Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. 99 mTc-Tetrofosmin SPECT-MPI
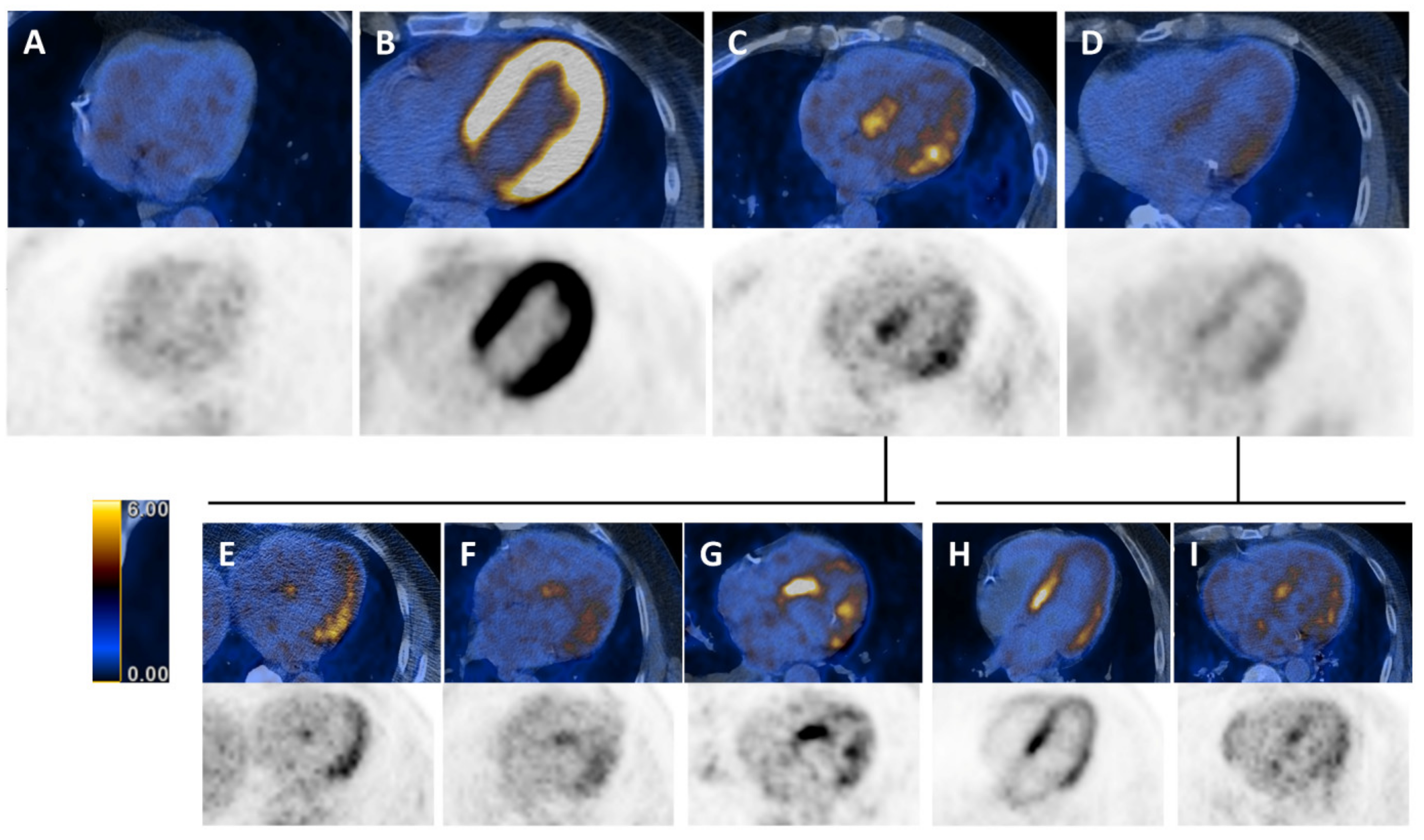
2.3. Whole-Body 18F-FDG PET/CT and Assessment of Myocardial 18F-FDG Uptake
2.4. Statistical Analysis
3. Results
3.1. Study Population
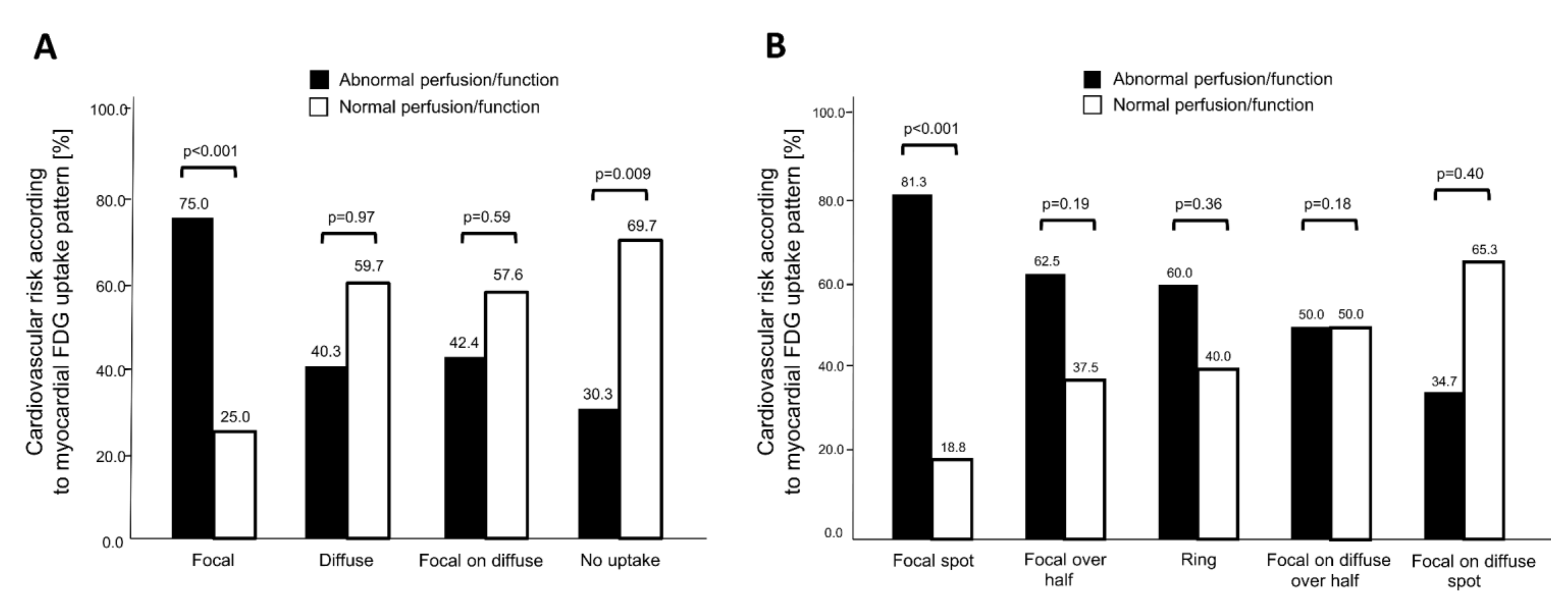
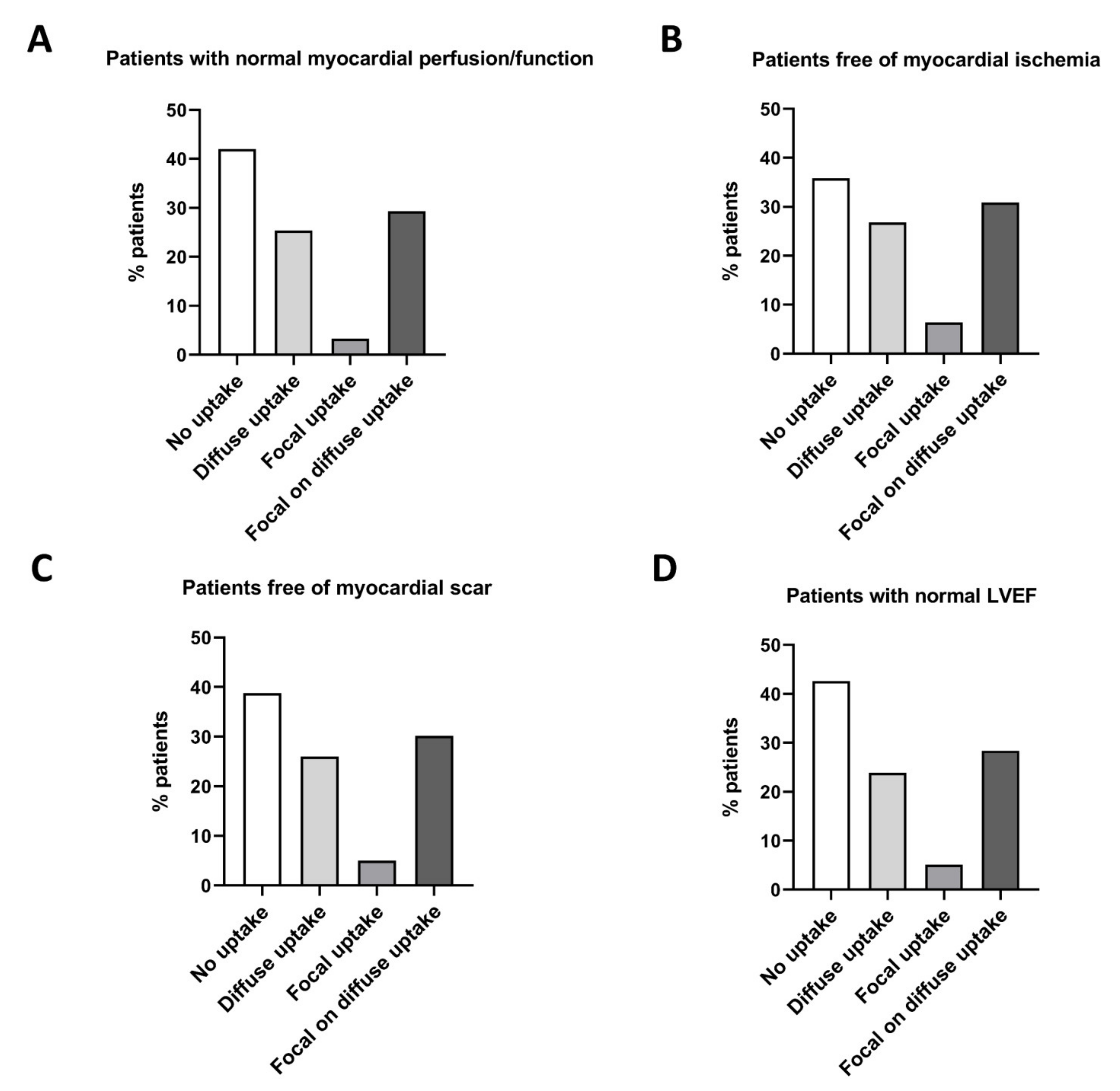
3.2. Association of 18F-FDG Uptake Patterns with Impaired Myocardial Function
3.3. Prognostic Value of Myocardial 18F-FDG Uptake in Patients Undergoing Oncologic PET/CT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lardinois, D.; Weder, W.; Hany, T.F.; Kamel, E.M.; Korom, S.; Seifert, B.; von Schulthess, G.K.; Steinert, H.C. Staging of non-small-cell lung cancer with integrated positron-emission tomography and computed tomography. N. Engl. J. Med. 2003, 348, 2500–2507. [Google Scholar] [CrossRef] [Green Version]
- Fischer, B.; Lassen, U.; Mortensen, J.; Larsen, S.; Loft, A.; Bertelsen, A.; Ravn, J.; Clementsen, P.; Hogholm, A.; Larsen, K.; et al. Preoperative staging of lung cancer with combined PET-CT. N. Engl. J. Med. 2009, 361, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, P.; Attal, M.; Caillot, D.; Macro, M.; Karlin, L.; Garderet, L.; Facon, T.; Benboubker, L.; Escoffre-Barbe, M.; Stoppa, A.M.; et al. Prospective Evaluation of Magnetic Resonance Imaging and [(18)F]Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography at Diagnosis and Before Maintenance Therapy in Symptomatic Patients With Multiple Myeloma Included in the IFM/DFCI 2009 Trial: Results of the IMAJEM Study. J. Clin. Oncol. 2017, 35, 2911–2918. [Google Scholar] [CrossRef] [PubMed]
- Lordick, F.; Ott, K.; Krause, B.J.; Weber, W.A.; Becker, K.; Stein, H.J.; Lorenzen, S.; Schuster, T.; Wieder, H.; Herrmann, K.; et al. PET to assess early metabolic response and to guide treatment of adenocarcinoma of the oesophagogastric junction: The MUNICON phase II trial. Lancet Oncol. 2007, 8, 797–805. [Google Scholar] [CrossRef]
- Fuchs, M.; Goergen, H.; Kobe, C.; Kuhnert, G.; Lohri, A.; Greil, R.; Sasse, S.; Topp, M.S.; Schafer, E.; Hertenstein, B.; et al. Positron Emission Tomography-Guided Treatment in Early-Stage Favorable Hodgkin Lymphoma: Final Results of the International, Randomized Phase III HD16 Trial by the German Hodgkin Study Group. J. Clin. Oncol. 2019, 37, 2835–2845. [Google Scholar] [CrossRef]
