Does Religious Involvement Mitigate the Effects of Major Discrimination on the Mental Health of African Americans? Findings from the Nashville Stress and Health Study


Abstract
:1. Introduction
2. Theoretical and Empirical Background
2.1. Discrimination and Mental Health
2.2. African American Religion as a Stress Buffer
2.2.1. Organizational Religiosity
2.2.2. Non-Organizational Religiosity
2.2.3. Church-Based Social Support
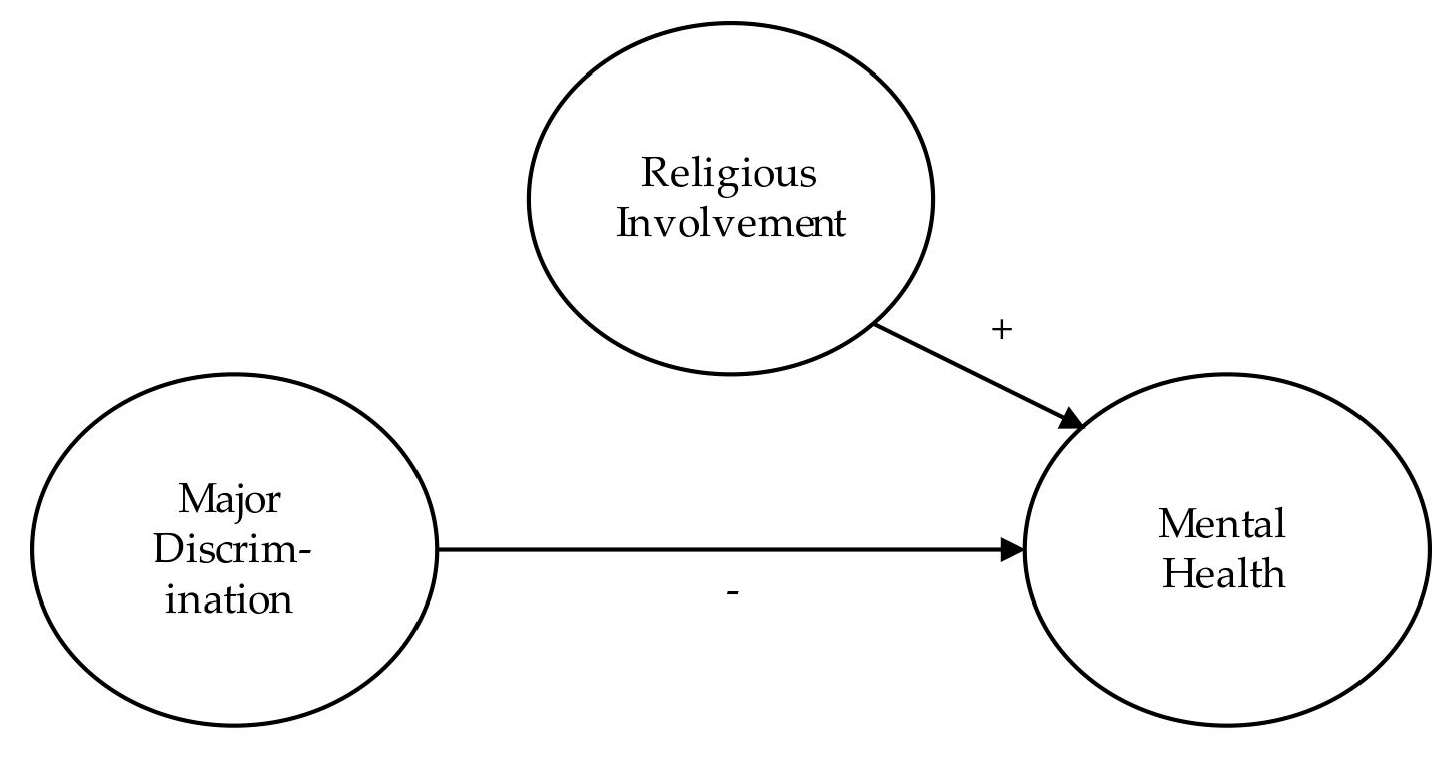
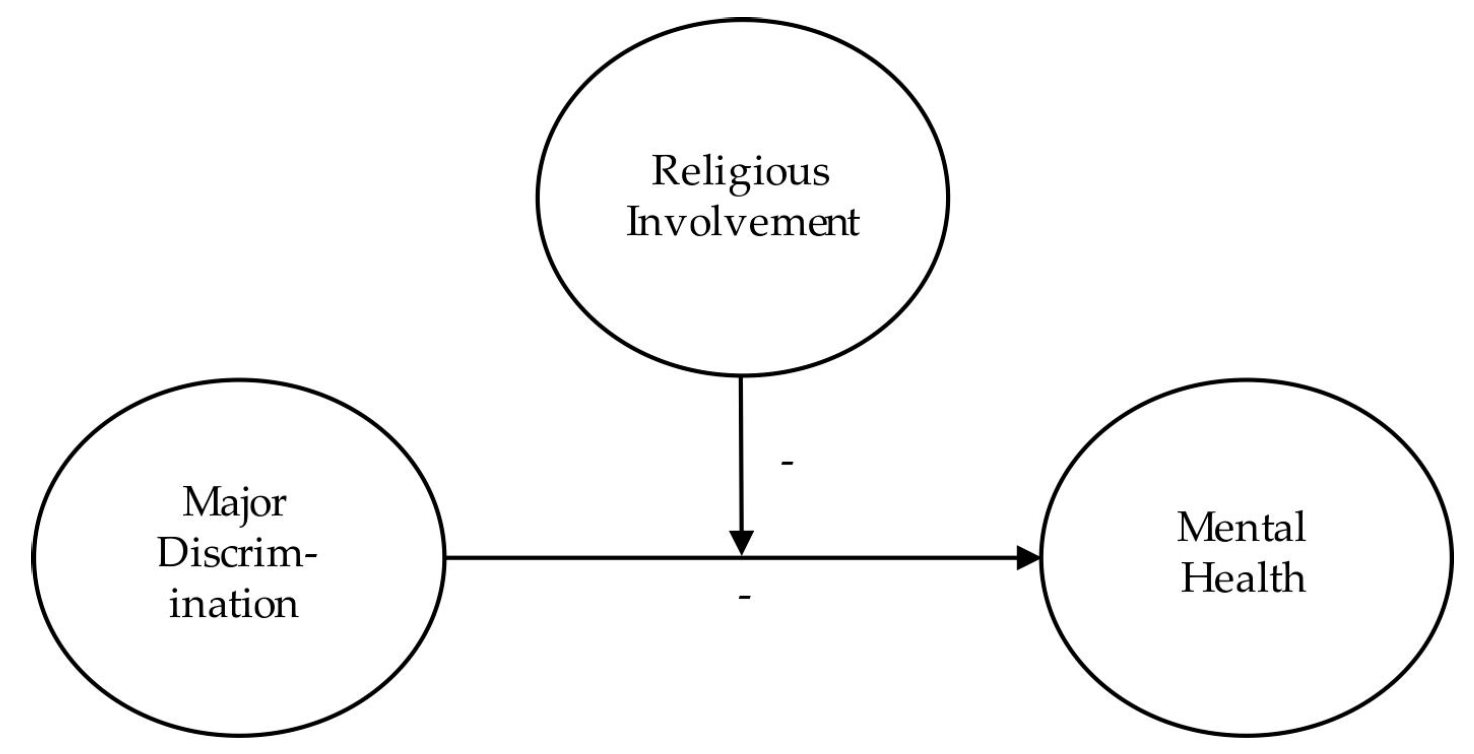
3. Conceptual Models
4. Methods
4.1. Data
4.2. Measures
4.2.1. Past-Month Depression
4.2.2. Life Satisfaction
4.2.3. Major Discrimination
4.2.4. Religious Involvement
4.2.5. Socio-Demographics
4.3. Analytic Strategy
5. Results
6. Discussion and Conclusions
Author Contributions
Conflicts of Interest
References
- Aiken, Leona S., Stephen G. West, and Raymond R. Reno. 1991. Multiple Regression: Testing and Interpreting Interactions. Thousand Oaks: Sage. [Google Scholar]
- Berger, Maximus, and Zoltan Saranyai. 2015. More than Skin Deep: Stress Neurobiology and Mental Health Consequences of Racial Discrimination. Stress 18: 1–10. [Google Scholar] [CrossRef] [PubMed]
- Berger, Peter L. 1967. The Sacred Canopy. Garden City: Doubleday. [Google Scholar]
- Bertrand, Marianne, and Sendhil Mullainathan. 2004. Are Emily and Greg More Employable than Lakisha and Jamal? A Field Experiment on Labor Market Discrimination. American Economic Review 94: 991–1013. [Google Scholar] [CrossRef]
- Bierman, Alex. 2006. Does Religion Buffer the Effects of Discrimination on Mental Health? Differing Effects by Race. Journal for the Scientific Study of Religion 45: 551–65. [Google Scholar] [CrossRef]
- Billingsley, Andrew. 1999. Mighty Like a River: The Black Church and Social Reform. New York: Oxford University Press. [Google Scholar]
- Chatters, Linda M., Kai M. Bullard, Robert J. Taylor, Amanda T. Woodward, Harold W. Neighbors, and James S. Jackson. 2008. Religious Participation and DSM-IV Disorders among Older African Americans: Findings from the National Survey of American Life (NSAL). American Journal of Geriatric Psychiatry 16: 957–65. [Google Scholar] [CrossRef] [PubMed]
- Chatters, Linda M., Robert J. Taylor, Kai M. Bullard, and James S. Jackson. 2009. Race and Ethnic Differences in Religious Participation: African Americans, Caribbean Blacks, and non-Hispanic Whites. Ethnic and Racial Studies 32: 1143–63. [Google Scholar] [CrossRef] [PubMed]
- Chatters, Linda M., Robert J. Taylor, Karen D. Lincoln, Ann Nguyen, and Sean Joe. 2015. Church-based Social Support and Suicidality among African Americans and Black Caribbeans. Archives of Suicide Research 15: 337–53. [Google Scholar] [CrossRef] [PubMed]
- Chatters, Linda M., Robert J. Taylor, Amanda T. Woodward, and Emily J. Nicklett. 2011. Social Support from Church Members and Family Members and Depressive Symptoms among Older African Americans. American Journal of Geriatric Psychiatry 23: 559–67. [Google Scholar] [CrossRef] [PubMed]
