1. Background
Based on the assumptions of Leventhal’s Self-Regulation Theory [
1], the individual being is an active problem solver that consciously activates efforts to modulate his thoughts, emotions and behaviours—particularly when facing illness or health affections. An important aspect for dealing with illness in terms of coping and illness interpretation are individual representations of disease. Relying on Diefenbach and Leventhal [
2,
3], there are two main types of representations,
i.e., cognitive and emotional processes. With respect to the “Transactional Model of Stress and Coping” of Park and Folkman [
4], the ability to cope with stress (including illness) requires that people can find meaning in it and recognize it as important. Taylor [
5] argued that patients with breast cancer adapted psychologically when they were able to find positive meanings in their illness.
Patients’ religiosity was found to be an important factor for individual coping strategies [
6]. Moreover, spirituality/religiosity can be seen also a resource of hope [
7,
8,
9] and transformation [
10,
11]. Wiechman and Magyar-Russell [
12] have shown that trauma survivors who use religious coping strategies show signs of posttraumatic growth’ with “greater appreciation of life and changed priorities; warmer, more intimate relations with others; a greater sense of personal strength, recognition of new possibilities, and spiritual development”.
The findings of previous studies that patients’ spirituality was related particularly with positive interpretations of illness (
i.e., illness as something of value to grown on, or as a challenge) [
13] would indicate that spirituality may influence cognitive processes related to meaning finding, and utilization of strategies to find hope despite of illness. These interpretations may be co-influenced by patients’ positive or negative emotions to God (or other transcendent resources).
The psychiatrist Lipowski [
14] described eight categories of how persons may interpret their illness (
i.e., Challenge, Value, Enemy, Punishment, Weakness, Loss, Relief, and Strategy) which may have influence on patients’ choice of coping strategies. With respect to these categories, Challenge was rated most often by British [
15], Canadian [
16], Swedish [
17] and German [
13] cancer patients, and also by British patients with chronic renal diseases [
18]. In contrast, German patients with chronic pain diseases rated their disease most often as an Adverse Interruption of life [
19]; also predominantly a-religious patients with chronic diseases (60% cancer) from Shanghai rated their disease as an Adverse Interruption or as a Threat / Enemy, but also as a Challenge [
20].
With respect to the findings described above, it is clear that a person’s spirituality/religiosity may have an influence on how her/she may see illness [
13,
21], and this may have an influence on life satisfaction, too. Yet, the underlying dimensions of spirituality/religiosity which may be related are so far unclear.
We assume that different qualities of spirituality (i.e., religious trust in God, existential search for meaning, ethical sensitivity, harmony, positive/negative emotions towards God) may be associated with different interpretations of illness, either positive or negative (i.e., illness as a value, as a chance, as a punishment etc.), and that these variables may have an influence on patients’ life satisfaction on the one hand or their (depressive) intention to escape from illness on the other hand.
Therefore we intended to analyse how patients with chronic diseases from Catholic Poland would interpret their illness, and how these specific interpretations were related to their religiosity/spirituality, their life satisfaction, and an intention to escape from illness. We hypothesize that both, the negative perceptions of illness (i.e., threat, interruption of life, punishment, failure) and also strategy associated disease perceptions (i.e., relieving break, call for help) are strongly influenced by patients’ attitudes to escape from illness rather than reframing reflective strategies, while positive disease perceptions are associated primarily with patients’ religiosity/spirituality and reflexive processes. Moreover, we assume that emotions towards God, either positive or negative, may be associated with their view of illness and also their life satisfaction, assuming that particularly negative emotions or disinterest in God would decrease life satisfaction.
3. Measures
All instruments were provided in their Polish language version.
3.1. Interpretation of Illness
The interpretation of illness was measured with 8 items according to Lipowski’s “Meaning of Illness” [
14] which were validated as a scale in patients with chronic diseases [
13]. This Interpretation of Illness Scale (IIS; Cronbach’s alpha = 0.73) includes positive interpretations (
i.e., challenge, value), strategy-associated interpretations (
i.e., relieving break of life, call for help), but also guilt-associated interpretations (
i.e., punishment, weakness/failure), and fatalistic negative interpretations (
i.e., threat/enemy, interruption of life). The items were scored on a 5-point scale from disagreement to agreement (0, does not apply at all; 1, does not truly apply; 2, don’t know (neither yes nor no); 3, applies quite a bit; 4, applies very much).
