
Religious Views of Suffering Profile Groups during COVID-19


Abstract
:1. Introduction
1.1. COVID-19 Stress and Anxiety
1.2. Religious Commitment and Well-Being
1.3. Meaning-Making
1.4. Theodicy
1.5. The Views of Suffering Scale (VOSS)
1.6. Theodicy and Well-Being
1.7. The Current Study
2. Results
2.1. Participants
2.2. Data Analysis Plan
2.3. Descriptive Statistics
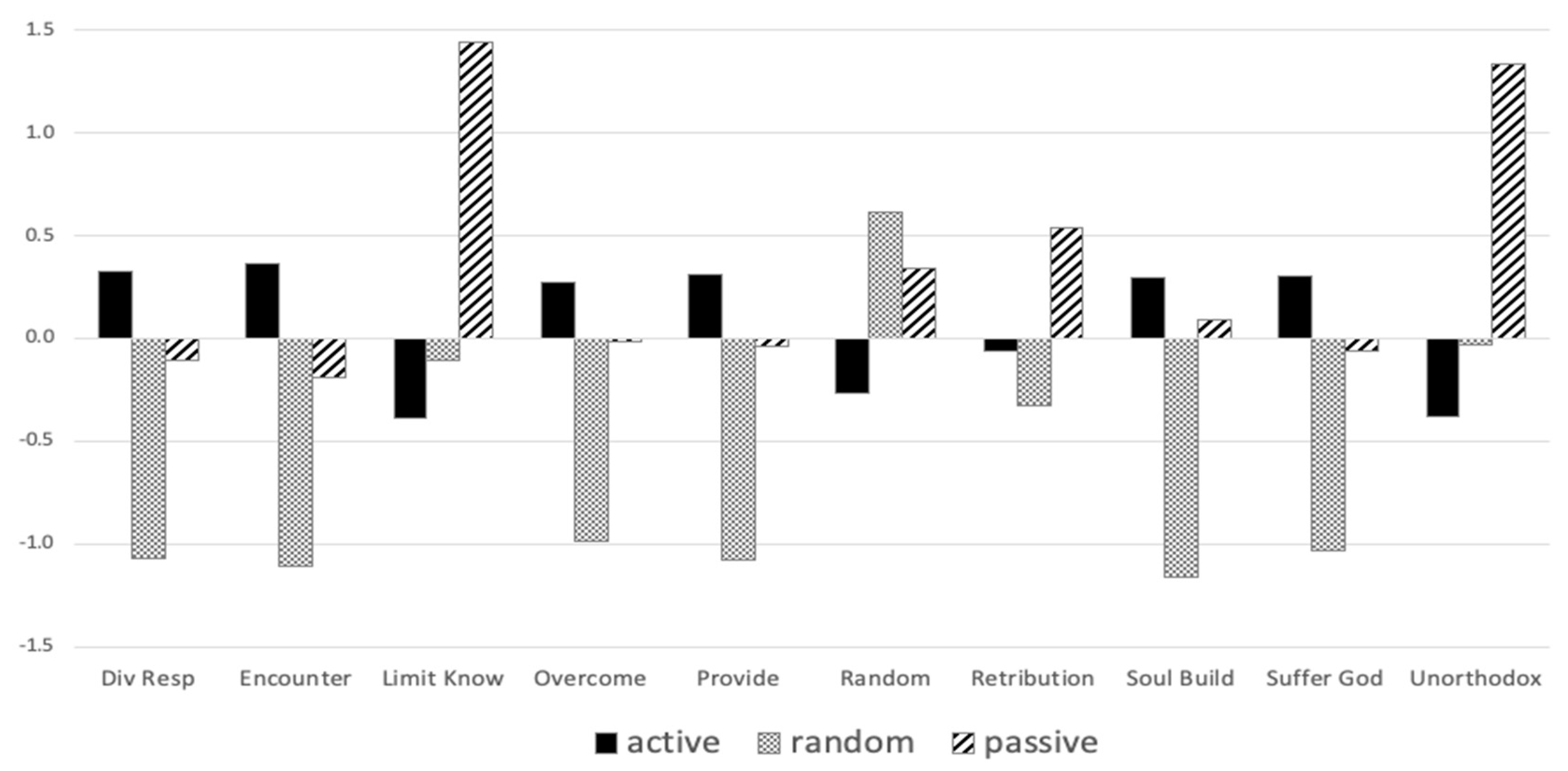
2.4. Cluster Analysis
2.5. Analyses of Variances
3. Discussion
3.1. Cluster Profiles
3.2. Views of Suffering and Adjustment
Generally, this sanctification has taken the form of seeing suffering as being permitted by God or in God’s will (e.g., Job 1:12, 2:6), as being used for God’s purposes (e.g., to increase perseverance; Romans 5:3–5; James 1:2–4), or as directing one toward God or connecting one with God (e.g., Philippians 3:10–11).(p. 798)
3.3. Limitations and Future Directions
3.4. Practical Implications
4. Materials and Methods
4.1. Procedure
4.2. Measures
4.2.1. Views of Suffering
4.2.2. Religious Commitment
4.2.3. COVID-19 Stress
4.2.4. General Anxiety
4.2.5. Mental Well-Being
4.3. Statistical Software
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- APA (American Psychological Association). 2020. Stress in America 2020: Stress in the Time of COVID-19, Volume One. Available online: https://www.apa.org (accessed on 2 January 2022).
- Beck, Richard, and Sara Taylor. 2008. The emotional burden of monotheism: Satan, theodicy, and relationship with God. Journal of Psychology and Theology 36: 151–60. [Google Scholar] [CrossRef]
- Boals, Adriel, and Jonathan B. Banks. 2020. Stress and cognitive functioning during a pandemic: Thoughts from stress researchers. Psychological Trauma: Theory, Research, Practice, and Policy 12: S255–S257. [Google Scholar] [CrossRef]
- Büssing, Arndt, Thomas Ostermann, and Peter F. Matthiessen. 2005. The Role of Religion and Spirituality in Medical Patients in Germany. Journal of Religion and Health 44: 321–40. [Google Scholar] [CrossRef]
