Validation of the Spiritual Distress Scale in Portuguese Cancer Patients Undergoing Chemotherapy: A Methodological Study


Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Setting
2.3. Population and Sampling
2.4. Instrument
2.5. Data Collection
2.6. Data Analysis
2.7. Ethical Considerations
3. Results
3.1. Descriptive Results of the SDS
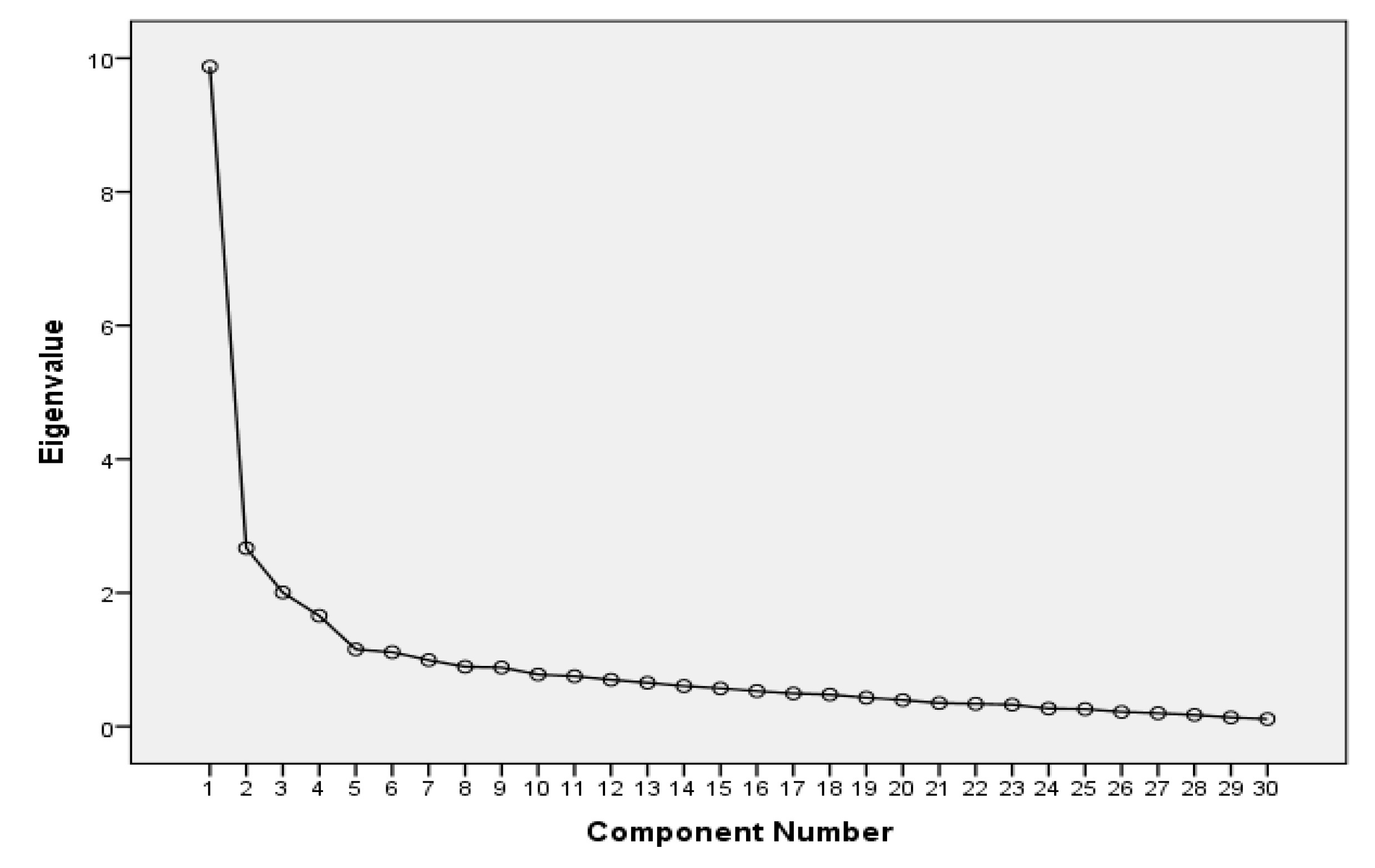
3.2. Exploratory Factor Analysis
3.3. Reliability
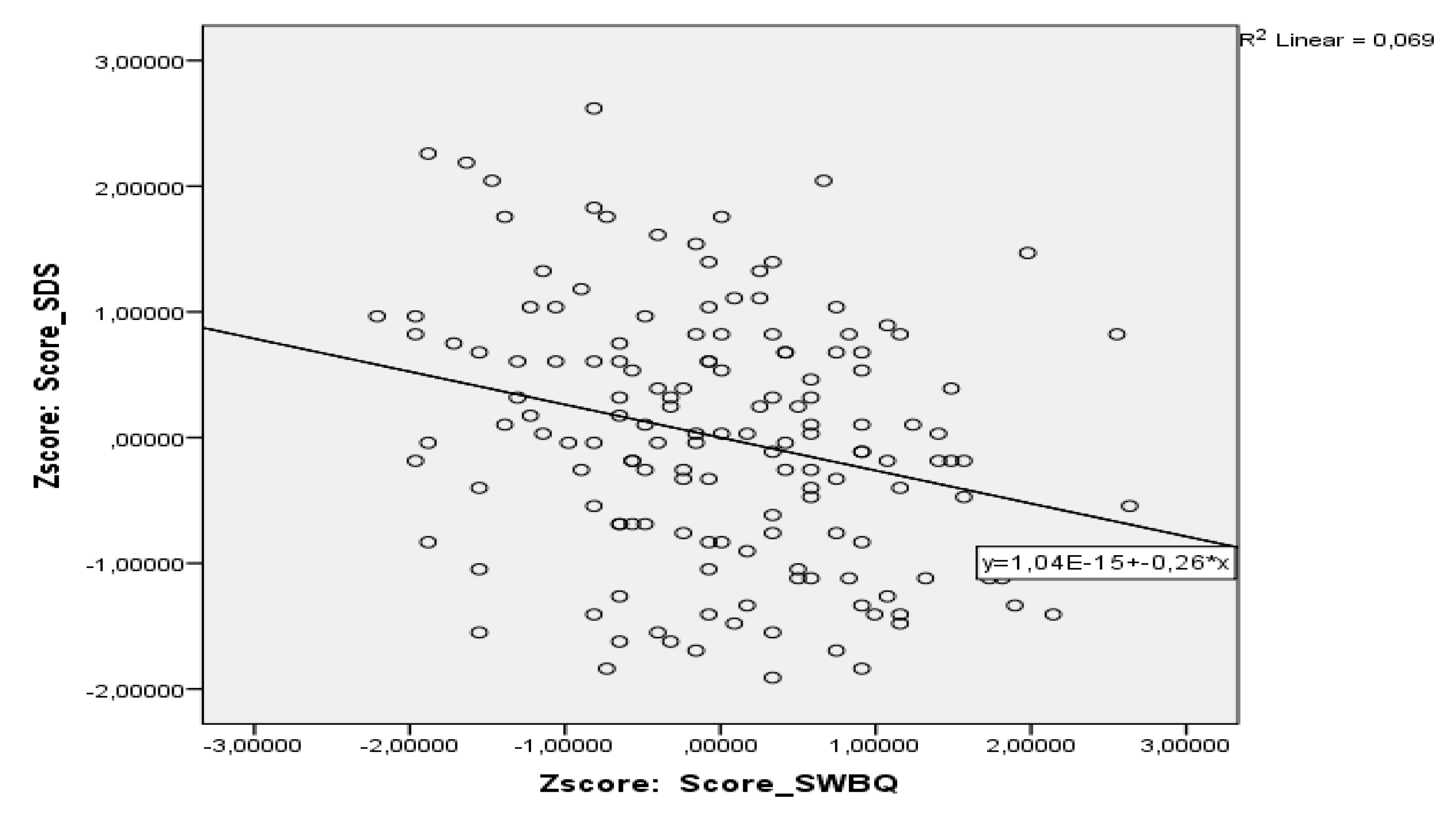
3.4. Divergent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bahraini, Sayna, Wendy Gifford, Ian D. Graham, Liquaa Wazni, Suzette Brémault-Phillips, Rebekah Hackbusch, Catrine Demers, and Mary Egan. 2019. The accuracy of measures in screening adults for spiritual suffering in health care settings: A systematic review. Palliative and Supportive Care 7: 1–14. [Google Scholar] [CrossRef]
- Best, Megan, Lynley Aldridge, Phyllis Butow, Ian Oliver, Melanie Price, and Fleur Webster. 2015. Assessment of Spiritual Suffering in the Cancer Context: A Systematic Literature Review. Palliative and Supportive Care 13: 1335–61. [Google Scholar] [CrossRef]
- Bornet, Marc-Antoine, Etienne Rochat, Anne-Véronique Dürst, Sarah Fustinoni, Christophe Büla, Armin von Gunten, and Stéfanie Monod. 2016. Instruments to Assess Depressive Symptoms and Spiritual Distress Investigate Different Dimensions. Clinical Gerontologist 39: 104–16. [Google Scholar] [CrossRef]
- Büssing, Arndt, Andreas Günther, Klaus Baumann, Eckhard Frick, and Christoph Jacobs. 2013. Spiritual Dryness as a Measure of a Specific Spiritual Crisis in Catholic Priests: Associations with Symptoms of Burnout and Distress. Evidence-Based Complementary and Alternative Medicine 2013: 246797. [Google Scholar] [CrossRef]
- Büssing, Arndt, Daniela Rodrigues Recchia, Koenig Harold, Klaus Baumann, and Eckhard Frick. 2018. Factor Structure of the Spiritual Needs Questionnaire (SpNQ) in Persons with Chronic Diseases, Elderly and Healthy Individuals. Religions 9: 13. [Google Scholar] [CrossRef]
- Caldeira, Sílvia, Emília Campos Carvalho, and Margarida Vieira. 2013. Spiritual Distress-Proposing a New Definition and Defining Characteristics. International Journal of Nursing Knowledge 24: 77–84. [Google Scholar] [CrossRef]
- Caldeira, Sílvia, Fiona Timmins, Emília Campos Carvalho, and Margarida Vieira. 2017. Spiritual Well-Being and Spiritual Distress in Cancer Patients Undergoing Chemotherapy: Utilizing the SWBQ as Component of Holistic Nursing Diagnosis. Journal of Religion & Health 56: 1489–502. [Google Scholar] [CrossRef]
- Caldeira, Sílvia, Joana Romeiro, and Helga Martins. 2019. The Role of the Nurse in Providing Spiritual Care: A Case Study Approach to Exploring Specific Care Provision by Healthcare Workers in the Context of an Interdisciplinary Healthcare Team. In Spirituality in Healthcare: Perspectives for Innovative Practice. Edited by Fiona Timmins and Sílvia Caldeira. Cham: Springer, pp. 117–42. [Google Scholar]