3.2. Escape from Illness
The 3-item scale Escape from Illness is an indicator of a depressive/fearful escape-avoidance strategy to deal with illness (
i.e., “fear what illness will bring”, “would like to run away from illness”, “when I wake up, I don’t know how to face the day”) [
24]. In patients with depressive and addictive diseases, the Escape scale correlates strongly positive with depressive symptoms (BDI; r = 0.57) [
25] and strongly negative with various disease acceptance styles (Büssing
et al., 2010a), while in patients with cancer Escape correlated moderately positive with anxiety (HADS, r = 0.47) and depression (HADS; r = 0.34), and negatively with SF-12’s mental health component (r = − 0.38) [
13].
The items were scored on a 5-point scale from disagreement to agreement (0, does not apply at all; (1) does not truly apply; (2) don’t know (neither yes nor no); (3) applies quite a bit; (4) applies very much). Scores > 50% indicate an intention to escape from illness.
3.3. Life Satisfaction
Life satisfaction was measured with the Brief Multidimensional Life Satisfaction Scale (BMLSS) [
26] which refers to Huebner’s “Brief Multidimensional Students” Life Satisfaction Scale’ [
27,
28]. The items of the BMLSS address intrinsic (Myself, Life in general), social (Friendships, Family life), external (Work situation, Where I live), and prospective dimensions (Financial situation, Future prospects). The internal consistency of the instrument was good (Cronbach’s alpha = 0.87) [
26]. Here we included two further items addressing patients’ health situation and their abilities to deal with daily life concerns. Each item was introduced by the phrase “I would describe my level of satisfaction as…”, and scored on a 7-point scale from dissatisfaction to satisfaction (0, terrible; 1, unhappy; 2, mostly dissatisfied; 3, mixed (about equally satisfied and dissatisfied); 4, mostly satisfied; 5, pleased; 6, delighted). The BMLSS-10 sum score refers to a 100% level (“delighted”). Scores > 50% indicate higher life satisfaction, while scores < 50% indicate dissatisfaction.
3.4. Self-Description Questionnaire of Spirituality
The Self-description Questionnaire of Spirituality (SQS) is an instrument tested first in Polish individuals [
29], and was used as an external measure sensitive for spiritual activities of Polish individuals. The scale uses originally 20 items and differentiates 3 factors,
i.e.Religious Attitudes (i.e., faith allows me to survive difficult periods in my life”. “while making decisions, I rely on my religious beliefs”, etc.)
Ethical Sensitivity (i.e., “react when someone is being hurt”, “care about other people’s situations”, etc.)
Harmony (i.e., “I am part of the world”, “while thinking about my life I experience peace and happiness”, etc.)
However, when testing this scale in our sample, explorative factor analysis indicated four main factors and some items which loaded weakly on the respective factors (< 0.5). These items were thus eliminated. The resulting 17-item version of the instrument (SQS-17) with its 2 main scales Religious Attitudes and Ethical Sensitivity, and the third scale Peace/Harmony with two sub-constructs, has a very good reliability coefficient (Cronbach’s alpha = 0.90) and explains 68% of variance. For this analysis, we used the SQS-17 version. The SQS-17 scores on a 5-point Likert scale ranging from “not at all” to “very much”. The sum of the subscales indicates overall spirituality.
3.5. Spirituality/Religiosity and a Resource
The contextual SpREUK-15 questionnaire (SpREUK; which is an acronym of the German translation of “Spiritual and Religious Attitudes in Dealing with Illness”) measures spirituality/religiosity attitudes and convictions of patients dealing with chronic diseases [
30,
31]. Referring to 15 items, it differentiates three factors,
i.e., Search, Trust and Reflection (Büssing, 2010). Confirmatory factor analysis confirmed the already established three subscales also in SpREUK’s Polish version with good internal consistency coefficients ranging from alpha 0.74 to 0.91, yet with 10 items (SpREUK-Polish) [
22]:
Search scale, or search (for support/access to spirituality/religiosity), deals with patients’ intention to find access to a spiritual or religious resource, which may be beneficial for coping with illness, and with their interest in spiritual or religious issues (insight and renewed interest).
Trust scale, or trust (in higher guidance/source), is a measure of intrinsic religiosity; the factor deals with patients’ conviction that they want to be connected with a higher source, and with their desire to be sheltered and guided by that source, whatever may happen to them, conviction that death is not an end.
Reflection scale, deals with a patient’s cognitive reappraisal of his or her life because of illness and subsequent attempts to change or see illness differently (i.e., change aspects of life or behavior, see illness as a chance for individual development, believing that the illness has meaning).
The items scored on a 5-point scale from disagreement to agreement (0, does not apply at all; 1, does not truly apply; 2, don’t know (neither yes nor no); 3, applies quite a bit; 4, applies very much). The scores were referred to a 100% level (transformed scale score). Scores > 50% indicate higher agreement (positive attitude), while scores < 50% indicate disagreement (negative attitude).