- Jaarsma, C.; Leiner, T.; Bekkers, S.C.; Crijns, H.J.; Wildberger, J.E.; Nagel, E.; Nelemans, P.J.; Schalla, S. Diagnostic performance of noninvasive myocardial perfusion imaging using single-photon emission computed tomography, cardiac magnetic resonance, and positron emission tomography imaging for the detection of obstructive coronary artery disease: A meta-analysis. J. Am. Coll. Cardiol. 2012, 59, 1719–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebhard, C.E.; Maredziak, M.; Portmann, A.; Bengs, S.; Haider, A.; Fiechter, M.; Herzog, B.A.; Messerli, M.; Treyer, V.; Kudura, K.; et al. Heart rate reserve is a long-term risk predictor in women undergoing myocardial perfusion imaging. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2032–2041. [Google Scholar] [CrossRef]
- Haider, A.; Bengs, S.; Maredziak, M.; Messerli, M.; Fiechter, M.; Giannopoulos, A.A.; Treyer, V.; Schwyzer, M.; Kamani, C.H.; Patriki, D.; et al. Heart rate reserve during pharmacological stress is a significant negative predictor of impaired coronary flow reserve in women. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1257–1267. [Google Scholar] [CrossRef] [PubMed]
- Joshi, N.V.; Vesey, A.T.; Williams, M.C.; Shah, A.S.; Calvert, P.A.; Craighead, F.H.; Yeoh, S.E.; Wallace, W.; Salter, D.; Fletcher, A.M.; et al. 18F-fluoride positron emission tomography for identification of ruptured and high-risk coronary atherosclerotic plaques: A prospective clinical trial. Lancet 2014, 383, 705–713. [Google Scholar] [CrossRef] [Green Version]
- Fiechter, M.; Haider, A.; Bengs, S.; Maredziak, M.; Burger, I.A.; Roggo, A.; Portmann, A.; Schade, K.; Warnock, G.I.; Treyer, V.; et al. Sex-dependent association between inflammation, neural stress responses, and impaired myocardial function. Eur. J. Nucl. Med. Mol. Imaging 2019. [Google Scholar] [CrossRef]
- Fiechter, M.; Bengs, S.; Roggo, A.; Haider, A.; Maredziak, M.; Portmann, A.; Treyer, V.; Burger, I.A.; Messerli, M.; Patriki, D.; et al. Association between vertebral bone mineral density, myocardial perfusion, and long-term cardiovascular outcomes: A sex-specific analysis. J. Nucl. Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Rischpler, C.; Dirschinger, R.J.; Nekolla, S.G.; Kossmann, H.; Nicolosi, S.; Hanus, F.; van Marwick, S.; Kunze, K.P.; Meinicke, A.; Götze, K.; et al. Prospective Evaluation of 18F-Fluorodeoxyglucose Uptake in Postischemic Myocardium by Simultaneous Positron Emission Tomography/Magnetic Resonance Imaging as a Prognostic Marker of Functional Outcome. Circ. Cardiovasc. Imaging 2016, 9, e004316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aikawa, T.; Naya, M.; Manabe, O.; Obara, M.; Matsushima, S.; Tamaki, N.; Tsutsui, H. Incidental focal myocardial 18F-FDG uptake indicating asymptomatic coronary artery disease. J. Nucl. Cardiol. 2016, 23, 596–598. [Google Scholar] [CrossRef] [Green Version]
