“Enablement”—Spirituality Engagement in Pre-Registration Nurse Education and Practice: A Grounded Theory Investigation




{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Definitions
1.2. Holistic Care
1.3. Spirituality Education
2. Method
2.1. Design
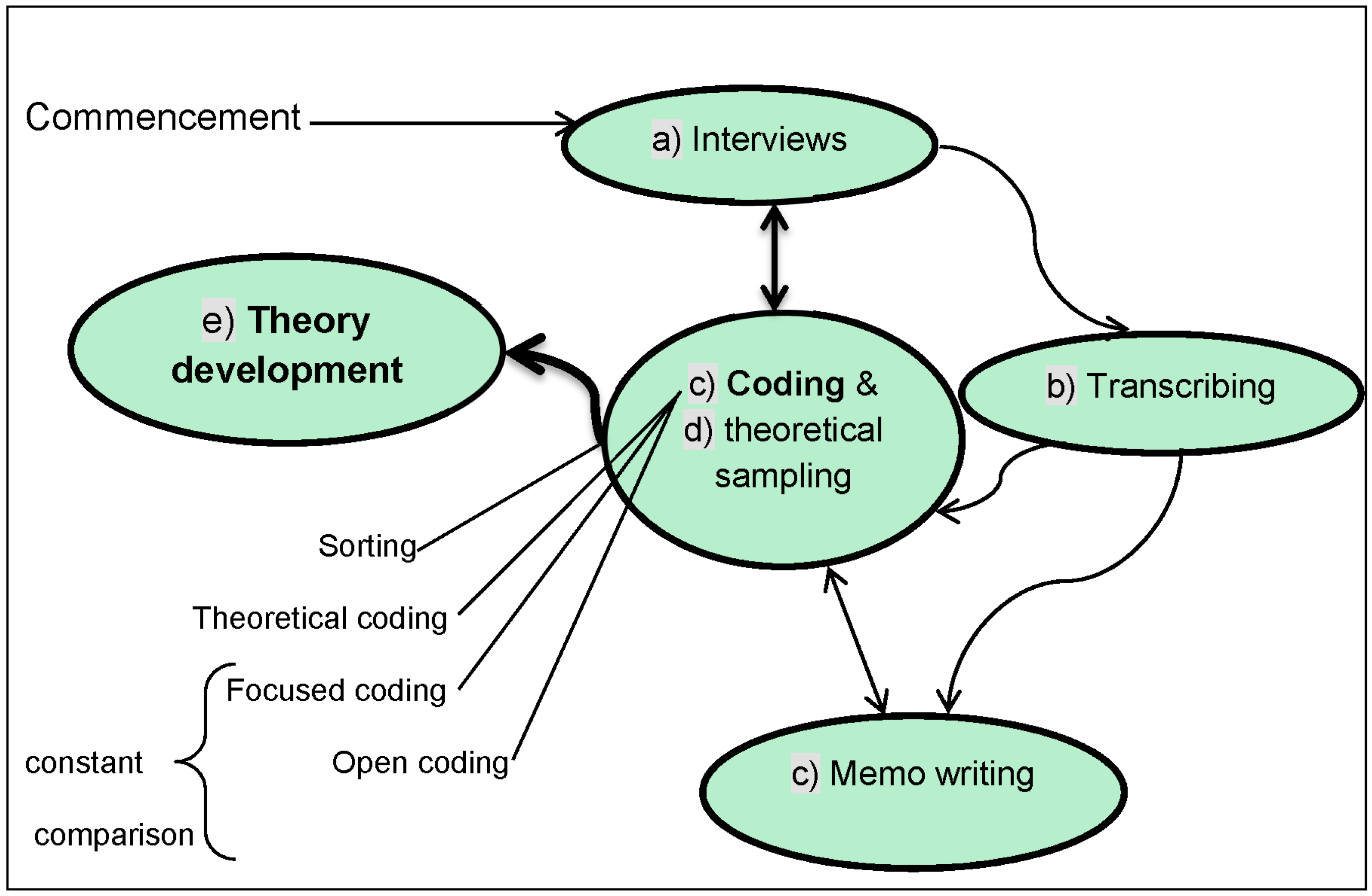
2.2. Grounded Theory Process
2.3. Participants
2.4. Ethical Considerations
2.5. Data Collection
- What do you understand spirituality to be?
- In what ways do you think spirituality education in your nursing course prepared you to meet the spiritual needs of patients?
- How could you recognise if a patient has a spiritual need?
- In what ways have you met the spiritual needs of patients?
