Screening Services in a Community Pharmacy in Poznan (Poland) to Increase Early Detection of Hypertension

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Limitation of the Study
Author Contributions
Funding
Conflicts of Interest
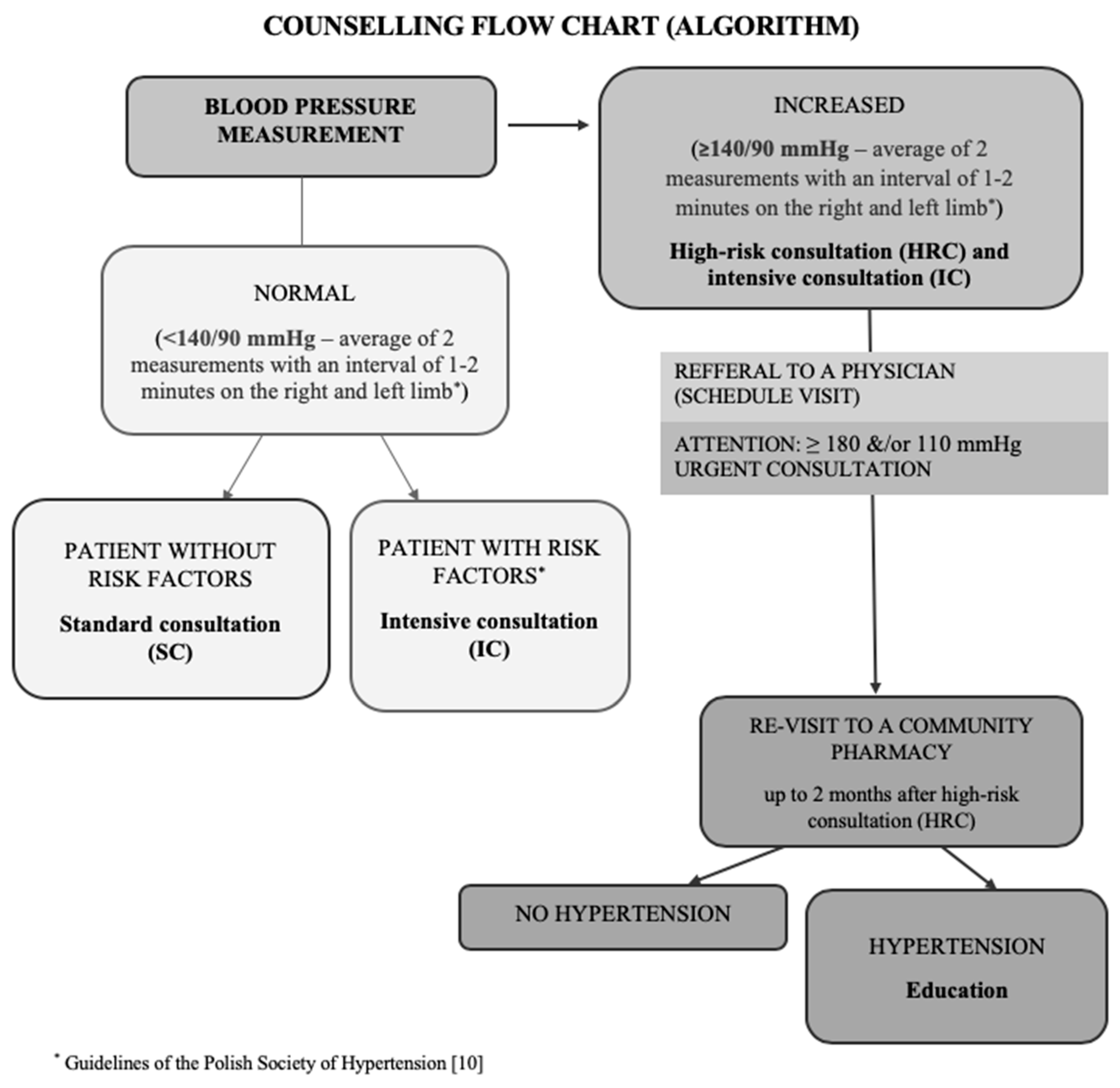
Appendix A. Flow Chart for Blood Pressure Screening and Counseling Performed in a Community Pharmacy

References
- World Health Organization. A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis. 2013. Available online: http://www.who.int/cardiovascular_diseases/publications/global_brief_hypertension/en/ (accessed on 15 March 2020).
