A Retrospective Comparison of DLI and gDLI for Post-Transplant Treatment

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Procedure
2.2. Statistical Analysis
3. Results
3.1. Patient and DLI Characteristics
3.2. Response
3.3. Safety
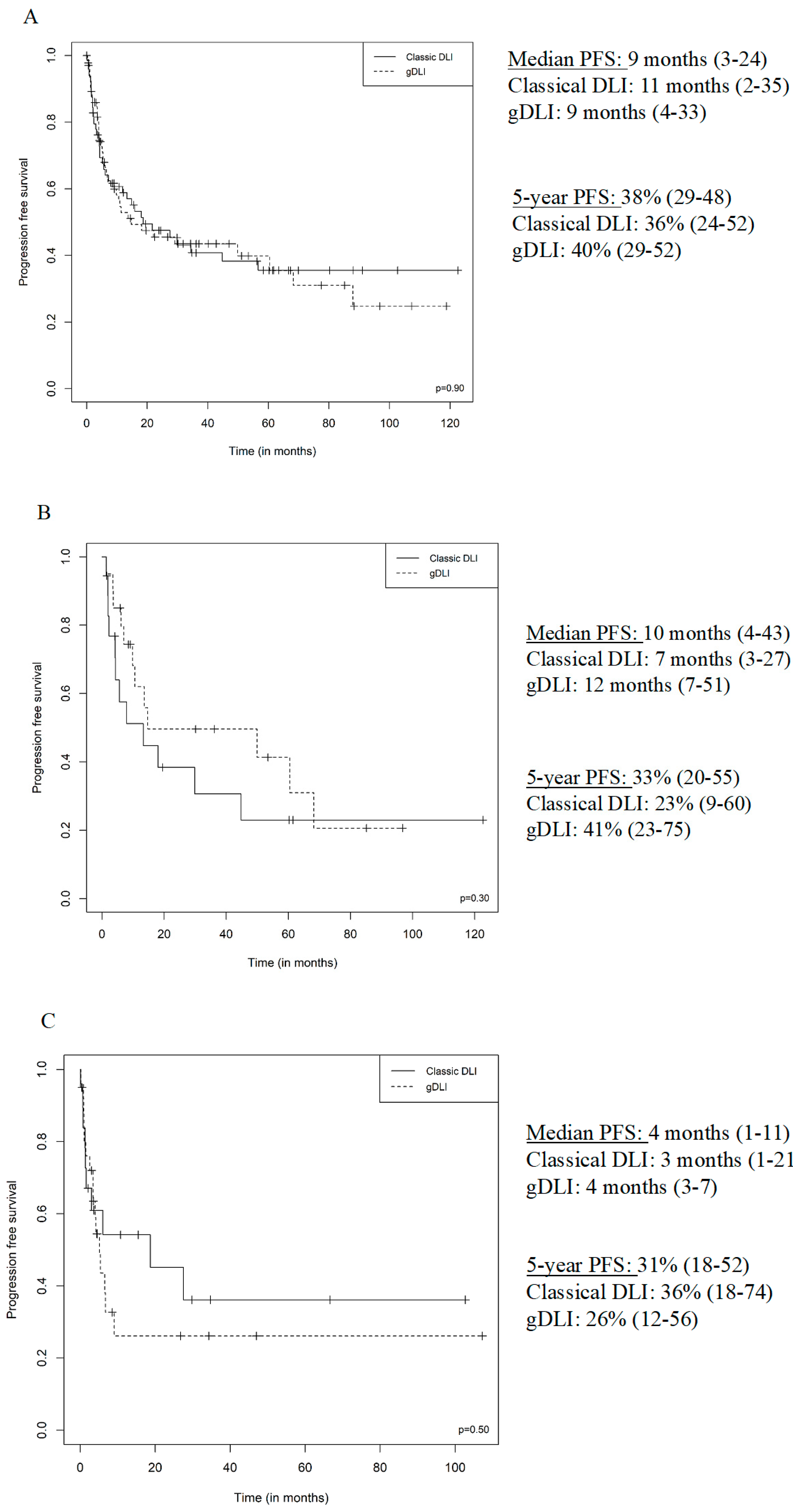
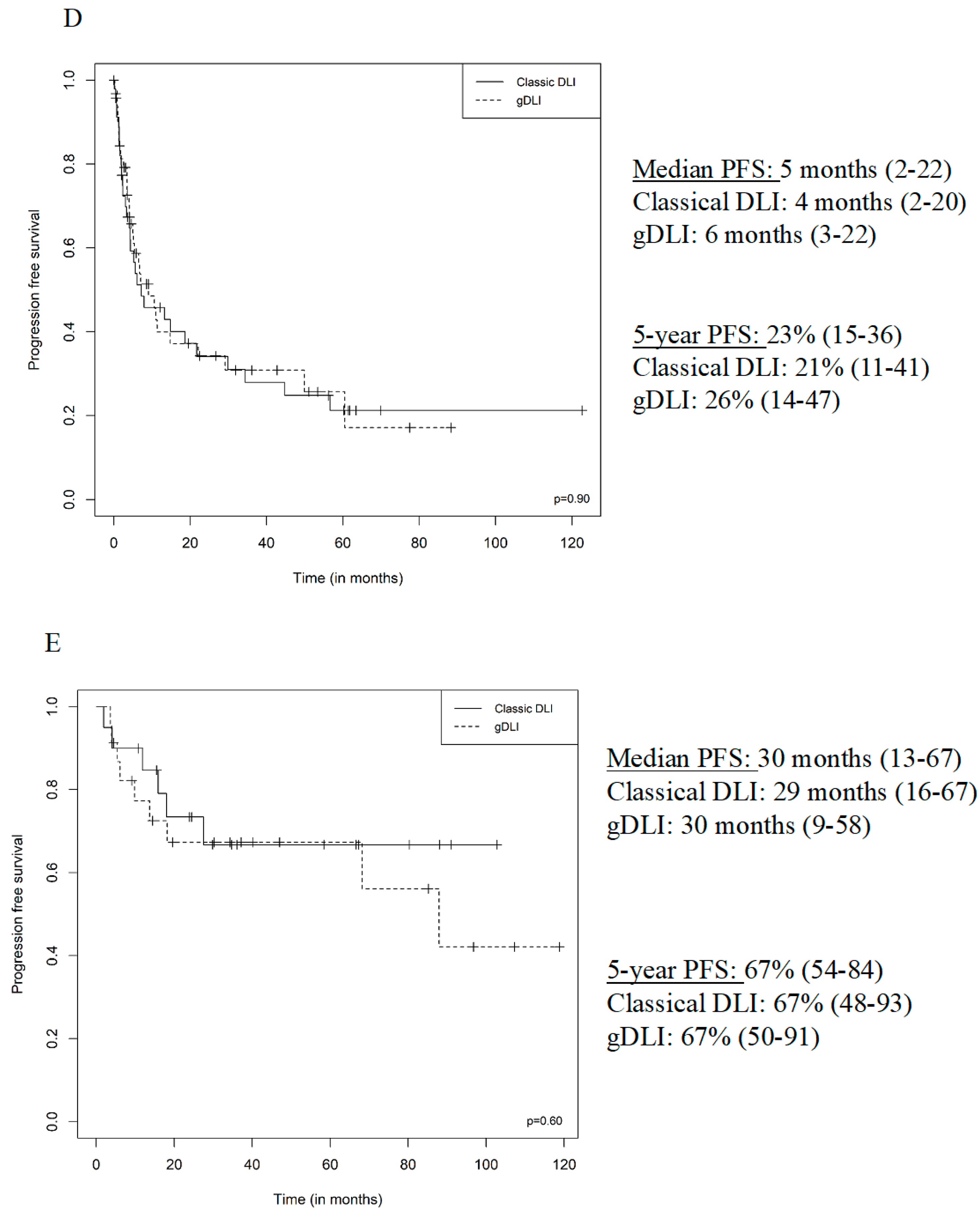
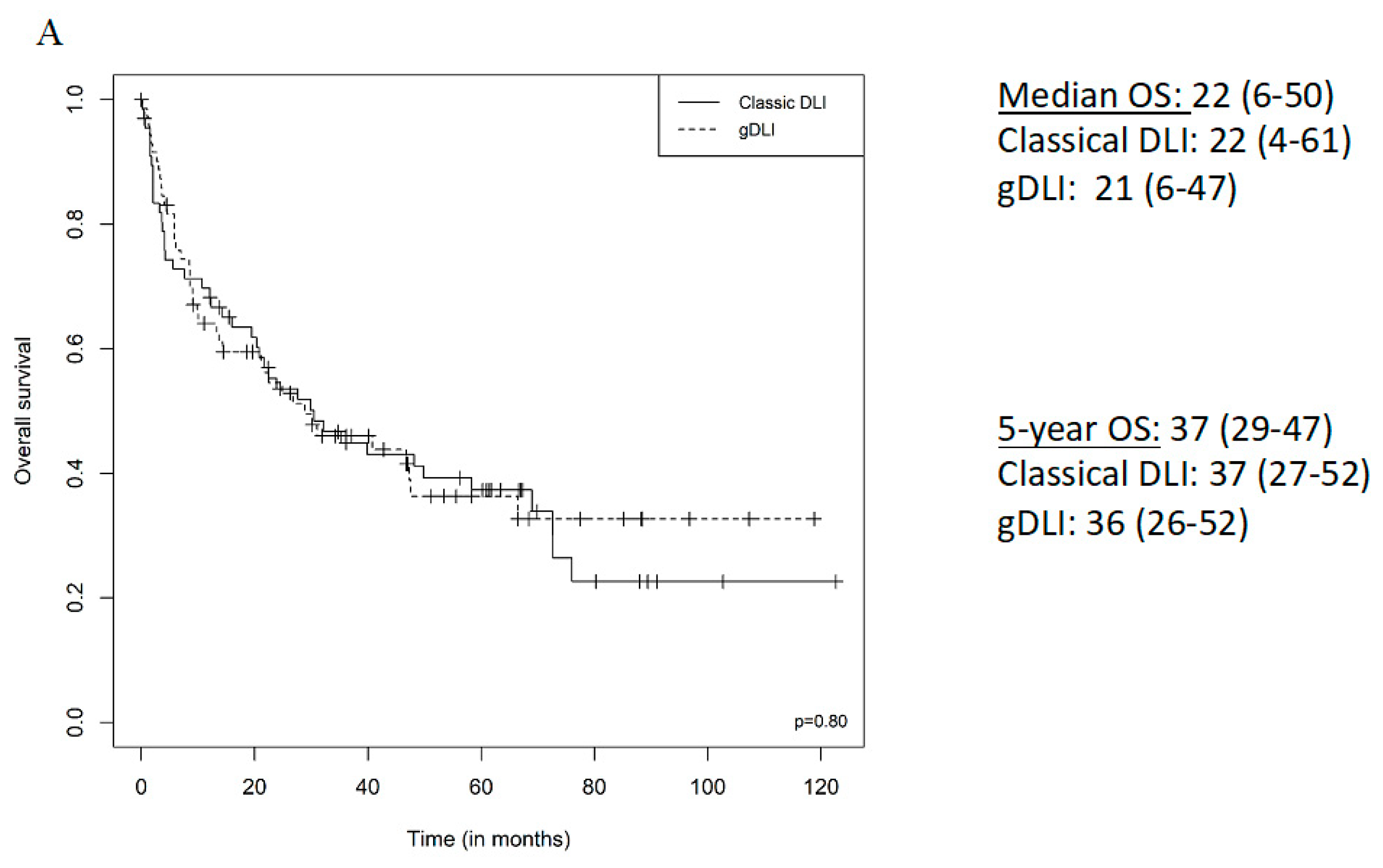
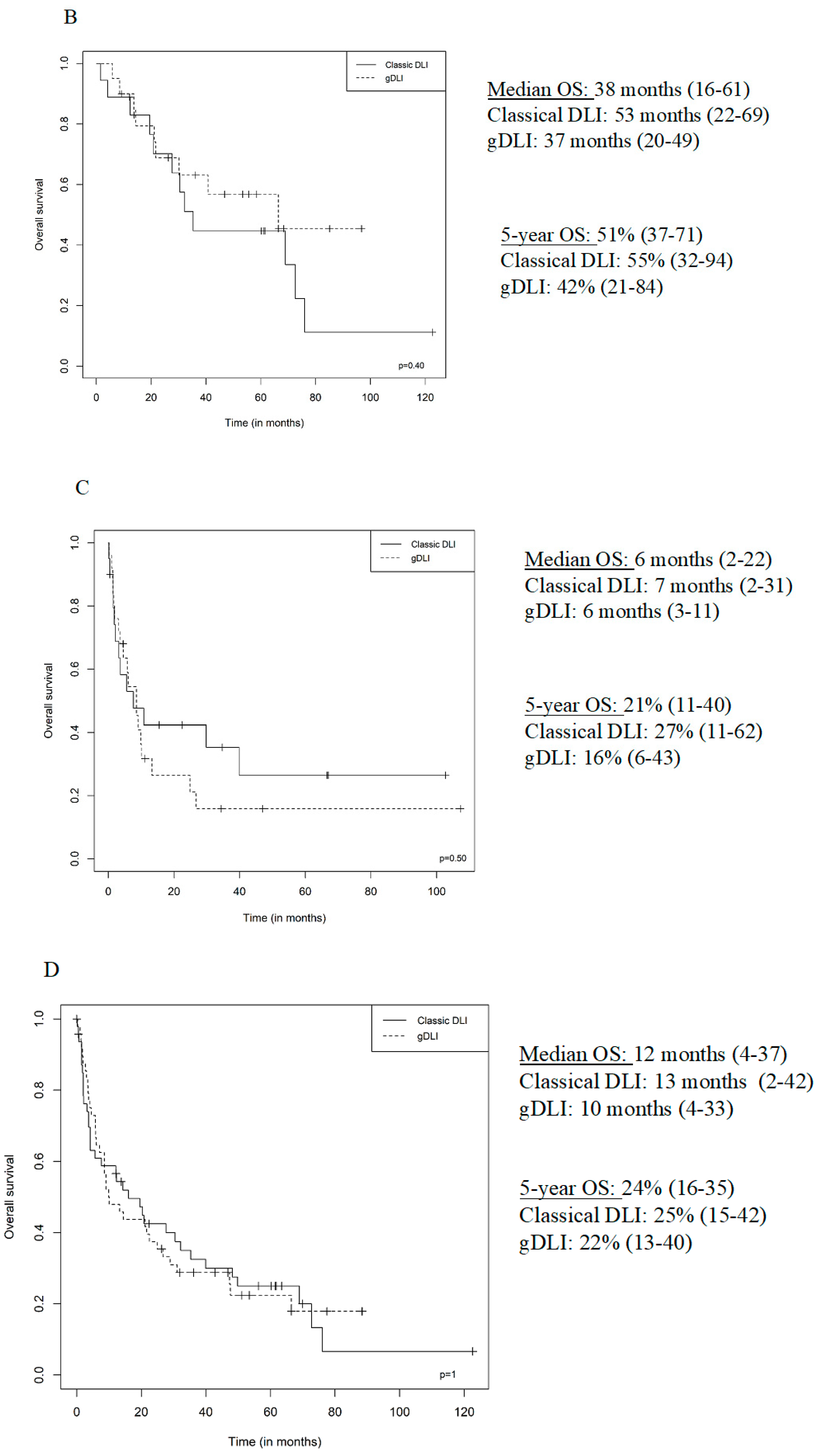
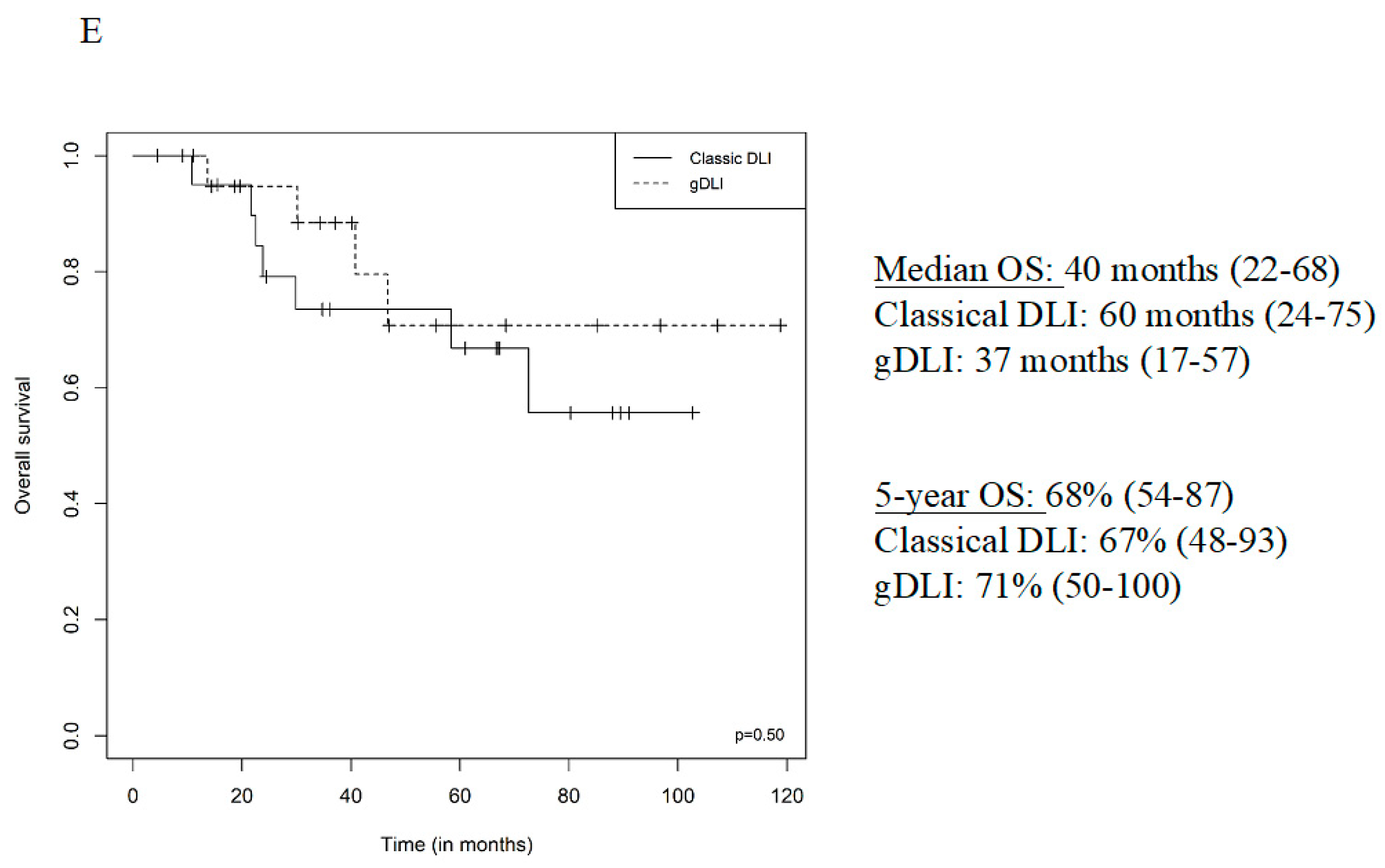
3.4. Survival
3.5. Sub-Group Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kolb, H.-J. Graft-versus-leukemia effects of transplantation and donor lymphocytes. Blood 2008, 112, 4371–4383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castagna, L.; Sarina, B.; Bramanti, S.; Perseghin, P.; Mariotti, J.; Morabito, L. Donor lymphocyte infusion after allogeneic stem cell transplantation. Transfus. Apher. Sci. 2016, 54, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, J.E.; Gill, S.; Negrin, R.S. Biology and clinical effects of natural killer cells in allogeneic transplantation. Curr. Opin. Oncol. 2010, 22, 130–137. [Google Scholar] [CrossRef]
- Solomon, S.R.; A Sizemore, C.; Zhang, X.; Brown, S.; Holland, H.K.; E Morris, L.; Bashey, A. Preemptive DLI without withdrawal of immunosuppression to promote complete donor T-cell chimerism results in favorable outcomes for high-risk older recipients of alemtuzumab-containing reduced-intensity unrelated donor allogeneic transplant: A prospective phase II trial. Bone Marrow Transplant. 2014, 49, 616–621. [Google Scholar]
- Scarisbrick, J.J.; Dignan, F.L.; Tulpule, S.; Gupta, E.D.; Kolade, S.; Shaw, B.; Evison, F.; Shah, G.; Tholouli, E.; Mufti, G.; et al. A multicentre UK study of GVHD following DLI: Rates of GVHD are high but mortality from GVHD is infrequent. Bone Marrow Transplant. 2015, 50, 62–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Cheikh, J.; Crocchiolo, R.; Fürst, S.; Ladaique, P.; Castagna, L.; Faucher, C.; Granata, A.; Oudin, C.; Lemarié, C.; Calmels, B.; et al. Lenalidomide plus donor-lymphocytes infusion after allogeneic stem-cell transplantation with reduced-intensity conditioning in patients with high-risk multiple myeloma. Exp. Hematol. 