- Cooper-Lewter, Nicholas C., and Henry H. Mitchell. 1986. Soul Theology: The Heart of American Black Culture. San Francisco: Harper and Row. [Google Scholar]
- DeAngelis, Reed T., and Christopher G. Ellison. 2017. Kept in His Care: The Role of Perceived Divine Control in Positive Reappraisal Coping. Religions 8. article 133. [Google Scholar] [CrossRef]
- Diener, Ed, Robert A. Emmons, Randy J. Larsen, and Sharon Green. 1985. The Satisfaction with Life Scale. Journal of Personality Assessment 49: 71–75. [Google Scholar] [CrossRef] [PubMed]
- Edwards, Korie. 2009. Race, Religion, and Worship: Are African American Worship Practices Distinct? Journal for the Scientific Study of Religion 48: 30–52. [Google Scholar] [CrossRef]
- Ellison, Christopher G. 1991. Religious Involvement and Subjective Well-being. Journal of Health and Social Behavior 32: 80–99. [Google Scholar] [CrossRef] [PubMed]
- Ellison, Christopher G. 1993. Religious Involvement and Self-Perceptions among Black Americans. Social Forces 71: 1027–55. [Google Scholar] [CrossRef]
- Ellison, Christopher G., Matt Bradshaw, Kevin J. Flannelly, and Kathleen C. Galek. 2014. Prayer, Attachment to God, and Symptoms of Anxiety-related Disorders among U.S. Adults. Sociology of Religion 75: 208–33. [Google Scholar] [CrossRef]
- Ellison, Christopher G., and Kevin J. Flannelly. 2009. Religious Involvement and Risk of Major Depression in a Prospective Nationwide Study of African American Adults. Journal of Nervous and Mental Disease 197: 568–73. [Google Scholar] [CrossRef] [PubMed]
- Ellison, Christopher G., and David A. Gay. 1990. Region, Religious Involvement, and Life Satisfaction among Black Americans. The Sociological Quarterly 31: 123–47. [Google Scholar] [CrossRef]
- Ellison, Christopher G., and Linda K. George. 1994. Religious Involvement, Social Ties, and Social Support in a Southeastern Community. Journal for the Scientific Study of Religion 33: 46–61. [Google Scholar] [CrossRef]
- Ellison, Christopher G., and Andrea K. Henderson. 2011. Religion and Mental Health: Through the Lens of the Stress Process. In Toward a Sociological Theory of Religion and Health. Edited by Anthony J. Blasi. Boston: Brill, pp. 11–44. [Google Scholar]
- Ellison, Christopher G., Robert A. Hummer, Amy M. Burdette, and Maureen R. Benjamins. 2010. Race, Religious Involvement, and Health: The Case of African Americans. In Religion, Families, and Health: Population-based Research in the United States. Edited by Christopher G. Ellison and Robert A. Hummer. New Brunswick: Rutgers University Press, pp. 321–48. [Google Scholar]
- Ellison, Christopher G., Marc A. Musick, and Andrea K. Henderson. 2008. Balm in Gilead: Racism, Religious Involvement, and Psychological Distress among African American Adults. Journal for the Scientific Study of Religion 47: 291–309. [Google Scholar] [CrossRef]