- CDC (Centers for Disease Control and Prevention). 2020a. Guidelines: Opening Up America Again. White House. Available online: https://www.whitehouse.gov/openingamerica/ (accessed on 2 January 2022).
- CDC (Centers for Disease Control and Prevention). 2020b. Mental Health: Household Pulse Survey. National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/covid19/pulse/mental-health.htm (accessed on 2 January 2022).
- Czeisler, Mark É., Kristy Marynak, Kristie E. Clarke, Zainab Salah, Iju Shakya, Joann M. Thierry, Nida Ali, Hannah McMillan, Joshua F. Wiley, Matthew D. Weaver, and et al. 2020. Delay or avoidance of medical care because of COVID-19–related concerns—United States, June 2020. Morbidity and Mortality Weekly Report 69: 1250–57. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, Timothy K., Aimee M. West, Melissa E. Williams, and Jakob M Brockman. 2009. Measuring theodicy: Individual differences in the perception of divine intervention. Pastoral Psychology 58: 43–47. [Google Scholar] [CrossRef]
- Edmondson, Donald, Crystal L. Park, Stephenie R. Chaudoir, and Jennifer H. Wortmann. 2008. Death Without God: Religious Struggle, Death Concerns, and Depression in the Terminally III. Psychological Science 19: 754–58. [Google Scholar] [CrossRef]
- Eriksson, Cynthia B., and Dow-Ann Yeh. 2012. Grounded transcendence: Resilience to trauma through spirituality and religion. In Individual Ttrauma: Recovering from Deep Wounds and Exploring the Potential for Renewal. Edited by Kathryn Gow and Marek J. Celinski. New York: Nova Science Publishers, pp. 53–71. [Google Scholar]
- Furnham, Adrian, and Laurence B. Brown. 1992. Theodicy: A neglected aspect of the psychology of religion. The International Journal for the Psychology of Religion 2: 37–45. [Google Scholar] [CrossRef]
- Gallup Inc. 2021. Religion. Available online: https://news.gallup.com/poll/1690/Religion.aspx (accessed on 2 January 2022).