- Draper, Peter. 2012. An Integrative Review of Spiritual Assessment: Implications for Nursing Management. Journal of Nursing Management 20: 970–98. [Google Scholar] [CrossRef]
- Gomez, Rapson, and John W. Fisher. 2003. Domains of Spiritual Well-Being and Development and Validation of the Spiritual Well-Being Questionnaire. Personality and Individual Differences 35: 1975–91. [Google Scholar] [CrossRef]
- Gomez, Rapson, and John W. Fisher. 2005a. Item Response Theory Analysis of the Spiritual Well-Being Questionnaire. Personality and Individual Differences 38: 1107–21. [Google Scholar] [CrossRef]
- Gomez, Rapson, and John W. Fisher. 2005b. The Spiritual Well -Being Questionnaire: Testing for Model Applicability, Measurement and Structural Equivalencies, and Latent Mean Differences Across Gender. Personality and Individual Differences 39: 1383–93. [Google Scholar] [CrossRef]
- Gouveia, Maria João, Marta Marques, and José Luís Pais-Ribeiro. 2009. Versão Portuguesa do Questionário de Bem-Estar Espiritual (SWBQ): Análise Confirmatória da sua Estrutura Factorial. Psicologia, Saúde & Doenças 10: 285–93. [Google Scholar]
- Gray, Jennifer R., Susan K. Grove, and Suzanne Sutherland. 2017. Burns and Grove’s the Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence, 8th ed. Grand Rapids: Elsevier, 738p. First published 1987. [Google Scholar]
- Guttman, Louis. 1954. Some Necessary Conditions for Common Factor Analysis. Psychometrika 19: 149–61. [Google Scholar] [CrossRef]
- Heale, Roberta, and Alison Twycross. 2015. Validity and Reliability in Quantitative Research. Evidence-Based Nursing 18: 66–67. [Google Scholar] [CrossRef]
- Herdman, Heather T., and Shigemi Kamitsuru, eds. 2018. NANDA: NANDA International Nursing Diagnoses: Definitions and Classification 2018–2020, 11th ed. Chichester and Ames: Wiley-Blackwell, 1187p. First published 1994. [Google Scholar]
- Kaiser, Henry F. 1961. A Note on Guttman’s Lower Bound for the Number of Common Factors. British Journal of Psychology 14: 1–2. [Google Scholar] [CrossRef]
- Kopacz, Marek S., Claire A. Hoffmire, Sybil W. Morley, and C. Garland Vance. 2015. Using a Spiritual Distress Scale to Assess Suicide Risk in Veterans: An Exploratory Study. Pastoral Psychology 64: 381–90. [Google Scholar] [CrossRef]
- Ku, Ya-Lie. 2005. Spiritual Distress Experienced by Cancer Patients-Develop a Spiritual Care for Cancer Patients. Taiwan Journal of Hospice Palliative Care 10: 221–33. [Google Scholar]
- Ku, Ya-Lie, Shih-Ming Kuo, and Ching-Yi Yao. 2010. Establishing the Validity of a Spiritual Distress Scale for Cancer Patients Hospitalized in Southern Taiwan. International Journal of Palliative Nursing 16: 133–37. [Google Scholar] [CrossRef]
- Lestari, Puji, Aan Nuraeni, and Dyah Setyorini. 2018. Spiritual Distress in Breast Cancer Patients. Journal of Nursing Care 1: 155–63. [Google Scholar] [CrossRef]
