1 Year Real-Life Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Patients and Study Design
2.2. Outcome Measures
2.3. Safety
2.4. Statistical Analysis
3. Results
3.1. Patient Demographic and Clinical Characteristics
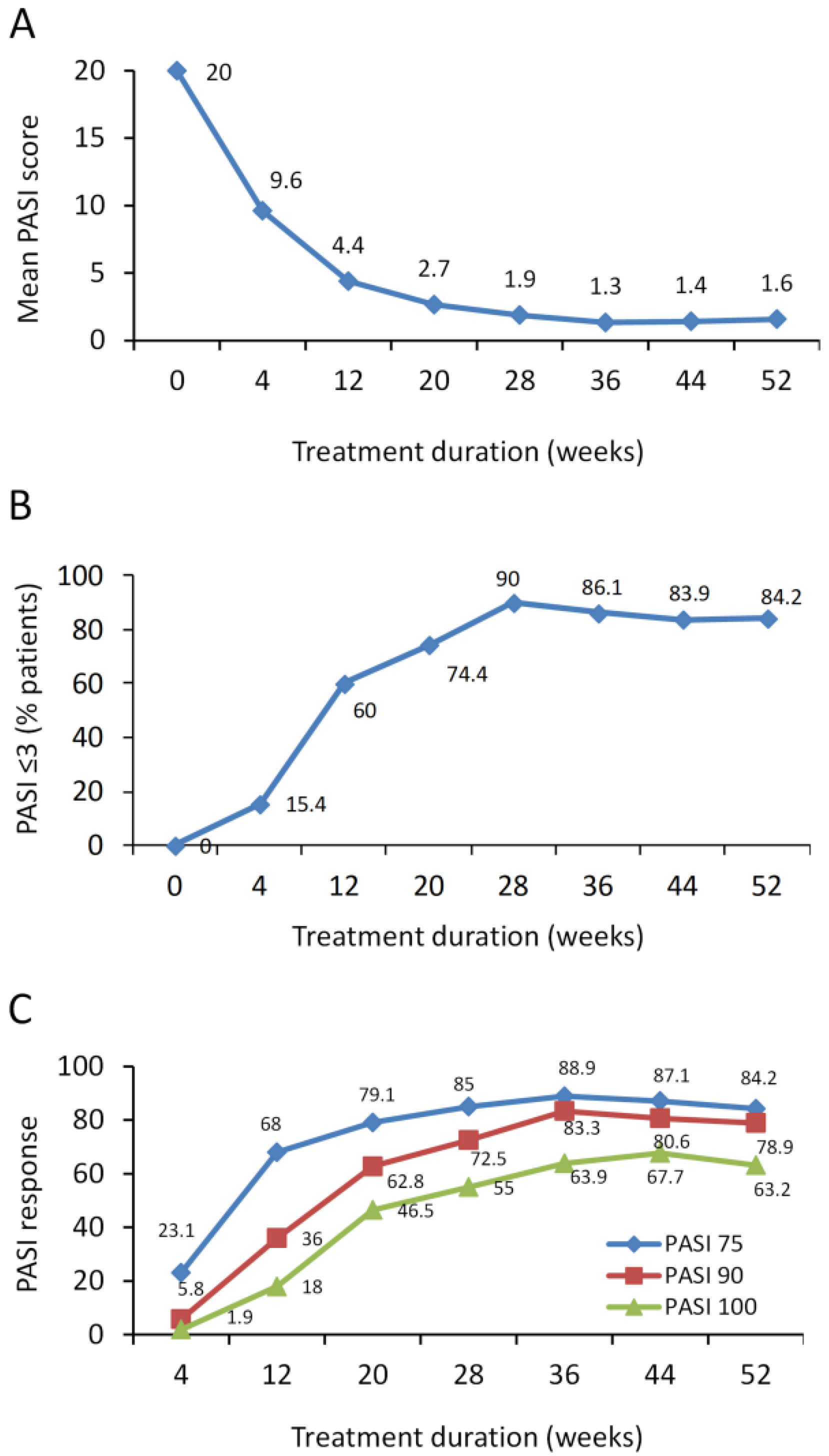
3.2. PASI Response
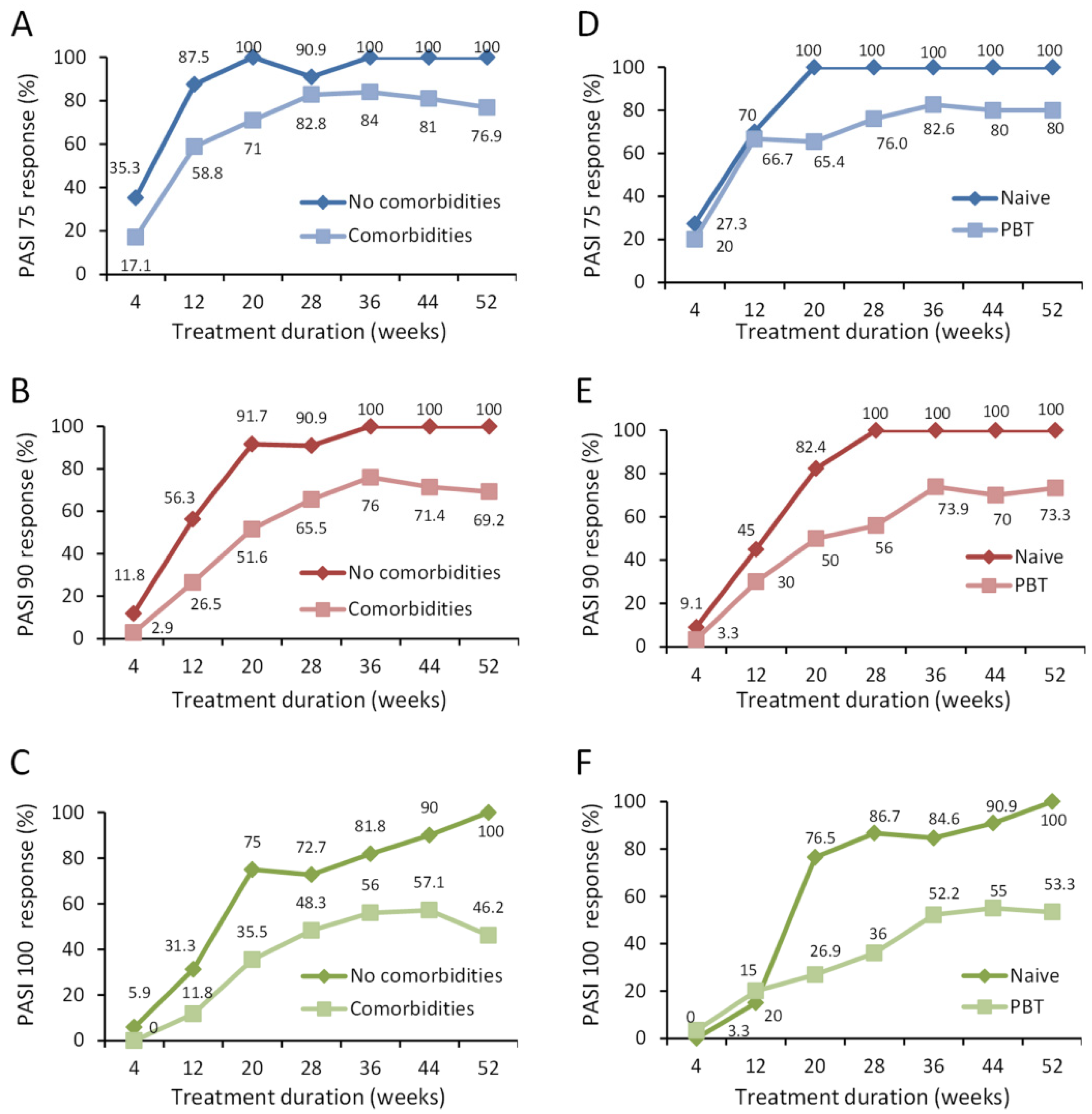
3.3. PASI Response in Different Patient Subgroups
3.4. Predictors of Improved PASI Response
3.5. Safety
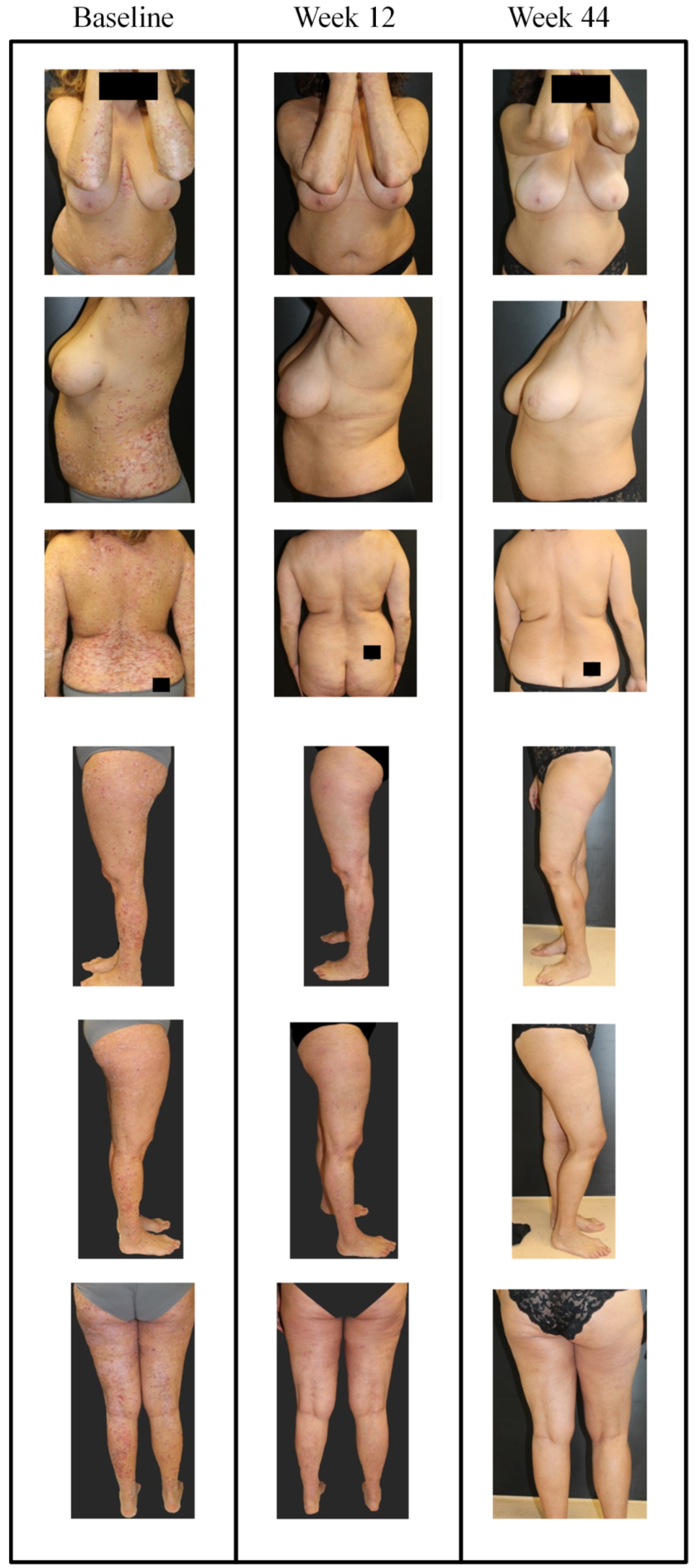
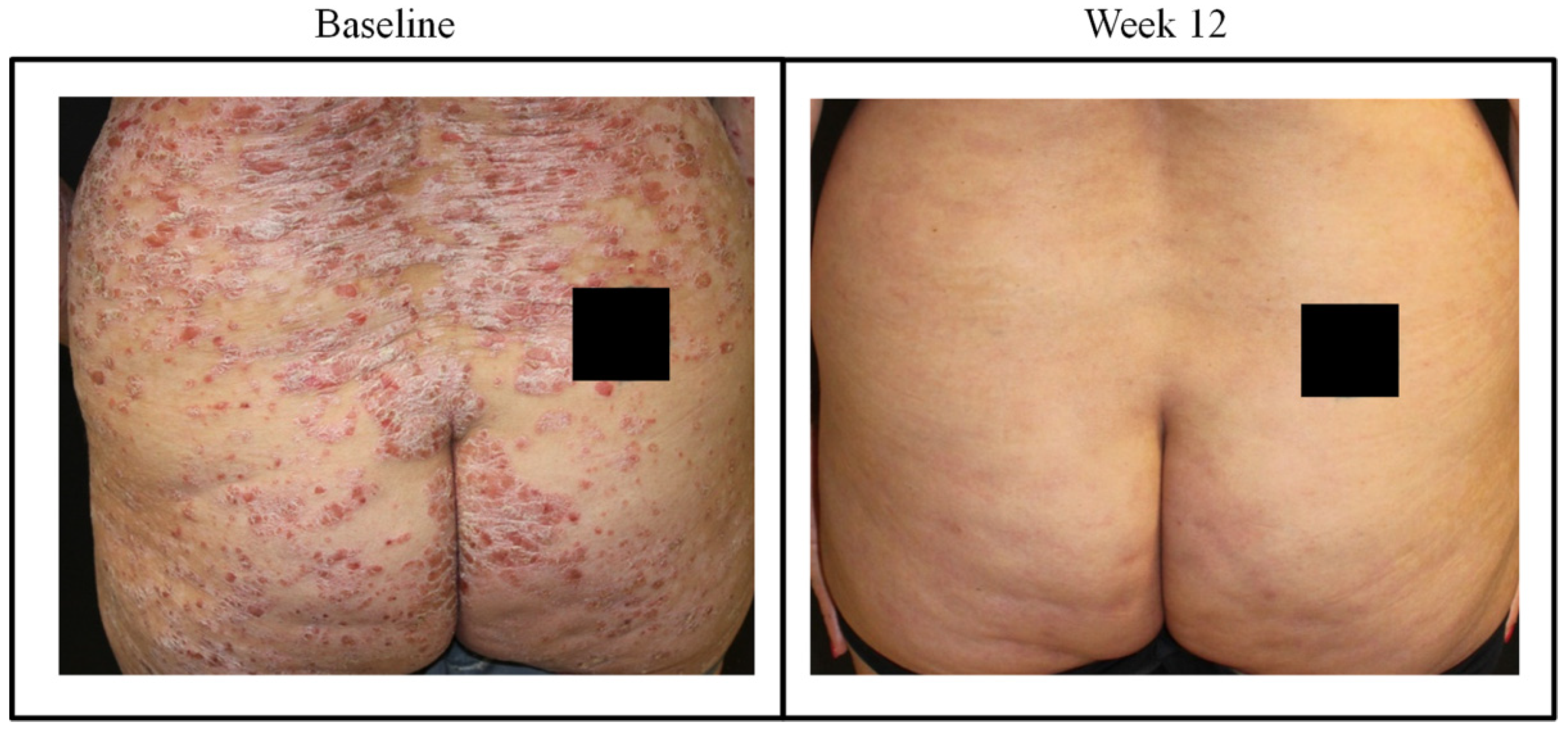
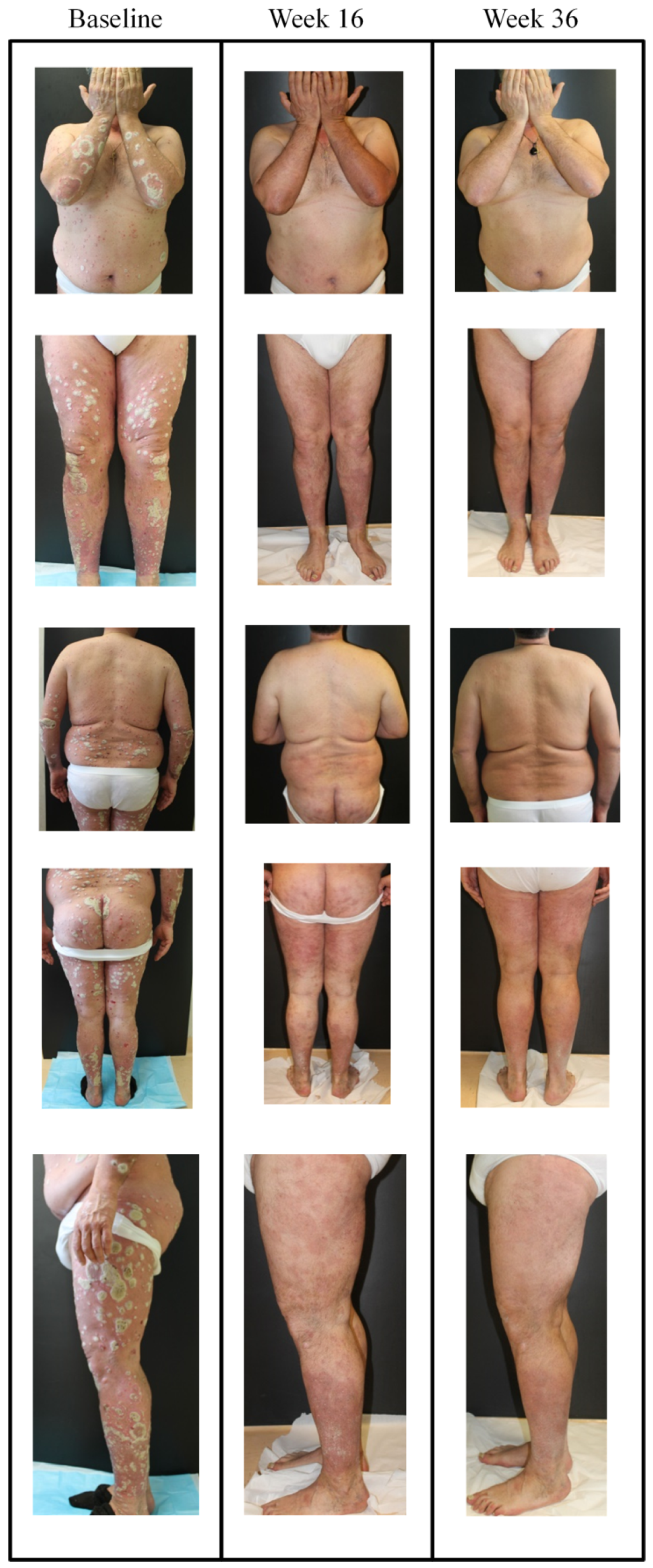
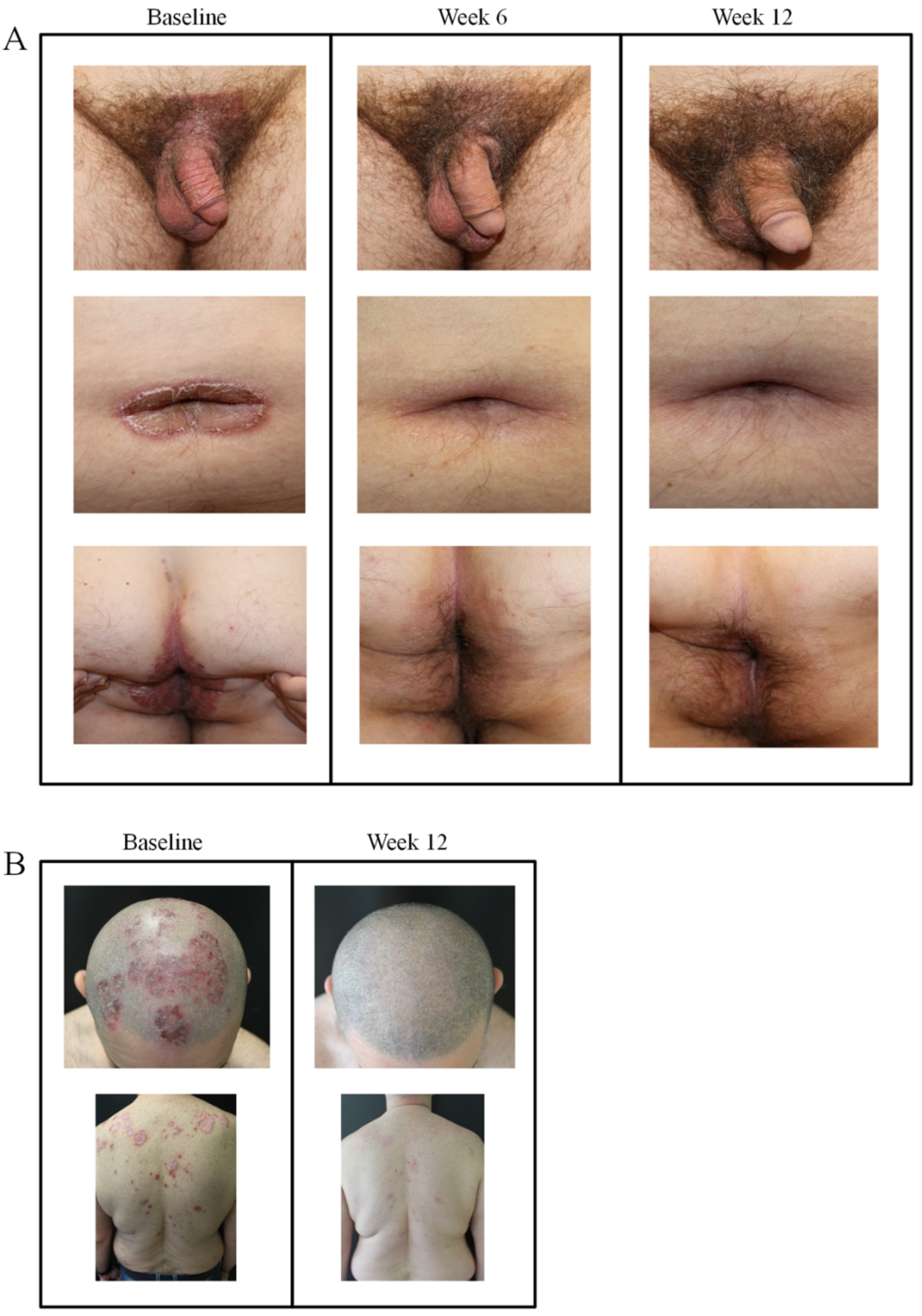
3.6. Difficult-to-Treat Locations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Parisi, R.; Symmons, D.P.M.; Griffiths, C.E.M.; Ashcroft, D.M. Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farley, E.; Menter, A. Psoriasis: Comorbidities and associations. G. Ital. Dermatol. Venereol. 2011, 146, 9–15. [Google Scholar] [PubMed]
- Krueger, G.; Koo, J.; Lebwohl, M.; Menter, A.; Stern, R.S.; Rolstad, T. The impact of psoriasis on quality of life: Results of a 1998 National Psoriasis Foundation patient-membership survey. Arch. Dermatol. 2001, 137, 280–284. [Google Scholar] [PubMed]