- Greenberg, Jeff, Sheldon Solomon, and Tom Pyszczynski. 1997. Terror management theory of self-esteem and cultural worldviews: Empirical assessments and conceptual refinements. Advances in Experimental Social Psychology 29: 61–139. [Google Scholar] [CrossRef]
- Hair, Joseph, and William C. Black. 2000. Cluster analysis. In Reading and Understanding More Multivariate Statistics. Edited by Laurence G. Grimm and Paul R. Yarnold. Washington: American Psychological Association, pp. 147–205. [Google Scholar]
- Hale-Smith, Amy, Crystal L. Park, and Donal Edmondson. 2012. Measuring beliefs about suffering: Development of the Views of Suffering Scale. Psychological Assessment 24: 855–66. [Google Scholar] [CrossRef] [Green Version]
- Hall, M. Elizabeth, and Peter Hill. 2019. Meaning-making, suffering, and religion: A worldview conception. Mental Health, Religion & Culture 22: 467–79. [Google Scholar]
- Hall, M. Elizabeth Lewis, Jason McMartin, David Wang, Laura Shannonhouse, Jamie D. Aten, Eric J. Silverman, and Lauren A. Decker. 2021. The Christian Sanctification of Suffering Scale: Measure development and relationship to well-being. Mental Health, Religion & Culture 24: 796–813. [Google Scholar]
- Harapan, Harapan, Naoya Itoh, Amanda Yufika, Wira Winardi, Synat Keam, Haypheng Te, Dewi Megawati, Zinatul Hayati, Abram L. Wagner, and Mudatsir Mudatsir. 2020. Coronavirus disease 2019 (COVID-19): A literature review. Journal of Infection and Public Health 13: 667–73. [Google Scholar] [CrossRef]
- Harris, J. Irene, Timothy Usset, and Zhen H. Cheng. 2018. Theodicy and spiritual distress among veterans managing posttraumatic stress. Spirituality in Clinical Practice 5: 240–50. [Google Scholar] [CrossRef]
- Hart, Curtis W., and Harold G. Koenig. 2020. Religion and health during the COVID-19 pandemic. Journal of Religion and Health 59: 1141–43. [Google Scholar] [CrossRef]
- Haver, Annie, Kristin Akerjordet, Peter Caputi, Trude Furunes, and Christopher Magee. 2015. Measuring mental well-being: A validation of the Short Warwick–Edinburgh Mental Well-Being Scale in Norwegian and Swedish. Scandinavian Journal of Public Health 43: 721–27. [Google Scholar] [CrossRef]
- Horesh, Danny, and Adam D. Brown. 2020. Traumatic stress in the age of COVID-19: A call to close critical gaps and adapt to new realities. Psychological Trauma: Theory, Research, Practice, and Policy 12: 331–35. [Google Scholar] [CrossRef]
- Ishikawa, Rachel Zack. 2020. I may never see the ocean again: Loss and grief among older adults during the COVID-19 pandemic. Psychological Trauma: Theory, Research, Practice, and Policy 12: S85–86. [Google Scholar] [CrossRef]
- Jonas, Eva, and Peter Fischer. 2006. Terror management and religion: Evidence that intrinsic religiousness mitigates worldview defense following mortality salience. Journal of Personality and Social Psychology 91: 553–67. [Google Scholar] [CrossRef]
- Koenig, Harold G., and Arndt Büssing. 2010. The Duke University Religion Index (DUREL): A five-Item measure for use in epidemiological studies. Religions 1: 78–85. [Google Scholar] [CrossRef] [Green Version]
- Lee, Bruce Y., and Andrew B. Newberg. 2005. Religion and Health: A Review and Critical Analysis. Zygon 40: 443–68. [Google Scholar] [CrossRef]
- Lim, Chaeyoon, and Robert D. Putnam. 2010. Religion, social networks, and life satisfaction. American Sociological Review 75: 914–33. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, Peter F., and Sydney H. Lovibond. 1995. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy 33: 335–43. [Google Scholar] [CrossRef]
- McElroy-Heltzel, Stacey E., Edward B. Davis, Don E. Davis, Jamie D. Aten, Joshua N. Hook, Daryl R. Van Tongeren, and Jenny Hwang. 2018. Benevolent theodicies protect against PTSD following a natural disaster. Journal of Psychology and Christianity 37: 6–16. [Google Scholar]
- NFDA (National Funeral Directors Association). 2020. Situation Update: Novel Coronavirus (COVID-19). Available online: https://www.nfda.org/covid-19 (accessed on 2 January 2022).
