Pain Neuroscience Education Plus Usual Care Is More Effective than Usual Care Alone to Improve Self-Efficacy Beliefs in People with Chronic Musculoskeletal Pain: A Non-Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
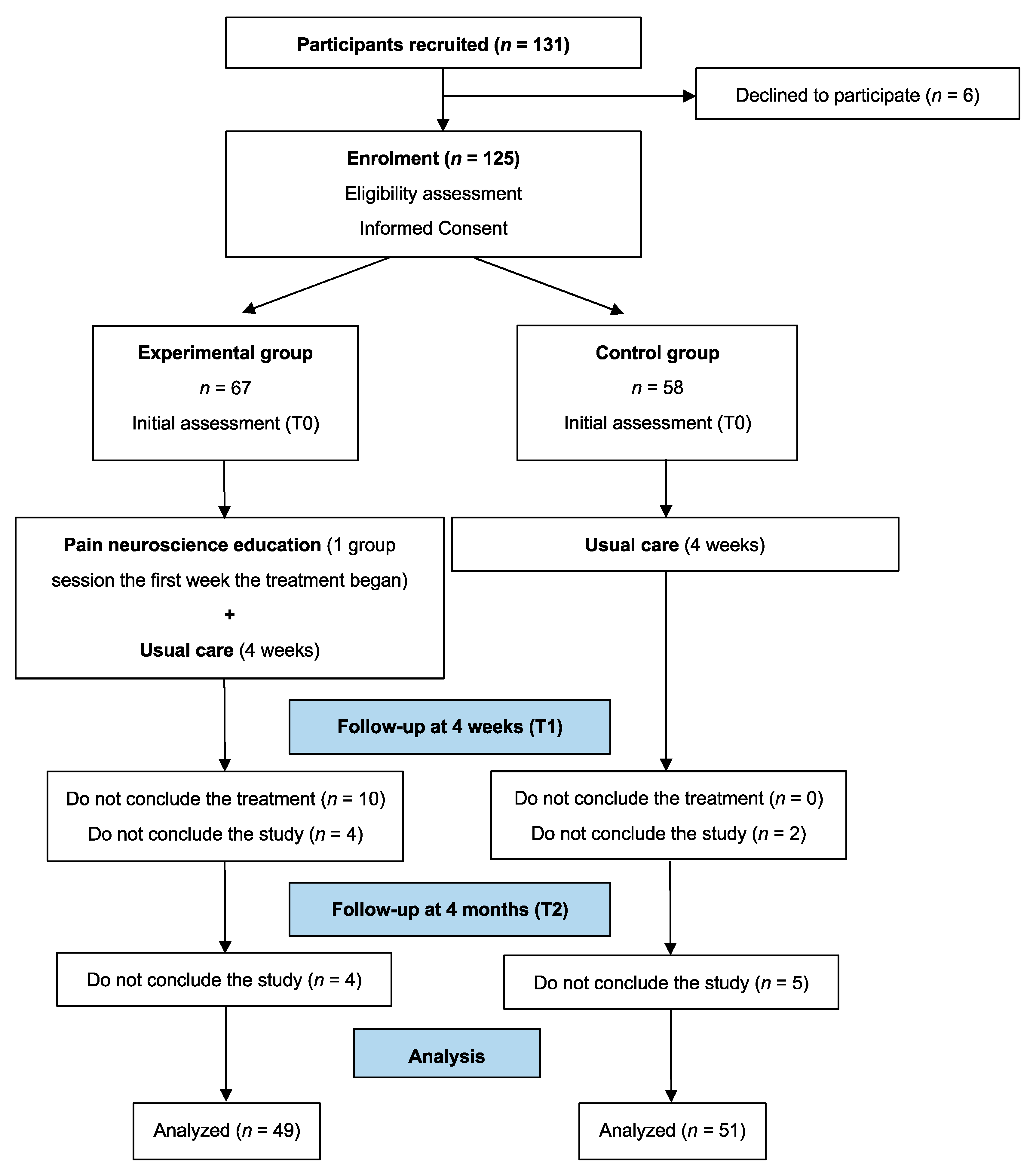
2.2. Participants and Setting
2.3. Allocation
2.4. Description of the Interventions
2.4.1. Pain Neuroscience Education
2.4.2. Usual Care Intervention (Physiotherapy)
2.5. Outcome Measures
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes
2.6. Sample Size Calculation
2.7. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Sample
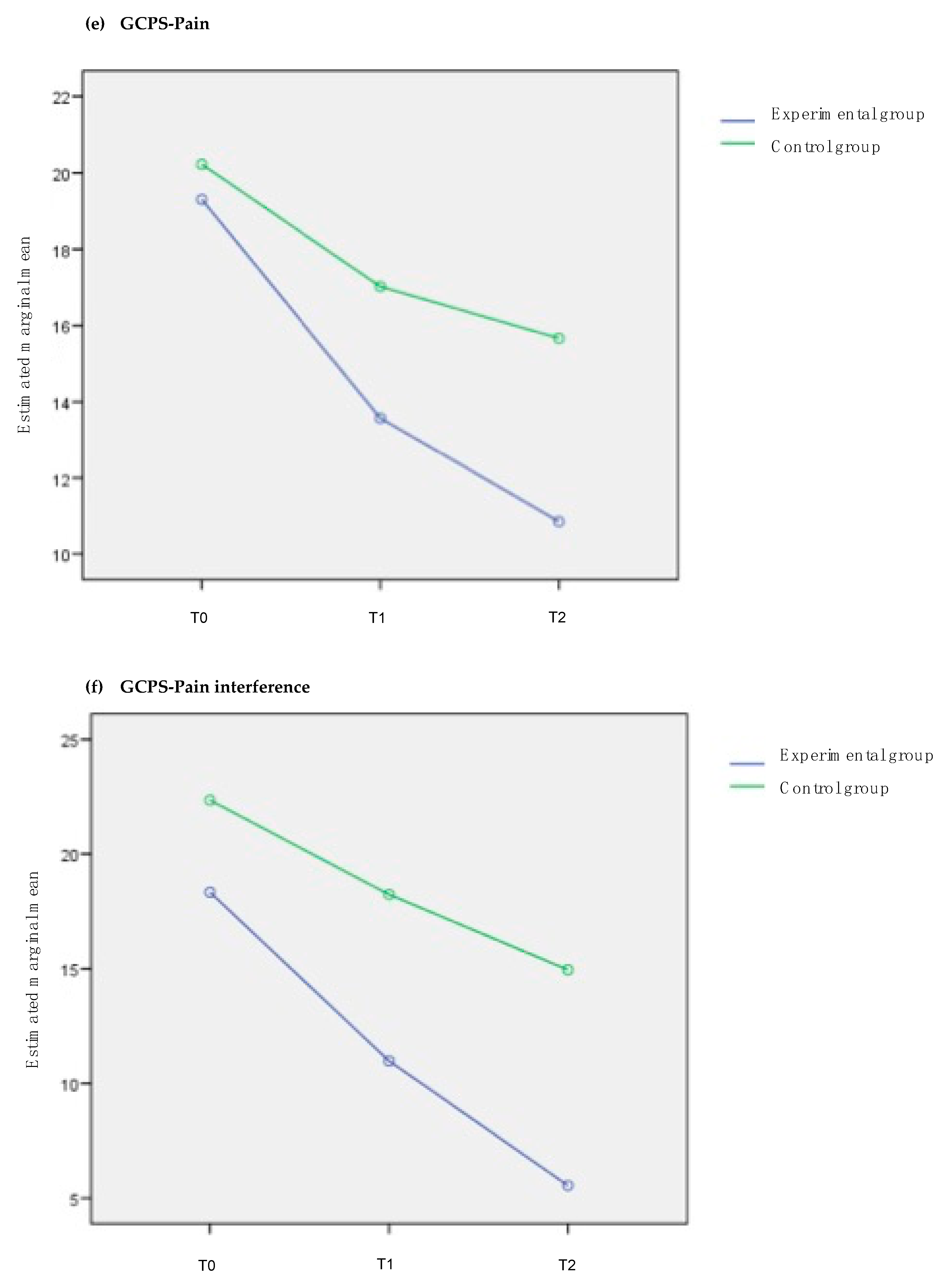
3.2. PNE Plus Usual Care (Experimental Group) Versus Usual Care Alone (Control Group)
3.3. PNE Plus Usual Care (Experimental Group) Versus Usual Care Alone (Control Group), Adjusted for Pain Duration
3.4. Secondary Analysis: Did Knowledge about Pain Neurophysiology Acquired after Intervention (Experimental Group) Influence the Effects Observed in the Different Outcomes?