- Ellison, Christopher G., and Darren E. Sherkat. 1995. The Semi-Involuntary Institution Revisited: Regional Variations in Church Participation among Black Americans. Social Forces 73: 1415–37. [Google Scholar] [CrossRef]
- Ellison, Christopher G., and Robert J. Taylor. 1996. Turning to Prayer: Social and Situational Antecedents of Religious Coping among African Americans. Review of Religious Research 38: 111–31. [Google Scholar] [CrossRef]
- English, Devin, Sharon F. Lambert, and Nicholas S. Ialongo. 2014. Longitudinal Associations between Experienced Racial Discrimination and Depressive Symptoms in African American Adolescents. Developmental Psychology 50: 1190–96. [Google Scholar] [CrossRef] [PubMed]
- Fix, Michael, and Margery Austin Turner. 1999. National Report Card on Discrimination in America. Washington: Urban Institute. [Google Scholar]
- Gilkes, Cheryl Townsend. 1980. The Black Church as a Therapeutic Community: Suggested Areas for Research into the Black Religious Experience. Journal of the Interdenominational Theological Center 8: 29–44. [Google Scholar]
- Griffith, Ezra E. H., Thelma English, and Viola Mayfield. 1980. Possession, Prayer, and Testimony: Therapeutic Elements of the Wednesday Night Prayer Meeting in a Black Church. Psychiatry 43: 120–28. [Google Scholar] [CrossRef] [PubMed]
- Harris, Anne-Marie G., Gerald R. Harrison, and Jerome D. Williams. 2005. Courting Customers: Assessing Consumer Racial Profiling and Other Marketplace Discrimination. Journal of Public Policy and Marketing 24: 163–71. [Google Scholar] [CrossRef]
- Hayward, R. David, and Neal Krause. 2015. Religion and Strategies for Coping with Racial Discrimination among African Americans and Caribbean Blacks. International Journal of Stress Management 22: 70–91. [Google Scholar] [CrossRef]
- Head, Rachel N., and Maxine Seaborn Thompson. 2017. Discrimination-related Anger, Religion, and Distress: Differences between African Americans and Caribbean Black Americans. Society and Mental Health. Published electronically June 11, 2017. [Google Scholar] [CrossRef]
- Henderson, Andrea K. 2016. The Long Arm of Religion: Childhood Adversity, Religion, and Self-Perception among Black Americans. Journal for the Scientific Study of Religion 55: 324–48. [Google Scholar] [CrossRef]
- Himmelstein, Mary S., Danielle M. Young, Diana T. Sanchez, and James S. Jackson. 2015. Vigilance in the Discrimination-Stress Model for Black Americans. Psychology and Health 30: 253–67. [Google Scholar] [CrossRef] [PubMed]
- Holt, Cheryl L., Emily Schulz, Beverly R. Williams, Eddie M. Clark, and Min Qi Wang. 2014. Social Support as a Mediator of Religious Involvement and Physical and Emotional Functioning in a National Sample of African Americans. Mental Health, Religion, and Culture 17: 421–35. [Google Scholar] [CrossRef]