2012, 40, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, T.; Rachlis, E.; Bug, G.; Stelljes, M.; Klein, S.; Steckel, N.K.; Wolf, D.; Ringhoffer, M.; Czibere, A.; Nachtkamp, K.; et al. Treatment of acute myeloid leukemia or myelodysplastic syndrome relapse after allogeneic stem cell transplantation with azacitidine and donor lymphocyte infusions—A retrospective multicenter analysis from the German Cooperative Transplant Study Group. Biol. Blood Marrow Transplant. 2015, 21, 653–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsirigotis, P.; Danylesko, I.; Gkirkas, K.; Shem-Tov, N.; Yerushalmi, R.; Stamouli, M.; Avigdor, A.; Spyridonidis, A.; Gauthier, J.; Goldstein, G.; et al. Brentuximab vedotin in combination with or without donor lymphocyte infusion for patients with Hodgkin lymphoma after allogeneic stem cell transplantation. Bone Marrow Transplant. 2016, 51, 1313–1317. [Google Scholar] [CrossRef]
- Shanavas, M.; Messner, H.A.; Kamel-Reid, S.; Atenafu, E.G.; Gupta, V.; Kuruvilla, J.; Kim, D.D.; Uhm, J.; Lambie, A.; Ellis, L.; et al. A comparison of long-term outcomes of donor lymphocyte infusions and tyrosine kinase inhibitors in patients with relapsed CML after allogeneic hematopoietic cell transplantation. Clin. Lymphoma Myeloma Leuk. 2014, 14, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Hasskarl, J.; Zerweck, A.; Wäsch, R.; Ihorst, G.; Bertz, H.; Finke, J. Induction of graft versus malignancy effect after unrelated allogeneic PBSCT using donor lymphocyte infusions derived from frozen aliquots of the original graft. Bone Marrow Transplant. 2012, 47, 277–282. [Google Scholar] [CrossRef]
- Huang, X.-J.; Liu, D.-H.; Liu, K.-Y.; Xu, L.-P.; Chen, Y.-H.; Wang, Y.; Han, W.; Chen, H. Modified donor lymphocyte infusion after HLA-mismatched/haploidentical T cell-replete hematopoietic stem cell transplantation for prophylaxis of relapse of leukemia in patients with advanced leukemia. J. Clin. Immunol. 2008, 28, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.-J.; Wang, Y.; Liu, D.-H.; Xu, L.-P.; Chen, H.; Chen, Y.-H.; Han, W.; Shi, H.-X.; Liu, K.-Y. Modified donor lymphocyte infusion (DLI) for the prophylaxis of leukemia relapse after hematopoietic stem cell transplantation in patients with advanced leukemia--feasibility and safety study. J. Clin. Immunol. 