Immediate and Short-Term Effects of Upper Cervical High-Velocity, Low-Amplitude Manipulation on Standing Postural Control and Cervical Mobility in Chronic Nonspecific Neck Pain: A Randomized Controlled Trial


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Size Calculation
2.3. Participants and Recruitment
2.4. Masking and Allocation
2.5. Outcome Measures
2.5.1. Cervical Flexion-Rotation Test (CFRT)
2.5.2. Static Postural Stability Assessment
2.6. Interventions
2.6.1. Experimental Group
2.6.2. Control Group
2.7. Statistical Analysis
3. Results
3.1. Descriptive Analysis
3.2. Inferential Analysis
3.2.1. Inter-Group Comparisons
3.2.2. Intra-Group Comparisons
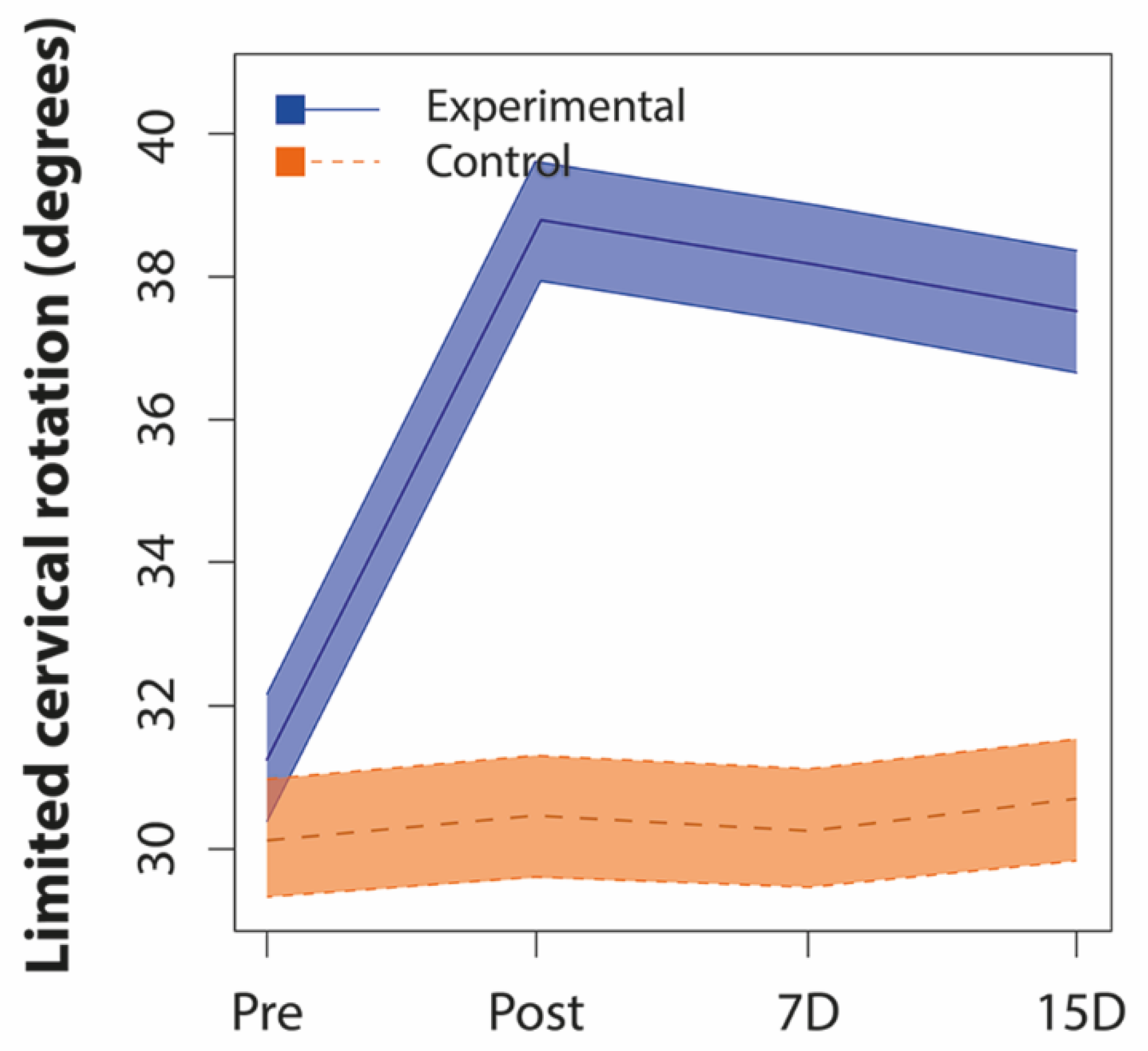
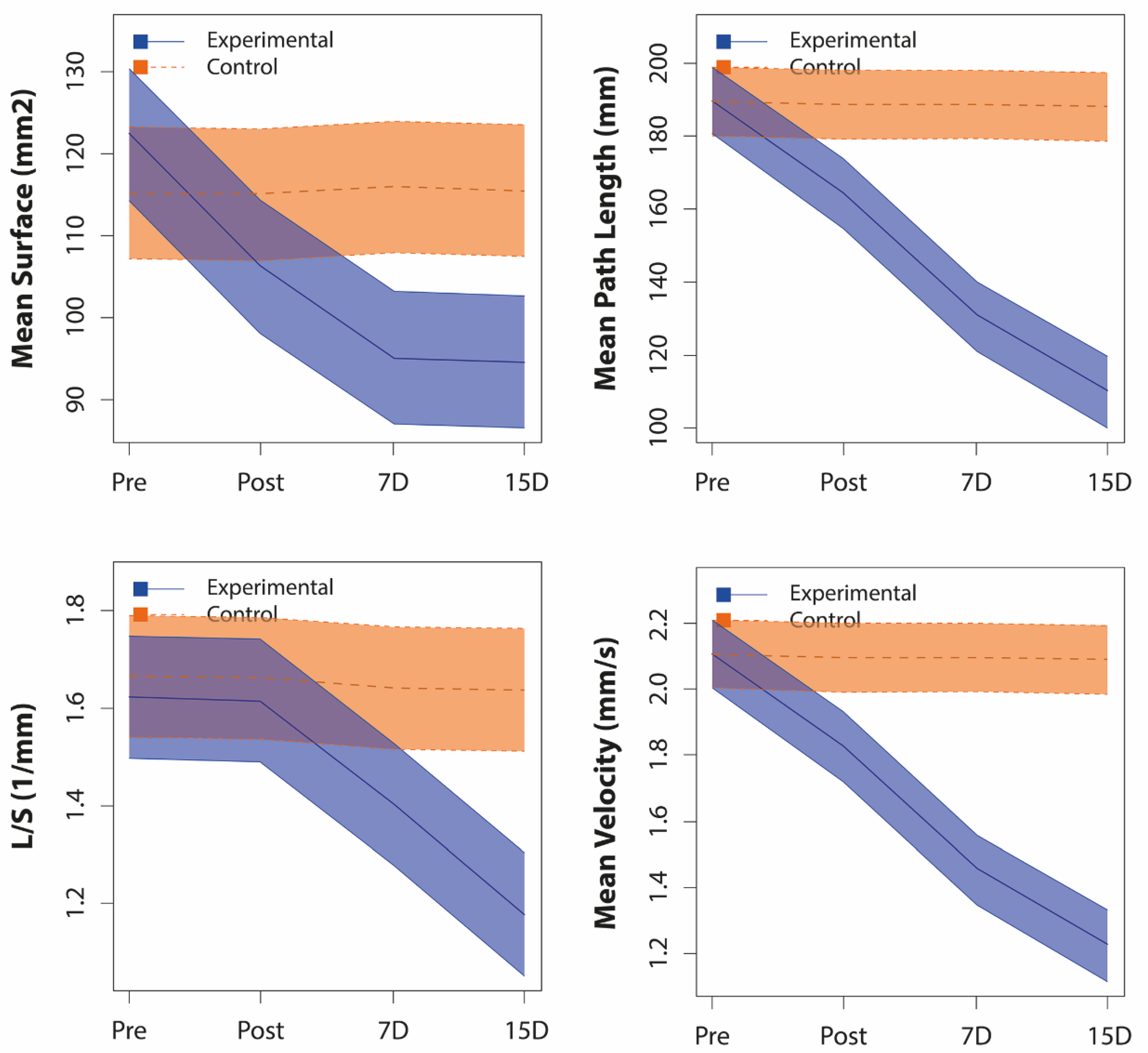
3.2.3. Correlations between Limited Cervical Rotation and Stabilometrics Variables
4. Discussion
4.1. Effects of Upper Cervical HVLA Manipulation on CROM
4.2. Effects of Upper Cervical HVLA Manipulation on Standing Postural Control
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bier, J.D.; Scholten-Peeters, G.G.; Staal, J.B.; Pool, J.; Van Tulder, M.W.; Beekman, E.; Knoop, J.; Meerhoff, G.; Verhagen, A.P. Clinical Practice Guideline for Physical Therapy Assessment and Treatment in Patients With Nonspecific Neck Pain. Phys. Ther. 2017, 98, 162–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoy, D.; March, L.; Woolf, A.D.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Barendregt, J.; Blore, J.; Murray, C.; et al. The global burden of neck pain: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Childs, J.D.; Clelandt, J.A.; Elliot, J.M.; Teyhen, D.S.; Wainner, R.S.; Whitmam, J.M.; Sopky, B.J.; Godges, J.J.; Flynn, T.W.; Delitto, A.; et al. Neck Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2008, 38, A1–A34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, B.A.; Taylor, H.H.; Marshall, P. The Effect of Spinal Manipulation on the Efficacy of a Rehabilitation Protocol for Patients with Chronic Neck Pain: A Pilot Study. J. Manip. Physiol. Ther. 2010, 33, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Côté, P.; Van Der Velde, G.; Cassidy, J.D.; Carroll, L.; Hogg-Johnson, S.; Holm, L.W.; Carragee, E.J.; Haldeman, S.; Nordin, M.; Hurwitz, E.L.; et al. The burden and determinants of neck pain in workers: Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J. Manip. Physiol. Ther. 2009, 32, S70–S86. [Google Scholar] [CrossRef] [PubMed]
- De Vries, J.; Ischebeck, B.; Voogt, L.; Van Der Geest, J.N.; Janssen, M.; Frens, M.A.; Kleinrensink, G. Joint position sense error in people with neck pain: A systematic review. Man. Ther. 2015, 20, 736–744. [Google Scholar] [CrossRef]
- Stanton, T.; Leake, H.B.; Chalmers, S.; Moseley, G.L. Evidence of Impaired Proprioception in Chronic, Idiopathic Neck Pain: Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 876–887. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, B.; McNair, P.; Taylor, D.; McNair, P. Head and Neck Position Sense. Sports Med. 2008, 38, 101–117. [Google Scholar] [CrossRef]
- Ruhe, A.; Fejer, R.; Walker, B.F. Altered postural sway in patients suffering from non-specific neck pain and whiplash associated disorder-A systematic review of the literature. Chiropr. Man. Ther. 2011, 19, 13. [Google Scholar] [CrossRef] [Green Version]
- Vuillerme, N.; Pinsault, N. Experimental neck muscle pain impairs standing balance in humans. Exp. Brain Res. 2009, 192, 723–729. [Google Scholar] [CrossRef] [Green Version]