- Hope, Meredith O., Shervin Assari, Yasmin C. Cole-Lewis, and Cleopatra H. Caldwell. 2017. Religious Social Support, Discrimination, and Psychiatric Disorders among Black Adolescents. Race and Social Problems 9: 102–14. [Google Scholar] [CrossRef]
- Hunt, Larry L., and Matthew O. Hunt. 1999. Regional Patterns of African American Church Attendance: Revisiting the Semi-Involuntary Thesis. Social Forces 78: 779–91. [Google Scholar] [CrossRef]
- Idler, Ellen L., Marc A. Musick, Christopher G. Ellison, Linda K. George, Neal Krause, Marcia Ory, Kenneth Pargament, Lynda Powell, Lynn G. Underwood, and David R. Williams. 2003. Measuring Multiple Dimensions of Religion and Spirituality for Health Research: Conceptual Background and Findings from the 1998 General Social Survey. Research on Aging 25: 327–65. [Google Scholar] [CrossRef]
- Jang, Sung-Joon, and Byron R. Johnson. 2004. Exploring Religious Effects on Distress among African Americans. Journal for the Scientific Study of Religion 43: 239–60. [Google Scholar] [CrossRef]
- Kessler, Ronald C., Kristin D. Mickelson, and David R. Williams. 1999. The Prevalence, Distribution, and Mental Health Consequences of Perceived Discrimination in the United States. Journal of Health and Social Behavior 40: 208–30. [Google Scholar] [CrossRef] [PubMed]
- Koenig, Harold G., Velma Carson, and Dana King. 2012. Handbook of Religion and Health, 2nd ed. New York: Oxford University Press. [Google Scholar]
- Krause, Neal. 2002. Exploring Race Differences in a Comprehensive Battery of Church-based Social Support Measures. Review of Religious Research 44: 126–49. [Google Scholar] [CrossRef]
- Krause, Neal. 2003. Exploring Race Differences in the Relationships between Social Interaction with Clergy and Feelings of Self-Worth in Late Life. Sociology of Religion 64: 183–205. [Google Scholar] [CrossRef]
- Krause, Neal. 2004a. Common Facets of Religion, Unique Facets of Religion, and Life Satisfaction among Older African Americans. Journal of Gerontology: Social Sciences 59B: S109–17. [Google Scholar] [CrossRef]
- Krause, Neal. 2004b. Assessing the Relationships among Prayer Expectations, Race, and Self-Esteem in Late Life. Journal for the Scientific Study of Religion 43: 395–408. [Google Scholar] [CrossRef]
- Krause, Neal. 2006. Exploring the Effects of Church-based and Secular Social Support on Self-Rated Health in Late Life. Journal of Gerontology: Social Sciences 61B: S35–43. [Google Scholar] [CrossRef]
- Krause, Neal. 2008a. Aging in the Church: How Social Relationships Affect Health. West Conshohocken: Templeton Press. [Google Scholar]
- Krause, Neal. 2008b. The Social Foundation of Religious Meaning in Life. Research on Aging 30: 395–427. [Google Scholar] [CrossRef]
- Krause, Neal. 2009. Religious Involvement, Gratitude, and Changes in Depressive Symptoms over Time. International Journal for the Psychology of Religion 19: 155–72. [Google Scholar] [CrossRef] [PubMed]