- Martins, Helga, and Sílvia Caldeira. 2018. Spiritual Distress in Cancer Patients: A Synthesis of Qualitative Studies. Religions 9: 285. [Google Scholar] [CrossRef]
- Martins, Ana Raquel, Sara Pinto, Sílvia Caldeira, and Francisco Luís Pimentel. 2015. Translation and Adaptation of the Spirituality and Spiritual Care Rating Scale in Portuguese Palliative Care Nurses. Revista de Enfermagem Referência 4: 89–97. [Google Scholar] [CrossRef]
- Monod, Stéfanie, Mark Brennan, Etienne Rochat, Estelle Martin, Stéphane Rochat, and Christophe J. Büla. 2011. Instruments Measuring Spirituality in Clinical Research: A Systematic Review. Journal of General Internal Medicine 26: 1345–57. [Google Scholar] [CrossRef]
- Munro, Barbara Hazard. 2005. Statistical Methods for Health Care Research, 5th ed. Philadelphia: Lippincott Williams & Wilkins, 577p. First published 1986. [Google Scholar]
- Seddigh, Ruohollah, Amir-Abbas Keshavarz-Akhlaghi, and Somayeh Azarnik. 2016. Questionnaires Measuring Patients’ Spiritual Needs: A Narrative Literature Review. Iranian Journal of Psychiatry and Behavioral Sciences 10: e4011. [Google Scholar] [CrossRef]
- Simão, Talita Pardo, Erika de Cassia Lopes Chaves, Emília Campos de Carvalho, Denismar Alves Nogueira, Camila Csizmar Carvalho, Ya-Lie Ku, and Denise Hollanda Iunes. 2015. Cultural Adaptation and Analysis of the Psychometric Properties of the Brazilian Version of the Spiritual Distress Scale. Journal of Clinical Nursing 25: 231–39. [Google Scholar] [CrossRef]
- Sousa, Valmi D., and Wilaiporn Rojjanasrirat. 2011. Translation, Adaptation and Validation of Instruments or Scales for use in Cross-Cultural Health Care Research: A Clear and User-Friendly Guideline. Journal of Evaluation in Clinical Practice 17: 268–74. [Google Scholar] [CrossRef]
- Tabachnick, Barbara G., and Linda S. Fidell. 2013. Using Multivariate Statistics, 6th ed. Harlow: Pearson Education Limited Harlow, 1061p. First published 1983. [Google Scholar]
- Taylor, Elizabeth, and Iris Mamier. 2013. Nurse Responses to Patient Expressions of Spiritual Distress. Holistic Nursing Practice 27: 217–24. [Google Scholar] [CrossRef]
- Velosa, Teresa, Sílvia Caldeira, and Manuel Luís Capelas. 2017. Depression and Spiritual Distress in Adult Palliative Patients: A Cross-Sectional Study. Religions 8: 156. [Google Scholar] [CrossRef]
- Waltz, Carolyn, Ora Lea Strickland, and Elizabeth Lenz. 2016. Measurement in Nursing and Health Research, 5th ed. New York: Springer, 632p. First published 1991. [Google Scholar]



{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Gender | ||
| Male | 53 | 35.3 |
| Female | 97 | 64.7 |
| Age group | ||
| 35–39 | 8 | 5.3 |
| 40–59 | 59 | 39.3 |
| 60–79 | 82 | 54.7 |
| 80–99 | 1 | 0.7 |
| Age range (35–83 years) | ||
| M = 59.50 ± s = 11.24 | ||
| Marital status | ||
| Single | 11 | 7.3 |
| Married | 102 | 68.0 |
| Widower | 13 | 8.7 |
| Divorced | 15 | 10.0 |