- Papp, K.A.; Langley, R.G.; Lebwohl, M.; Krueger, G.G.; Szapary, P.; Yeilding, N.; Guzzo, C.; Hsu, M.-C.; Wang, Y.; Li, S.; et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 52-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 2). Lancet 2008, 371, 1675–1684. [Google Scholar] [CrossRef]
- Griffiths, C.E.M.; Reich, K.; Lebwohl, M.; van de Kerkhof, P.; Paul, C.; Menter, A.; Cameron, G.S.; Erickson, J.; Zhang, L.; Secrest, R.J.; et al. Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis (UNCOVER-2 and UNCOVER-3): Results from two phase 3 randomised trials. Lancet 2015, 386, 541–551. [Google Scholar] [CrossRef]
- Langley, R.G.; Elewski, B.E.; Lebwohl, M.; Reich, K.; Griffiths, C.E.M.; Papp, K.; Puig, L.; Nakagawa, H.; Spelman, L.; Sigurgeirsson, B.; et al. Secukinumab in plaque psoriasis--results of two phase 3 trials. N. Engl. J. Med. 2014, 371, 326–338. [Google Scholar] [CrossRef] [Green Version]
- Blauvelt, A.; Papp, K.A.; Griffiths, C.E.M.; Randazzo, B.; Wasfi, Y.; Shen, Y.-K.; Li, S.; Kimball, A.B. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: Results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J. Am. Acad. Dermatol. 2017, 76, 405–417. [Google Scholar] [CrossRef] [Green Version]