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B




References
- Kovačević, I.; Kogler, V.M.; Turković, T.M.; Dunkić, L.F.; Ivanec, Ž.; Petek, D. Self-Care of Chronic Musculoskeletal Pain—Experiences and Attitudes of Patients and Health Care Providers. BMC Musculoskelet. Disord. 2018, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Nicholas, M.K. The Pain Self-Efficacy Questionnaire: Taking Pain into Account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef]
- Mishali, M.; Omer, H.; Heymann, A.D. The Importance of Measuring Self-Efficacy in Patients with Diabetes. Fam. Pract. 2011, 28, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Jackson, T.; Wang, Y.; Wang, Y.; Fan, H. Self-Efficacy and Chronic Pain Outcomes: A Meta-Analytic Review. J. Pain 2014, 15, 800–814. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Calderon, J.; Zamora-Campos, C.; Navarro-Ledesma, S.; Luque-Suarez, A. The Role of Self-Efficacy on the Prognosis of Chronic Musculoskeletal Pain: A Systematic Review. J. Pain 2018, 19, 10–34. [Google Scholar] [CrossRef] [PubMed]
- Peñacoba Puente, C.; Velasco Furlong, L.; Écija Gallardo, C.; Cigarán Méndez, M.; Bedmar Cruz, D.; Fernández-de-las-Peñas, C. Self-Efficacy and Affect as Mediators Between Pain Dimensions and Emotional Symptoms and Functional Limitation in Women With Fibromyalgia. Pain Manag. Nurs. 2015, 16, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.; Da, C.M.; Maher, C.G.; McAuley, J.H.; Hancock, M.J.; Smeets, R.J.E.M. Self-Efficacy Is More Important than Fear of Movement in Mediating the Relationship between Pain and Disability in Chronic Low Back Pain. Eur. J. Pain 2011, 15, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Ahlstrand, I.; Vaz, S.; Falkmer, T.; Thyberg, I.; Björk, M. Self-Efficacy and Pain Acceptance as Mediators of the Relationship between Pain and Performance of Valued Life Activities in Women and Men with Rheumatoid Arthritis. Clin. Rehabil. 2017, 31, 824–834. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.A.; Holtzman, S.; Mancl, L. Mediators, Moderators, and Predictors of Therapeutic Change in Cognitive-Behavioral Therapy for Chronic Pain. Pain 2007, 127, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Booth, J.; Moseley, G.L.; Schiltenwolf, M.; Cashin, A.; Davies, M.; Hübscher, M. Exercise for Chronic Musculoskeletal Pain: A Biopsychosocial Approach. Musculoskelet. Care 2017, 15, 413–421. [Google Scholar] [CrossRef]
- Picha, K.J.; Howell, D.M. A Model to Increase Rehabilitation Adherence to Home Exercise Programmes in Patients with Varying Levels of Self-Efficacy. Musculoskelet. Care 2018, 16, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Asghari, A.; Nicholas, M.K. Pain Self-Efficacy Beliefs and Pain Behaviour. A Prospective Study. Pain 2001, 94, 85–100. [Google Scholar] [CrossRef]
- Bandura, A. Sel-Efficacy: Toward a Unifying Theory of Behavioral Change. Advances in Behaviour Research and Therapy. Public Health 1978, 1, 139–161. [Google Scholar]
- Martinez-Calderon, J.; Flores-Cortes, M.; Morales-Asencio, J.M.; Fernandez-Sanchez, M.; Luque-Suarez, A. Which Interventions Enhance Pain Self-Efficacy in People with Chronic Musculoskeletal Pain? A Systematic Review and Meta Analysis of Randomized Controlled Trials Including over 12,000 Participants. J. Orthop. Sport. Phys. Ther. in press.