- Dou, K.F.; Yang, M.F.; Yang, Y.J.; Jain, D.; He, Z.X. Myocardial 18F-FDG uptake after exercise-induced myocardial ischemia in patients with coronary artery disease. J. Nucl. Med. 2008, 49, 1986–1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, N.; Rimoldi, O.E.; Beanlands, R.S.; Camici, P.G. Assessment of myocardial ischaemia and viability: Role of positron emission tomography. Eur. Heart J. 2010, 31, 2984–2995. [Google Scholar] [CrossRef]
- Accordino, M.K.; Neugut, A.I.; Hershman, D.L. Cardiac effects of anticancer therapy in the elderly. J. Clin. Oncol. 2014, 32, 2654–2661. [Google Scholar] [CrossRef] [Green Version]
- Sturgeon, K.M.; Deng, L.; Bluethmann, S.M.; Zhou, S.; Trifiletti, D.M.; Jiang, C.; Kelly, S.P.; Zaorsky, N.G. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur. Heart J. 2019. [Google Scholar] [CrossRef] [Green Version]
- Fiechter, M.; Roggo, A.; Burger, I.A.; Bengs, S.; Treyer, V.; Becker, A.; Maredziak, M.; Haider, A.; Portmann, A.; Messerli, M.; et al. Association between resting amygdalar activity and abnormal cardiac function in women and men: A retrospective cohort study. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 625–632. [Google Scholar] [CrossRef]
- Pazhenkottil, A.P.; Nkoulou, R.N.; Ghadri, J.R.; Herzog, B.A.; Buechel, R.R.; Kuest, S.M.; Wolfrum, M.; Fiechter, M.; Husmann, L.; Gaemperli, O.; et al. Prognostic value of cardiac hybrid imaging integrating single-photon emission computed tomography with coronary computed tomography angiography. Eur. Heart J. 2011, 32, 1465–1471. [Google Scholar] [CrossRef] [Green Version]
- Hesse, B.; Tagil, K.; Cuocolo, A.; Anagnostopoulos, C.; Bardies, M.; Bax, J.; Bengel, F.; Busemann Sokole, E.; Davies, G.; Dondi, M.; et al. EANM/ESC procedural guidelines for myocardial perfusion imaging in nuclear cardiology. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 855–897. [Google Scholar] [CrossRef]
- Verberne, H.J.; Acampa, W.; Anagnostopoulos, C.; Ballinger, J.; Bengel, F.; De Bondt, P.; Buechel, R.R.; Cuocolo, A.; van Eck-Smit, B.L.; Flotats, A.; et al. EANM procedural guidelines for radionuclide myocardial perfusion imaging with SPECT and SPECT/CT: 2015 revision. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1929–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, D.S.; Kiat, H.; Friedman, J.D.; Wang, F.P.; van Train, K.; Matzer, L.; Maddahi, J.; Germano, G. Separate acquisition rest thallium-201/stress technetium-99m sestamibi dual-isotope myocardial perfusion single-photon emission computed tomography: A clinical validation study. J. Am. Coll. Cardiol. 1993, 22, 1455–1464. [Google Scholar] [CrossRef] [Green Version]
