The Role of Health Preconditions on COVID-19 Deaths in Portugal: Evidence from Surveillance Data of the First 20293 Infection Cases

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collected
2.3. General Characteristics and Outcome
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Infected Individuals
3.2. Mortality Among the Infected
3.3. Association Between Characteristics and Lethality
3.4. Other Associations with Health Precondition
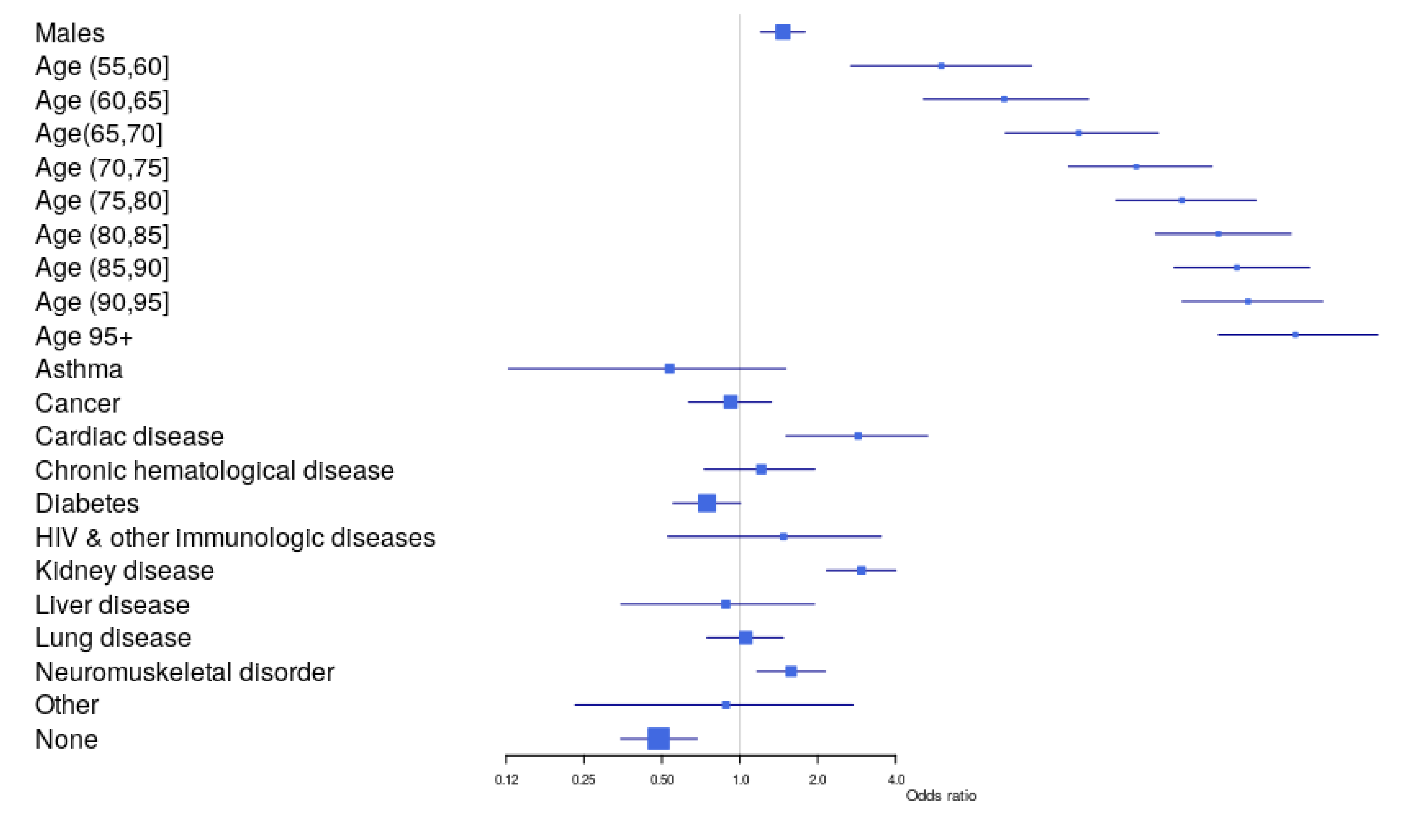
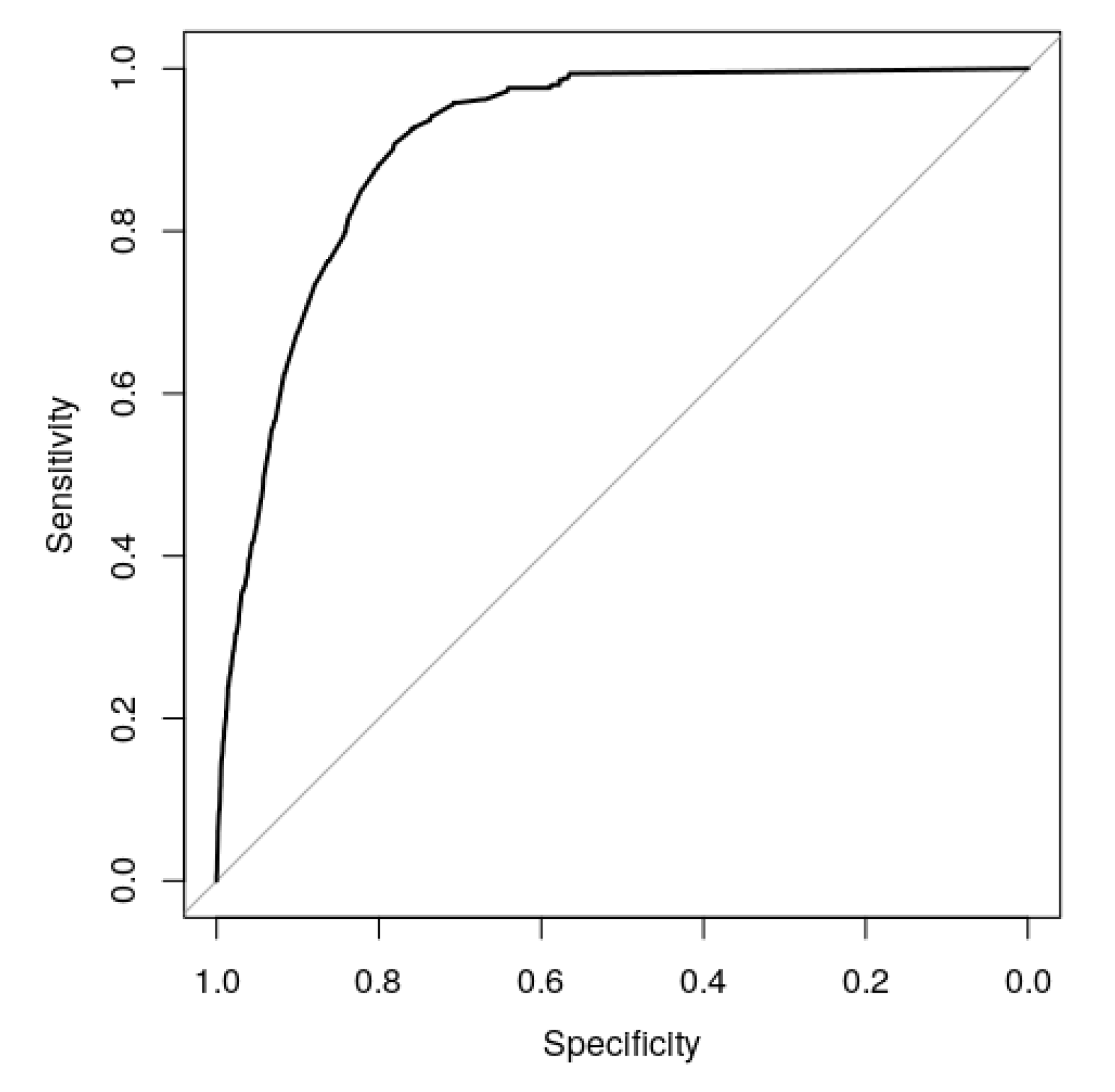
3.5. Factors Associated with Lethality
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.; Liang, W.; Zhao, Y.; Liang, H.; Chen, Z.; Li, Y.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with Covid-19 in China: A Nationwide Analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, A.; Caul, S. Deaths involving COVID-19, England and Wales: Deaths occurring in March 2020. Office for National Statistics. 2020; pp. 1–18. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19englandandwales/deathsoccurringinmarch2020 (accessed on 10 May 2020).