- Joypaul, S.; Kelly, F.; McMillan, S.S.; King, M.A. Multi-Disciplinary Interventions for Chronic Pain Involving Education: A Systematic Review. PLoS ONE 2019, 14, 1–24. [Google Scholar] [CrossRef]
- Louw, A.; Zimney, K.; Puentedura, E.J. Retention of Pain Neuroscience Knowledge: A Multi-Centre Trial. N. Z. J. Physiother. 2016, 44, 91–96. [Google Scholar] [CrossRef]
- Louw, A.; Vogsland, R.; Marth, L.; Marshall, P.; Cox, T.; Landers, M. Interdisciplinary Pain Neuroscience Continuing Education in the Veteran’s Affairs: Live Training and Live-Stream with 1-Year Follow-Up. Clin. J. Pain 2019, 35, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Colleary, G.; O’Sullivan, K.; Griffin, D.; Ryan, C.G.; Martin, D.J. Effect of Pain Neurophysiology Education on Physiotherapy Students’ Understanding of Chronic Pain, Clinical Recommendations and Attitudes towards People with Chronic Pain: A Randomised Controlled Trial. Physiotherapy 2017, 103, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Watson, J.A.; Cooper, L.; Whittle, R.; Lavender, M.; Atkinson, G.; Martin, D.J. Pain Neuroscience Education for Adults with Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. J. Pain 2019, 20, 1140.e22. [Google Scholar] [CrossRef]
- Reeves, B.; Gaus, W. Guidelines for Reporting Non-Randomised Studies. Complementary Med. Res. 2004, 11, 46–52. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dworkin, R.H.; Bruehl, S.; Fillingim, R.B.; Loeser, J.D.; Terman, G.W.; Turk, D.C. Multidimensional Diagnostic Criteria for Chronic Pain: Introduction to the ACTTION–American Pain Society Pain Taxonomy (AAPT). J. Pain 2016, 17, T1–T9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domenech, J.; Segura-Ortí, E.; Lisón, J.F.; Espejo-Tort, B.; Sánchez-Zuriaga, D. Psychometric Properties and Factor Structure of the Spanish Version of the HC-PAIRS Questionnaire. Eur. Spine J. 2013, 22, 985–994. [Google Scholar] [CrossRef] [Green Version]
- Moseley, G.L.; Butler, D.S. Explain Pain, 2nd ed.; Noigroup Publications: Adelaide, Australia, 2013; p. 133. [Google Scholar]
- Moseley, G.L.; Butler, D.S. The Explain Pain Handbook: Protectometer; Noigroup Publications: Adelaide, Australia, 2015; p. 48. [Google Scholar]
- Courtney, C.A.; Steffen, A.D.; Fernández-de-las-Pñas, C.; Kim, J.; Chmell, S.J. Joint Mobilization Enhances Mechanisms of Conditioned Pain Modulation in Individuals With Osteoarthritis of the Knee. J. Orthop. Sports Phys. Ther. 2016, 46, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijs, J.; Torres-Cueco, R.; van Wilgen, C.P.; Girbés, E.L.; Struyf, F.; Roussel, N.; Van Oosterwijck, J.; Daenen, L.; Kuppens, K.; Vanderweeën, L.; et al. Applying Modern Pain Neuroscience in Clinical Practice: Criteria for the Classification of Central Sensitization Pain. Pain Phys. 2014, 17, 447–457. [Google Scholar]