| Unmarried | 9 | 6.0 |
| Educational level | ||
| 1° Cycle | 53 | 35.3 |
| 2° Cycle | 11 | 7.3 |
| 3° Cycle | 25 | 16.7 |
| High school | 38 | 25.3 |
| Diploma/Degree | 22 | 14.7 |
| Master’s degree | 1 | 0.7 |
| Professional occupation | ||
| Specialists in intellectual and scientific activities | 18 | 12.0 |
| Middle level technicians and professions | 6 | 4.0 |
| Administrative staff | 4 | 2.7 |
| Workers in personal and protective services | 1 | .7 |
| Farmers and skilled workers | 7 | 4.7 |
| Skilled industry workers | 7 | 4.7 |
| Plant and machine operators | 2 | 1.3 |
| Unskilled workers | 34 | 22.7 |
| Retired | 62 | 41.3 |
| Domestic | 7 | 4.7 |
| Unemployed | 2 | 1.3 |
| Religion | ||
| Catholic | 130 | 86.7 |
| Protestant | 9 | 6.0 |
| Agnostic | 11 | 7.3 |
| Clinical diagnosis | ||
| Lung | 23 | 15.3 |
| Pancreas | 2 | 1.3 |
| Colorectal | 39 | 26.0 |
| Uterus | 6 | 4.0 |
| Breast | 53 | 35.3 |
| Stomach | 3 | 2.0 |
| Prostate | 6 | 4.0 |
| Others | 6 | 4.0 |
| Non-Hodgkin’s lymphoma | 5 | 3.3 |
| Hodgkin’s lymphoma | 2 | 1.3 |
| Multiple myeloma | 3 | 2.0 |
| Testicles | 1 | 0.7 |
| Liver | 1 | 0.7 |
| Variable | Total Mean Score (M) | Standard Deviation (s) |
|---|---|---|
| Gender | ||
| Male | 61.23 | 13.38 |
| Female | 61.76 | 14.25 |
| Age group | ||
| 35–39 | ||
| 40–59 | 60.13 | 5.32 |
| 60–79 | 64.15 | 1.93 |
| 80–99 | 59.98 | 1.43 |
| Marital status | ||
| Single | 62.27 | 17.49 |
| Married | 61.59 | 13.62 |
| Widower | 59.00 | 10.25 |
| Divorced | 62.47 | 19.01 |
| Unmarried | 62.78 | 8.57 |
| Educational level | ||
| 1° Cycle | 59.77 | 13.79 |
| 2° Cycle | 68.82 | 11.99 |
| 3° Cycle | 64.80 | 14.49 |
| High school | 60.87 | 12.45 |
| Diploma/Degree | 58.86 | 15.52 |
| Master’s degree | 83.00 | |
| Professional occupation | ||
| Specialists in intellectual and scientific activities | 60.33 | 15.69 |
| Middle level technicians and professions | 65.50 | 10.89 |
| Administrative staff | 70.25 | 19.75 |
| Workers in personal and protective services | 75.00 | |
| Farmers and skilled workers | 68.14 | 19.91 |
| Skilled industry workers | 65.29 | 13.31 |
| Plant and machine operators | 58.00 | 24.04 |
| Unskilled workers | 61.35 | 14.30 |
| Retired | 59.92 | 13.13 |
| Domestic | 61.43 | 7.82 |
| Unemployed | 60.00 | 2.82 |
| Religion | ||
| Catholic | 61.91 | 14.07 |
| Protestant | 55.56 | 13.36 |
| Agnostic | 62.55 | 12.25 |
| Clinical diagnosis | ||
| Lung | 62.62 | 12.47 |
| Pancreas | 62.13 | 13.59 |
| Colorectal | 56.74 | 14.53 |
| Uterus | 50.50 | 12.02 |
| Breast | 63.17 | 19.83 |
| Stomach | 73.67 | 9.71 |
| Prostate | 62.17 | 12.31 |
| Others | 64.83 | 23.19 |
| Non-Hodgkin’s lymphoma | 64.40 | 11.86 |
| Hodgkin’s lymphoma | 60.00 | 25.45 |
| Multiple myeloma | 58.33 | 16.07 |
| Testicles | 50.00 | |
| Liver | 59.00 |
| Item | SDS Items in English | SDS Items in European Portuguese | M (Range of Values: 1–5) | s |
|---|---|---|---|---|