- Shi, Q.; Zhao, K.; Yu, J.; Feng, J.; Zhao, K.; Zhang, X.; Chen, X.; Hu, P.; Hong, Y.; Li, M.; et al. Clinical Characteristics of 101 Non-Survivors Hospitalized with COVID-19—A Single Center, Retrospective Study. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. J. Am. Med. Assoc. 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, R.H.; Liang, L.R.; Yang, C.Q.; Wang, W.; Cao, T.Z.; Li, M.; Guo, G.Y.; Du, J.; Zheng, C.L.; Zhu, Q.; et al. Predictors of Mortality for Patients with COVID-19 Pneumonia Caused by SARS-CoV-2: A Prospective Cohort Study. Eur. Respir. J. 2020, 55, 2000525. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Mattiuzzi, C.; Sanchis-Gomar, F.; Henry, B.M. Clinical and demographic characteristics of patients dying from COVID-19 in Italy versus China. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Direcção Geral da Saúde. COVID-19: Disponibilização de Dados. 2020. Available online: https://covid19.min-saude.pt/disponibilizacao-de-dados/ (accessed on 9 April 2020).
- Direcção Geral da Saúde. COVID-19: FASE DE MITIGAÇÃO: Abordagem do Doente com Suspeita ou Infeção por SARS-CoV-2. Norma 004/2020. 2020. Available online: https://www.dgs.pt/directrizes-da-dgs/normas-e-circulares-normativas/norma-n-0042020-de-23032020-pdf.aspx (accessed on 6 May 2020).
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel. Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Nogueira, P.J.; Nobre, M.D.A.; Nicola, P.J.; Furtado, C.; Vaz Carneiro, A. Excess Mortality Estimation During the COVID-19 Pandemic: Preliminary Data from Portugal. Acta Med. Port. 2020, 33, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, S0163–4453, 30234–30236. [Google Scholar]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Bertakis, K.D.; Azari, R.; Helms, L.J.; Callahan, E.J.; Robbins, J.A. Gender Differences in the Utilization of Health Care Services. J. Fam. Pract. 2000, 49, 147–152. [Google Scholar]
- Suen, L.K.P.; So, Z.Y.Y.; Yeung, S.K.W.; Lo, K.Y.K.; Lam, S.C. Epidemiological investigation on hand hygiene knowledge and behaviour: A cross-sectional study on gender disparity. BMC Public. Health 2019, 19, 401. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Bencivenga, L.; Rengo, G.; Varricchi, G. Elderly at time of COronaVIrus disease 2019 (COVID-19): Possible role of immunosenescence and malnutrition. Geroscience 2020, 1–4. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, X.; Deng, M.; Liu, P.; Li, F.; Xie, N.; Pang, Y.; Zhang, X.; Luo, W.; Peng, Y.; et al. Epidemiology of COVID-19 in older persons, Wuhan, China. Age Ageing 2020, afaa145. [Google Scholar] [CrossRef]
- Rivera-Izquierdo, M.; Del Carmen Valero-Ubierna, M.; R-delAmo, J.L.; Fernández-García, M.Á.; Martínez-Diz, S.; Tahery-Mahmoud, A.; Rodríguez-Camacho, M.; Gámiz-Molina, A.B.; Barba-Gyengo, N.; Gámez-Baeza, P.; et al. Sociodemographic, clinical and laboratory factors on admission associated with COVID-19 mortality in hospitalized patients: A retrospective observational study. PLoS ONE 2020, 15, e0235107. [Google Scholar] [CrossRef]
- Bravi, F.; Flacco, M.E.; Carradori, T.; Volta, C.A.; Cosenza, G.; De Togni, A.; Martellucci, C.A.; Parruti, G.; Mantovani, L.; Manzoli, L. Predictors of severe or lethal COVID-19, including Angiotensin Converting Enzyme inhibitors and Angiotensin II Receptor Blockers, in a sample of infected Italian citizens. PLoS ONE 2020, 15, e0235248. [Google Scholar] [CrossRef]
- Wang, J.; Zhu, X.; Xu, Z.; Yang, G.; Mao, G.; Jia, Y.; Xie, Z.; Wang, J.; Ao, W. Clinical and CT findings of COVID-19: Differences among three age groups. BMC Infect. Dis. 2020, 20, 434. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Gao, H.Y.; Feng, Z.Y.; Wu, Q.J. A Retrospective Analysis of the Clinical and Epidemiological Characteristics of COVID-19 Patients in Henan Provincial People’s Hospital, Zhengzhou, China. Front. Med. (Lausanne) 2020, 7, 286. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, G.; Grassi, G.; Borghi, C.; Ferri, C.; Salvetti, M.; Volpe, M. Age and Multimorbidity Predict Death Among COVID-19 Patients: Results of the SARS-RAS Study of the Italian Society of Hypertension. Hypertension 2020, 76, 366–372. [Google Scholar] [CrossRef]