- Koltyn, K.F.; Brellenthin, A.G.; Cook, D.B.; Sehgal, N.; Hillard, C. Mechanisms of Exercise-Induced Hypoalgesia. J. Pain 2014, 15, 1294–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijs, J.; Apeldoorn, A.; Hallegraeff, H.; Clark, J.; Smeets, R.; Malfliet, A.; Girbes, E.L.; De Kooning, M.; Ickmans, K. Low Back Pain: Guidelines for the Clinical Classification of Predominant Neuropathic, Nociceptive, or Central Sensitization Pain. Pain Phys. 2015, 18, E333–E346. [Google Scholar]
- Meeus, M.; Nijs, J.; Van Wilgen, P.; Noten, S.; Goubert, D.; Huijnen, I. Moving on to Movement in Patients with Chronic Joint Pain. Pain 2016, 1, 23–35. [Google Scholar]
- Martín-Aragón, M.; Pastor, M.A.; Rodríguez-Marín, J.; March, M.J.; Lledó, A.; López-Roig, S.; Terol, M.C. Percepción de Autoeficacia En Dolor Crónico. Adaptación y Validación de La Chronic Pain Self-Efficacy Scale. Rev. Psicol. Salud 1999, 11, 53–75. [Google Scholar]
- Ferrer-Peña, R.; Gil-Martínez, A.; Pardo-Montero, J.; Jiménez-Penick, V.; Gallego-Iquierdo, T.; La Touche, R. Adaptation and Validation of the Graded Chronic Pain Scale Into Spanish. Reumatol. Clınica 2016, 12, 130–138. [Google Scholar] [CrossRef]
- Catley, M.J.; O’Connell, N.E.; Moseley, G.L. How Good Is the Neurophysiology of Pain Questionnaire? A Rasch Analysis of Psychometric Properties. J. Pain 2013, 14, 818–827. [Google Scholar] [CrossRef]
- Wild, D.; Grove, A.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Librero, J.; Peiró, S.; Ordiñana, R. Chronic Comorbidity and Outcomes of Hospital Care: Length of Stay, Mortality, and Readmission at 30 and 365 Days. J. Clin. Epidemiol. 1999, 52, 171–179. [Google Scholar] [CrossRef]
- Louw, A.; Puentedura, E.J.; Reed, J.; Zimney, K.; Grimm, D.; Landers, M.R. A Controlled Clinical Trial of Preoperative Pain Neuroscience Education for Patients about to Undergo Total Knee Arthroplasty. Clin. Rehabil. 2019, 33, 1722–1731. [Google Scholar] [CrossRef] [PubMed]
- Valiente-Castrillo, P.; Martin-Pintado, A.; Calvo-Lobo, C.; Beltran-Alacreu, H.; Fernández-Carnero, J. Effects of Pain Neuroscience Education and Dry Needling for the Management of Patients with Chronic Myofascial Neck Pain: A Randomized Clinical Trial. Acupunct. Med. 2020. [Google Scholar] [CrossRef]
- Horler, C.; Hebron, C.; Martyn, K. Personalizing Education: The Clinical Reasoning Processes of Physiotherapists Using Education for the Treatment of People with Chronic Low Back Pain. Physiother. Theory Pract. 2020, 1–10. [Google Scholar] [CrossRef]
- Reeves, B.C. Principles of Research: Limitations of Non-Randomized Studies. Surgery 2008, 26, 120–124. [Google Scholar] [CrossRef]
- Rajati, F.; Sadeghi, M.; Feizi, A.; Sharifirad, G.; Hasandokht, T.; Mostafavi, F. Self-Efficacy Strategies to Improve Exercise in Patients with Heart Failure: A Systematic Review. ARYA Atheroscler. 2014, 10, 319–333. [Google Scholar]
- Moseley, G.L.; Butler, D.S. Explain Pain Supercharged, 1st ed.; Noigroup Publications: Adelaide, Australia, 2017; p. 244. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Experimental (n = 49) | Control (n = 51) | |
|---|---|---|---|
| Gender (%) | Male | 12.2% | 19.6% |
| Female | 87.8% | 80.4% | |