| Domain: Relationship with self | Domínio: Relação com o próprio | 2.08 | 0.85 | |
| 1 | I feel shock | Sinto-me em choque | 1.90 | 0.86 |
| 2 | I feel denial | Sinto-me em negação | 1.99 | 0.94 |
| 3 | I feel fear | Sinto-me com medo | 2.41 | 0.77 |
| 4 | I feel suffering | Sinto-me em sofrimento | 2.38 | 0.98 |
| 5 | I feel sorrow | Sinto mágoa | 1.87 | 0.82 |
| 6 | I feel loneliness | Sinto solidão | 1.99 | 0.87 |
| 7 | I feel numb | Sinto entorpecimento (dormente) | 1.89 | 0.82 |
| 8 | I feel regret | Sinto arrependimento | 1.95 | 0.80 |
| 9 | I feel discontented | Sinto descontentamento | 2.21 | 0.89 |
| 10 | I feel worry | Sinto preocupação | 2.70 | 0.88 |
| 11 | I feel fatalism | Sinto fatalismo | 1.95 | 0.80 |
| 12 | I feel like giving up the life | Sinto vontade de desistir da vida | 1.61 | 0.71 |
| 13 | I feel pessimistic | Sinto-me pessimista | 2.21 | 0.86 |
| 14 | I feel something in my mind | Sinto algo na minha mente | 2.00 | 0.81 |
| Domain: relationship with others | Domínio: Relação com os outros | 2.15 | 0.80 | |
| 15 | I cannot be satisfied by others | Não consigo ser satisfeito por outros | 1.97 | 0.71 |
| 16 | I cannot trust others | Não consigo confiar nos outros | 2.44 | 0.80 |
| 17 | I cannot obey others | Não consigo obedecer aos outros | 2.27 | 0.71 |
| 18 | I cannot forgive others | Não consigo perdoar os outros | 2.13 | 0.87 |
| 19 | I feel alienated from others | Sinto-me alienado (distante) dos outros | 1.96 | 0.89 |
| Domain: Relationship with God | Domínio: Relação com Deus | 2.03 | 0.95 | |
| 20 | I feel no respect for God | Não sinto respeito por Deus | 1.73 | 1.07 |
| 21 | I feel God is powerless | Sinto que Deus é impotente | 2.13 | 1.12 |
| 22 | I feel no protection from my ancestors | Sinto que não sou protegido pelos meus antepassados | 1.90 | 0.94 |
| 23 | I feel tied up by my faith | Sinto-me preso pela minha fé | 1.61 | 0.75 |
| 24 | I feel sinful | Sinto-me pecador | 2.43 | 0.74 |
| 25 | I feel no peace of mind | Não sinto paz de espírito | 2.08 | 0.87 |
| 26 | I cannot attend religious activities | Não consigo participar em atividades religiosas | 2.35 | 1.14 |
| Domain: Facing death | Domínio: Encarar a morte | 1.89 | 0.87 | |
| 27 | I am afraid to discuss death | Tenho medo de conversar sobre a morte | 2.08 | 0.95 |
| 28 | I worry about my dying situation | Preocupo-me com a situação da minha morte | 2.16 | 0.93 |
| 29 | I worry about my dying ceremony | Preocupo-me com a minha cerimónia fúnebre | 1.58 | 0.75 |
| 30 | I worry about where I am going after death | Preocupo-me para onde vou depois de morrer | 1.72 | 0.84 |
| Variable | Initial | Extraction |
|---|---|---|
| SDS 1 (shock) | 1.00 | 0.74 |
| SDS 2 (denial) | 1.00 | 0.55 |
| SDS 3 (fear) | 1.00 | 0.61 |
| SDS 4 (suffering) | 1.00 | 0.67 |
| SDS 5 (sorrow) | 1.00 | 0.49 |
| SDS 6 (loneliness) | 1.00 | 0.71 |
| SDS 7 (numb) | 1.00 | 0.73 |
| SDS 8 (regret) | 1.00 | 0.51 |