3.6. Positive Emotions (Associated with God)
To measure positive or negative emotions associated with God, we used a 12-item scale which was not yet validated for the Polish population. The instrument addresses positive emotions with 6 items (i.e., Happiness/Joy, Love, Affection, Security, Shelter, Confidence/Trust), negative emotions with 5 items (i.e., Guilt, Punishment, Failure, Fear, Anger/Rage), while 1 item addresses a person’s disinterest in God. Within this sample, the sub-scale measuring positive emotions has a very good internal reliability (alpha = 0.95), and the sub-scale measuring negative perceptions a good internal reliability (alpha = 0.85).
These items were scored on a 5-point scale from disagreement to agreement (0, does not apply at all; 1, does not truly apply; 2, don’t know (neither yes nor no); 3, applies quite a bit; 4, applies very much). The score was referred to a 100% level (transformed scale score).
3.7. Statistical Analysis
The research team performed descriptive data analyses, cross tabulation (Pearson Chi2), analyses of variance (ANOVA), correlation (Spearman rho), stepwise regression and linear regression analyses with SPSS 22.0.
The team judged p < 0.05 as significant. With respect to the correlation analyses, we regarded r > 0.5 as a strong correlation, an r between 0.3 and 0.5 as a moderate correlation, an r between 0.2 and 0.3 as a weak correlation, and r < 0.2 as no or a negligible correlation.
4. Results
4.1. Participants
As shown in table 1, patients’ mean age was 56 ± 16 years; 74% were women and 26% men. Most were married and had a medium educational level. All had chronic diseases, predominantly cancer (35%), diabetes mellitus (16%), chronic pain diseases (10%), and other chronic conditions.
Polish patients were 100% Catholics; 78% regarded themselves as religious and spiritual (R + S +), 7% as religious but not spiritual (R + S −), 2% as not religious but spiritual (R – S +), and 13% as neither religious nor spiritual (R – S −).
4.2. Patients’ Interpretations of Illness
As shown in
Table 2, most regarded their disease as an Adverse Interruption of life (61%) or as a Threat/Enemy (50%), but also as a Challenge (42%). Several may see their illness as a Call for help (22%), as an own Weakness/Failure (20%), or as something of Value to grow (18%), and only a few as a Relieving Break from the demands of life (12%) or as a Punishment (8%).
Table 2.
Interpretations of Illness (multiple answers).
Table 2.
Interpretations of Illness (multiple answers).
| | NO (%) | Undecided (%) | YES (%) | Non-responder (%) |
|---|
| Threat/Enemy | 26 | 24 | 50 | < 1 |
| Adverse interruption of life | 21 | 19 | 61 | 0 |
| Punishment | 70 | 22 | 8 | < 1 |
| Own Failure | 53 | 27 | 20 | 1 |
| Relieving break from the demands of life | 68 | 20 | 12 | 0 |
| Call for help | 58 | 21 | 22 | < 1 |
| Something of value to grow | 52 | 30 | 18 | 1 |
| Challenge | 35 | 23 | 42 | < 1 |
Because patients had multiple options to assess their illness, there might be also combinations. We focused on the most often cited disease perception, and found that 71% of those who see their illness as an Adverse Interruption may see it also as a Threat/Enemy, while 41% can see it also as a Challenge (
Table 3).
Table 3.
Interpretations of Illness with respect to adverse interruption (cross tabulation).
Table 3.
Interpretations of Illness with respect to adverse interruption (cross tabulation).
| | Adverse interruption of life | p-value (Chi2) |
|---|
| | | Disagreement/undecided (%) | Agreement (%) |
|---|
| Threat/Enemy | No/undecided | 83 | 29 | < 0.0001 |
| Agreement | 17 | 71 | |
| Punishment | No/undecided | 96 | 89 | |
| Agreement | 4 | 11 | 0.018 |
| Own Failure | No/undecided | 87 | 76 | |
| Agreement | 13 | 24 | 0.022 |
| Relieving break from the demands of life | No/undecided | 90 | 86 | n.s. |
| Agreement | 10 | 14 | |
| Call for help | No/undecided | 89 | 72 | < 0.0001 |
| Agreement | 11 | 28 | |
| Something of value to grow | No/undecided | 71 | 89 | < 0.0001 |
| Agreement | 29 | 11 | |
| Challenge | No/undecided | 56 | 59 | n.s. |
| Agreement | 44 | 41 | |
We next intended to analyse the influence of socio-demographic data, and found that the view of illness as something of Value was significantly lower in male patients than in women, while the view of illness as a Threat/Enemy was higher in men (
Table 4). Patients with cancer had significantly higher perceptions of illness as a Threat/Enemy than those with other (primarily non-fatal) diseases, while all other interpretations did not significantly differ between both subgroups (
Table 4). Of interest, patients who would regard themselves as R-S- had significantly higher scores for Adverse Interruption and Punishment and had lower scores for Value than their religious/spiritual counterparts. Age, educational level and family status had no significant influence on the disease interpretations (data not shown), with the exception of Call for Help, which was highest in elderly (F = 4.5;
p = 0.001) and widowed persons (F = 4.6,
p = 0.11), and also in those with a lower educational level (F = 3.2;
p = 0.024).