- Oman, Doug, and Carl E. Thoresen. 2005. Do religion and spirituality influence health. In Handbook of the Psychology of Religion and Spirituality. Edited by Raymond F. Paloutzian and Crystal L. Park. New York: Guilford Press, pp. 435–59. [Google Scholar]
- Pargament, Kenneth I., Nalini Tarakeshwar, Christopher G. Ellison, and Keith M. Wulff. 2001. Religious coping among the religious: The relationships between religious coping and well-being in a national sample of Presbyterian clergy, elders, and members. Journal for the Scientific Study of Religion 40: 497–513. [Google Scholar] [CrossRef]
- Park, Crystal L. 2005. Religion as a meaning-making framework in coping with life stress. Journal of Social Issues 61: 707–29. [Google Scholar] [CrossRef]
- Park, Crystal L. 2010. Making sense of the meaning literature: An integrative review of meaning making and its effects on adjustment to stressful life events. Psychological Bulletin 136: 257–301. [Google Scholar] [CrossRef]
- Park, Crystal L., and Susan Folkman. 1997. Meaning in the context of stress and coping. Review of General Psychology 1: 115–44. [Google Scholar] [CrossRef]
- Park, Crystal L., Joseph M. Currier, J. Irene Harris, and Jeanne M. Slattery. 2017. Trauma, Meaning, and Spirituality: Translating Research into Clinical Practice. Washington: American Psychological Association. [Google Scholar]
- Park, Crystal L., Beth S. Russell, Michael Fendrich, Lucy Finkelstein-Fox, Morica Hutchison, and Jessica Becker. 2020. Americans’ COVID-19 stress, coping, and adherence to CDC guidelines. Journal of General Internal Medicine 35: 2296–303. [Google Scholar] [CrossRef]
- PeConga, Emma K., Gabrielle M. Gauthier, Ash Holloway, Rosemary S. W. Walker, Peter L. Rosencrans, Lori A. Zoellner, and Michele Bedard-Gilligan. 2020. Resilience is spreading: Mental health within the COVID-19 pandemic. Psychological Trauma: Theory, Research, Practice, and Policy 12: S47–S48. [Google Scholar] [CrossRef]
- Pew Research Center. 2020. Most Americans Say Coronavirus Outbreak Has Impacted Their Lives. Social & Demographic Trends. Available online: https://www.pewsocialtrends.org/2020/03/30/most-americans-say-coronavirus-outbreak-has-impacted-their-lives/ (accessed on 2 January 2022).
- Roberto, Anka, Alicia Sellon, Sabrina T. Cherry, Josalin Hunter-Jones, and Heidi Winslow. 2020. Impact of spirituality on resilience and coping during the COVID-19 crisis: A mixed-method approach investigating the impact on women. Health Care for Women International 41: 1313–34. [Google Scholar] [CrossRef]
- Rubin, G. James, Richard Amlôt, Lisa Page, and Simon Wessely. 2009. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: Cross sectional telephone survey. BMJ 339: b2651. [Google Scholar] [CrossRef] [Green Version]
- Seryczyńska, Berenika, Lluis Oviedo, Piotr Roszak, Suvi-Maria Katariina Saarelainen, Hilla Inkilä, Josefa Torralba Albaladejo, and Francis-Vincent Anthony. 2021. Religious capital as a central factor in coping with the COVID-19: Clues from an international survey. European Journal of Science and Theology 17: 67–81. [Google Scholar]