| Age, years (mean ± SD) | 47.2 (±8.5) | 48.6 (±9.5) | |
| Body mass index (mean ± SD) | 26.1(±4.4) | 25.8 (±4.8) | |
| Educational level (%) | University | 12.2 | 5.9 |
| High school | 22.4 | 11.8 | |
| Secondary | 32.7 | 39.2 | |
| Elementary | 32.7 | 43.1 | |
| No formal studies | 0.0 | 0.0 | |
| Employment situation (%) | Unemployed | 24.5 | 17.6 |
| Sick leave | 0.0 | 5.9 | |
| Pensioner | 4.1 | 3.9 | |
| Housework | 10.2 | 11.8 | |
| Working | 61.2 | 60.8 | |
| Pain duration (%) * | >3 months | 2.0 | 7.8 |
| >6 months | 6.1 | 19.6 | |
| >12 months | 91.8 | 72.5 | |
| Charlson comorbidity index (%) | No comorbidity | 87.8 | 94.1 |
| Low comorbidity | 8.2 | 3.9 | |
| High comorbidity | 4.1 | 2.0 | |
| ACTTION–AAPT (%) | Osteoarthritis | 0.0 | 0.0 |
| Other arthritis (e.g., rheumatoid arthritis, gout, connective tissue diseases) | 0.0 | 0.0 | |
| MSK lower back pain | 32.7 | 25.5 | |
| Myofascial pain, chronic widespread pain and fibromyalgia | 0.0 | 0.0 | |
| Other predominantly MSK pain | 67.3 | 74.5 | |
| Other MSK pain conditions (%) | Shoulder | 40.8 | 37.3 |
| Lumbar spine | 32.7 | 25.5 | |
| Neck | 22.4 | 13.7 | |
| Knee | 4.1 | 9.8 | |
| Hip | 0.0 | 13.7 | |
| CPSS (mean ± SD) | Symptoms | 53.3 (±14.7) | 48.5 (±16.9) |
| Physical | 46.9 (±11.0) | 44.6 (±14.9) | |
| Pain | 31.5 (±12.0) | 28.1 (±13.1) | |
| GCPS (mean ± SD) | Pain | 19.4 (±5.2) | 20.8 (±5.0) |
| Pain interference | 18.7 (±10.2) | 21.9 (±11.1) | |
| Analgesic consumption (mean ± SD) | 0.7 (±1.2) | 0.7 (±1.1) | |
| Therapeutic group of analgesic medication (%) | None | 67.3 | 58.8 |
| Non-opioids | 16.3 | 35.3 | |
| Minor opioids | 16.3 | 3.9 | |
| Major opioids | 0.0 | 2.0 | |
| Four-Week Follow-up | Experimental (n = 49) Mean (SD) | Control (n = 51) Mean (SD) | Group Difference, Mean (95% CI) | p-Value | d-Cohen |
|---|---|---|---|---|---|
| CPSS | |||||
| Symptoms | 61.5 (16.5) | 49.9 (18.2) | 11.5 (4.6; 18.5) | 0.001 * | 0.67 |
| Physical | 53.8 (9.0) | 44.4 (16.0) | 9.3 (4.1; 14.5) | 0.001 * | 0.69 |
| Pain | 37.7 (10.0) | 29.7 (13.1) | 7.9 (3.3; 12.6) | 0.001 * | 0.69 |
| Total score | 153.0 (30.6) | 124.1 (44.1) | 28.9 (13.8; 44.1) | <0.001 * | 0.76 |
| GCPS | |||||
| Pain | 13.7 (5.0) | 16.8 (5.9) | −3.16 (−5.3; −0.9) | 0.005 * | 0.57 |
| Pain interference | 11.1 (8.9) | 18.1 (11.3) | −7.0 (−11.0; −2.9) | 0.001 * | 0.69 |
| Total score | 24.8 (13.0) | 35.0 (15.3) | −10.1 (−15.8; −4.5) | 0.001 * | 0.72 |
| Four-Month Follow-up | Experimental (n = 49) Mean (SD) | Control (n = 51) Mean (SD) | Group Difference, Mean (95% CI) | p-Value | d-Cohen |
|---|---|---|---|---|---|
| CPSS | |||||
| Symptoms | 65.4 (14.8) | 55.3 (17.9) | 10.1 (3.5; 16.6) | 0.003 * | 0.61 |
| Physical | 52.8 (10.7) | 45.8 (15.1) | 6.9 (1.7; 12.2) | 0.009 * | 0.99 |
| Pain | 40.3 (10.3) | 29.5 (13.8) | 10.7 (5.9; 15.6) | <0.001 * | 0.88 |
| Total score | 158.6 (33.1) | 130.8 (42.8) | 27.8 (12.6; 43.1) | <0.001 * | 0.73 |
| GCPS | |||||
| Pain | 11.1 (6.9) | 15.4 (7.1) | −4.3 (−7.1; −1.5) | 0.003 * | 0.61 |