| SDS 9 (discontented) | 1.00 | 0.62 |
| SDS 10 (worry) | 1.00 | 0.58 |
| SDS 11 (fatalism) | 1.00 | 0.72 |
| SDS 12 (giving up) | 1.00 | 0.56 |
| SDS 13 (pessimistic) | 1.00 | 0.60 |
| SDS 14 (my mind) | 1.00 | 0.50 |
| SDS 15 (satisfied by others) | 1.00 | 0.51 |
| SDS 16 (trust others) | 1.00 | 0.51 |
| SDS 17 (obey others) | 1.00 | 0.58 |
| SDS 18 (forgive others) | 1.00 | 0.62 |
| SDS 19 (alienated) | 1.00 | 0.75 |
| SDS 20 (respect for God) | 1.00 | 0.73 |
| SDS 21 (God is powerless) | 1.00 | 0.59 |
| SDS 22(my ancestors) | 1.00 | 0.52 |
| SDS 23 (faith) | 1.00 | 0.40 |
| SDS 24 (sinful) | 1.00 | 0.54 |
| SDS 25 (peace of mind) | 1.00 | 0.60 |
| SDS 26 (religious activities) | 1.00 | 0.60 |
| SDS 27 (discuss death) | 1.00 | 0.71 |
| SDS 28 (dying situation) | 1.00 | 0.57 |
| SDS 29 (dying ceremony) | 1.00 | 0.75 |
| SDS 30 (after death) | 1.00 | 0.75 |
| Components | ||||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |
| SDS 1 (shock) | 0.70 | 0.46 | 0.05 | 0.16 | 0.06 | 0.14 |
| SDS 2 (denial) | 0.68 | 0.28 | −0.03 | 0.17 | 0.04 | 0.08 |
| SDS 3 (fear) | 0.74 | 0.04 | −0.18 | 0.03 | 0.14 | −0.14 |
| SDS 4 (suffering) | 0.71 | 0.26 | −0.13 | 0.02 | −0.04 | 0.30 |
| SDS 5 (sorrow) | 0.38 | 0.37 | 0.11 | 0.44 | 0.08 | 0.02 |
| SDS 6 (loneliness) | 0.39 | 0.20 | 0.08 | 0.72 | −0.02 | 0.04 |
| SDS 7 (numb) | 0.678 | 0.39 | 0.10 | 0.28 | 0.03 | 0.18 |
| SDS 8 (regret) | 0.33 | 0.19 | −0.05 | 0.32 | 0.31 | 0.42 |
| SDS 9 (discontented) | 0.71 | 0.09 | 0.07 | 0.26 | 0.21 | −0.01 |
| SDS 10 (worry) | 0.70 | −0.05 | −0.02 | 0.16 | 0.27 | −0.05 |
| SDS 11 (fatalism) | 0.72 | 0.32 | 0.11 | 0.25 | −0.03 | 0.16 |
| SDS 12 (giving up) | 0.54 | 0.38 | 0.19 | 0.29 | −0.08 | −0.05 |
| SDS 13 (pessimistic) | 0.69 | 0.24 | 0.11 | 0.18 | −0.05 | −0.13 |
| SDS 14 (my mind) | 0.57 | 0.19 | 0.27 | 0.20 | 0.18 | −0.01 |
| SDS 15 (satisfied by others) | 0.25 | 0.20 | 0.28 | 0.33 | 0.43 | −0.21 |
| SDS 16 (trust others) | 0.08 | −0.20 | 0.13 | 0.23 | 0.62 | −0.14 |
| SDS 17 (obey others) | −0.02 | 0.17 | 0.01 | −0.06 | 0.72 | 0.23 |
| SDS 18 (forgive others) | 0.27 | 0.18 | 0.11 | −0.03 | 0.67 | 0.27 |
| SDS 19 (alienated) | 0.30 | 0.09 | 0.16 | 0.76 | 0.04 | 0.22 |
| SDS 20 (respect for God) | 0.00 | −0.11 | 0.831 | 0.16 | 0.05 | −0.04 |
| SDS 21 (God is powerless) | −0.01 | −0.08 | 0.75 | 0.12 | 0.13 | −0.04 |
| SDS 22(my ancestors) | 0.18 | 0.03 | 0.63 | −0.09 | 0.06 | 0.29 |
| SDS 23 (faith) | 0.22 | 0.16 | −0.14 | 0.47 | 0.22 | −0.21 |
| SDS 24 (sinful) | −0.05 | 0.04 | 0.04 | 0.03 | 0.12 | 0.73 |
| SDS 25 (peace of mind) | 0.59 | −0.03 | 0.25 | 0.21 | 0.33 | −0.20 |
| SDS 26 (religious activities) | −0.01 | 0.26 | 0.73 | −0.06 | 0.00 | −0.05 |
| SDS 27 (discuss death) | 0.34 | 0.73 | −0.03 | 0.04 | 0.25 | −0.06 |
| SDS 28 (dying situation) | 0.39 | 0.63 | 0.02 | 0.13 | 0.08 | −0.03 |
| SDS 29 (dying ceremony) | 0.15 | 0.83 | 0.06 | 0.13 | −0.14 | 0.05 |