- Strimpakos, N.; Sakellari, V.; Gioftsos, G.; Kapreli, E.; Oldham, J. Cervical joint position sense: An intra- and inter-examiner reliability study. Gait Posture 2006, 23, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Proske, U. What is the role of muscle receptors in proprioception? Muscle Nerve 2005, 31, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Röijezon, U.; Clark, N.C.; Treleaven, J. Proprioception in musculoskeletal rehabilitation. Part 1: Basic science and principles of assessment and clinical interventions. Man. Ther. 2015, 20, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Treleaven, J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control. Man. Ther. 2008, 13, 2–11. [Google Scholar] [CrossRef]
- Boyd-Clark, L.C.; Briggs, C.A.; Galea, M.P. Muscle Spindle Distribution, Morphology, and Density in Longus Colli and Multifidus Muscles of the Cervical Spine. Spine 2002, 27, 694–701. [Google Scholar] [CrossRef] [Green Version]
- Clark, N.C.; Röijezon, U.; Treleaven, J. Proprioception in musculoskeletal rehabilitation. Part 2: Clinical assessment and intervention. Man. Ther. 2015, 20, 378–387. [Google Scholar] [CrossRef]
- López-Rodríguez, S.; Fernández-De-Las-Peñas, C.; Alburquerque-Sendín, F.; Rodríguez-Blanco, C.; Palomeque-Del-Cerro, L. Immediate Effects of Manipulation of the Talocrural Joint on Stabilometry and Baropodometry in Patients With Ankle Sprain. J. Manip. Physiol. Ther. 2007, 30, 186–192. [Google Scholar] [CrossRef]
- Alburquerque-Sendín, F.; Fernández-De-Las-Peñas, C.; Santos-Del-Rey, M.; Vallejo, J.M. Immediate effects of bilateral manipulation of talocrural joints on standing stability in healthy subjects. Man. Ther. 2009, 14, 75–80. [Google Scholar] [CrossRef]
- Farazdaghi, M.R.; Motealleh, A.; Abtahi, F.; Panjan, A.; Sarabon, N.; Ghaffarinejad, F. Effect of sacroiliac manipulation on postural sway in quiet standing: A randomized controlled trial. Braz. J. Phys. Ther. 2017, 22, 120–126. [Google Scholar] [CrossRef]
- Méndez-Sánchez, R.; González-Iglesias, J.; Sánchez-Sánchez, J.L.; Puente-González, A.S. Immediate Effects of Bilateral Sacroiliac Joint Manipulation on Plantar Pressure Distribution in Asymptomatic Participants. J. Altern. Complement. Med. 2014, 20, 251–257. [Google Scholar] [CrossRef]
- García-Pérez-Juana, D.; Fernández-De-Las-Peñas, C.; Arias-Buría, J.L.; Cleland, J.A.; Manzano, G.P.; Ortega-Santiago, R. Changes in Cervicocephalic Kinesthetic Sensibility, Widespread Pressure Pain Sensitivity, and Neck Pain After Cervical Thrust Manipulation in Patients With Chronic Mechanical Neck Pain: A Randomized Clinical Trial. J. Manip. Physiol. Ther. 2018, 41, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Coulter, I.D.; Crawford, C.; Vernon, H.; Hurwitz, E.L.; Khorsan, R.; Booth, M.S.; Herman, P.M. Manipulation and Mobilization for Treating Chronic Nonspecific Neck Pain: A Systematic Review and Meta-Analysis for an Appropriateness Panel. Pain Physician 2019, 22, E55–E70. [Google Scholar] [PubMed]
- Gyer, G.; Michael, J.; Inklebarger, J.; Tedla, J.S. Spinal manipulation therapy: Is it all about the brain? A current review of the neurophysiological effects of manipulation. J. Integr. Med. 2019, 17, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Dunning, J.R.; Butts, R.; Mourad, F.; Young, I.; Fernández-De-Las-Peñas, C.; Hagins, M.; Stanislawski, T.; Donley, J.; Buck, D.; Hooks, T.; et al. Upper cervical and upper thoracic manipulation versus mobilization and exercise in patients with cervicogenic headache: A multi-center randomized clinical trial. BMC Musculoskelet. Disord. 2016, 17, 64. [Google Scholar] [CrossRef] [Green Version]