2008, 28, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.-H.; Liu, D.-H.; Xu, L.-P.; Liu, K.-Y.; Zhao, T.; Wang, Y.; Chen, H.; Chen, Y.-H.; Han, W.; Huang, X.-J. Modified donor lymphocyte infusion-associated acute graft-versus-host disease after haploidentical T-cell-replete hematopoietic stem cell transplantation: Incidence and risk factors. Clin. Transplant. 2012, 26, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Rutella, S.; Zavala, F.; Danese, S.; Kared, H.; Leone, G. Granulocyte colony-stimulating factor: A novel mediator of T cell tolerance. J. Immunol. 2005, 175, 7085–7091. [Google Scholar] [CrossRef]
- Condomines, M.; Quittet, P.; Lu, Z.-Y.; Nadal, L.; Latry, P.; Lopez, E.; Baudard, M.; Requirand, G.; Duperray, C.; Schved, J.; et al. Functional regulatory T cells are collected in stem cell autografts by mobilization with high-dose cyclophosphamide and granulocyte colony-stimulating factor. J. Immunol. 2006, 176, 6631–6639. [Google Scholar] [CrossRef]
- Glucksberg, H.; Storb, R.; Fefer, A.; Buckner, C.D.; Neiman, P.E.; Clift, R.A.; Lerner, K.G.; Thomas, E.D. Clinical manifestations of graft-versus-host Disease in human recipients of marrow from HL-A-matched sibling donor,S. Transplantation 1974, 18, 295. [Google Scholar] [CrossRef]
- Thiede, C.; Florek, M.; Bornhauser, M.; Ritter, M.; Mohr, B.; Brendel, C.; Ehninger, G.; Neubauer, A. Rapid quantification of mixed chimerism using multiplex amplification of short tandem repeat markers and fluorescence detection. Bone Marrow Transplant. 1999, 23, 1055–1060. [Google Scholar] [CrossRef] [Green Version]
- Guillaume, T.; Porcheron, S.; Audat, F.; Bancillon, N.; Berceanu, A.; Charbonnier, A.; Dulery, R.; Edy, N.; El Cheikh, J.; Hermet, E.; et al. Prophylactic, preemptive and curative use of donor lymphocyte infusion in patients undergoing allogeneic stem cell transplantation: Guidelines of the SFGM-TC. Pathol. Biol. 2014, 62, 193–196. [Google Scholar] [CrossRef]
- Appelbaum, F.R. Hematopoietic-cell transplantation at 50. N. Engl. J. Med. 2007, 357, 1472–1475. [Google Scholar] [CrossRef] [Green Version]