- Reich, K.; Armstrong, A.W.; Foley, P.; Song, M.; Wasfi, Y.; Randazzo, B.; Li, S.; Shen, Y.-K.; Gordon, K.B. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: Results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J. Am. Acad. Dermatol. 2017, 76, 418–431. [Google Scholar] [CrossRef] [Green Version]
- Galluzzo, M.; D’Adamio, S.; Silvaggio, D.; Lombardo, P.; Massaro, A.; Egan, C.G.; Bianchi, L.; Talamonti, M. Ustekinumab treatment for moderate-to-severe plaque psoriasis: Eight-year real-life experience. Expert Opin. Biol. Ther. 2020, 20, 95–104. [Google Scholar] [CrossRef]
- Kimball, A.B.; Jacobson, C.; Weiss, S.; Vreeland, M.G.; Wu, Y. The psychosocial burden of psoriasis. Am. J. Clin. Dermatol. 2005, 6, 383–392. [Google Scholar] [CrossRef]
- Gisondi, P.; Altomare, G.; Ayala, F.; Bardazzi, F.; Bianchi, L.; Chiricozzi, A.; Costanzo, A.; Conti, A.; Dapavo, P.; De Simone, C.; et al. Italian guidelines on the systemic treatments of moderate-to-severe plaque psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 