- Haavik, H.; Murphy, B.A. The role of spinal manipulation in addressing disordered sensorimotor integration and altered motor control. J. Electromyogr. Kinesiol. 2012, 22, 768–776. [Google Scholar] [CrossRef]
- Ferreira, M.; Ferreira, P.; Hodges, P. Changes in postural activity of the trunk muscles following spinal manipulative therapy. Man. Ther. 2007, 12, 240–248. [Google Scholar] [CrossRef]
- Honoré, M.; Leboeuf-Yde, C.; Gagey, O.; Wedderkopp, N. How big is the effect of spinal manipulation on the pressure pain threshold and for how long does it last?–secondary analysis of data from a systematic review. Chiropr. Man. Ther. 2019, 27, 22. [Google Scholar] [CrossRef] [Green Version]
- Sterling, M.; De Zoete, R.M.J.; Coppieters, I.; Farrell, S.F. Best Evidence Rehabilitation for Chronic Pain Part 4: Neck Pain. J. Clin. Med. 2019, 8, 1219. [Google Scholar] [CrossRef] [Green Version]
- Blanpied, P.; Gross, A.; Elliott, J.M.; Devaney, L.; Clewley, D.; Walton, D.M.; Sparks, C.; Robertson, E.K. Neck Pain: Revision 2017. J. Orthop. Sports Phys. Ther. 2017, 47, A1–A83. [Google Scholar] [CrossRef] [Green Version]
- Grassi, D.D.O.; De Souza, M.Z.; Ferrareto, S.B.; Montebelo, M.I.D.L.; Guirro, E.C.D.O. Immediate and lasting improvements in weight distribution seen in baropodometry following a high-velocity, low-amplitude thrust manipulation of the sacroiliac joint. Man. Ther. 2011, 16, 495–500. [Google Scholar] [CrossRef]
- Oliva-Pascual-Vaca, Á.; Punzano-Rodríguez, R.; Escribá-Astaburuaga, P.; Fernández-Domínguez, J.C.; Ricard, F.; Franco-Sierra, M.A.; Blanco, C.R. Short-Term Changes in Algometry, Inclinometry, Stabilometry, and Urinary pH Analysis After a Thoracolumbar Junction Manipulation in Patients with Kidney Stones. J. Altern. Complement. Med. 2017, 23, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Goertz, C.M.; Xia, T.; Long, C.R.; Vining, R.D.; Pohlman, K.A.; DeVocht, J.W.; Gudavalli, M.R.; Owens, E.F.; Meeker, W.C.; Wilder, D.G. Effects of spinal manipulation on sensorimotor function in low back pain patients–a randomized controlled trial. Man. Ther. 2016, 21, 183–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, A.R.; Bacon, C.; Mannion, J.V. The Effect of Cervical Spine Manipulation on Postural Sway in Patients with Nonspecific Neck Pain. J. Manip. Physiol. Ther. 2015, 38, 65–73. [Google Scholar] [CrossRef]
- Dunning, J.R.; Cleland, J.A.; Waldrop, M.A.; Arnot, C.; Young, I.; Turner, M.; Sigurdsson, G. Upper Cervical and Upper Thoracic Thrust Manipulation Versus Nonthrust Mobilization in Patients With Mechanical Neck Pain: A Multicenter Randomized Clinical Trial. J. Orthop. Sports Phys. Ther. 2012, 42, 5–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, L.-J.; Stokell, R.; Treleaven, J. The effect of neck torsion on postural stability in subjects with persistent whiplash. Man. Ther. 2011, 16, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, M.; Martoni, M.; Esposito, M.J.; Brighetti, G.; Natale, V. Postural control after a night without sleep. Neuropsychologia 2006, 44, 2520–2525. [Google Scholar] [CrossRef]