Table 4.
Interpretations of illness and socio-demographic variables.
Table 4.
Interpretations of illness and socio-demographic variables.
| | | Threat/Enemy | Adverse Interruption | Punishment | Weakness/ Failure | Relieving Break | Call for Help | Value | Challenge |
|---|
| All patients | Mean | 2.37 | 2.61 | 1.01 | 1.47 | 1.16 | 1.47 | 1.50 | 2.01 |
| SD | 1.22 | 1.20 | 1.04 | 1.19 | 1.13 | 1.23 | 1.12 | 1.28 |
| Gender |
| Women (74%) | Mean | 2.25 | 2.57 | 0.99 | 1.42 | 1.16 | 1.47 | 1.63 | 1.94 |
| SD | 1.27 | 1.21 | 1.04 | 1.19 | 1.10 | 1.19 | 1.14 | 1.27 |
| Men (26%) | Mean | 2.68 | 2.74 | 1.08 | 1.64 | 1.17 | 1.47 | 1.13 | 2.24 |
| SD | 1.05 | 1.16 | 1.04 | 1.19 | 1.22 | 1.34 | 0.95 | 1.27 |
| F value | | 6.6 | 1.1 | 0.4 | 1.9 | 0.0 | 0.0 | 11.2 | 3.0 |
| P value | | 0.011 | n.s. | n.s. | n.s. | n.s. | n.s. | 0.001 | 0.087 |
| Disease |
| Chronic diseases (65%) | Mean | 2.22 | 2.52 | 0.97 | 1.49 | 1.14 | 1.38 | 1.49 | 2.01 |
| SD | 1.18 | 1.19 | 1.03 | 1.21 | 1.06 | 1.22 | 1.12 | 1.24 |
| Cancer (35%) | Mean | 2.64 | 2.78 | 1.10 | 1.44 | 1.21 | 1.63 | 1.52 | 2.02 |
| SD | 1.26 | 1.18 | 1.07 | 1.16 | 1.26 | 1.24 | 1.12 | 1.35 |
| F value | | 7.3 | 3.2 | 1.1 | 0.1 | 0.2 | 2.6 | 0.0 | 0.0 |
| P value | | 0.007 | 0.077 | n.s. | n.s. | n.s. | n.s. | n.s. | n.s. |
| Religious orientation (R-S- vs. R/S) |
| No (15%) | Mean | 2.59 | 3.10 | 1.37 | 1.73 | 1.27 | 1.41 | 0.83 | 1.98 |
| SD | 0.97 | 0.83 | 1.11 | 1.16 | 1.32 | 1.26 | 0.83 | 1.27 |
| Yes (85%) | Mean | 2.32 | 2.52 | 0.95 | 1.42 | 1.15 | 1.48 | 1.62 | 2.02 |
| SD | 1.26 | 1.23 | 1.02 | 1.18 | 1.10 | 1.23 | 1.12 | 1.28 |
| F value | | 1.6 | 8.4 | 5.7 | 2.5 | 0.4 | 0.1 | 18.4 | 0.0 |
| P value | | n.s. | 0.004 | 0.018 | n.s. | n.s. | n.s. | < 0.0001 | n.s. |
4.3. Interpretations of Illness and Their Association with External Measures
To clarify which specific interpretations of illness were associated with different aspects of spirituality on the one hand, and life satisfaction and escape from illness on the other hand, we performed first order correlation analyses.
In line with our hypothesis, particularly the positive interpretation Value was moderately to strongly related to patients’ religiosity/spirituality (particularly with religious Trust and Reflection), while Challenge (which was only marginally related to Value) was weakly associated only with spiritual Search and Reflection (
Table 5).
In line with our suggestion, the Escape scale was strongly correlated with fatalistic negative interpretations (
i.e., Threat/Enemy, Interruption) and moderately with Call for Help and Punishment (
Table 5). Life satisfaction correlated best (and negative) with Call for help. Because Escape and life satisfaction are negatively correlated (r =−0.50), it is evident that the pattern of the aforementioned variables is inversely associated.
Table 5.
Interpretations of illness and their correlations with life Satisfaction, escape from illness, and aspects of spirituality.