- Haider, A.; Possner, M.; Messerli, M.; Bengs, S.; Osto, E.; Maredziak, M.; Portmann, A.; Fiechter, M.; Giannopoulos, A.A.; Treyer, V.; et al. Quantification of intrathoracic fat adds prognostic value in women undergoing myocardial perfusion imaging. Int. J. Cardiol. 2019, 292, 258–264. [Google Scholar] [CrossRef]
- Siegrist, P.T.; Gaemperli, O.; Koepfli, P.; Schepis, T.; Namdar, M.; Valenta, I.; Aiello, F.; Fleischmann, S.; Alkadhi, H.; Kaufmann, P.A. Repeatability of cold pressor test-induced flow increase assessed with H(2)(15)O and PET. J. Nucl. Med. 2006, 47, 1420–1426. [Google Scholar] [PubMed]
- Wyss, C.A.; Koepfli, P.; Fretz, G.; Seebauer, M.; Schirlo, C.; Kaufmann, P.A. Influence of altitude exposure on coronary flow reserve. Circulation 2003, 108, 1202–1207. [Google Scholar] [CrossRef] [Green Version]
- Koepfli, P.; Wyss, C.A.; Namdar, M.; Klainguti, M.; von Schulthess, G.K.; Luscher, T.F.; Kaufmann, P.A. Beta-adrenergic blockade and myocardial perfusion in coronary artery disease: Differential effects in stenotic versus remote myocardial segments. J. Nucl. Med. 2004, 45, 1626–1631. [Google Scholar]
- Fiechter, M.; Haider, A.; Bengs, S.; Maredziak, M.; Burger, I.A.; Roggo, A.; Portmann, A.; Warnock, G.I.; Schade, K.; Treyer, V.; et al. Sex Differences in the Association between Inflammation and Ischemic Heart Disease. Thromb. Haemost. 2019, 119, 1471–1480. [Google Scholar] [CrossRef]
- Burger, I.A.; Lohmann, C.; Messerli, M.; Bengs, S.; Becker, A.; Maredziak, M.; Treyer, V.; Haider, A.; Schwyzer, M.; Benz, D.C.; et al. Age- and sex-dependent changes in sympathetic activity of the left ventricular apex assessed by 18F-DOPA PET imaging. PLoS ONE 2018, 13, e0202302. [Google Scholar] [CrossRef]
- Nose, H.; Otsuka, H.; Otomi, Y.; Terazawa, K.; Takao, S.; Iwamoto, S.; Iwase, T.; Yamada, H.; Sata, M.; Harada, M. The physiological uptake pattern of (18)F-FDG in the left ventricular myocardium of patients without heart disease. J. Med. Investig. 2014, 61, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Floyd, J.D.; Nguyen, D.T.; Lobins, R.L.; Bashir, Q.; Doll, D.C.; Perry, M.C. Cardiotoxicity of cancer therapy. J. Clin. Oncol. 2005, 23, 7685–7696. [Google Scholar] [CrossRef]