- Esteve, A.; Permanyer, I.; Boertien, D.; Vaupel, J.W. National age and coresidence patterns shape COVID-19 vulnerability. Proc. Natl. Acad. Sci. USA 2020, 202008764. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, L.; Yang, H.; Duan, G.; Wang, Y. Acute kidney injury is associated with the mortality of coronavirus disease 2019. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Kellum, J.A. Determinants of blood pH in health and disease. Crit. Care. 2000, 4, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Rojas, M.A.; Vega-Veja, O.; Bobadilla, N.A. Is the kidney a target of SARS-CoV-2? Am. J. Physiol. Renal. Physiol. 2020, 318, F1454–F1462. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Pranata, R.; Huang, I.; Lim, M.A.; Wahjoepramono, P.E.J.; July, J. Impact of Cerebrovascular and Cardiovascular Diseases on Mortality and Severity of COVID-19—Systematic Review, Meta-analysis, and Meta-regression. J. Stroke. Cerebrovasc. Dis. 2020. [Google Scholar] [CrossRef]
- Ceriello, A.; Standl, E.; Catrinoiu, D.; Itzhak, B.; Lalic, N.M.; Rahelic, D.; Schnell, O.; Škrha, J.; Valensi, P. Issues of Cardiovascular Risk Management in People With Diabetes in the COVID-19 Era. Diabetes Care 2020. [Google Scholar] [CrossRef]
- Dehghani, P.; Davidson, L.J.; Grines, C.L.; Nayak, K.; Saw, J.; Kaul, P.; Bagai, A.; Garberich, R.; Schmidt, C.; SM, H.Q.L.M.; et al. North American COVID-19 ST-segment elevation myocardial infarction (NACMI) registry: Rationale, design, and implications. Am. Heart J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Moderato, L.; Monello, A.; Lazzeroni, D.; Binno, S.; Giacalone, R.; Ferraro, S.; Piepoli, M.F.; Villani, G.Q. Takotsubo syndrome during SARS-CoV-2 pneumonia: A possible cardiovascular complication. G Ital. Cardiol. (Rome) 2020, 21, 417–420. [Google Scholar] [CrossRef]
- Lorente-Ros, A.; Monteagudo Ruiz, J.M.; Rincón, L.M.; Pérez, R.O.; Rivas, S.; Martínez-Moya, R.; Sanromán, M.A.; Manzano, L.; Alonso, G.L.; Ibáñez, B.; et al. Myocardial injury determination improves risk stratification and predicts mortality in COVID-19 patients. Cardiol. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. The Heart in COVID19: Primary Target or Secondary Bystander? JACC Basic Transl. Sci. 2020, 5, 537–542. [Google Scholar] [CrossRef]
- Tomasoni, D.; Italia, L.; Adamo, M.; Inciardi, R.M.; Lombardi, C.M.; Solomon, S.D.; Metra, M. COVID 19 and heart failure: From infection to inflammation and angiotensin II stimulation. Searching for evidence from a new disease. Eur. J. Heart. Fail. 2020. [Google Scholar] [CrossRef]
- Guidon, A.C.; Amato, A.A. COVID-19 and neuromuscular disorders. Neurology 2020, 94, 959–969. [Google Scholar] [CrossRef] [Green Version]
- Solé, G.; Salort-Campana, E.; Pereon, Y.; Stojkovic, T.; Wahbi, K.; Cintas, P.; Adams, D.; Laforet, P.; Tiffreau, V.; Desguerre, I.; et al. Guidance for the care of neuromuscular patients during the COVID-19 pandemic outbreak from the French Rare Health Care for Neuromuscular Diseases Network. Rev. Neurol. (Paris) 2020, 176, 507–515. [Google Scholar] [CrossRef]
- Zhu, L.; She, Z.G.; Cheng, X.; Qin, J.J.; Zhang, X.J.; Cai, J.; Lei, F.; Wang, H.; Xie, J.; Wang, W.; et al. Association of Blood Glucose Control and Outcomes in Patients with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab. 2020, 31, 1068–1077. [Google Scholar] [CrossRef]
- Alves, A.C.; Rato, Q.; Bourbon, M. Diabetes na população portuguesa: Uma análise do estudo e_COR. Bol. Epidemiológico Obs. 2016, 15, 3–5. [Google Scholar]
- Direção Geral da Saúde. Novo Coronavirus COVID-19, Relatório de situação n° 116-26/06/2020. 2020. Available online: https://covid19.min-saude.pt/wp-content/uploads/2020/06/116_DGS_boletim_20200626-1.pdf (accessed on 26 June 2020).