- Krause, Neal, and Linda M. Chatters. 2005. Exploring Race Differences in a Multidimensional Battery of Prayer Measures among Older Adults. Sociology of Religion 66: 23–43. [Google Scholar] [CrossRef]
- Krause, Neal, and Christopher G. Ellison. 2003. Forgiveness by God, Forgiveness of Others, and Psychological Well-being in Late Life. Journal for the Scientific Study of Religion 42: 77–93. [Google Scholar] [CrossRef] [PubMed]
- Kwate, Naa Oyo, and Melody S. Goodman. 2015. Cross-sectional and Longitudinal Effects of Racism on Mental Health among Residents of Black Neighborhoods in New York City. American Journal of Public Health 105: 711–18. [Google Scholar] [CrossRef] [PubMed]
- Levin, Jeffrey S., Linda M. Chatters, and Robert J. Taylor. 1995. Religious Effects on Health and Life Satisfaction among Black Americans. Journal of Gerontology: Social Sciences 50: S154–63. [Google Scholar] [CrossRef]
- Lim, Chaeyoon, and Robert D. Putnam. 2010. Religion, Social Networks, and Life Satisfaction. American Sociological Review 75: 914–33. [Google Scholar] [CrossRef]
- Lincoln, C. Eric, and Lawrence H. Mamiya. 1990. The Black Church in the African American Experience. Durham: Duke University Press. [Google Scholar]
- Mattis, Jacqueline S., and Robert Jagers. 2001. A Relational Framework for the Study of Religiosity and Spirituality in the Lives of African Americans. Journal of Community Psychology 29: 519–39. [Google Scholar] [CrossRef]
- Neighbors, Harold W., Marc A. Musick, and David R. Williams. 1998. The African American Minister as a Source of Help for Serious Personal Crises: Bridge or Barrier to Mental Health Care? Health Education and Behavior 25: 759–77. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Ann, Linda M. Chatters, and Robert J. Taylor. 2016. African American Extended Family and Church-based Support Network Typologies. Family Relations 65: 701–15. [Google Scholar] [CrossRef] [PubMed]
- Oates, Gary L., and Jennifer Goode. 2013. Racial Differences in the Effects of Religiosity and Mastery on Psychological Distress: Evidence from National Longitudinal Data. Society and Mental Health 3: 40–58. [Google Scholar] [CrossRef] [PubMed]
- Pager, Devah, and Hana Shepherd. 2008. The Sociology of Discrimination: Racial Discrimination in Employment, Housing, Credit, and Consumer Markets. Annual Review of Sociology 34: 181–209. [Google Scholar] [CrossRef] [PubMed]
- Pargament, Kenneth I. 1997. The Psychology of Religion and Coping. New York: Guilford. [Google Scholar]
- Pargament, Kenneth I., Harold G. Koenig, and Lisa Perez. 2000. The Many Methods of Religious Coping: Development and Initial Validation of the RCOPE. Journal of Clinical Psychology 56: 519–43. [Google Scholar] [CrossRef]
- Pollner, Melvin L. 1989. Divine Relations, Social Relations, and Well-being. Journal of Health and Social Behavior 30: 92–104. [Google Scholar] [CrossRef] [PubMed]
- Radloff, Lenore S. 1977. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement 1: 385–401. [Google Scholar] [CrossRef]