Table 5.
Interpretations of illness and their correlations with life Satisfaction, escape from illness, and aspects of spirituality.
| | Threat/Enemy | Adverse Interruption | Punishment | Weakness/ Failure | Relieving Break | Call for Help | Value | Challenge |
|---|
| Interpretations of Illness |
| Threat/Enemy | 1.000 | 0.650 ** | 0.312 ** | 0.177 ** | 0.120 | 0.366 ** | −0.150 | 0.157 ** |
| Adverse interruption | | 1.000 | 0.281 ** | 0.140 | 0.056 | 0.250 ** | −0.266 ** | −0.023 |
| Punishment | | | 1.000 | 0.387 ** | 0.223 ** | 0.386 ** | −0.038 | 0.037 |
| Failure | | | | 1.000 | 0.136 | 0.194 ** | 0.074 | −0.051 |
| Relieving break | | | | | 1.000 | 0.455 ** | 0.207 ** | 0.140 |
| Call for help | | | | | | 1.000 | 0.153 | 0.145 |
| Something of value | | | | | | | 1.000 | 0.206 ** |
| Challenge | | | | | | | | 1.000 |
| Spirituality (SQS and SpREUK Polish) |
| Religious attitudes | −0.069 | −0.161 ** | −0.134 | −0.104 | 0.034 | 0.168 ** | 0.356 ** | 0.045 |
| Ethical Sensitivity | 0.019 | 0.032 | −0.094 | −0.047 | −0.018 | 0.120 | 0.313 ** | 0.062 |
| Harmony | −0.168 ** | −0.188 ** | −0.143 | −0.085 | 0.050 | −0.044 | 0.230 ** | 0.166 ** |
| Search | 0.017 | −0.108 | −0.005 | −0.034 | 0.029 | 0.217 ** | 0.369 ** | 0.215 ** |
| Trust | −0.083 | −0.163 ** | −0.093 | −0.021 | 0.010 | 0.136 | 0.511 ** | 0.174 ** |
| Reflection | −0.173 ** | −0.260 ** | −0.160 ** | −0.134 | 0.033 | 0.124 | 0.478 ** | 0.201** |
| Emotions towards God |
| Positive | −0.191 ** | −0.248 ** | −0.111 | −0.102 | −0.035 | 0.059 | 0.310 ** | 0.055 |
| Negative | 0.211 ** | 0.208 ** | 0.222 ** | 0.067 | 0.175 ** | 0.203 ** | −0.008 | 0.079 |
| Life satisfaction | | | | | | | | |
| Life Satisfaction | −0.277 ** | −0.285 ** | −0.287 ** | −0.116 | −0.125 | −0.381 ** | 0.237 ** | −0.031 |
| Escape from Illness | 0.589 ** | 0.546 ** | 0.363 ** | 0.119 | 0.175 ** | 0.482 ** | −0.235 ** | 0.005 |
4.4. Predictors of Interpretations of Illness
To analyse which variables may be the best predictors of the specific perceptions of illness, particularly with respect to measures of spirituality, we performed stepwise regression analyses. Because the included variables predicted less than 15% of variance of the disease perceptions Weakness/Failure (R2 = 0.05), Relieving Break (R2 = 0.04), Punishment (R2 = 0.12) and Challenge (R2 = 0.14), the respective models were too weak to draw valid conclusion.
As shown in
Table 6, Threat can be predicted best by Escape from Illness and male gender (R
2 = 0.38). Interruption of Life can be predicted best by Escape from Illness, with a further negative influence of Reflection, and a positive influence of Ethical Sensitivity (R
2 = 0.36). Also The strategy-associated interpretation Call for Help was explained best by Escape from Illness, with further influences of spiritual Search and Ethical Sensitivity, and a negative influence of life satisfaction (R
2 = 0.35). The positive interpretation Value was explained best by religious Trust, with further negative influences of Escape from Illness, living with partner, and positive influence of Reflection (R
2 = 0.33).
Table 6.
Predictors of interpretations of illness (stepwise regression analyses).
Table 6.