- Minamimoto, R.; Morooka, M.; Miyata, Y.; Ito, K.; Okasaki, M.; Hara, H.; Okazaki, O.; Moroi, M.; Kubota, K. Incidental focal FDG uptake in heart is a lighthouse for considering cardiac screening. Ann. Nucl. Med. 2013, 27, 572–580. [Google Scholar] [CrossRef]
- Chavez-MacGregor, M.; Niu, J.; Zhang, N.; Elting, L.S.; Smith, B.D.; Banchs, J.; Hortobagyi, G.N.; Giordano, S.H. Cardiac Monitoring During Adjuvant Trastuzumab-Based Chemotherapy Among Older Patients With Breast Cancer. J. Clin. Oncol. 2015, 33, 2176–2183. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Zhao, Y.; Chen, C.; Han, C.; Xue, L.; Xing, D.; Huang, O.; Tao, M. BNP as a marker for early prediction of anthracycline-induced cardiotoxicity in patients with breast cancer. Oncol. Lett. 2019, 18, 4992–5001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanderian, A.S.; Francis, G.S. Cardiac troponins and chronic kidney disease. Kidney Int. 2006, 69, 1112–1114. [Google Scholar] [CrossRef] [Green Version]
- Tarkin, J.M.; Joshi, F.R.; Rudd, J.H. PET imaging of inflammation in atherosclerosis. Nat. Rev. Cardiol. 2014, 11, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Birnie, D.H.; Kandolin, R.; Nery, P.B.; Kupari, M. Cardiac manifestations of sarcoidosis: Diagnosis and management. Eur. Heart J. 2016, 38, 2663–2670. [Google Scholar] [CrossRef] [Green Version]
- Gewirtz, H.; Dilsizian, V. Myocardial viability. Circ. Res. 2017, 120, 1197–1212. [Google Scholar] [CrossRef] [PubMed]
- Ohira, H.; Tsujino, I.; Ishimaru, S.; Oyama, N.; Takei, T.; Tsukamoto, E.; Miura, M.; Sakaue, S.; Tamaki, N.; Nishimura, M. Myocardial imaging with 18F-fluoro-2-deoxyglucose positron emission tomography and magnetic resonance imaging in sarcoidosis. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Pak, K.; Kim, K. Diagnostic performance of F-18 FDG PET for detection of cardiac sarcoidosis; A systematic review and meta-analysis. J. Nucl. Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ishimaru, S.; Tsujino, I.; Takei, T.; Tsukamoto, E.; Sakaue, S.; Kamigaki, M.; Ito, N.; Ohira, H.; Ikeda, D.; Tamaki, N.; et al. Focal uptake on 18F-fluoro-2-deoxyglucose positron emission tomography images indicates cardiac involvement of sarcoidosis. Eur. Heart J. 2005, 26, 1538–1543. [Google Scholar] [CrossRef]
- Stanley, W.C.; Recchia, F.A.; Lopaschuk, G.D. Myocardial substrate metabolism in the normal and failing heart. Physiol. Rev. 2005, 85, 1093–1129. [Google Scholar] [CrossRef]