{kind=link}
{kind=link}
| Variable | n (%) | Deaths (%) | p-Value * | |
|---|---|---|---|---|
| Outcome | Recovered | 1244 (6.1%) | ||
| Died COVID-19 | 502 (2.5%) | |||
| Ongoing Treatment | 18,524 (91.3%) | |||
| Unknown | 23 (0.1%) | |||
| Sex | Female | 11,903 (58.7%) | 253 (2.13%) | <0.001 |
| Male | 8390 (41.3%) | 249 (2.97%) | ||
| Age | (0,18) | 711 (2.5%) | 0 (0%) | <0.001 |
| (19,35) | 4153 (20.5%) | 0 (0%) | ||
| (36,45) | 3259 (16.1%) | 3 (0.09%) | ||
| (46,55) | 3653 (18.1%) | 10 (0.27%) | ||
| (56,65) | 3046 (15.1%) | 30 (0.98%) | ||
| (66,75) | 1926 (9.5%) | 78 (4.05%) | ||
| (76,85) | 1864 (9.2%) | 177 (9.50%) | ||
| 86+ | 1618 (8.0%) | 204 (12.61%) | ||
| Region | North | 12211 (60.2%) | 319 (2.61%) | <0.001 |
| Algarve | 472 (2.3%) | 6 (1.27%) | ||
| Center | 2817 (13.9%) | 97 (3.44%) | ||
| Lisbon Metropolitan Area | 4264 (21.0%) | 74 (1.74%) | ||
| Alentejo | 391 (1.9%) | 6 (1.53%) | ||
| Madeira | 48 (0.2%) | 0 (0%) | ||
| Azores | 90 (0.4%) | 0 (0%) | ||
| Hospitalization | No | 15,697 (77.4%) | 126 (0.80%) | <0.001 |
| Unknown | 1623 (8.0%) | 46 (2.83%) | ||
| Yes | 2973 (14.7%) | 330 (11.10%) | ||
| Intensive Care | No | 15,697 (77.4%) | 126 (0.80%) | <0.001 |
| Unknown | 4335 (21.4%) | 475 (10.96%) | ||
| Yes | 261 (1.3%) | 27 (10.34%) | ||
| Respiratory Support | No | 1315 (6.5%) | 156 (11.86%) | <0.001 |
| Oxygen | 59 (0.3%) | 0 (0%) | ||
| Ventilator | 26 (0.1%) | 0 (0%) | ||
| Unknown | 18,893 (93.1%) | 346 (1.83%) | ||
| Precondition | ||||
| Asthma | Presence | 277 (1.4%) | 3 (1.08%) | 0.192 |
| Absence | 20,016 (98.7%) | 499 (2.50%) | ||
| Cancer | Presence | 611 (3.0%) | 47 (7.69%) | <0.001 |
| Absence | 19,682 (97.0%) | 455 (2.3%) | ||
| Cardiac Disease | Presence | 54 (0.3%) | 19 (35.2%) | <0.001 |
| Absence | 20,239 (99.7%) | 483 (2.4%) | ||
| Hematological Disorder | Presence | 220 (1.1%) | 29 (13.2%) | <0.001 |
| Absence | 20,073 (98.9%) | 473 (2.4%) | ||
| Diabetes | Presence | 1145 (5.6%) | 83 (7.3%) | <0.001 |
| Absence | 19,148 (94.4%) | 419 (2.2%) | ||
| HIV/other Immune Deficiency | Presence | 107 (0.5%) | 6 (5.6%) | 0.075 |
| Absence | 20,186 (99.5%) | 496 (2.5%) | ||
| Kidney Disorder | Presence | 401 (2.0%) | 98 (24.4%) | <0.001 |
| Absence | 19,892 (98.0%) | 404 (2.0%) | ||
| Liver Disorder | Presence | 107 (0.5%) | 7 (6.5%) | 0.016 |
| Absence | 20,186 (99.5%) | 495 (2.5%) | ||
| Lung Disorder | Presence | 688 (3.4%) | 60 (8.7%) | <0.001 |
| Absence | 19,605 (96.6%) | 442 (2.3%) | ||
| Neuromuscular Disorder | Presence | 795 (3.9%) | 123 (15.5%) | <0.001 |
| Absence | 19,498 (96.1%) | 379 (1.9%) | ||
| Other Condition | Presence | 76 (0.4%) | 4 (5.3%) | 0.231 |
| Absence | 20,217 (99.6%) | 498 (2.5%) | ||