- Piña-Pozo, F.; Heredia-Rizo, A.M.; Madeleine, P.; Escobio-Prieto, I.; Luque-Carrasco, A.; Oliva-Pascual-Vaca, Á. Local and Widespread Pressure Pain Hyperalgesia Is Not Side Specific in Females with Unilateral Neck Pain that Can Be Reproduced during Passive Neck Rotation. J. Clin. Med. 2019, 8, 1246. [Google Scholar] [CrossRef] [Green Version]
- Hall, T.M.; Briffa, K.; Hopper, D. The influence of lower cervical joint pain on range of motion and interpretation of the flexion–rotation test. J. Man. Manip. Ther. 2010, 18, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Ogince, M.; Hall, T.; Robinson, K.; Blackmore, A.M. The diagnostic validity of the cervical flexion-rotation test in C1/2- related cervicogenic headache. Man. Ther. 2007, 12, 256–262. [Google Scholar] [CrossRef]
- Hall, T.; Robinson, K.W.; Fujinawa, O.; Akasaka, K.; Pyne, E.A. Intertester Reliability and Diagnostic Validity of the Cervical Flexion-Rotation Test. J. Manip. Physiol. Ther. 2008, 31, 293–300. [Google Scholar] [CrossRef]
- Takasaki, H.; Hall, T.; Oshiro, S.; Kaneko, S.; Ikemoto, Y.; Jull, G.A. Normal kinematics of the upper cervical spine during the Flexion–Rotation Test – In vivo measurements using magnetic resonance imaging. Man. Ther. 2011, 16, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, T.; Briffa, K.; Hopper, D.; Robinson, K. Long-Term Stability and Minimal Detectable Change of the Cervical Flexion-Rotation Test. J. Orthop. Sports Phys. Ther. 2010, 40, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Hall, T.M.; Robinson, K. The flexion–rotation test and active cervical mobility—A comparative measurement study in cervicogenic headache. Man. Ther. 2004, 9, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Ruhe, A.; Fejer, R.; Walker, B.F. The test–retest reliability of centre of pressure measures in bipedal static task conditions – A systematic review of the literature. Gait Posture 2010, 32, 436–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagymáté, G.; Orlovits, Z.; Kiss, R.M. Reliability analysis of a sensitive and independent stabilometry parameter set. PLoS ONE 2018, 13, e0195995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scoppa, F.; Capra, R.; Gallamini, M.; Shiffer, R. Clinical stabilometry standardization: Basic definitions-acquisition interval-sampling frequency. Gait Posture 2013, 37, 290–292. [Google Scholar] [CrossRef]
- Dunning, J.R.; Mourad, F.; Barbero, M.; Leoni, D.; Cescon, C.; Butts, R. Bilateral and multiple cavitation sounds during upper cervical thrust manipulation. BMC Musculoskelet. Disord. 2013, 14, 24. [Google Scholar] [CrossRef] [Green Version]
- Gray, C.D.; Kinnear, P.R. IBM SPSS Statistics 19 Made Simple; Psychology Press: Hove, UK, 2012. [Google Scholar]
- Salom-Moreno, J.; Ortega-Santiago, R.; Cleland, J.A.; Palacios-Ceña, M.; Truyols-Domínguez, S.; Fernández-De-Las-Peñas, C. Immediate Changes in Neck Pain Intensity and Widespread Pressure Pain Sensitivity in Patients with Bilateral Chronic Mechanical Neck Pain: A Randomized Controlled Trial of Thoracic Thrust Manipulation vs Non–Thrust Mobilization. J. Manip. Physiol. Ther. 2014, 37, 312–319. [Google Scholar] [CrossRef]