- Dorbala, S.; Di Carli, M.F.; Delbeke, D.; Abbara, S.; DePuey, E.G.; Dilsizian, V.; Forrester, J.; Janowitz, W.; Kaufmann, P.A.; Mahmarian, J.; et al. SNMMI/ASNC/SCCT guideline for cardiac SPECT/CT and PET/CT 1.0. J. Nucl. Med. 2013, 54, 1485–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, L.K.; Hoffman, J.M.; Bacharach, S.; Graham, M.M.; Karp, J.; Lammertsma, A.A.; Larson, S.; Mankoff, D.A.; Siegel, B.A.; Van den Abbeele, A.; et al. Consensus recommendations for the use of 18F-FDG PET as an indicator of therapeutic response in patients in National Cancer Institute Trials. J. Nucl. Med. 2006, 47, 1059–1066. [Google Scholar]
- Maurer, A.H.; Burshteyn, M.; Adler, L.P.; Steiner, R.M. How to differentiate benign versus malignant cardiac and paracardiac 18F FDG uptake at oncologic PET/CT. Radiographics 2011, 31, 1287–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, L.R.; Gropler, R.J. Radionuclide imaging of myocardial metabolism. Circ. Cardiovasc. Imaging 2010, 3, 211–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camici, P.; Araujo, L.I.; Spinks, T.; Lammertsma, A.A.; Kaski, J.C.; Shea, M.J.; Selwyn, A.P.; Jones, T.; Maseri, A. Increased uptake of 18F-fluorodeoxyglucose in postischemic myocardium of patients with exercise-induced angina. Circulation 1986, 74, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Total Cohort n = 302 | No Myocardial 18F-FDG Uptake n = 109 | Diffuse Myocardial 18F-FDG Uptake n = 77 | Focal Myocardial 18F-FDG Uptake n = 24 | Focal on Diffuse Myocardial 18F-FDG Uptake n = 92 | p-Value |
|---|---|---|---|---|---|---|
| Male sex, n (%) | 210 (71.4) | 75 (68.8) | 50 (64.9) | 18 (75.0) | 67 (72.8) | 0.58 |
| Age, mean ± SD | 66.8 ± 10.2 | 66.2 ± 11.1 | 66.9 ± 9.5 | 65.1 ± 10.6 | 68.0 ± 9.7 | 0.49 |
| BMI, mean ± SD | 26.2 ± 5.3 | 26.2 ± 5.1 | 25.1 ± 5.1 | 28.6 ± 5.4 | 26.4 ± 5.3 | 0.05 |
| Active malignancy, n (%) | 193 (63.9) | 80 (73.4) | 43 (55.8) | 14 (58.3) | 56 (60.9) | 0.07 |
| Diabetes, n (%) | 56 (18.5) | 23 (21.1) | 8 (10.4) | 5 (20.8) | 20 (21.7) | 0.21 |
| Hypertension, n (%) | 142 (47.0) | 46 (42.2) | 40 (51.9) | 11 (45.8) | 45 (48.9) | 0.59 |
| Smoking, n (%) | 93 (30.9) | 35 (32.1) | 20 (26.0) | 9 (37.5) | 29 (31.9) | 0.69 |
| Dyslipidemia, n (%) | 73 (24.2) | 25 (22.9) | 19 (24.7) | 6 (25.0) | 23 (25.0) | 0.98 |
| Positive family history, n (%) | 25 (8.3) | 9 (8.3) | 7 (9.1) | 5 (20.8) | 4 (4.3) | 0.074 |
| Known CAD, n (%) | 117 (38.7) | 45 (41.3) | 27 (35.1) | 13 (54.2) | 32 (34.8) | 0.29 |
| Previous MI, n (%) | 54 (18.9) | 17 (15.6) | 16 (20.8) | 8 (33.3) | 16 (17.4) | 0.23 |
| Previous PCI/CABG, n (%) | 82 (27.2) | 32 (29.4) | 18 (23.4) | 7 (29.2) | 25 (27.2) | 0.83 |