- Sharp, Shane. 2014. Monotheistic theodicy as imaginary face-work. Sociological Forum 29: 873–92. [Google Scholar] [CrossRef]
- Singhal, Tanu. 2020. A review of coronavirus disease-2019 (COVID-19). The Indian Journal of Pediatrics 87: 281–86. [Google Scholar] [CrossRef] [Green Version]
- Taylor, Steven, Caeleigh A. Landry, Michelle M. Paluszek, Thomas A. Fergus, Dean McKay, and Gordon J. G. Asmundson. 2020. Development and initial validation of the COVID Stress Scales. Journal of Anxiety Disorders 72: 102232. [Google Scholar] [CrossRef]
- Tennant, Ruth, Louise Hiller, Ruth Fishwick, Stephen Platt, Stephen Joseph, Scott Weich, Jane Parkinson, Jenny Secker, and Sarah Stewart-Brown. 2007. The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health and Quality of life Outcomes 5: 1–13. [Google Scholar] [CrossRef] [Green Version]
- Van Tongeren, Daryl R., Mark Sanders, Megan Edwards, Edward B. Davis, Jamie D. Aten, Jennifer M. Ranter, and Angela Tsarouhis. 2019. Religious and spiritual struggles alter god representations. Psychology of Religion and Spirituality 11: 225–32. [Google Scholar] [CrossRef]
- Van Tongeren, Daryl R., Jeffrey D. Green, and Taylor Richmond. 2021. In the valley of the shadow of death: The existential benefits of imbuing life and death with meaning. Psychology of Religion and Spirituality. Advance online publication. [Google Scholar] [CrossRef]
- Vázquez Bandín, Carmen. 2020. Only the living can witness the passing of death: Mourning in times of pandemic. The Humanistic Psychologist 48: 357–62. [Google Scholar] [CrossRef]
- Wang, Lisheng, Yiru Wang, Dawei Ye, and Qingquan Liu. 2020. A review of the 2019 Novel Coronavirus (COVID-19) based on current evidence. International Journal of Antimicrobial Agents 55: 105948. [Google Scholar] [CrossRef]
- Wang, Kenneth T., Miriam S. Kang, Hsiu-Chi Lee, and Irene Sipan. 2021. The Religious Perfectionism Scale: A cross-cultural psychometric evaluation among Christians in the United States. Journal of Psychology and Theology. Advance online publication. [Google Scholar] [CrossRef]
- Watts, Stéphanie, André Marchand, Stéphanie Bouchard, Patrick Gosselin, Frédéric Langlois, Geneviéve Belleville, and Michel J. Dugas. 2020. Telepsychotherapy for generalized anxiety disorder: Impact on the working alliance. Journal of Psychotherapy Integration 30: 208–25. [Google Scholar] [CrossRef]
- Wheaton, Michael G., Jonathan S. Abramowitz, Noah C. Berman, Laura E. Fabricant, and Bumi O Olatunji. 2012. Psychological predictors of anxiety in response to the H1N1 (swine flu) pandemic. Cognitive Therapy and Research 36: 210–18. [Google Scholar] [CrossRef]
- WHO (World Health Organization). 2020. Coronavirus Disease (COVID-19): Situation Report, 162. Available online: https://apps.who.int/iris/handle/10665/332970 (accessed on 2 January 2022).