- Spyridonidis, A.; Labopin, M.; Schmid, C.; Volin, L.; Yakoub-Agha, I.; Stadler, M.; Milpied, N.; Socie, G.; Browne, P.; Lenhoff, S.; et al. Outcomes and prognostic factors of adults with acute lymphoblastic leukemia who relapse after allogeneic hematopoietic cell transplantation. An analysis on behalf of the Acute Leukemia Working Party of EBMT. Leukemia 2012, 26, 1211–1217. [Google Scholar] [CrossRef] [Green Version]
- Shiobara, S.; Nakao, S.; Ueda, M.; Yamazaki, H.; Takahashi, S.; Asano, S.; Yabe, H.; Kato, S.; Imoto, S.; Maruta, A.; et al. Donor leukocyte infusion for Japanese patients with relapsed leukemia after allogeneic bone marrow transplantation: Lower incidence of acute graft-versus-host disease and improved outcome. Bone Marrow Transplant. 2000, 26, 769–774. [Google Scholar] [CrossRef] [Green Version]
- Bloor, A.J.; Thomson, K.; Chowdhry, N.; Verfuerth, S.; Ings, S.J.; Chakraverty, R.; Linch, D.C.; Goldstone, A.H.; Peggs, K.S.; MacKinnon, S. High response rate to donor lymphocyte infusion after allogeneic stem cell transplantation for indolent non-Hodgkin lymphoma. Biol. Blood Marrow Transplant. 2008, 14, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peggs, K.S.; Kayani, I.; Edwards, N.; Kottaridis, P.; Goldstone, A.H.; Linch, D.C.; Hough, R.; Morris, E.C.; Fielding, A.; Chakraverty, R.; et al. Donor lymphocyte infusions modulate relapse risk in mixed chimeras and induce durable salvage in relapsed patients after T-cell-depleted allogeneic transplantation for Hodgkin’s lymphoma. J. Clin. Oncol. 2011, 29, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, P.; Potter, V.T.; Barber, L.D.; Kulasekararaj, A.G.; Lim, Z.Y.; Pearce, R.M.; De Lavallade, H.; Kenyon, M.; Ireland, R.M.; Marsh, J.C.; et al. Outcome of donor lymphocyte infusion after T cell-depleted allogeneic hematopoietic stem cell transplantation for acute myelogenous leukemia and myelodysplastic syndromes. Biol. Blood Marrow Transplant. 2013, 19, 562–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutz, C.; Massenkeil, G.; Nagy, M.; Neuburger, S.; Tamm, I.; Rosen, O.; Dörken, B.; Arnold, R. A pilot study of prophylactic donor lymphocyte infusions to prevent relapse in adult acute lymphoblastic leukemias after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2008, 41, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Dey, B.R.; McAfee, S.; Colby, C.; Sackstein, R.; Saidman, S.; Tarbell, N.; Sachs, D.; Sykes, M.; Spitzer, T.R. Impact of prophylactic donor leukocyte infusions on mixed chimerism, graft-versus-host disease, and antitumor response in patients with advanced hematologic malignancies treated with nonmyeloablative conditioning and allogeneic bone marrow transplantation. Biol. Blood Marrow Transplant. 2003, 9, 320–329. [Google Scholar] [CrossRef] [Green Version]
- Schneidawind, C.; Jahnke, S.; Schober-Melms, I.; Schumm, M.; Handgretinger, R.; Faul, C.; Kanz, L.; Bethge, W.; Schneidawind, D. G-CSF administration prior to donor lymphocyte apheresis promotes anti-leukaemic effects in allogeneic HCT patients. Br. J. Haematol. 2019, 186, 60–71. [Google Scholar] [CrossRef]
- Abbi, K.K.S.; Zhu, J.; Ehmann, W.C.; Epner, E.; Carraher, M.; Mierski, J.; Talamo, G.; Lucas, K.; Rybka, W.; Claxton, D. G-CSF mobilized vs conventional donor lymphocytes for therapy of relapse or incomplete engraftment after allogeneic hematopoietic transplantation. Bone Marrow Transplant. 2013, 48, 357–362. [Google Scholar] [CrossRef] [Green Version]
- Hossain, N.M.; Klumpp, T.; Ulicny, J.; Gaener, M.; Kropf, P.L.; Mangan, K.F.; Barta, S.K.; Fung, H.C.; Martin, M.E. Donor Lymphocyte Infusion in Hematologic Malignancies—Good to be Fresh? Clin. Lymphoma Myeloma Leuk. 2016, 16, 111–115. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All DLI n = 139 | Classical DLI n = 68 (48.9%) | gDLI n = 71 (51.1%) | p | |
|---|---|---|---|---|
| Age at DLI, median (IQR) | 52 (41–61) | 49 (24–58) | 55 (47–63) | <0.01 |
| Men, n (%) | 76 (54.7) | 39 (57.4) | 37 (52.1) | 0.61 |
| Disease, n (%) | 0.05 | |||
| Acute lymphoblastic leukaemia | 20 (14.4) | 15 (22.1) | 5 (7.1) | |
| Acute myeloblastic leukaemia | 45 (32.4) | 20 (29.4) | 25 (35.2) | |
| Hodgkin lymphoma | 8 (5.8) | 3 (4.4) | 5 (7.1) | |
| Chronic lymphocytic leukaemia | 7 (5.0) | 6 (8.8) | 1 (1.4) | |
| Chronic myeloid leukaemia | 2 (1.4) | 1 (1.5) | 1 (1.4) | |
| Non-Hodgkin Lymphoma | 10 (7.2) | 3 (4.4) | 7 (9.9) | |
| Myeloma | 38 (27.3) | 18 (26.5) | 20 (28.2) | |
| Osteomyelofibrosis | 1 (0.7) | 0 | 1 (1.4) | |
| Myelodysplasia | 8 (5.8) | 2 (2.9) | 6 (8.5) | |