774–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gisondi, P.; Del Giglio, M.; Girolomoni, G. Treatment Approaches to Moderate to Severe Psoriasis. Int. J. Mol. Sci. 2017, 18, 2427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, K.B.; Duffin, K.C.; Bissonnette, R.; Prinz, J.C.; Wasfi, Y.; Li, S.; Shen, Y.-K.; Szapary, P.; Randazzo, B.; Reich, K. A Phase 2 Trial of Guselkumab versus Adalimumab for Plaque Psoriasis. N. Engl. J. Med. 2015, 373, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Galluzzo, M.; D’Adamio, S.; Campione, E.; Bianchi, L.; Talamonti, M. A safety evaluation of guselkumab for the treatment of psoriasis. Expert Opin. Drug. Saf. 2018, 17, 741–751. [Google Scholar] [CrossRef]
- Langley, R.G.; Tsai, T.-F.; Flavin, S.; Song, M.; Randazzo, B.; Wasfi, Y.; Jiang, J.; Li, S.; Puig, L. Efficacy and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: Results of the randomized, double-blind, phase III NAVIGATE trial. Br. J. Dermatol. 2018, 178, 114–123. [Google Scholar] [CrossRef] [Green Version]
- Gordon, K.B.; Blauvelt, A.; Foley, P.; Song, M.; Wasfi, Y.; Randazzo, B.; Shen, Y.K.; You, Y.; Griffiths, C.E.M. Efficacy of guselkumab in subpopulations of patients with moderate-to-severe plaque psoriasis: A pooled analysis of the phase III VOYAGE 1 and VOYAGE 2 studies. Br. J. Dermatol. 2018, 178, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, A.; Blauvelt, A.; Flavin, S.; Hsu, M.; Randazzo, B.; Reich, K.; Langley, R. Guselkumab Demonstrates Greater Efficacy Compared to Secukinumab Across Body Weight Quartiles and Body Mass Index Categories: Week 48 Results From the ECLIPSE Trial. 2. In Proceedings of the 28th EADV Congress, Madrid, Spain, 9–13 October 2019. Abstract P1631. [Google Scholar]
- Foley, P.; Gordon, K.; Griffiths, C.E.M.; Wasfi, Y.; Randazzo, B.; Song, M.; Li, S.; Shen, Y.-K.; Blauvelt, A. Efficacy of Guselkumab Compared With Adalimumab and Placebo for Psoriasis in Specific Body Regions: A Secondary Analysis of 2 Randomized Clinical Trials. JAMA Dermatol. 2018, 154, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Warren, R.B.; Brown, B.C.; Lavery, D.; Ashcroft, D.M.; Griffiths, C.E.M. Biologic therapies for psoriasis: Practical experience in a U.K. tertiary referral centre. Br. J. Dermatol. 2009, 160, 162–169. [Google Scholar] [CrossRef]