| Symptoms, n (%) Typical angina Atypical angina Dyspnea None | 30 (9.9) 23 (7.6) 39 (12.9) 210 (69.5) | 9 (8.3) 8 (7.3) 18 (16.5) 74 (67.9) | 7 (9.1) 2 (2.6) 10 (13.0) 58 (75.3) | 6 (25.0) 3 (12.5) 1 (4.2) 14 (58.3) | 8 (8.7) 10 (10.9) 10 (10.9) 64 (69.6) | 0.114 |
| Chronic pain, n (%) | 90 (30.1) | 33 (31.1) | 20 (26.0) | 11 (45.8) | 26 (28.3) | 0.30 |
| Depression, n (%) | 19 (6.5) | 6 (5.8) | 8 (10.4) | 1 (4.3) | 4 (4.5) | 0.43 |
| Medication, n (%) Statin Betablocker ACE inhibitors/ARBs Aspirin Corticosteroids Analgesics | 126 (44.5) 146 (51.6) 156 (55.1) 128 (45.2) 40 (14.2) 135 (47.9) | 43 (42.6) 52 (51.5) 48 (47.5) 43 (42.6) 17 (16.8) 51 (50.5) | 33 (45.2) 36 (49.3) 46 (63.0) 37 (50.7) 9 (12.3) 40 (54.8) | 13 (59.1) 14 (63.6) 16 (72.7) 11 (50.0) 4 (18.2) 10 (45.5) | 37 (42.5) 44 (50.6) 46 (52.9) 37 (42.5) 10 (11.6) 34 (39.5) | 0.53 0.69 0.07 0.65 0.67 0.25 |
| Creatinine (µM/L), mean ± SD | 116.3 ± 124.0 | 102.0 ± 94.1 | 118.1 ± 126.9 | 173.0 ± 210.3 | 117.3 ± 122.0 | 0.11 |
| CRP (mg/L), mean ± SD | 24.6 ± 43.5 | 28.5 ± 47.6 | 19.5 ± 39.0 | 29.1 ± 37.6 | 22.8 ± 43.4 | 0.59 |
| WCB count (10*/µ/L), mean ± SD | 7.8 ± 3.3 | 8.2 ± 3.3 | 7.3 ± 3.2 | 8.0 ± 4.4 | 7.8 ± 2.9 | 0.44 |
| NT proBNP (ƞg/L), mean ± SD | 3604.2 ± 13345.4 | 903.0 ± 1406.3 | 13584.3 ± 27932.0 | 2306.2 ± 2229.4 | 718.4 ± 808.6 | 0.045 |
| Baseline Characteristics | Total Cohort n = 302 | Normal Myocardial Perfusion/Function n = 181 | Abnormal Myocardial Perfusion/Function n = 121 | p-Value |
|---|---|---|---|---|
| Male sex, n (%) | 210 (71.4) | 113 (38.4) | 97 (33.0) | 0.002 |
| Age, mean ± SD | 66.8 ± 10.2 | 66.5 ± 10.5 | 67.4 ± 9.8 | 0.45 |
| BMI, mean ± SD | 26.2 ± 5.3 | 26.1 ± 5.2 | 26.3 ± 5.3 | 0.74 |
| Active malignancy, n (%) | 193 (63.9) | 118 (39.1) | 75 (24.8) | 0.33 |
| Diabetes, n (%) | 56 (18.5) | 33 (10.9) | 23 (7.6) | 0.49 |
| Hypertension, n (%) | 142 (47.0) | 84 (27.8) | 58 (19.2) | 0.44 |
| Smoking, n (%) | 93 (30.9) | 54 (17.9) | 39 (13.0) | 0.39 |
| Dyslipidemia, n (%) | 73 (24.2) | 42 (13.9) | 31 (10.3) | 0.36 |
| Positive family history, n (%) | 25 (8.3) | 15 (5.0) | 10 (3.3) | 0.59 |
| Known CAD, n (%) | 117 (38.7) | 51 (16.9) | 66 (21.9) | <0.001 |
| Previous MI, n (%) | 54 (18.9) | 15 (5.0) | 42 (13.9) | <0.001 |
| Previous PCI/CABG, n (%) | 82 (27.2) | 34 (11.3) | 48 (15.9) | <0.001 |
| Chronic pain, n (%) | 90 (30.1) | 51 (17.1) | 39 (13.0) | 0.27 |
| Depression, n (%) | 19 (6.5) | 11 (3.8) | 8 (2.7) | 0.49 |
| CRP (mg/L), mean ± SD | 24.6 ± 43.5 | 27.3 ± 51.6 | 26.3 ± 44.4 | 0.89 |
| WCB count (10*/µ/L), mean ± SD | 7.8 ± 3.3 | 7.8 ± 2.7 | 7.8 ± 3.3 | 0.94 |