| Status at transplant, n (%) | 0.95 | |||
| Complete remission | 76 (54.7) | 37 (54.4) | 39 (54.9) | |
| Partial remission | 38 (27.3) | 18 (26.5) | 20 (28.2) | |
| Stable or progressive disease | 25 (18.0) | 13 (19.1) | 12 (16.9) | |
| Conditioning, n (%), n = 138 | n = 70 | 0.02 | ||
| Myeloablative conditioning | 32 (23.2) | 22 (32.4) | 10 (14.3) | |
| Reduced intensity conditioning | 92 (66.7) | 42 (61.8) | 50 (71.4) | |
| Sequential | 14 (10.1) | 4 (5.9) | 10 (14.3) | |
| Donor type, n (%) | <0.001 | |||
| Related | 68 (48.9) | 44 (64.7) | 24 (33.8) | |
| Unrelated | 71 (51.1) | 24 (35.3) | 47 (66.2) | |
| HLA compatibility, n (%) | 0.30 | |||
| 10/10 | 122 (87.8) | 62 (91.2) | 60 (84.5) | |
| 9/10 | 17 (12.2) | 6 (8.8) | 11 (15.5) | |
| Cell source, n (%) | <0.0001 | |||
| Bone marrow | 24 (17.3) | 24 (35.3) | 0 | |
| Peripheral hematopoietic stem cells | 115 (82.7) | 44 (64.7) | 71 (100) | |
| CD34 cells (×106), median, (IQR) | 5.0 (4.4–5.5) | 4.7 (4.0–5.5) | n = 70 5.0 (5.0–5.4) | 0.02 |
| CD3 cells (×107), median (IQR) | 16.9 (9.6–23.0) | 16.9 (5.5–29.8) | n = 70 16.9 (10.8–20.6) | 0.99 |
| GvHD, n (%) | 0.86 | |||
| All grades of acute GvHD | 111(79.9) | 48 (70.6) | 63 (88.7) | |
| Grade 1 acute GvHD | 80 (57.6) | 37 (54.4) | 43 (60.6) | |
| Grade 2 acute GvHD | 21 (15.1) | 5 (7.4) | 16 (22.5) | |
| Grade 3 acute GvHD | 9 (6.5) | 5 (7.4) | 4 (5.6) | |
| Grade 4 acute GvHD | 0 | 0 | 0 | |
| Chronic GvHD, n (%) | 22 (15.8) | 15 (22.1) | 7 (9.9) | 0.04 |
| 3-month chimerism, n (%), n = 138 | n = 67 | 0.39 | ||
| 100% donor | 56 (40.6) | 30 (44.8) | 26 (36.6) | |
| Mixed | 81 (58.7) | 37 (55.2) | 44 (62.0) | |
| Recipient | 1 (0.7) | 1 (1.4) | ||
| Indication for DLI 1, n (%) | 0.84 | |||
| Pre-emptive: mixed chimerism | 22 (15.8) | 11 (16.2) | 11 (15.5) | |
| Pre-emptive: detectable minimal residual disease | 21 (15.1) | 9 (13.2) | 12 (16.9) | |
| Relapse | 96 (69.1) | 48 (70.6) | 48 (67.6) | |
| Number of DLIs, n (%) | 0.24 | |||
| <3 | 105 (75.5) | 48 (70.6) | 57 (80.3) | |
| ≥3 | 34 (24.5) | 20 (29.4) | 14 (19.7) | |
| Period, n (%) | <0.0001 | |||
| 1998–2004 | 18 (12.9) | 18 (26.5) | 0 | |
| 2005–2011 | 59 (42.4) | 33 (48.5) | 26 (36.6) | |
| 2012–2018 | 62 (44.6) | 17 (25.0) | 45 (63.4) | |