| Pain interference | 6.0 (8.9) | 14.4 (12.2) | −8.4 (−12.7; −4.1) | <0.001 * | 0.79 |
| Total score | 17.1 (14.5) | 29.9 (18.5) | −12.7 (−19.4; −6.1) | <0.001 * | 0.77 |
| Experimental (n = 49) Estimated Marginal Mean | Control (n = 51) Estimated Marginal Mean | Group Difference, Mean (95% CI) | p-Value | |
|---|---|---|---|---|
| CPSS | ||||
| Symptoms | 60.8 (56.8; 64.8) | 50.5 (46.6; 54.4) | 10.3 (4.6; 15.9) | <0.001 * |
| Physical | 51.9 (48.5; 55.3) | 44.2 (40.9; 47.6) | 7.6 (2.7; 12.5) | 0.002 * |
| Pain | 37.1 (34.1; 40.2) | 28.5 (25.5; 31.5) | 8.6 (4.3; 12.9) | <0.001 * |
| Total score | 149.9 (140.4; 159.5) | 123.3 (113.9; 132.7) | 26.6 (13.0; 40.2) | <0.001 * |
| GCPS | ||||
| Pain | 14.5 (13.2; 15.9) | 17.6 (16.3; 18.9) | −3.0 (−4.9; −1.1) | 0.002 * |
| Pain interference | 11.6 (9.0; 14.2) | 18.5 (15.9; 21.0) | −6.8 (−10.5; −3.2) | <0.001 * |
| Total score | 26.2 (22.5; 29.8) | 36.1 (32.5; 39.7) | −9.9 (−15.1; −4.7) | <0.001 * |
| Experimental (n = 49) | Control (n = 51) | ||||||
|---|---|---|---|---|---|---|---|
| Increase % | No Change % | Decrease % | Increase % | No Change % | Decrease % | p-Value | |
| Four-Week Follow-Up | 0.0 | 77.6 | 22.4 | 2.0 | 88.2 | 9.8 | 0.089 * |
| Four-Month Follow-Up | 0.0 | 75.5 | 24.5 | 5.9 | 78.4 | 15.7 | 0.270 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rondon-Ramos, A.; Martinez-Calderon, J.; Diaz-Cerrillo, J.L.; Rivas-Ruiz, F.; Ariza-Hurtado, G.R.; Clavero-Cano, S.; Luque-Suarez, A. Pain Neuroscience Education Plus Usual Care Is More Effective than Usual Care Alone to Improve Self-Efficacy Beliefs in People with Chronic Musculoskeletal Pain: A Non-Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2195. https://doi.org/10.3390/jcm9072195
Rondon-Ramos A, Martinez-Calderon J, Diaz-Cerrillo JL, Rivas-Ruiz F, Ariza-Hurtado GR, Clavero-Cano S, Luque-Suarez A. Pain Neuroscience Education Plus Usual Care Is More Effective than Usual Care Alone to Improve Self-Efficacy Beliefs in People with Chronic Musculoskeletal Pain: A Non-Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(7):2195. https://doi.org/10.3390/jcm9072195
Chicago/Turabian StyleRondon-Ramos, Antonio, Javier Martinez-Calderon, Juan Luis Diaz-Cerrillo, Francisco Rivas-Ruiz, Gina Rocio Ariza-Hurtado, Susana Clavero-Cano, and Alejandro Luque-Suarez. 2020. "Pain Neuroscience Education Plus Usual Care Is More Effective than Usual Care Alone to Improve Self-Efficacy Beliefs in People with Chronic Musculoskeletal Pain: A Non-Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 7: 2195. https://doi.org/10.3390/jcm9072195
APA StyleRondon-Ramos, A., Martinez-Calderon, J., Diaz-Cerrillo, J. L., Rivas-Ruiz, F., Ariza-Hurtado, G. R., Clavero-Cano, S., & Luque-Suarez, A. (2020). Pain Neuroscience Education Plus Usual Care Is More Effective than Usual Care Alone to Improve Self-Efficacy Beliefs in People with Chronic Musculoskeletal Pain: A Non-Randomized Controlled Trial. Journal of Clinical Medicine, 9(7), 2195. https://doi.org/10.3390/jcm9072195