- Wilt, Joshua A., Julie J. Exline, Joshua B. Grubbs, Crystal C. Park, and Kenneth I. Pargament. 2016. God’s role in suffering: Theodicies, divine struggle, and mental health. Psychology of Religion and Spirituality 8: 352–62. [Google Scholar] [CrossRef]
- Wilt, Joshua A., Julie J. Exline, Matthew J. Lindberg, Crystal L. Park, and Kenneth I. Pargament. 2017. Theological beliefs about suffering and interactions with the divine. Psychology of Religion and Spirituality 9: 137–47. [Google Scholar] [CrossRef]
- Yonker, Julie E., Chelsea A. Schnabelrauch, and Laura G. DeHaan. 2012. The relationship between spirituality and religiosity on psychological outcomes in adolescents and emerging adults: A meta-analytic review. Journal of Adolescence 35: 299–314. [Google Scholar] [CrossRef]


{kind=link}
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Div Resp | 0.37 | |||||||||||||
| 2 | Encounter | 0.45 | 0.60 | ||||||||||||
| 3 | Limit Know | −0.10 | −0.01 | 0.82 | |||||||||||
| 4 | Overcome | 0.26 | 0.32 | 0.05 | 0.66 | ||||||||||
| 5 | Provide | 0.39 | 0.37 | −0.02 | 0.33 | 0.78 | |||||||||
| 6 | Random | −0.19 | −0.12 | 0.22 | −0.13 | −0.19 | 0.74 | ||||||||
| 7 | Retribution | 0.11 | 0.00 | 0.20 | 0.26 | −0.04 | −0.06 | 0.65 | |||||||
| 8 | Soul Build. | 0.49 | 0.41 | −0.01 | 0.34 | 0.54 | −0.21 | 0.13 | 0.86 | ||||||
| 9 | Suffer God | 0.41 | 0.52 | 0.08 | 0.36 | 0.32 | −0.11 | 0.02 | 0.30 | 0.85 | |||||
| 10 | Unorthodox | −0.15 | −0.17 | 0.42 | −0.12 | −0.02 | 0.10 | 0.17 | −0.04 | −0.24 | 0.58 | ||||
| 11 | DUREL | 0.51 | 0.46 | −0.28 | 0.24 | 0.28 | −0.25 | −0.16 | 0.27 | 0.47 | −0.42 | 0.85 | |||
| 12 | COVID | −0.10 | −0.06 | 0.01 | −0.20 | −0.22 | 0.14 | −0.05 | −0.17 | 0.02 | 0.05 | −0.17 | 0.88 | ||
| 13 | Anxiety | −0.13 | 0.02 | 0.23 | −0.04 | −0.09 | 0.21 | 0.04 | −0.01 | 0.02 | 0.10 | −0.21 | 0.30 | 0.81 | |
| 14 | Well-being | 0.25 | 0.04 | −0.06 | 0.16 | 0.09 | −0.24 | −0.02 | 0.00 | 0.07 | −0.03 | 0.25 | −0.22 | −0.44 | 0.80 |
| Mean | 12.17 | 12.68 | 4.27 | 8.94 | 9.57 | 8.65 | 5.79 | 11.10 | 13.37 | 3.86 | 4.03 | 26.99 | 3.17 | 23.92 | |
| S.D. | 2.98 | 3.39 | 2.30 | 3.16 | 4.00 | 3.51 | 2.49 | 3.69 | 3.86 | 1.89 | 0.93 | 7.46 | 3.64 | 4.04 |
| Active | Random | Passive | ||||||
|---|---|---|---|---|---|---|---|---|
| n = 149 | n = 41 | n = 43 | ||||||
| Subscale | M | SD | M | SD | M | SD | F | η2 |
| DUREL | 4.38 a | 0.59 | 3.19 b | 1.12 | 3.59 c | 1.04 | 43.91 *** | 0.28 |
| COVID | 26.11 a | 7.83 | 29.66 b | 5.53 | 27.50 ab | 7.23 | 3.86 * | 0.03 |
| Anxiety | 2.64 a | 3.14 | 3.51 ab | 3.93 | 4.67 b | 4.50 | 5.68 ** | 0.05 |
| Well-being | 24.36 | 3.73 | 23.22 | 4.75 | 23.06 | 4.21 | 2.48 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, K.T.; Cowan, K.J.; Eriksson, C.B.; Januzik, M.; Conant, M.R. Religious Views of Suffering Profile Groups during COVID-19. Religions 2022, 13, 453. https://doi.org/10.3390/rel13050453
Wang KT, Cowan KJ, Eriksson CB, Januzik M, Conant MR. Religious Views of Suffering Profile Groups during COVID-19. Religions. 2022; 13(5):453. https://doi.org/10.3390/rel13050453
Chicago/Turabian StyleWang, Kenneth T., Krista J. Cowan, Cynthia B. Eriksson, Matthew Januzik, and Moriah R. Conant. 2022. "Religious Views of Suffering Profile Groups during COVID-19" Religions 13, no. 5: 453. https://doi.org/10.3390/rel13050453
APA StyleWang, K. T., Cowan, K. J., Eriksson, C. B., Januzik, M., & Conant, M. R. (2022). Religious Views of Suffering Profile Groups during COVID-19. Religions, 13(5), 453. https://doi.org/10.3390/rel13050453