| Associated treatment with DLI, n = 133 | n = 62 | 0.14 | ||
| Yes | 46(34.6) | 17 (27.4) | 29 (40.8) | |
| No | 87(65.4) | 45 (72.6) | 42 (59.2) |
| DLI 1 | DLI 2 | DLI 3 | DLI 4 | DLI 5 | DLI 6 | DLI 7 | |
|---|---|---|---|---|---|---|---|
| Patients, n (%) | 139 (100) | 67 (48.2) | 34 (24.5) | 15 (10.8) | 7 (5.0) | 5 (3.6) | 1 (0.7) |
| Term, median from transplant (IQR) (month) | 8.5 (5.7–15.5) | 14.4 (11.3–24.1) | 27.1 (18.0–65.1) | 48.6 (26.6–71.5) | 60.2 (58.4–68.0) | 71.6 (71.2–72.9) | 73.3 (NA) |
| CD3+, median (IQR) (107/kg) | 1 (0.5–1) | 1.4 (1–5) | 2.2 (1–6.6) | 3.4 (1.8–5.5) | 5 (1.1–10) | 2.5 (1.2–5.2) | 1 (NA) |
| All DLI n = 139 | Classical DLI n = 68 (48.9%) | gDLI n = 71 (51.1%) | p | |
|---|---|---|---|---|
| Complete response, n (%), n = 131 | n = 64 | n = 67 | 0.28 | |
| Yes | 50 (38.2) | 21 (32.8) | 29 (43.3) | |
| No | 81 (61.8) | 43 (67.2) | 38 (56.7) | |
| Post-DLI GvHD, n (%), n = 137 | n = 66 | |||
| All grades of GvHD | 64 (46.7) | 30 (45.5) | 34 (47.9) | 0.86 |
| Treatment-requiring GvHD, n (%) | 32 (23.4) | 14 (21.2) | 18 (25.4) | 0.81 |
| Chimerism, n (%), n = 127 | n = 61 | n = 66 | 0.63 | |
| 100% donor | 88 (69.3) | 43 (70.5) | 45 (68.2) | |
| Mixed | 38 (29.9) | 17 (27.9) | 21 (31.8) | |
| Recipient | 1 (0.8) | 1 (1.6) | ||
| Progression-free survival | ||||
| Median PFS (months, IQR) | 9 (3–35) | 11 (2–35) | 9 (4–33) | 0.90 |
| 5-year PFS (%, IQR) | 38 (29–48) | 36 (24–52) | 40 (29–56) | |
| Overall survival, | ||||
| Median OS (months, IQR) | 22 (6–50) | 22 (4–33) | 21 (6–47) | 0.50 |
| 5 years of OS (%, IQR) | 37 (29–47) | 37 (27–52) | 36 (26–52) | |
| Cause of Mortality, n (%), n = 82 | n = 70 | 0.14 | ||
| Progression | 65 (47.1) | 37 (54.4) | 28 (40) | |
| Toxicity | 14 (10.1) | 5 (7.4) | 9 (12.9) | |
| Other | 3 (2.2) | 0 | 3 (4.3) |
| Univariate OR (95% CI) | p | Multivariate OR (95% CI) * | p | |
|---|---|---|---|---|
| Age at DLI1 >60 years, n = 38 | 0.94 (0.42–2.08) | 0.88 | ||
| Gender | ||||
| Female | 1 (ref) | - | ||
| Male (n = 76) | 0.82 (0.41–1.68) | 0.59 | ||
| Disease | 14.07 (4.05–59.57) | <0.0001 | ||
| Hodgkin Lymphoma | 2.12 (0.41–10.99) | 0.37 | ||
| Acute lymphoblastic leukaemia | 1.01 (0.29–3.45) | 0.99 | ||