Predictors of interpretations of illness (stepwise regression analyses).
| | Beta | T | p | Collinearity statistics * |
|---|
| tolerance | VIF |
|---|
| Threat | | | | | |
| Model 2: R2 = 0.38 | (constant) | | 0.739 | 0.461 | | |
| Escape from Illness | 0.595 | 12.359 | 0.000 | 1.000 | 1.000 |
| Male gender | 0.154 | 3.205 | 0.002 | 1.000 | 1.000 |
| Interruption | | | | | |
| Model 3: R2 = 0.36 | (constant) | | 1.723 | 0.086 | | |
| Escape from Illness | 0.515 | 10.326 | 0.000 | 0.961 | 1.041 |
| Reflection | −0.237 | −4.380 | 0.000 | 0.819 | 1.221 |
| Ethical Sensitivity | 0.158 | 2.987 | 0.003 | 0.850 | 1.177 |
| Call for Help | | | | | |
| Model 4: R2 = 0.35 | (constant) | | 0.785 | 0.433 | | |
| Escape from Illness | 0.368 | 6.550 | 0.000 | 0.775 | 1.290 |
| Search | 0.188 | 3.448 | 0.001 | 0.819 | 1.222 |
| Life Satisfaction | −0.268 | −4.671 | 0.000 | 0.741 | 1.349 |
| Ethical Sensitivity | 0.135 | 2.419 | 0.016 | 0.781 | 1.280 |
| Value | | | | | |
| Model 4: R2 = 0.33 | (constant) | | 1.177 | 0.240 | | |
| Trust | 0.363 | 4.572 | 0.000 | 0.404 | 2.473 |
| Escape from Illness | −0.170 | −3.314 | 0.001 | 0.963 | 1.039 |
| Reflection | 0.171 | 2.149 | 0.033 | 0.399 | 2.506 |
| living with partner | −0.106 | −2.079 | 0.039 | 0.983 | 1.017 |
Thus, religious issues were of strong relevance particularly for Value, and also for Call for help, while fatalistic negative interpretations were predicted best by patients’ intention to escape from illness with no significant influence of specific religious issues.
4.5. Predictors of Life Satisfaction and Escape from Illness
Now we intended to analyse the influence of specific disease interpretations (
i.e., Value, Call for Help, Threat/Enemy and Adverse interruption) and other variables (
i.e., emotions towards God, religious Trust, gender, age and living with or without a partner) on life satisfaction and Escape from Illness. To identify the best fitting predictors, we therefore applied linear regression models (
Table 7). It is expected that the positive variable Value will have a positive influence on life satisfaction, while the negative disease perceptions will have a negative (promoting) influence on escape from illness.
In the first linear regression model with life satisfaction as dependent variable (
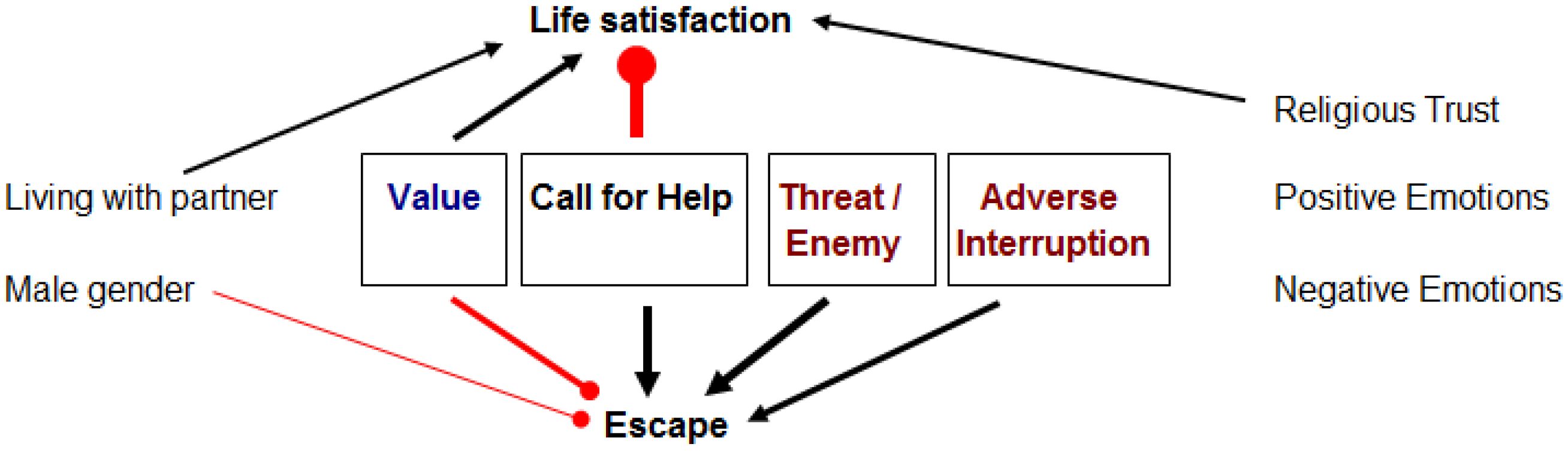
Table 7), the illness interpretation Call for Help was the best (negative) predictor, with further promoting effects of Value, living with a partner, and religious Trust. These variables account of 29% of variance.
Table 7.