- Roberts, J. Deotis. 2005. Liberation and Reconciliation: A Black Theology, 2nd ed. Louisville: Westminster John Knox. [Google Scholar]
- Roscigno, Vincent J. 2007. The Face of Discrimination: How Race and Gender Impact Work and Home Lives. Lanham: Rowman and Littlefield. [Google Scholar]
- Ross, Stephen L., and John Yinger. 2002. The Color of Credit: Mortgage Discrimination, Research Methodology and Fair Lending Enforcement. Cambridge: MIT Press. [Google Scholar]
- Schieman, Scott, Alex Bierman, and Christopher G. Ellison. 2013. Religion and Mental Health. In Handbook of the Sociology of Mental Health. Edited by Carol S. Aneshensel, Jo C. Phelan and Alex Bierman. Dordrecht: Springer, pp. 457–78. [Google Scholar]
- Sharp, Shane. 2010. How Does Prayer Help Manage Emotions? Social Psychology Quarterly 73: 417–37. [Google Scholar] [CrossRef]
- Tabak, Melanie A., and Kristin D. Mickelson. 2009. Religious Service Attendance and Distress: The Moderating Role of Stressful Life Events and Race/Ethnicity. Sociology of Religion 70: 149–64. [Google Scholar] [CrossRef]
- Taylor, Robert J., Linda M. Chatters, and Jamie M. Abelson. 2012. Religious Involvement and DSM-IV 12-Month and Lifetime Major Depressive Disorder among African Americans. Journal of Nervous and Mental Disease 200: 856–62. [Google Scholar] [CrossRef] [PubMed]
- Taylor, Robert J., Linda M. Chatters, and Sean Joe. 2011. Religious Involvement and Suicidal Behavior among African Americans and Black Caribbeans. Journal of Nervous and Mental Disease 199: 478–86. [Google Scholar] [CrossRef] [PubMed]
- Taylor, Robert J., Linda M. Chatters, and Jeffrey S. Levin. 2004. Religion in the Lives of African Americans: Social, Psychological, and Health Perspectives. Thousand Oaks: Sage. [Google Scholar]
- Taylor, Robert J., Christopher G. Ellison, Linda M. Chatters, Jeffrey S. Levin, and Karen D. Lincoln. 2000. Mental Health Services within Faith Communities: The Role of Clergy in Black Churches. Social Work 45: 73–87. [Google Scholar] [CrossRef] [PubMed]
- Taylor, Robert J., Michael C. Thornton, and Linda M. Chatters. 1987. Blacks’ Perceptions of the Sociohistorical Role of the Church. Journal of Black Studies 18: 123–38. [Google Scholar] [CrossRef]
- Toussaint, Loren, Everett Worthington, and David R. Williams, eds. 2015. Forgiveness and Health: Scientific Evidence and Theories Relating Forgiveness to Better Health. New York: Springer. [Google Scholar]
- Tsitsos, William. 2003. Race Differences in Congregational Social Service Activity. Journal for the Scientific Study of Religion 42: 205–15. [Google Scholar] [CrossRef]
- Vishkin, Allon, Yochana E. Bigman, Roni Porat, Nevin Solak, Eran Halperin, and Maya Tamir. 2016. God Rest our Hearts: Religiosity and Cognitive Reappraisal. Emotion 16: 252–62. [Google Scholar] [CrossRef] [PubMed]