| Acute myeloblastic leukaemia | 1 (ref) | - | ||
| Chronic lymphocytic leukaemia | 2.12 (0.41–10.99) | 0.37 | ||
| Chronic myeloid leukaemia | 2.83 (0.16–49.22) | 0.48 | ||
| Non-Hodgkin lymphoma | 11.28 (2.07–61.44) | <0.01 | ||
| Multiple myeloma | 1.67 (0.63–4.40) | 0.30 | ||
| Osteomyelofibrosis | 2.71 × 10−4 (3.59 × 10−91–2.04 × 1083) | 0.94 | ||
| Myelodysplasia | 8.46 (1.48–48.26) | 0.02 | ||
| Indication for DLI | ||||
| Pre-emptive | 1 (ref) | - | ||
| Relapse | 0.21 (0.09–0.45) | <0.0001 | 0.18 (0.07–0.45) | <0.001 |
| Associated treatment | ||||
| No | 1 (ref) | |||
| Yes | 0.59 (0.27–1.27) | 0.18 | ||
| Type of DLI | ||||
| Classical | 1 (ref) | - | ||
| gDLI | 1.56 (0.77–3.18) | 0.22 | ns | |
| Post DLI GvHD | 8.53 (3.01–26.78) | <0.0001 | ||
| No GvHD | 1 (ref) | |||
| GvHD not requiring treatment | 1.91 (0.78–4.69) | 0.16 | ||
| Treatment-requiring GvHD | 9.08 (3.28–25.14) | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamure, S.; Paul, F.; Gagez, A.-L.; Delage, J.; Vincent, L.; Fegueux, N.; Sirvent, A.; Gehlkopf, E.; Veyrune, J.L.; Yang, L.Z.; et al. A Retrospective Comparison of DLI and gDLI for Post-Transplant Treatment. J. Clin. Med. 2020, 9, 2204. https://doi.org/10.3390/jcm9072204
Lamure S, Paul F, Gagez A-L, Delage J, Vincent L, Fegueux N, Sirvent A, Gehlkopf E, Veyrune JL, Yang LZ, et al. A Retrospective Comparison of DLI and gDLI for Post-Transplant Treatment. Journal of Clinical Medicine. 2020; 9(7):2204. https://doi.org/10.3390/jcm9072204
Chicago/Turabian StyleLamure, Sylvain, Franciane Paul, Anne-Laure Gagez, Jérémy Delage, Laure Vincent, Nathalie Fegueux, Anne Sirvent, Eve Gehlkopf, Jean Luc Veyrune, Lu Zhao Yang, and et al. 2020. "A Retrospective Comparison of DLI and gDLI for Post-Transplant Treatment" Journal of Clinical Medicine 9, no. 7: 2204. https://doi.org/10.3390/jcm9072204
APA StyleLamure, S., Paul, F., Gagez, A. -L., Delage, J., Vincent, L., Fegueux, N., Sirvent, A., Gehlkopf, E., Veyrune, J. L., Yang, L. Z., Kanouni, T., Cacheux, V., Moreaux, J., Bonafoux, B., Cartron, G., De Vos, J., & Ceballos, P. (2020). A Retrospective Comparison of DLI and gDLI for Post-Transplant Treatment. Journal of Clinical Medicine, 9(7), 2204. https://doi.org/10.3390/jcm9072204