| None | No Precondition | 16,927 (83.4%) | 212 (1.3%) | <0.001 |
| (Absence of Precondition) | At least one Precondition | 3366 (16.6%) | 290 (8.6%) |
| Variables | Sex Odds Ratio (OR) (95% CI) 1 | p-Value | Hospitalization Odds Ratio (OR) (95% CI) 2 | p-Value | Intensive Care Odds Ratio (OR) (95% CI) 3 | p-Value |
|---|---|---|---|---|---|---|
| Asthma | 0.71 (0.55;0.92) | p = 0.008 | 0.59 (0.38;0.87) | p = 0.011 | 1.13 (0.30;2.95) | p = 0.784 |
| Cancer | 1.61 (1.37;1.90) | p < 0.001 | 5.85 (4.94;6.92) | p < 0.001 | 3.04 (1.85;4.75) | p < 0.001 |
| Cardiac Disease | 1.65 (0.93;2.94) | p = 0.072 | 87.66 (32.19;361) | p < 0.001 | 18.09 (8.02;37.0) | p < 0.001 |
| Hematological | 1.23 (0.93;1.62) | p = 0.130 | 10.15 (7.61;13.64) | p < 0.001 | 2.96 (1.25;6.02) | p = 0.008 |
| Diabetes | 1.51 (1.33;1.70) | p < 0.001 | 5.40 (4.75;6.14) | p < 0.001 | 4.42 (3.18;6.04) | p < 0.001 |
| HIV/other imune deficiency | 1.96 (1.31;2.95) | p = 0.009 | 4.10 (2.74;6.10) | p < 0.001 | 5.49 (2.13;11.9) | p < 0.001 |
| Kidney Disorder | 2.02 (1.64;2.48) | p < 0.001 | 14.33 (11.48;18.01) | p < 0.001 | 8.02 (5.34;11.74) | p < 0.001 |
| Liver Disorder | 3.50 (2.27;5.51) | p < 0.001 | 9.07 (6.09;13.68) | p < 0.001 | 3.82 (1.20;9.31) | p = 0.012 |
| Lung Disorder | 1.51 (1.29;1.76) | p < 0.001 | 4.85 (4.12;5.69) | p < 0.001 | 4.92 (3.34;7.06) | p < 0.001 |
| Neuromuscular | 1.01 (0.87;1.17) | p = 0.883 | 11.48 (9.82;13.45) | p < 0.001 | 2.65 (1.67;4.04) | p < 0.001 |
| Other Condition | 1.03 (0.63;1.67) | p = 0.907 | 5.18 (3.24;8.28) | p < 0.001 | 2.08 (0.25;7.87) | p = 0.256 |
| None | 0.77 (0.71;0.82) | p < 0.001 | 0.13 (0.12;0.14) | p < 0.001 | 0.17 (0.13;0.21) | p < 0.001 |
| Variables | Odds Ratio (OR) Crude Values (95% CI) ^ | p-Value | Odds Ratio (OR) Adjusted Values (95% CI) 1 | p-Value | Odds Ratio (OR) Adjusted Values (95% CI) 2 | p-Value | Odds Ratio (OR) Adjusted Values (95% CI) 3 | p-Value |
|---|---|---|---|---|---|---|---|---|
| Sex | ||||||||
| Female | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) | |||||
| Male | 1.41 (1.17;1.69) | p < 0.001 | 1.99 (1.49;2.65) | <0.001 | 1.47 (1.20;1.79) | <0.001 | ||
| Age (0–55) years | 1.0 (reference) | 1.0 (reference) | <0.001 | 1.0 (reference) | ||||
| Age (56–60) years | 6.50 (2.92;14.36) | p < 0.001 | 13.20 (3.23;64.41) | <0.001 | 6.01 (2.68;13.40) | <0.001 | ||
| Age (61–65) years | 12.25 (6.02;25.59) | p < 0.001 | 29.57 (8.81;133.44) | <0.001 | 10.50 (5.12;22.17) | <0.001 | ||
| Age (66–70) years | 26.53 (13.98;53.09) | p < 0.001 | 53.71 (16.72;237.98) | <0.001 | 20.36 (10.59;41.31) | <0.001 | ||
| Age (71–75) years | 51.22 (28.60;98.67) | p < 0.001 | 115.37 (39.16;492.19) | <0.001 | 34.01 (18.64;66.69) | <0.001 | ||