- Niklas, A.; Flotynska, A.; Puchwalczak, A.; Polakowska, M.; Topormadry, R.; Polak, M.; Piotrowski, W.; Kwaśniewska, M.; Nadrowski, P.; Pająk, A.; et al. Prevalence, awareness, treatment and control of hypertension in the adult Polish population—Multi-center National Population Health Examination Surveys—WOBASZ studies. Arch. Med. Sci. 2018, 5, 951–961. [Google Scholar] [CrossRef]
- Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 2017, 389, 37–55. [CrossRef] [Green Version]
- Egan, B.M.; Kjeldsen, S.E.; Grassi, G.; Murray, E.; Guiseppe, M. The global burden of hypertension exceeds 1.4 billion people. J. Hypertens. 2019, 37, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Department of Analysis and Strategy. National Health Fund about Health: Hypertension; National Health Fund: Warsaw, Poland, 2019; pp. 4–8. [Google Scholar]
- Beaney, T.; Burrell, L.M.; Castillo, R.R.; Charchar, F.J.; Cro, S.; Damasceno, A.; Kruger, R.; Nilsson, P.M.; Prabhakaran, D.; Ramirez, A.J.; et al. May Measurement Month 2018: A pragmatic global screening campaign to raise awareness of blood pressure by the International Society of Hypertension. Eur. Heart J. 2019, 40, 2006–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rycombel, A.; Lomper, K.; Uchmanowicz, I. Adherence i compliance w leczeniu nadciśnienia tętniczego. Arter. Hypertens. 2014, 18, 151–158. [Google Scholar]
- Marfo, A.; Owusu-Daaku, F. Exploring the extended role of the community pharmacist in improving blood pressure control among hypertensive patients in a developing setting. J. Pharm. Policy Pract. 2017, 10, 39–61. [Google Scholar] [CrossRef] [Green Version]
- Omboni, S.; Caserini, M. Effectiveness of pharmacist’s intervention in the management of cardiovascular diseases. Open Heart 2018, 5, e000687. [Google Scholar] [CrossRef] [Green Version]
- Tykarski, A.; Filipiak, K.J.; Januszewicz, A.; Litwin, M.; Narkiewicz, K.; Prejbisz, A.; Ostalska-Nowicka, D.; Widecka, K.; Kostka-Jeziorny, K. Guidelines for the Management of Hypertension; National Health Fund: Warsaw, Poland, 2019; pp. 3–11. [Google Scholar]
- Obesity, High Blood Pressure, High Cholesterol, Alcohol and Tobacco: The World Health Organization’s Response. 2019. Available online: https://www.who.int/whr/media_centre/factsheet3/en/ (accessed on 15 March 2020).
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Dua, S.; Bhuker, M.; Sharma, P.; Dhall, M.; Kapoor, S. Body mass index relates to blood pressure among adults. N. Am. J. Med. Sci. 2014, 6, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Tesfaye, F.; Nawi, N.; Van Minh, H.; Byass, P.; Berhane, Y.; Bonita, R.; Wall, S. Association between body mass index and blood pressure across three populations in Africa and Asia. J. Hum. Hypertens. 2007, 21, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Bays, H.E.; Chapman, R.H.; Grandy, S. The relationship of body mass index to diabetes mellitus, hypertension, and dyslipidemia: Comparison of data from two national surveys. Int. J. Clin. Pract. 2007, 61, 737–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landi, F.; Calvani, R.; Picca, A.; Tosato, M.; Ortolani, E.; Sisto, A.; D’Angelo, E.; Serafini, E.; Desideri, G.; Fuga, M.T.; et al. Body mass index is strongly associated with hypertension: Results from the longevity check-up 7+ study. Nutrients 2018, 10, 1976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St-Onge, M.P.; Gallagher, D. Body composition changes with aging: The cause or the result of alterations in metabolic rate and macronutrient oxidation? Nutrition 2010, 26, 152–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St-Onge, M.P.; Gallagher, D.; Singh, S.; Shankar, R.; Singh, G.P. Prevalence and Associated Risk Factors of Hypertension: A Cross-Sectional Study in Urban Varanasi. Intern. J. Hypertens. 2017, 2017, 54918381. [Google Scholar]
- De Venecia, T.; Lu, M.; Figueredo, V.M. Hypertension in young adults. Postgrad. Med. 2016, 128, 201–207. [Google Scholar] [CrossRef]