- Martínez-Segura, R.; De-La-Llave-Rincón, A.I.; Ortega-Santiago, R.; Cleland, J.A.; Fernández-De-Las-Peñas, C. Immediate Changes in Widespread Pressure Pain Sensitivity, Neck Pain, and Cervical Range of Motion After Cervical or Thoracic Thrust Manipulation in Patients With Bilateral Chronic Mechanical Neck Pain: A Randomized Clinical Trial. J. Orthop. Sports Phys. Ther. 2012, 42, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Mansilla-Ferragut, P.; Fernández-De-Las-Peñas, C.; Alburquerque-Sendín, F.; Cleland, J.A.; Boscá-Gandía, J.J. Immediate Effects of Atlanto-Occipital Joint Manipulation on Active Mouth Opening and Pressure Pain Sensitivity in Women With Mechanical Neck Pain. J. Manip. Physiol. Ther. 2009, 32, 101–106. [Google Scholar] [CrossRef]
- De Oliveira-Souza, A.; Florencio, L.L.; Carvalho, G.F.; Fernández-De-Las-Peñas, C.; Dach, F.; Bevilaqua-Grossi, D. Reduced flexion rotation test in women with chronic and episodic migraine. Braz. J. Phys. Ther. 2019, 23, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Saadat, M.; Salehi, R.; Negahban, H.; Shaterzadeh, M.J.; Mehravar, M.; Hessam, M. Postural stability in patients with non-specific chronic neck pain: A comparative study with healthy people. Med J. Islam. Repub. Iran 2018, 32, 33. [Google Scholar] [CrossRef] [PubMed]
- Clements, B.; Gibbons, P.; McLaughlin, P. The amelioration of atlanto-axial rotation asymmetry using high velocity low amplitude manipulation: Is the direction of thrust important? J. Osteopat. Med. 2001, 4, 8–14. [Google Scholar] [CrossRef]
- Mohamed, A.A.; Shendy, W.S.; Semary, M.; Mourad, H.S.; Battecha, K.H.; Soliman, E.S.; El Sayed, S.H.; Mohamed, G.I. Combined use of cervical headache snag and cervical snag half rotation techniques in the treatment of cervicogenic headache. J. Phys. Ther. Sci. 2019, 31, 376–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferracini, G.N.; Florencio, L.L.; Dach, F.; Bevilaqua-Grossi, D.; Palacios-Ceña, M.; Ordás-Bandera, C.; Chaves, T.C.; Speciali, J.G.; Fernández-De-Las-Peñas, C. Musculoskeletal disorders of the upper cervical spine in women with episodic or chronic migraine. Eur. J. Phys. Rehabil. Med. 2017, 53, 342–350. [Google Scholar] [PubMed]
- Malo-Urriés, M.; Tricás-Moreno, J.M.; Estébanez-De-Miguel, E.; Hidalgo-García, C.; Carrasco, A.; Cabanillas-Barea, S. Immediate Effects of Upper Cervical Translatoric Mobilization on Cervical Mobility and Pressure Pain Threshold in Patients with Cervicogenic Headache: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2017, 40, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Amaral, G.; Martins, H.; Silva, A.G. Postural control in subclinical neck pain: A comparative study on the effect of pain and measurement procedures. Scand. J. Pain 2018, 18, 295–302. [Google Scholar] [CrossRef]
- De Zoete, R.M.; Osmotherly, P.G.; Rivett, D.A.; Snodgrass, S.J. No Differences between Individuals With Chronic Idiopathic Neck Pain and Asymptomatic Individuals on 7 Cervical Sensorimotor Control Tests: A Cross-sectional Study. J. Orthop. Sports Phys. Ther. 2020, 50, 33–43. [Google Scholar] [CrossRef]
- Miranda, I.F.; Facchini, D.; Manfio, E.F. Influence of Cervical Spine Manipulation on Neck Joint Position Sense error in patients with chronic neck pain. Man. Ther. Posturology Rehabilitation J. 2016, 14, 405. [Google Scholar] [CrossRef]
- Reid, S.; Callister, R.; Katekar, M.G.; Rivett, D.A. Effects of Cervical Spine Manual Therapy on Range of Motion, Head Repositioning, and Balance in Participants with Cervicogenic Dizziness: A Randomized Controlled Trial. Arch. Phys. Med. Rehabilitation 2014, 95, 1603–1612. [Google Scholar] [CrossRef]