| Age (76–80) years | 80.27 (45.75;152.50) | p < 0.001 | 187.76 (65.80;789.55) | <0.001 | 50.91 (28.46;98.50) | <0.001 | ||
| Age (81–85) years | 108.56 (63.20;203.27) | p < 0.001 | 281.18 (102.16;1162.9) | <0.001 | 70.65 (40.35;134.69) | <0.001 | ||
| Age (86–90) years | 125.87 (73.28;235.68) | p < 0.001 | 357.87 (130.42;1478.17) | <0.001 | 83.23 (47.51;58.70) | <0.001 | ||
| Age (91–95) years | 125.67 (71.30;239.55) | p < 0.001 | 407.45 (145.58;1698.79) | <0.001 | 91.83 (51.10;178.31) | <0.001 | ||
| Age (96–104) years | 183.30 (94.32;374.16) | p < 0.001 | 640.17 (203.95;2818.60) | <0.001 | 140.17 (70.69;291.53) | <0.001 | ||
| Asthma | 0.03 (0.02;0.03) | p = 0.145 | 0.80 (0.19;2.21) | 0.740 | 0.54 (0.13;1.51) | 0.305 | ||
| Cancer | 3.52 (2.55;4.76) | p < 0.001 | 1.48 (1.06;2.04) | 0.018 | 0.92 (0.64;1.32) | 0.666 | ||
| Cardiac Disease | 22.20 (12.38;38.65) | p < 0.001 | 6.40 (3.48;11.51) | <0.001 | 2.86 (1.51;5.32) | <0.001 | ||
| Chronic Hematological Disorder | 6.29 (4.13;9.24) | p < 0.001 | 2.33 (1.50;3.51) | <0.001 | 1.21 (0.73;1.95) | 0.447 | ||
| Diabetes | 3.49 (2.72;4.43) | p < 0.001 | 1.39 (1.08;1.79) | 0.010 | 0.75 (0.55;1.01) | 0.057 | ||
| HIV/Other Imune Deficiency | 2.36 (0.92;4.95) | p = 0.042 | 3.12 (1.15;7.19) | 0.014 | 1.48 (0.53;3.52) | 0.414 | ||
| Kidney Disorder | 15.60 (12.13;19.93) | p < 0.001 | 4.97 (3.80;6.46) | <0.001 | 2.95 (2.16;4.00) | <0.001 | ||
| Liver Disorder | 2.79 (1.17;5.60) | p = 0.010 | 1.77 (0.72;3.76) | 0.168 | 0.88 (0.35;1.94) | 0.773 | ||
| Lung Disorder | 4.14 (3.10;5.44) | p < 0.001 | 1.79 (1.32;2.39) | <0.001 | 1.05 (0.75;1.47) | 0.761 | ||
| Neuromuscular Disorder | 9.23 (7.41;11.44) | p < 0.001 | 2.67 (2.11;3.34) | <0.001 | 1.58 (1.17;2.14) | 0.003 | ||
| None | 0.14 (0.11;0.16) | p < 0.001 | 0.34 (0.28;0.41) | <0.001 | 0.49 (0.35;0.68) | <0.001 | ||
| Other condition | 2.20 (0.67;5.33) | p = 0.126 | 1.31 (0.38;3.43) | 0.625 | 0.88 (0.23;2.74) | 0.341 |
| Variables | Odds Ratio (OR) Adjusted Values (95% CI) * | p-Value | Odds Ratio (OR) Adjusted Values (95% CI) ** | p-Value |
|---|---|---|---|---|
| Sex | ||||
| Female | 1.0 (reference) | 1.0 (reference) | ||
| Male | 1.59 (1.24;2.06) | <0.001 | 1.05 (0.81;1.35) | =0.713 |
| Age (0–55) years | 1.0 (reference) | 1.0 (reference) | ||
| Age (56–60) years | 8.29 (3.41;20.77) | <0.001 | 2.94 (1.13;7.56) | =0.024 |
| Age (61–65) years | 12.26 (5.40;29.52) | <0.001 | 2.53 (1.01;6.37) | 0.045 |
| Age (66–70) years | 21.76 (10.05;51.01) | <0.001 | 3.96 (1.78;9.33) | <0.001 |
| Age (71–75) years | 37.94 (18.68;85.59) | <0.001 | 5.62 (2.76;12.53) | <0.001 |
| Age (76–80) years | 67.09 (33.77;149.30) | <0.001 | 8.37 (4.22;18.34) | <0.001 |
| Age (81–85) years | 92.48 (47.10;204.31) | <0.001 | 12.82 (6.65;27.55) | <0.001 |