- Warren, R.B.; Brown, B.C.; Lavery, D.; Griffiths, C.E.M. Adalimumab for psoriasis: Practical experience in a U.K. tertiary referral centre. Br. J. Dermatol. 2010, 163, 859–862. [Google Scholar] [CrossRef]
- Laws, P.M.; Downs, A.M.; Parslew, R.; Dever, B.; Smith, C.H.; Barker, J.N.; Moriarty, B.; Murphy, R.; Kirby, B.; Burden, A.D.; et al. Practical experience of ustekinumab in the treatment of psoriasis: Experience from a multicentre, retrospective case cohort study across the U.K. and Ireland. Br. J. Dermatol. 2012, 166, 189–195. [Google Scholar] [CrossRef]
- Fernández-Torres, R.M.; Paradela, S.; Fonseca, E. Long-term response to etanercept monotherapy in moderate to severe psoriasis: Assessment in daily practice by the maintenance of low values of PASI and BSA. J. Dermatol. Treat. 2014, 25, 54–56. [Google Scholar] [CrossRef]
- Janssen Biotech Inc. Janssen Announces US FDA Approval of TREMFYA (T) (Guselkumab) for the Treatment of Moderate to Severe Plaque Psoriasis; Janssen Biotech Inc.: Horsham, PA, USA, 2017. [Google Scholar]
- Tremfya. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/tremfya (accessed on 30 June 2020).