- Moustafa, I.M.; Diab, A.A. The addition of upper cervical manipulative therapy in the treatment of patients with fibromyalgia: A randomized controlled trial. Rheumatol. Int. 2015, 35, 1163–1174. [Google Scholar] [CrossRef] [PubMed]
- Fischetti, F.; Cataldi, S.; Giunto, A.; Greco, G. Effect of home-based oculomotor exercises on postural stability in healthy female adults. J. Hum. Sport Exerc. 2019, 15, 1–8. [Google Scholar] [CrossRef]
- Forti, S.; Filipponi, E.; Di Berardino, F.; Barozzi, S.; Cesarani, A. The influence of music on static posturography. J. Vestib. Res. 2010, 20, 351–356. [Google Scholar] [CrossRef]
- Quek, J.M.T.; Pua, Y.-H.; Bryant, A.L.; Clark, R.A. The Influence of Cervical Spine Flexion-Rotation Range-of-Motion Asymmetry on Postural Stability in Older Adults. Spine 2013, 38, 1648–1655. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.-L.; Chen, C.P.; Nikkhoo, M.; Lin, C.-F.; Ching, C.T.-S.; Niu, C.-C.; Cheng, C.-H. Fatigue changes neck muscle control and deteriorates postural stability during arm movement perturbations in patients with chronic neck pain. Spine J. 2020, 20, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Eguaras, N.; Rodríguez-López, E.S.; Lopez-Dicastillo, O.; Franco-Sierra, M.Á.; Ricard, F.; Oliva-Pascual-Vaca, Á. Effects of Osteopathic Visceral Treatment in Patients with Gastroesophageal Reflux: A Randomized Controlled Trial. J. Clin. Med. 2019, 8, 1738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliva-Pascual-Vaca, Á.; González-González, C.; Oliva-Pascual-Vaca, J.; Piña-Pozo, F.; Ferragut-Garcías, A.; Fernandez-Dominguez, J.C.; Heredia-Rizo, A.M. Visceral Origin: An Underestimated Source of Neck Pain. A Systematic Scoping Review. Diagnostics 2019, 9, 186. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Experimental | Control | p-Value |
|---|---|---|---|
| Gender, women %(n) | 50.00 (11) | 54.55 (10) | 0.763 |
| Age (year) | 38.36 ± 11.664 | 37.50 ± 11.827 | 0.809 |
| Weight (Kg) | 64.32 ± 12.411 | 63.59 ± 9.404 | 0.828 |
| Height (m) | 1.67 ± 0.973 | 1.68 ± 0.626 | 0.971 |
| BMI (kg/m2) | 22.66 ± 3.349 | 22.55 ± 3.213 | 0.909 |
| Limited Rotation (degrees) | 31.36 ± 0.902 | 30.14 ± 1.167 | <0.001 * |
| Mean velocity (mm/s) | 2.11 ± 0.269 | 2.11 ± 0.280 | 0.996 |
| Surface length ratio L/S (1/mm) | 1.63 ± 0.455 | 1.67 ± 0.289 | 0.721 |
| Mean Surface (mm2) | 122.42 ± 25.679 | 115.17 ± 15.807 | 0.266 |
| Mean Path length (mm) | 189.20 ± 24.147 | 189.50 ± 25.256 | 0.998 |
| Mean Pressure (g/cm2) | 313.28 ± 51.123 | 299.65 ± 65.406 | 0.445 |
| Mean COP X | −0.26 ± 5.328 | 0.60 ± 6.100 | 0.623 |
| Mean COP Y | −5.36 ± 5.001 | −3.67 ± 1.912 | 0.145 |
| Mean Anterior Velocity (mm/s) | 1.24 ± 0.366 | 1.16 ± 0.201 | 0.390 |
| Mean Lateral Velocity (mm/s) | 0.76 ± 0.181 | 0.85 ± 0.171 | 0.131 |
| Variable | Group | Time * Group | ||||
|---|---|---|---|---|---|---|
| F | p-Value | (ƞ 2 p) | F | p-Value | (ƞ 2 p) | |
| Limited Rotation (degrees) | 132.087 * | <0.001 | 0.759 | 46.447 * | <0.001 | 0.777 |
| Surface length ratio L/S (1/mm) | 6.133 * | 0.017 | 0.127 | 16.434 * | <0.001 | 0.552 |
| Mean velocity (mm/s) | 41.636 * | <0.001 | 0.498 | 78.990 * | <0.001 | 0.856 |
| Mean Surface (mm2) | 4.040 | 0.051 | 0.088 | 14.695 * | <0.001 | 0.524 |
| Mean Path length (mm) | 41.668 * | <0.001 | 0.498 | 78.180 * | <0.001 | 0.854 |
| Mean Pressure (g/cm2) | <0.001 | 0.999 | <0.001 | 6.374 * | 0.001 | 0.323 |