| Age (86–90) years | 141.25 (71.63;313.08) | <0.001 | 14.22 (7.33;30.72) | <0.001 |
| Age (91–95) years | 174.32 (83.94;400.32) | <0.001 | 14.77 (7.25;33.00) | <0.001 |
| Age (96–104) years | 347.63 (140.08;913.73) | <0.001 | 18.32 (7.37;46.94) | <0.001 |
| Asthma | 1.01 (0.23;3.09) | =0.994 | 0.38 (0.02;2.00) | =0.363 |
| Cancer | 1.02 (0.64;1.59) | =0.939 | 0.98 (0.64;1.48) | =0.930 |
| Cardiac Disease | 2.09 (0.99;4.25) | =0.046 | 2.14 (1.09;4.09) | =0.024 |
| Chronic Hematological Disorder | 0.96 (0.49;1.79) | =0.907 | 1.53 (0.89;2.56) | =0.118 |
| Diabetes | 0.63 (0.42;0.94) | =0.027 | 0.69 (0.49;0.98) | =0.040 |
| HIV/other imune deficiency | 2.17 (0.74;5.59) | =0.129 | 1.27 (0.40;3.32) | =0.650 |
| Kidney Disorder | 1.98 (1.35;2.91) | <0.001 | 2.84 (1.99;4.04) | <0.001 |
| Liver Disorder | 1.79 (0.49;5.18) | =0.324 | 0.88 (0.34;1.98) | =0.779 |
| Lung Disorder | 1.04 (0.69;1.57) | =0.844 | 0.97 (0.64;1.44) | =0.872 |
| Neuromuscular Disorder | 1.44 (0.98;2.11) | =0.065 | 1.39 (0.98;1.97) | =0.066 |
| None | 0.59 (0.38;0.90) | =0.014 | 0.84 (0.55;1.27) | =0.394 |
| Other condition | 1.05 (0.14;5.00) | =0.960 | 0.57 (0.12;2.04) | =0.426 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nogueira, P.J.; de Araújo Nobre, M.; Costa, A.; Ribeiro, R.M.; Furtado, C.; Bacelar Nicolau, L.; Camarinha, C.; Luís, M.; Abrantes, R.; Vaz Carneiro, A. The Role of Health Preconditions on COVID-19 Deaths in Portugal: Evidence from Surveillance Data of the First 20293 Infection Cases. J. Clin. Med. 2020, 9, 2368. https://doi.org/10.3390/jcm9082368
Nogueira PJ, de Araújo Nobre M, Costa A, Ribeiro RM, Furtado C, Bacelar Nicolau L, Camarinha C, Luís M, Abrantes R, Vaz Carneiro A. The Role of Health Preconditions on COVID-19 Deaths in Portugal: Evidence from Surveillance Data of the First 20293 Infection Cases. Journal of Clinical Medicine. 2020; 9(8):2368. https://doi.org/10.3390/jcm9082368
Chicago/Turabian StyleNogueira, Paulo Jorge, Miguel de Araújo Nobre, Andreia Costa, Ruy M. Ribeiro, Cristina Furtado, Leonor Bacelar Nicolau, Catarina Camarinha, Márcia Luís, Ricardo Abrantes, and António Vaz Carneiro. 2020. "The Role of Health Preconditions on COVID-19 Deaths in Portugal: Evidence from Surveillance Data of the First 20293 Infection Cases" Journal of Clinical Medicine 9, no. 8: 2368. https://doi.org/10.3390/jcm9082368
APA StyleNogueira, P. J., de Araújo Nobre, M., Costa, A., Ribeiro, R. M., Furtado, C., Bacelar Nicolau, L., Camarinha, C., Luís, M., Abrantes, R., & Vaz Carneiro, A. (2020). The Role of Health Preconditions on COVID-19 Deaths in Portugal: Evidence from Surveillance Data of the First 20293 Infection Cases. Journal of Clinical Medicine, 9(8), 2368. https://doi.org/10.3390/jcm9082368