| NT proBNP (ƞg/L), mean ± SD | 3604 ± 13,345 | 612 ± 946 | 6956 ± 19,045 | 0.08 |
| Stepwise Logistic Regression Model for Abnormal Myocardial Function/Perfusion in Total Cohort (n = 302) | |||
|---|---|---|---|
| Independent Variables | OR | OR (95% CI) | p-Value |
| Model 1 Previous MI | 6.50 | 3.11–13.58 | <0.001 |
| Model 2 Focal myocardial 18F-FDG uptake Previous MI | 4.72 6.37 | 1.59–14.01 3.02–13.44 | 0.005 <0.001 |
| Model 3 Male sex Focal myocardial 18F-FDG uptake Previous MI | 2.15 5.32 6.27 | 1.13–4.08 1.73–16.34 2.94–13.38 | 0.020 0.003 <0.001 |
| A. Stepwise Logistic Regression Model for Reversible Perfusion Defect in Total Cohort (n = 302) * | |||
|---|---|---|---|
| Independent Variables | OR | OR (95% CI) | p-Value |
| Model 1 Focal myocardial 18F-FDG uptake | 4.17 | 1.53–11.4 | 0.005 |
| B. Stepwise logistic regression model for irreversible perfusion defect in total cohort (n = 302) * | |||
| Independent variables | OR | OR (95% CI) | p-value |
| Model 1 Focal myocardial 18F-FDG uptake | 3.78 | 1.47–9.69 | 0.006 |
| C. Stepwise logistic regression model for LVEF <50% in total cohort (n = 302) * | |||
| Independent variables | OR | OR (95% CI) | p-value |
| Model 1 No myocardial 18F-FDG uptake | 0.36 | 0.19–0.67 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haider, A.; Bengs, S.; Schade, K.; Wijnen, W.J.; Portmann, A.; Etter, D.; Fröhlich, S.; Warnock, G.I.; Treyer, V.; Burger, I.A.; et al. Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT. J. Clin. Med. 2020, 9, 2279. https://doi.org/10.3390/jcm9072279
Haider A, Bengs S, Schade K, Wijnen WJ, Portmann A, Etter D, Fröhlich S, Warnock GI, Treyer V, Burger IA, et al. Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT. Journal of Clinical Medicine. 2020; 9(7):2279. https://doi.org/10.3390/jcm9072279
Chicago/Turabian StyleHaider, Ahmed, Susan Bengs, Katharina Schade, Winandus J. Wijnen, Angela Portmann, Dominik Etter, Sandro Fröhlich, Geoffrey I. Warnock, Valerie Treyer, Irene A. Burger, and et al. 2020. "Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT" Journal of Clinical Medicine 9, no. 7: 2279. https://doi.org/10.3390/jcm9072279
APA StyleHaider, A., Bengs, S., Schade, K., Wijnen, W. J., Portmann, A., Etter, D., Fröhlich, S., Warnock, G. I., Treyer, V., Burger, I. A., Fiechter, M., Kudura, K., Fuchs, T. A., Pazhenkottil, A. P., Buechel, R. R., Kaufmann, P. A., Meisel, A., Stolzmann, P., & Gebhard, C. (2020). Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT. Journal of Clinical Medicine, 9(7), 2279. https://doi.org/10.3390/jcm9072279