- Reich, K.; Armstrong, A.W.; Langley, R.G.; Flavin, S.; Randazzo, B.; Li, S.; Hsu, M.-C.; Branigan, P.; Blauvelt, A. Guselkumab versus secukinumab for the treatment of moderate-to-severe psoriasis (ECLIPSE): Results from a phase 3, randomised controlled trial. Lancet 2019, 394, 831–839. [Google Scholar] [CrossRef]
- Hyrich, K.L.; Symmons, D.P.M.; Silman, A.J. OMERACT 7 Special Interest Group Reconciling subject differences in recruitment to clinical trials and clinical practice. J. Rheumatol. 2005, 32, 2475–2476. [Google Scholar] [PubMed]
- Rodriguez Fernandez-Freire, L.; Galán-Gutierrez, M.; Armario-Hita, J.C.; Perez-Gil, A.; Ruiz-Villaverde, R. Guselkumab: Short-term effectiveness and safety in real clinical practice. Dermatol. Ther. 2020, e13344. [Google Scholar] [CrossRef] [PubMed]
- Fougerousse, A.-C.; Ghislain, P.-D.; Reguiai, Z.; Maccari, F.; Parier, J.; Bouilly Auvray, D.; Chaby, G.; Pallure, V.; Schmutz, J.-L.; Clément, C.; et al. Effectiveness and short-term (16-week) tolerance of guselkumab for psoriasis under real-life conditions: A retrospective multicenter study. J. Eur. Acad. Dermatol. Venereol. 2020. [Google Scholar] [CrossRef]
- Zweegers, J.; Roosenboom, B.; van de Kerkhof, P.C.M.; van den Reek, J.M.P.A.; Otero, M.E.; Atalay, S.; Kuijpers, A.L.A.; Koetsier, M.I.A.; Arnold, W.P.; Berends, M.A.; et al. Frequency and predictors of a high clinical response in patients with psoriasis on biological therapy in daily practice: Results from the prospective, multicenter BioCAPTURE cohort. Br. J. Dermatol. 2017, 176, 786–793. [Google Scholar] [CrossRef]
- Papp, K.; Crowley, J.; Rubel, D.; Landells, I.; Song, M.; Wasfi, Y.; You, Y.; Shen, Y.K.; Thaci, D. Consistency of response by weight across subgroups of patients with psoriasis treated with guselkumab: Results from the VOYAGE 1 and 2 trials. J. Am. Acad. Dermatol. 2018, 79. [Google Scholar] [CrossRef]
- Naldi, L.; Addis, A.; Chimenti, S.; Giannetti, A.; Picardo, M.; Tomino, C.; Maccarone, M.; Chatenoud, L.; Bertuccio, P.; Caggese, E.; et al. Impact of body mass index and obesity on clinical response to systemic treatment for psoriasis. Evidence from the Psocare project. Dermatology 2008, 217, 365–373. [Google Scholar] [CrossRef]
- Mourad, A.; Straube, S.; Armijo-Olivo, S.; Gniadecki, R. Factors predicting persistence of biologic drugs in psoriasis: A systematic review and meta-analysis. Br. J. Dermatol. 2019, 181, 450–458. [Google Scholar] [CrossRef]
- Romaní, J.; Caixàs, A.; Carrascosa, J.M.; Ribera, M.; Rigla, M.; Luelmo, J. Effect of narrowband ultraviolet B therapy on inflammatory markers and body fat composition in moderate to severe psoriasis. Br. J. Dermatol. 2012, 166, 1237–1244. [Google Scholar] [CrossRef]
- Carrascosa, J.M.; Vilavella, M.; Garcia-Doval, I.; Carretero, G.; Vanaclocha, F.; Daudén, E.; Gómez-García, F.J.; Herrera-Ceballos, E.; De la Cueva Dobao, P.; Belinchón, I.; et al. Body mass index in patients with moderate-to-severe psoriasis in Spain and its impact as an independent risk factor for therapy withdrawal: Results of the Biobadaderm Registry. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Naldi, L.; Chatenoud, L.; Linder, D.; Belloni Fortina, A.; Peserico, A.; Virgili, A.R.; Bruni, P.L.; Ingordo, V.; Lo Scocco, G.; Solaroli, C.; et al. Cigarette smoking, body mass index, and stressful life events as risk factors for psoriasis: Results from an Italian case-control study. J. Investig. Dermatol. 2005, 125, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Lønnberg, A.S.; Skov, L.; Skytthe, A.; Kyvik, K.O.; Pedersen, O.B.; Thomsen, S.F. Association of Psoriasis With the Risk for Type 2 Diabetes Mellitus and Obesity. JAMA Dermatol. 2016, 152, 761–767. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristic | N = 52 |
|---|---|
| General | |
| Male gender, n (%) | 30 (57.7) |
| Age (years) | 51.3 ± 14.1 |
| BMI (Kg/M2) | 29.9 ± 6.3 |
| Current cigarette smoker, n (%) | 25 (48) |
| Disease characteristics | |
| Age at disease onset | 29.1 ± 15.9 |
| Disease duration | 22.1 ± 16.2 |
| PASI at baseline | 20.0 ± 13.3 |
| Biologic therapy, n (%) | |
| Biologic naïve | 22 (42.3) |
| 1 biologic | 9 (17.3) |
| 2 biologics | 10 (19.2) |
| ≥3 biologics | 11 (21.1) |
| Comorbidities, n (%) | |
| Hypertension | 22 (42.3) |
| Obesity | 21 (40.4) |
| Dyslipidemia | 8 (15.4) |