- Washington, Joseph M. 1994. Conversations with God: Two Centuries of Prayers by African Americans. New York: Harper. [Google Scholar]
- White, Ian R., Patrick Royston, and Angela M. Wood. 2011. Multiple Imputation Using Chained Equations: Issues and Guidance for Practice. Statistics in Medicine 30: 377–99. [Google Scholar] [CrossRef] [PubMed]
- Williams, David R., and Selina A. Mohammed. 2009. Discrimination and Racial Disparities in Health: Evidence and Needed Research. Journal of Behavioral Medicine 32: 20–47. [Google Scholar] [CrossRef] [PubMed]
- Williams, David R., and Ruth Williams-Morris. 2000. Racism and Mental Health: The African American Experience. Ethnicity and Health 5: 243–68. [Google Scholar] [CrossRef] [PubMed]
- Williams, Richard A., Reynold Nesiba, and Eileen Diaz McConnell. 2005. The Changing Face of Inequality in Home Mortgage Lending. Social Problems 52: 181–208. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Range | Mean (%) | SD | |
|---|---|---|---|
| Mental Health Outcomes | |||
| Depression | 1−4 | 1.69 | 0.48 |
| Life satisfaction | 1−4 | 2.63 | 0.65 |
| Focal Independent Variable | |||
| Major discrimination | 0−7 | 1.18 | 1.42 |
| Religious Measures | |||
| Church attendance | 0−3 | 2.01 | 1.02 |
| Prayer | 1−6 | 5.01 | 1.32 |
| Religious social support | 1−4 | 1.85 | 1.04 |
| Attends “weekly or more” | 0−1 | (44) | |
| Prays “several times a day” | 0−1 | (51) | |
| Receives support “very often” | 0−1 | (10) | |
| Socio-demographics | |||
| Age | 22−69 | 46.19 | 11.21 |
| Female | 0−1 | (53) | |
| Male (reference) | 0−1 | (47) | |
| Education (in years) | 0−25 | 13.02 | 3.08 |
| Married | 0−1 | (30) | |
| Not married (reference) | 0−1 | (70) | |
| Employed | 0−1 | (66) | |
| Unemployed (reference) | 0−1 | (34) | |
| Household income | 0−15 | 6.28 | 3.81 |
| (1) | (2) | (3) | (4) | |||||
|---|---|---|---|---|---|---|---|---|
| Focal Variables | ||||||||
| Major discrimination | 0.061 | ** | 0.061 | * | 0.062 | * | 0.060 | * |
| Church attendance | 0.019 | 0.019 | 0.018 | 0.019 | ||||
| Prayer | −0.004 | −0.004 | −0.003 | −0.004 | ||||
| Religious social support | −0.028 | −0.028 | −0.028 | −0.023 | ||||
| Interactions [Major discrimination ×…] | ||||||||
| Church attendance | −0.002 | |||||||
| Prayer | −0.003 | |||||||
| Religious social support | −0.025 | * | ||||||
| Socio-demographics | ||||||||
| Age | −0.008 | *** | −0.008 | *** | −0.008 | *** | −0.008 | *** |
| Female | 0.135 | * | 0.134 | * | 0.134 | * | 0.131 | * |
| Education | −0.006 | * | −0.006 | * | −0.006 | * | −0.006 | * |
| Married | −0.040 | −0.039 | −0.040 | −0.041 | ||||
| Employed | −0.153 | ** | −0.153 | ** | −0.152 | ** | −0.157 | ** |
| Household income | −0.025 | ** | −0.025 | ** | −0.025 | ** | −0.024 | ** |
| Constant | 2.294 | 2.388 | 2.337 | 2.303 | ||||
| R2 | 0.184 | 0.184 | 0.184 | 0.189 | ||||
| (1) | (2) | (3) | (4) | |||||
|---|---|---|---|---|---|---|---|---|
| Focal Variables | ||||||||