Predictors of life satisfaction and escape from illness (stepwise regression analyses).
Table 7.
Predictors of life satisfaction and escape from illness (stepwise regression analyses).
| | Beta | T | p | Collinearity statistics * |
|---|
| tolerance | VIF |
|---|
| Dependent variable: Life satisfaction | | | | | |
| Model 4: R2 = 0.29 | (constant) | | 23.789 | < 0.0001 | | |
| Illness = Call for Help | −0.434 | −8.183 | < 0.0001 | 0.963 | 1.039 |
| Illness = Value | 0.239 | 3.893 | < 0.0001 | 0.719 | 1.390 |
| Living with partner | 0.131 | 2.470 | 0.014 | 0.962 | 1.039 |
| Religious Trust | 0.149 | 2.420 | 0.016 | 0.719 | 1.392 |
| Dependent variable: Escape | | | | | |
| Model 5: R2 = 0.51 | (constant) | | 7.462 | < 0.0001 | | |
| Illness = Threat/Enemy | 0.313 | 5.262 | < 0.0001 | 0.535 | 1.869 |
| Illness = Call for Help | 0.332 | 6.864 | < 0.0001 | 0.814 | 1.229 |
| Illness = Value | −0.215 | −4.589 | < 0.0001 | 0.861 | 1.161 |
| Illness = Adverse Interruption | 0.199 | 3.440 | 0.001 | 0.566 | 1.768 |
| Male gender | −0.106 | −2.347 | 0.020 | 0.934 | 1.071 |
In the second linear regression model with Escape as dependent variable (R2 = 0.51), both negative disease perceptions Call for Help and Threat/Enemy were the strongest predictors, with further promoting (aggravating) effect of Adverse Interruption, and negative (ameliorating) effects of Value and male gender.
Religious Trust explains only 5% of variance in life satisfaction, and positive emotions towards God 4% of variance; both variables were thus not of relevance in the prediction model. Religious Trust explains 3% of Escape’s variance, and positive emotions towards God explains 4%, and were thus not of relevance in the respective prediction model.
5. Discussion
Most of the Catholic Polish patients investigated in this study exhibited fatalistic negative interpretations of their illness (i.e., Adverse Interruption, Threat/Enemy), while a large fraction can nevertheless see it also as a Challenge. Interestingly, 41% of those who regard their illness as an Adverse Interruption would see it also as a Challenge.
In line with our primary hypothesis, the current data underline that the intention to escape from illness, as a depressive escape-avoidance strategy, is strongly related to fatalistic negative perceptions of disease but also with the perception of illness as Call for help or even a Punishment, but not with illness as a Challenge. Patients’ ability to reflect their life concerns, to change attitudes and behaviour, and to see illness differently (SpREUK’s Reflection subscale), was moderately associated only with Value. It is consistent with the underlying theory that having trust in God is related with the view that even illness can be something of value for an inner development or even “spiritual transformation”, as observed also in persons with HIV [
10,
11], and/or a feeling of control in difficult situations [
32]. Moreover, exclusively Value as an interpretation of illness was associated moderately with different dimensions of patients’ spirituality and positive emotions towards God. This would confirm our second hypothesis that a positive disease interpretation is associated primarily with patients’ religiosity/spirituality. However, while this is true for Value, the view of illness as a Challenge was only weakly associated with measures of spirituality. Challenge was neither related to life satisfaction, nor negatively to Escape from Illness, nor to positive or negative emotions towards God, and only weakly associated with a persons’ ability to reflect life concerns (which is consistent with the underlying construct) on the one hand, and an attitude of Search for a spiritual source which might be helpful, and marginally with religious Trust. Yet, it was not significantly associated with Religious attitudes or Ethical Sensitivity. This would indicate that the view of illness as a Challenge is rather related to spirituality as a strategy to cope (state) than an intrinsic aspect of religiosity (trait).
The role of Polish patients’ spirituality was investigated by Krok [
33], too. In his study using the Self-description Questionnaire of Spirituality (which was used in this study, too), spirituality was an important buffer against stressful events to help people to cope with distress and difficulties in life. Interestingly, the underlying three spiritual dimensions (
i.e., Religious Attitudes, Ethical Sensitivity, and Harmony) have a different impact on particular coping styles depending. While Religious Attitudes were not significantly related to specific coping styles, Ethical Sensitivity was associated with Avoidance and Social Diversion coping, and the subscale Harmony was related to a Task-oriented coping, and negatively with Avoidance-oriented coping [
33]. This means that people characterized by a high level of spirituality will try to solve problems through efforts aimed at solving the problem and seeking social support.