| SDS 30 (after death) | 0.15 | 0.83 | −0.01 | 0.15 | 0.07 | 0.16 |
| Components | ||||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| SDS 1 (shock) | 0.67 | 0.50 | 0.02 | 0.11 |
| SDS 2 (denial) | 0.65 | 0.32 | −0.05 | 0.06 |
| SDS 3 (fear) | 0.70 | 0.02 | −0.21 | 0.03 |
| SDS 4 (suffering) | 0.58 | 0.38 | −0.18 | 0.09 |
| SDS 5 (sorrow) | 0.53 | 0.35 | 0.16 | 0.07 |
| SDS 6 (loneliness) | 0.63 | 0.22 | 0.16 | −0.03 |
| SDS 7 (numb) | 0.69 | 0.45 | 0.09 | 0.09 |
| SDS 8 (regret) | 0.40 | 0.24 | −0.02 | 0.45 |
| SDS 9 (discontented) | 0.76 | 0.09 | 0.06 | 0.14 |
| SDS 10 (worry) | 0.72 | −0.06 | −0.04 | 0.17 |
| SDS 11 (fatalism) | 0.71 | 0.40 | 0.08 | 0.03 |
| SDS 12 (giving up) | 0.59 | 0.40 | 0.19 | −0.10 |
| SDS 13 (pessimistic) | 0.70 | 0.25 | 0.08 | −0.12 |
| SDS 14 (my mind) | 0.61 | 0.17 | 0.26 | 0.12 |
| SDS 15 (satisfied by others) | 0.44 | 0.05 | 0.33 | 0.27 |
| SDS 16 (trust others) | 0.26 | −0.35 | 0.18 | 0.45 |
| SDS 17 (obey others) | 0.02 | 0.01 | 0.03 | 0.75 |
| SDS 18 (forgive others) | 0.27 | 0.08 | 0.11 | 0.71 |
| SDS 19 (alienated) | 0.55 | 0.15 | 0.25 | 00.09 |
| SDS 20 (respect for God) | 0.07 | −0.12 | 0.84 | −0.01 |
| SDS 21 (God is powerless) | 0.05 | −0.11 | 0.75 | 0.06 |
| SDS 22(my ancestors) | 0.08 | 0.11 | 0.57 | 0.16 |
| SDS 23 (faith) | 0.45 | 0.05 | −0.05 | 0.09 |
| SDS 24 (sinful) | −0.13 | 0.20 | 0.03 | 0.43 |
| SDS 25 (peace of mind) | 0.68 | −0.11 | 0.25 | 0.15 |
| SDS 26 (religious activities) | −0.02 | 0.22 | 0.71 | −0.02 |
| SDS 27 (discuss death) | 0.37 | 0.63 | −0.01 | 0.23 |
| SDS 28 (dying situation) | 0.41 | 0.59 | 0.03 | 0.09 |
| SDS 29 (dying ceremony) | 0.17 | 0.82 | 0.08 | −0.04 |
| SDS 30 (after death) | 0.67 | 0.50 | 0.02 | 0.11 |
| Scale M if Item Deleted | Scale Variance if Item Deleted | Corrected Item-Total Correlation | Squared Multiple Correlation | Cronbach’s Alpha If Item Deleted | |
|---|---|---|---|---|---|
| SDS 1 (shock) | 59.67 | 175.47 | 0.75 | 0.82 | 0.90 |
| SDS 2 (denial) | 59.58 | 176.98 | 0.62 | 0.61 | 0.90 |
| SDS 3 (fear) | 59.17 | 182.70 | 0.48 | 0.54 | 0.90 |
| SDS 4 (suffering) | 59.19 | 177.99 | 0.55 | 0.56 | 0.90 |
| SDS 5 (sorrow) | 59.71 | 179.53 | 0.60 | 0.49 | 0.90 |
| SDS 6 (loneliness) | 59.59 | 178.63 | 0.60 | 0.64 | 0.90 |
| SDS 7 (numb) | 59.69 | 176.08 | 0.76 | 0.80 | 0.90 |
| SDS 8 (regret) | 59.63 | 182.12 | 0.49 | 0.47 | 0.90 |
| SDS 9 (discontented) | 59.37 | 176.61 | 0.67 | 0.60 | 0.90 |
| SDS 10 (worry) | 58.87 | 179.58 | 0.55 | 0.55 | 0.90 |
| SDS 11 (fatalism) | 59.62 | 176.78 | 0.74 | 0.72 | 0.90 |
| SDS 12 (giving up) | 59.97 | 180.66 | 0.64 | 0.60 | 0.90 |
| SDS 13 (pessimistic) | 59.37 | 178.18 | 0.62 | 0.58 | 0.90 |
| SDS 14 (my mind) | 59.57 | 178.82 | 0.63 | 0.58 | 0.90 |
| SDS 15 (satisfied by others) | 59.61 | 183.08 | 0.50 | 0.49 | 0.90 |
| SDS 16 (trust others) | 59.13 | 188.21 | 0.20 | 0.33 | 0.91 |
| SDS 17 (obey others) | 59.30 | 189.12 | 0.19 | 0.28 | 0.91 |