| Psychiatric illness | 3 (5.8) |
| Diabetes mellitus | 3 (5.8) |
| Other pathologies/disorders | 6 (11.5) |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| 20 weeks | ||
| Number of PBT | 2.86 (1.41–5.88) | 0.004 |
| Number of comorbidities | 2.56 (1.14–5.88) | 0.023 |
| PBT + comorbidities | 1.96 (1.27–3.03) | 0.003 |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| 12 weeks | ||
| Number of PBT | 1.96 (1.14–3.45) | 0.017 |
| Number of comorbidities | 2.00 (1.03–3.85) | 0.041 |
| PBT + comorbidities | 1.69 (1.11–2.56) | 0.015 |
| 20 weeks | ||
| Number of PBT | 2.00 (1.19–3.33) | 0.008 |
| Number of comorbidities | 2.94 (1.32–6.25) | 0.008 |
| PBT + comorbidities | 1.85 (1.22–2.78) | 0.004 |
| 28 weeks | ||
| Number of PBT | 2.17 (1.22–3.85) | 0.008 |
| Number of comorbidities | 2.44 (1.14–5.26) | 0.023 |
| PBT + comorbidities | 1.75 (1.18–2.56) | 0.005 |
| 36 weeks | ||
| Number of PBT | 2.17 (1.12–4.17) | 0.021 |
| Number of comorbidities | 5.26 (1.37–20.00) | 0.015 |
| PBT + comorbidities | 1.96 (1.20–3.23) | 0.007 |
| 44 weeks | ||
| Number of PBT | 2.04 (1.18–4.17) | 0.014 |
| Number of comorbidities | 4.76 (1.33–16.67) | 0.016 |
| PBT + comorbidities | 1.89 (1.16–3.03) | 0.010 |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| 20 weeks | ||
| Number of PBT | 2.86 (1.47–5.88) | 0.002 |
| Number of comorbidities | 2.78 (1.30–5.88) | 0.008 |
| PBT + comorbidities | 2.63 (1.39–5.00) | 0.003 |
| 28 weeks | ||
| Number of PBT | 2.22 (1.27–4.00) | 0.006 |
| Number of comorbidities | 2.38 (1.15–5.00) | 0.019 |
| PBT + comorbidities | 1.89 (1.20–2.94) | 0.006 |
| 36 weeks | ||
| Number of PBT | 2.04 (1.16–3.70) | 0.013 |
| Number of comorbidities | 2.78 (1.23–6.25) | 0.014 |
| PBT + comorbidities | 1.82 (1.18–2.78) | 0.007 |
| 44 weeks | ||
| Number of PBT | 2.22 (1.18–4.17) | 0.014 |
| Number of comorbidities | 3.33 (1.30–9.09) | 0.012 |
| PBT + comorbidities | 1.89 (1.19–2.94) | 0.007 |
| 52 weeks | ||
| Number of PBT | 2.63 (1.08–6.25) | 0.034 |
| Number of comorbidities | 6.67 (1.25–33.33) | 0.026 |
| PBT + comorbidities | 2.13 (1.10–4.17) | 0.025 |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| PASI 75 | ||
| 20 weeks | ||
| Number of PBT (low to high) | 2.85 (1.41–5.88) | 0.004 |
| PASI 90 | ||
| 12 weeks | ||
| Number of PBT (low to high) | 1.96 (1.14–3.45) | 0.017 |
| 20 weeks | ||
| Number of comorbidities (low to high) | 2.94 (1.32–6.25) | 0.008 |
| 28 weeks | ||
| Number of PBT (low to high) | 2.17 (1.22–3.85) | 0.008 |
| 36 weeks | ||
| Number of comorbidities (low to high) | 5.26 (1.37–20.00) | 0.015 |
| 44 weeks | ||
| Number of comorbidities (low to high) | 4.76 (1.33–16.67) | 0.016 |
| PASI 100 | ||
| 20 weeks | ||
| Number of PBT (low to high) | 2.86 (1.47–5.88) | 0.002 |
| 28 weeks | ||
| Number of PBT (low to high) | 2.22 (1.27–4.00) | 0.006 |
| 36 weeks | ||
| Number of PBT (low to high) | 2.04 (1.16–3.70) | 0.013 |
| 44 weeks | ||
| Number of comorbidities (low to high) | 3.33 (1.30–9.09) | 0.012 |
| 52 weeks | ||
| Number of comorbidities (low to high) | 6.67 (1.25–33.33) | 0.026 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galluzzo, M.; Tofani, L.; Lombardo, P.; Petruzzellis, A.; Silvaggio, D.; Egan, C.G.; Bianchi, L.; Talamonti, M. Use of Guselkumab for the Treatment of Moderate-to-Severe Plaque Psoriasis: A 1 Year Real-Life Study. J. Clin. Med. 2020, 9, 2170. https://doi.org/10.3390/jcm9072170
Galluzzo M, Tofani L, Lombardo P, Petruzzellis A, Silvaggio D, Egan CG, Bianchi L, Talamonti M. Use of Guselkumab for the Treatment of Moderate-to-Severe Plaque Psoriasis: A 1 Year Real-Life Study. Journal of Clinical Medicine. 2020; 9(7):2170. https://doi.org/10.3390/jcm9072170
Chicago/Turabian StyleGalluzzo, Marco, Lorenzo Tofani, Paolo Lombardo, Alessandra Petruzzellis, Dionisio Silvaggio, Colin Gerard Egan, Luca Bianchi, and Marina Talamonti. 2020. "Use of Guselkumab for the Treatment of Moderate-to-Severe Plaque Psoriasis: A 1 Year Real-Life Study" Journal of Clinical Medicine 9, no. 7: 2170. https://doi.org/10.3390/jcm9072170
APA StyleGalluzzo, M., Tofani, L., Lombardo, P., Petruzzellis, A., Silvaggio, D., Egan, C. G., Bianchi, L., & Talamonti, M. (2020). Use of Guselkumab for the Treatment of Moderate-to-Severe Plaque Psoriasis: A 1 Year Real-Life Study. Journal of Clinical Medicine, 9(7), 2170. https://doi.org/10.3390/jcm9072170