5.1. Interaction Model between Interpretations of Illness, Emotions towards God, Life Satisfaction and Escape from Illness
It is intuitive that having a positive view of the illness (
i.e., something of value to grow) would be of benefit to cope, and thus would increase patients’ life satisfaction. Moreover, having or not a concrete partner to rely on in times of need would mean, patients have someone who is providing support and care on the one hand, or a positive relation towards God who is expected to help in times of need and thus providing hope and emotional comfort, would all contributing to higher life satisfaction, too. In contrast, when illness is interpreted as a Call for Help then patients are in strong need for external support, and thus their life satisfaction might be low. This Call for Help can, but must not necessarily have a religious connotation. In the respective regression model, it was patients’ religious Trust on the one hand and living with a partner were among the significant contributors to life satisfaction. This means, having a reliable source of help (either a concrete partner or a helping God) will contribute to a persons’ experienced life satisfaction. This is consistent with the theory and literature that loneliness is negatively related to life satisfaction [
34], while partnership is positively related with life satisfaction [
35,
36].
In contrast, seeing illness as something negative was in fact the best predictor of patients’ intention to escape from illness. Theoretically, negative emotions towards God (implying illness as a punishment) might be associated with higher intention to escape from illness and lower life satisfaction; yet, neither positive nor negative emotions were among the significant predictors in both models. However, in a small study enrolling patients with multiple sclerosis from Poland found a negative correlation between negative emotion and consequences of own illness, and SQS’s Harmony scale [
37]. In our study, we did not analyse the association of negative emotions with measures of spirituality, yet we can confirm that negative disease interpretations are related to negative interpretations. However, in our sample these negative interpretations were only marginally related with SQS’s Harmony or other scales.
The main findings of this interaction model are summarized in
Figure 1.
Figure 1.
Interaction model with respect to the regression analyses. Positive influences on the dependent variables on life satisfaction or escape were indicated as arrow lines, while inhibitory influences were indicated as lines with thickened ends. The thickness of lines correspond with the T values of the regression models. Round ends indicate negative influences, while arrowed ends indicate positive influences.
Figure 1.
Interaction model with respect to the regression analyses. Positive influences on the dependent variables on life satisfaction or escape were indicated as arrow lines, while inhibitory influences were indicated as lines with thickened ends. The thickness of lines correspond with the T values of the regression models. Round ends indicate negative influences, while arrowed ends indicate positive influences.
5.2. Limitations
A limitation of this study is the cross-sectional design, which does not allow for causal interpretations. To substantiate the findings, longitudinal studies are needed. We also have no information about how many patients rejected to fill the questionnaire at all, and thus the sample should be regarded as a convenience sample Moreover, the data may not be representative for patients from whole Poland because the patients were recruited only in the city of Wieliszew and in the province of Warsaw; thus, a more diverse sample is highly encouraged.
6. Conclusions
The data show that specific dimensions of spirituality are important predictor for patients’ distinct interpretation of illness. Particularly religious Trust was identified as the best predictor of Polish patients’ interpretation of illness as something of Value, indicating potentially the chance for a “spiritual transformation”. Yet, religious Trust has only a very weak influence on patients’ depressive intention to escape from the current life situation; it is not a buffer against suffering, but might be a positive resource to cope and to find new perspectives—and thus a matter of hope. In fact, a study among Polish cancer patients by Wnuk
et al., [
38] confirmed a positive relationship between frequency of spiritual experiences and strength of hope. Indeed, the ability to reflect life concerns and to change life or behaviour (Reflection scale), which was also related in this study to the disease interpretation Value, has clearly a religious connotation and is strongly associated with positive views of God, also the experience of gratitude and awe [
22].
In this context, it is of importance to underline that negative interpretations were mainly related to the intention to escape from illness and reduced life satisfaction. Particularly when patients’ state negative disease perceptions, psychologists, nurses and physicians should be aware that these may be indicators that patients may require further psychological and/or pastoral assistance to cope with their burden. These disease interpretations may help to understand how patients react towards their illness, which strategies they may use to cope, and how they can be supported to adapt to the complex process of chronic illness. When positive interpretations predominate they may indicate some kind of “inner transformation” with processes to change attitudes, priorities, and life style, while persisting negative interpretations indicate the need for specific psychological support. In fact, although the causality is unclear, in Canadian breast cancer patients their negative disease perceptions (
i.e., Enemy, Loss, or Punishment) were related to higher mental health affections and lower quality of life within a 3 year follow up than women who indicated a more positive meaning [
16]. Moreover, also the view of illness as a call for help means that patients are searching for a helpful source because they feel that they cannot manage the implications of illness alone. These persons obviously require further support, either by chaplains, psychologists, social workers, nurses, physicians, or their relatives.





{kind=link}