| SDS 18 (forgive others) | 59.45 | 182.49 | 0.43 | 0.43 | 0.91 |
| SDS 19 (alienated) | 59.61 | 179.08 | 0.56 | 0.62 | 0.90 |
| SDS 20 (respect for God) | 59.84 | 185.92 | 0.21 | 0.61 | 0.91 |
| SDS 21 (God is powerless) | 59.44 | 185.83 | 0.20 | 0.50 | 0.91 |
| SDS 22 (my ancestors) | 59.67 | 184.94 | 0.29 | 0.35 | 0.91 |
| SDS 23 (faith) | 59.97 | 185.64 | 0.35 | 0.30 | 0.91 |
| SDS 24 (sinful) | 59.15 | 191.18 | 0.08 | 0.20 | 0.91 |
| SDS 25 (peace of mind) | 59.49 | 179.08 | 0.58 | 0.57 | 0.90 |
| SDS 26 (religious activities) | 59.23 | 184.79 | 0.23 | 0.37 | 0.91 |
| SDS 27 (discuss death) | 59.49 | 177.71 | 0.58 | 0.60 | 0.90 |
| SDS 28 (dying situation) | 59.41 | 178.04 | 0.58 | 0.58 | 0.90 |
| SDS 29 (dying ceremony) | 59.99 | 183.63 | 0.45 | 0.71 | 0.90 |
| SDS 30 (after death) | 59.85 | 181.09 | 0.51 | 0.72 | 0.90 |
| Domains | Cronbach’s α |
|---|---|
| Relationship with self | 0.92 |
| Relationship with others | 0.63 |
| Relationship with God | 0.64 |
| Facing death | 0.85 |
| Domains | Facing Death Domain | Relationship with Others Domain | Relationship with God Domain | Relationship with Self Domain |
|---|---|---|---|---|
| Facing death domain | - | |||
| Relationship with others domain | 0.30 ** | - | ||
| Relationship with God domain | 0.20 * | 0.43 ** | - | |
| Relationship with self domain | 0.62 ** | 0.52 ** | 0.33 ** | - |
| Domains | Personal Domain | Communal Domain | Environmental Domain | Transcendental Domain | Score SWBQ | Score SDS |
|---|---|---|---|---|---|---|
| Personal domain | - | |||||
| Communal domain | 0.67 ** | - | ||||
| Environmental domain | 0.24 ** | 0.39 ** | - | |||
| Transcendental domain | 0.20 * | 0.26 ** | 0.19 * | - | ||
| Score SWBQ | 0.64 ** | 0.72 ** | 0.67 ** | 0.72 ** | - | |
| Score SDS | −0.52 ** | −0.25 ** | 0.018 | −0.11 | −0.26 ** | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martins, H.; Caldeira, S.; Dias Domingues, T.; Vieira, M.; Ku, Y.-L. Validation of the Spiritual Distress Scale in Portuguese Cancer Patients Undergoing Chemotherapy: A Methodological Study. Religions 2019, 10, 599. https://doi.org/10.3390/rel10110599
Martins H, Caldeira S, Dias Domingues T, Vieira M, Ku Y-L. Validation of the Spiritual Distress Scale in Portuguese Cancer Patients Undergoing Chemotherapy: A Methodological Study. Religions. 2019; 10(11):599. https://doi.org/10.3390/rel10110599
Chicago/Turabian StyleMartins, Helga, Sílvia Caldeira, Tiago Dias Domingues, Margarida Vieira, and Ya-Lie Ku. 2019. "Validation of the Spiritual Distress Scale in Portuguese Cancer Patients Undergoing Chemotherapy: A Methodological Study" Religions 10, no. 11: 599. https://doi.org/10.3390/rel10110599
APA StyleMartins, H., Caldeira, S., Dias Domingues, T., Vieira, M., & Ku, Y. -L. (2019). Validation of the Spiritual Distress Scale in Portuguese Cancer Patients Undergoing Chemotherapy: A Methodological Study. Religions, 10(11), 599. https://doi.org/10.3390/rel10110599