- Csige, I.; Ujvarosy, D.; Szabo, Z.; Lorincz, I.; Paragh, G.; Harangi, M.; Somodi, S. The Impact of Obesity on the Cardiovascular System. J. Diabetes Res. 2018, 2018, 3407306. [Google Scholar] [CrossRef] [Green Version]
- Diaz, K.M.; Shimbo, D. Physical activity and the prevention of hypertension. Curr. Hypertens. Rep. 2013, 15, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Loria, C.M.; Liu, K.; Lewis, C.E.; Hulley, S.B.; Sidney, S.; Schreiner, P.J.; Williams, O.D.; Bild, D.E.; Detrano, R. Early adult risk factor levels and subsequent coronary artery calcification the cardia study. J. Am. Coll. Cardiol. 2007, 49, 2013–2020. [Google Scholar] [CrossRef] [Green Version]
- Waszyk-Nowaczyk, M.; Szukalska, B.; Guzenda, W.; Michalak, M. Implementation of professional pharmaceutical counselling scheme in community pharmacies in Poznan and Warsaw (Poland). Farmacia 2019, 67, 531–536. [Google Scholar] [CrossRef]
- Waszyk-Nowaczyk, M.; Skura, O.; Michalak, M.; Ratka, A. Opinions of pharmacists on community pharmacy-based health screenings for common chronic diseases. Acta Pol. Pharm. 2018, 75, 819–826. [Google Scholar]
- Dalton, K.; Byrne, S. Role of the pharmacist in reducing healthcare costs: Current insights. Integr. Pharm. Res. Pract. 2017, 6, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Examined Patients n (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Type of Consultation | SC Standard Consultation | IC Intensive Consultation | HRC High-Risk Consultation | Total | |||||
| Sex | Male | Female | Male | Female | Male | Female | Male | Female | Total |
| Total Respondents | 16 (13.6) | 57 (48.3) | 11 (9.3) | 14 (11.9) | 9 (7.6) | 11 (9.3) | 36 (30.5) | 82 (69.5) | 118 (100) |
| Age [years] n = 118 | |||||||||
| 19–29 | 4 (25.0) | 24 (42.1) | 1 (9.1) | 4 (28.7) | 1 (11.1) | 3 (27.3) | 6 (16.7) | 31 (37.8) | 37 (31.4) |
| 30–39 | 6 (37.5) | 21 (36.8) | 6 (54.5) | 1 (7.1) | 4 (44.5) | 3 (27.3) | 16 (44.5) | 25 (30.5) | 41 (34.7) |
| 40–49 | 3 (18.7) | 12 (21.1) | 3 (27.3) | 5 (35.7) | 2 (22.2) | 2 (18.1) | 8 (22.2) | 19 (23.1) | 27 (22.9) |
| 50–59 | 2 (12.5) | 0 (0.0) | 1 (9.1) | 3 (21.4) | 0 (0.0) | 0 (0.0) | 3 (8.3) | 3 (3.7) | 6 (5.1) |
| ≥60 | 1 (6.3) | 0 (0.0) | 0 (0.0) | 1 (7.1) | 2 (22.2) | 3 (27.3) | 3 (8.3) | 4 (4.9) | 7 (5.9) |
| Education n = 111 | |||||||||
| High school | 1 (6.7) | 1 (1.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (3.0) | 1 (1.3) | 2 (1.8) |
| Vocational | 0 (0.0) | 0 (0.0) | 1 (9.1) | 2 (14.3) | 1 (12.5) | 0 (0.0) | 2 (5.9) | 2 (2.6) | 4 (3.6) |
| Secondary | 5 (33.3) | 11 (21.2) | 1 (9.1) | 7 (50.0) | 2 (25.0) | 5 (45.5) | 8 (23.5) | 23 (29.9) | 31 (27.9) |
| Higher | 9 (60.0) | 40 (76.9) | 9 (81.8) | 5 (35.7) | 5 (62.5) | 6 (54.5) | 23 (67.6) | 51 (66.2) | 74 (66.7) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waszyk-Nowaczyk, M.; Guzenda, W.; Plewka, B.; Michalak, M.; Cerbin-Koczorowska, M.; Stryczyński, Ł.; Byliniak, M.; Ratka, A. Screening Services in a Community Pharmacy in Poznan (Poland) to Increase Early Detection of Hypertension. J. Clin. Med. 2020, 9, 2572. https://doi.org/10.3390/jcm9082572
Waszyk-Nowaczyk M, Guzenda W, Plewka B, Michalak M, Cerbin-Koczorowska M, Stryczyński Ł, Byliniak M, Ratka A. Screening Services in a Community Pharmacy in Poznan (Poland) to Increase Early Detection of Hypertension. Journal of Clinical Medicine. 2020; 9(8):2572. https://doi.org/10.3390/jcm9082572
Chicago/Turabian StyleWaszyk-Nowaczyk, Magdalena, Weronika Guzenda, Beata Plewka, Michał Michalak, Magdalena Cerbin-Koczorowska, Łukasz Stryczyński, Michał Byliniak, and Anna Ratka. 2020. "Screening Services in a Community Pharmacy in Poznan (Poland) to Increase Early Detection of Hypertension" Journal of Clinical Medicine 9, no. 8: 2572. https://doi.org/10.3390/jcm9082572
APA StyleWaszyk-Nowaczyk, M., Guzenda, W., Plewka, B., Michalak, M., Cerbin-Koczorowska, M., Stryczyński, Ł., Byliniak, M., & Ratka, A. (2020). Screening Services in a Community Pharmacy in Poznan (Poland) to Increase Early Detection of Hypertension. Journal of Clinical Medicine, 9(8), 2572. https://doi.org/10.3390/jcm9082572