| Mean COP X | 0.559 | 0.459 | 0.013 | 0.668 | 0.576 | 0.048 |
| Mean COP Y | 16.046 * | <0.001 | 0.276 | 3.746 * | 0.018 | 0.219 |
| Mean Anterior Velocity (mm/s) | 0.361 | 0.551 | 0.009 | 3.831 * | 0.017 | 0.223 |
| Mean Lateral Velocity (mm/s) | 3.662 | 0.062 | 0.080 | 3.831 * | 0.017 | 0.223 |
| Variable | Time-Evaluation | Differences (EG-CG) | p-Value | CI 95% | ||
|---|---|---|---|---|---|---|
| Mean | ±SEM | Lower | Upper | |||
| Limited Rotation | Baseline | 1.227 * | 0.314 | <0.001 | 0.593 | 1.862 |
| (degrees) | Post-immediate | 8.318 * | 0.752 | <0.001 | 6.800 | 9.836 |
| 7 days | 7.909 * | 0.667 | <0.001 | 6.563 | 9.255 | |
| 15 days | 6.818 * | 0.638 | <0.001 | 5.530 | 8.106 | |
| Surface length ratio L/S | Baseline | −0.041 | 0.115 | 0.721 | −0.273 | 0.190 |
| (1/mm) | Post-immediate | −0.045 | 0.107 | 0.675 | −0.262 | 0.171 |
| 7 days | −0.235 * | 0.073 | 0.002 | −0.382 | −0.089 | |
| 15 days | −0.460 * | 0.065 | <0.001 | −0.591 | −0.330 | |
| Mean velocity | Baseline | <0.001 | 0.083 | 0.996 | −0.167 | 0.166 |
| (mm/s) | Post-immediate | −0.271 * | 0.077 | 0.001 | −0.427 | −0.116 |
| 7 days | −0.645 * | 0.072 | <0.001 | −0.791 | −0.498 | |
| 15 days | −0.867 * | 0.076 | <0.001 | −1.021 | −0.713 | |
| Mean Surface | Baseline | 7.246 | 6.429 | 0.266 | −5.728 | 20.220 |
| (mm2) | Post-immediate | −8.786 | 6.427 | 0.179 | −21.757 | 4.184 |
| 7 days | −20.845 * | 5.535 | 0.001 | −32.016 | −9.675 | |
| 15 days | −21.023 * | 5.276 | <0.001 | −31.670 | −10.376 | |
| Mean Path length | Baseline | 0.018 | 7.450 | 0.998 | −15.016 | 15.052 |
| (mm) | Post-immediate | −24.564 * | 6.923 | 0.001 | −38.536 | −10.592 |
| 7 days | −57.945 * | 6.517 | <0.001 | −71.098 | −44.793 | |
| 15 days | −78.023 * | 6.892 | <0.001 | −91.932 | −64.113 | |
| Mean Pressure | Baseline | 13.638 | 17.699 | 0.445 | −22.080 | 49.356 |
| (g/cm2) | Post-immediate | −1.836 | 16.789 | 0.913 | −35.717 | 32.045 |
| 7 days | −5.280 | 16.415 | 0.749 | −38.406 | 27.846 | |
| 15 days | −6.623 | 16.735 | 0.694 | −40.394 | 27.149 | |
| Mean COP X | Baseline | −0.855 | 1.727 | 0.623 | −4.339 | 2.630 |
| Post-immediate | −1.600 | 1.704 | 0.353 | −5.039 | 1.839 | |
| 7 days | −1.255 | 1.578 | 0.431 | −4.439 | 1.930 | |
| 15 days | −1.091 | 1.557 | 0.487 | −4.232 | 2.051 | |
| Mean COP Y | Baseline | −1.695 | 1.143 | 0.145 | −4.001 | 0.610 |
| Post-immediate | −3.477 * | 0.958 | 0.001 | −5.410 | −1.545 | |
| 7 days | −4.259 * | 0.874 | <0.001 | −6.022 | −2.496 | |
| 15 days | −4.486 * | 0.913 | <0.001 | −6.330 | −2.643 | |
| Mean Anterior Velocity | Baseline | 0.077 | 0.089 | 0.390 | −0.102 | 0.257 |
| (mm/s) | Post-immediate | −0.045 | 0.073 | 0.535 | −0.192 | 0.101 |
| 7 days | −0.118 | 0.068 | 0.088 | −0.255 | 0.018 | |
| 15 days | −0.077 | 0.080 | 0.342 | −0.240 | 0.085 | |
| Mean Lateral Velocity | Baseline | −0.082 | 0.053 | 0.131 | −0.189 | 0.025 |
| (mm/s) | Post-immediate | −0.145 | 0.076 | 0.062 | −0.299 | 0.008 |
| 7 days | −0.136 | 0.083 | 0.106 | −0.303 | 0.030 | |
| 15 days | −0.155 | 0.078 | 0.053 | −0.311 | 0.002 | |
| Variable. | Time-Evaluation | Difference (Baseline-x) | p-Value | CI 95% | ||
|---|---|---|---|---|---|---|
| Mean | ±SEM | Lower | Upper | |||
| Limited Rotation | Post-immediate | −7.409 * | 0.463 | <0.001 | −8.687 | −6.131 |
| (degrees) | 7 days | −6.818 * | 0.411 | <0.001 | −7.952 | −5.684 |