| Major discrimination | −0.061 | † | −0.060 | −0.066 | * | −0.060 | † | |
| Church attendance | 0.013 | 0.014 | 0.014 | 0.012 | ||||
| Prayer | 0.035 | 0.034 | 0.033 | 0.035 | ||||
| Religious social support | 0.040 | * | 0.040 | * | 0.040 | † | 0.035 | † |
| Interactions [Major discrimination ×…] | ||||||||
| Church attendance | −0.009 | |||||||
| Prayer | 0.010 | |||||||
| Religious social support | 0.025 | |||||||
| Socio-demographics | ||||||||
| Age | 0.002 | 0.002 | 0.002 | 0.002 | ||||
| Female | −0.012 | −0.013 | −0.010 | −0.009 | ||||
| Education | −0.002 | −0.001 | −0.001 | −0.001 | ||||
| Married | 0.119 | 0.121 | 0.119 | 0.121 | ||||
| Employed | −0.043 | −0.043 | −0.045 | −0.038 | ||||
| Household income | 0.045 | ** | 0.044 | ** | 0.045 | ** | 0.044 | ** |
| Constant | 2.087 | 2.051 | 2.187 | 2.101 | ||||
| R2 | 0.120 | 0.121 | 0.121 | 0.124 | ||||
| Depression | Life Satisfaction | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |||||||
| Direct Associations | ||||||||||||
| Major discrimination | 0.067 | * | 0.048 | 0.069 | ** | −0.069 | −0.049 | −0.071 | * | |||
| Attends “weekly or more” | −0.028 | −0.029 | −0.029 | 0.084 | 0.087 | 0.087 | ||||||
| Prays “several times a day” | 0.023 | 0.017 | 0.020 | 0.038 | 0.043 | 0.042 | ||||||
| Receives support “very often” | −0.137 | * | −0.135 | * | −0.118 | * | 0.099 | *** | 0.098 | *** | 0.074 | * |
| Interactions [Major discrimination ×…] | ||||||||||||
| Attends “weekly or more” | −0.015 | 0.023 | ||||||||||
| Prays “several times a day” | 0.027 | −0.022 | ||||||||||
| Receives support “very often” | −0.071 | * | 0.093 | * | ||||||||
| Constant | 2.303 | 2.308 | 2.301 | 2.214 | 2.208 | 2.216 | ||||||
| R2 | 0.190 | 0.191 | 0.194 | 0.118 | 0.118 | 0.122 | ||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ellison, C.G.; DeAngelis, R.T.; Güven, M. Does Religious Involvement Mitigate the Effects of Major Discrimination on the Mental Health of African Americans? Findings from the Nashville Stress and Health Study. Religions 2017, 8, 195. https://doi.org/10.3390/rel8090195
Ellison CG, DeAngelis RT, Güven M. Does Religious Involvement Mitigate the Effects of Major Discrimination on the Mental Health of African Americans? Findings from the Nashville Stress and Health Study. Religions. 2017; 8(9):195. https://doi.org/10.3390/rel8090195
Chicago/Turabian StyleEllison, Christopher G., Reed T. DeAngelis, and Metin Güven. 2017. "Does Religious Involvement Mitigate the Effects of Major Discrimination on the Mental Health of African Americans? Findings from the Nashville Stress and Health Study" Religions 8, no. 9: 195. https://doi.org/10.3390/rel8090195
APA StyleEllison, C. G., DeAngelis, R. T., & Güven, M. (2017). Does Religious Involvement Mitigate the Effects of Major Discrimination on the Mental Health of African Americans? Findings from the Nashville Stress and Health Study. Religions, 8(9), 195. https://doi.org/10.3390/rel8090195