| 15 days | −6.136 * | 0.381 | <0.001 | −7.188 | −5.085 | |
| Surface length ratio L/S | Post-immediate | 0.007 | 0.058 | 1.000 | −0.152 | 0.167 |
| (1/mm) | 7 days | 0.219 * | 0.064 | 0.008 | 0.042 | 0.395 |
| 15 days | 0.447 * | 0.066 | <0.001 | 0.265 | 0.629 | |
| Mean velocity | Post-immediate | 0.283 * | 0.046 | <0.001 | 0.157 | 0.409 |
| (mm/s) | 7 days | 0.655 * | 0.041 | <0.001 | 0.541 | 0.769 |
| 15 days | 0.884 * | 0.040 | <0.001 | 0.774 | 0.993 | |
| Mean Surface | Post-immediate | 16.210 * | 3.030 | <0.001 | 7.845 | 24.575 |
| (mm2) | 7 days | 27.287 * | 2.989 | <0.001 | 19.035 | 35.540 |
| 15 days | 27.892 * | 3.605 | <0.001 | 17.939 | 37.845 | |
| Mean Path length | Post-immediate | 25.618 * | 4.121 | <0.001 | 14.240 | 36.996 |
| (mm) | 7 days | 58.914 * | 3.729 | <0.001 | 48.618 | 69.210 |
| 15 days | 79.577 * | 3.578 | <0.001 | 69.698 | 89.456 | |
| Mean Pressure | Post-immediate | 17.519 * | 3.415 | <0.001 | 8.090 | 26.948 |
| (g/cm2) | 7 days | 18.817 * | 3.388 | <0.001 | 9.463 | 28.172 |
| 15 days | 19.873 * | 3.226 | <0.001 | 10.968 | 28.779 | |
| Mean COP X | Post-immediate | 0.741 | 0.418 | 0.407 | −0.412 | 1.894 |
| 7 days | 0.445 | 0.480 | 0.930 | −0.880 | 1.771 | |
| 15 days | 0.395 | 0.508 | 0.969 | −1.007 | 1.798 | |
| Mean COP Y | Post-immediate | 1.891 * | 0.678 | 0.046 | 0.020 | 3.762 |
| 7 days | 2.814 * | 0.695 | 0.001 | 0.895 | 4.732 | |
| 15 days | 2.873 * | 0.683 | 0.001 | 0.988 | 4.757 | |
| Mean Anterior Velocity | Post-immediate | 0.164 * | 0.058 | 0.043 | 0.004 | 0.324 |
| (mm/s) | 7 days | 0.186 * | 0.047 | 0.002 | 0.055 | 0.317 |
| 15 days | 0.150 * | 0.052 | 0.037 | 0.006 | 0.294 | |
| Mean Lateral Velocity | Post-immediate | 0.027 | 0.037 | 0.975 | −0.074 | 0.128 |
| (mm/s) | 7 days | 0.064 | 0.039 | 0.497 | −0.043 | 0.171 |
| 15 days | 0.095 * | 0.033 | 0.033 | 0.005 | 0.186 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez, F.; Escribá, P.; Oliva-Pascual-Vaca, J.; Méndez-Sánchez, R.; Puente-González, A.S. Immediate and Short-Term Effects of Upper Cervical High-Velocity, Low-Amplitude Manipulation on Standing Postural Control and Cervical Mobility in Chronic Nonspecific Neck Pain: A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2580. https://doi.org/10.3390/jcm9082580
Gómez F, Escribá P, Oliva-Pascual-Vaca J, Méndez-Sánchez R, Puente-González AS. Immediate and Short-Term Effects of Upper Cervical High-Velocity, Low-Amplitude Manipulation on Standing Postural Control and Cervical Mobility in Chronic Nonspecific Neck Pain: A Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(8):2580. https://doi.org/10.3390/jcm9082580
Chicago/Turabian StyleGómez, Francisco, Pablo Escribá, Jesús Oliva-Pascual-Vaca, Roberto Méndez-Sánchez, and Ana Silvia Puente-González. 2020. "Immediate and Short-Term Effects of Upper Cervical High-Velocity, Low-Amplitude Manipulation on Standing Postural Control and Cervical Mobility in Chronic Nonspecific Neck Pain: A Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 8: 2580. https://doi.org/10.3390/jcm9082580
APA StyleGómez, F., Escribá, P., Oliva-Pascual-Vaca, J., Méndez-Sánchez, R., & Puente-González, A. S. (2020). Immediate and Short-Term Effects of Upper Cervical High-Velocity, Low-Amplitude Manipulation on Standing Postural Control and Cervical Mobility in Chronic Nonspecific Neck Pain: A Randomized Controlled Trial. Journal of Clinical Medicine, 9(8), 2580. https://doi.org/10.3390/jcm9082580