2.6. Rigour
2.7. Data Analysis
2.7.1. The Main Concern
2.7.2. Explaining Spirituality
I think it’s a bit of everything really, a lot of the caring side of nursing. It doesn’t necessarily need to be religious ….(P3)
I think it’s quite hard… to really clarify what spirituality is, so I think it’s kind of up to you to make your mind up yourself.(P4)
2.7.3. Remembering Spirituality Education and the Content
Anything I can remember was from the third year.(P6)
This inability of a number of participants to remember when spirituality education took place in the earlier years of their nursing programme and the actual content of the same concur with the findings in a study by Linda et al. (2015) whereby the research sample were unable to remember what, when, and how they learned spiritual care. However, in this investigation, information overload was given as one probable reason for such an occurrence, as expressed below:I think we had a couple of sessions, I don’t know whether it was the first year … but I remember we definitely had dedicated sessions in the second and third year, but I can’t remember back to the first—too long ago for me to remember.(P7)
However, the infinitesimal spirituality content in the overall curriculum, and its sometimes unobtrusive presence, compared to the more obvious representation of other subjects in the nursing programme is an important factor:I think when you are in the first year there’s so much to take on board, it [spirituality] probably was there but not as much as in my third year … I don’t really recollect the first year to be honest.(P10)
However, this common occurrence of participants’ inability to remember accurately when spirituality was covered in their nursing programme could also suggest the low priority given to this domain in nurse education. Nevertheless, even a limited amount of spirituality education has the potential to create an interest for further knowledge and understanding of the concept:I think too much is focused on the clinical, the condition rather than the other needs of the patient. They all go on about holistic care—but what does holistic care encompass really, whereas we focus a lot on interventions and how that directly affects the patient, rather than the other side [spiritual].(P5)
I think anything I can remember was from the third year … it was just one lecture, from a professor trying to explain what spirituality was … it was too short … But then I actually wanted to know more, understand it better but you didn’t have that opportunity ….(P6)
I think it’s mentioned a lot over the three years—but it’s involved in … cultural beliefs and stuff we have … I wouldn’t say we specifically have focus on spirituality.(P8)
The fact that participants remembered some spirituality education in their third year seems logical, being the most recent coverage of the subject. However, there is no denying their desire for more formal spirituality education.One of the modules was very ethics based, so we did discuss spiritual beliefs and spirituality quite a bit in that particular module.(P9)
I think there should be something [spirituality content] every year as we have in other subjects.(P2)
Thus, a conclusion from Phase 1 is that spirituality education does not occupy a consistent recognisable place in the nursing programme. In addition, some participants had uncertainties about facilitating patients’ spiritual needs.I think as nurses we need more support and guidance and understanding what spirituality is and how we can help … I think it’s something that needs to be looked at more often throughout the three years of training.(P6)
2.7.4. Uncertainties Surrounding Facilitation of Spiritual Needs
The nursing student’s role is seen as limited in terms of not being able to adequately recognise patients’ needs in general. Furthermore, participants expressed some caution in trying to meet spiritual needs within professional boundaries, especially for fear of unfavourable accusations, if misunderstood by patients or colleagues, for example:I know I am … still learning about recognising needs, but also I think you’re very aware of not just spirituality but other things in general. You’re very aware of what you can and can’t say because you know you’ve got limitations … not go over the boundaries of what we should be doing as a … student nurse.(P1)
Clearly, there appears to be an element of cognitive dissonance in relation to spiritual care of a religious nature. However, some participants realised that attending to spiritual needs was included in a broader integral frame:There was something in the media a while ago wasn’t there about a nurse who prayed with a patient? and she got into terrible trouble for it? … You need to keep your distance at the same time as keep caring for them and meeting their other needs—I think it’s [spiritual care] something you should be able to do—but I don’t know where the boundaries are.(P2)
I think it’s [spiritual care] built into what you do anyway ….(P12)
So spiritual care can be unobtrusive within other nursing activities, and trying to identify specific examples could be difficult at times.It’s difficult to point out really … I couldn’t maybe point out one scenario where I feel I have met a patient’s spiritual needs, but you know, you sit and you talk to patients and you support.(P4)
However, participants who had palliative nursing experience were in no doubt that spiritual care is prominent:… to me just being there … we are meeting the spiritual need without realising that we are doing it.(P13)
I spent a lot of time with palliative care … in that setting it [spirituality] was a very big part of the nursing care.(P3)
There is agreement that the spirituality education acquired as a result of palliative care experience was substantial; also, theory and practice came together in a rounded learning experience. In addition, the importance of the spiritual dimension for other patients is highlighted.I went to a hospice palliative care setting, … it kind of introduced to you that there is more about people’s wants and beliefs and things, and it [spirituality] is highlighted how important it is to address those needs … from that I have been able to understand it in other areas of nursing.(P12)
3. Findings
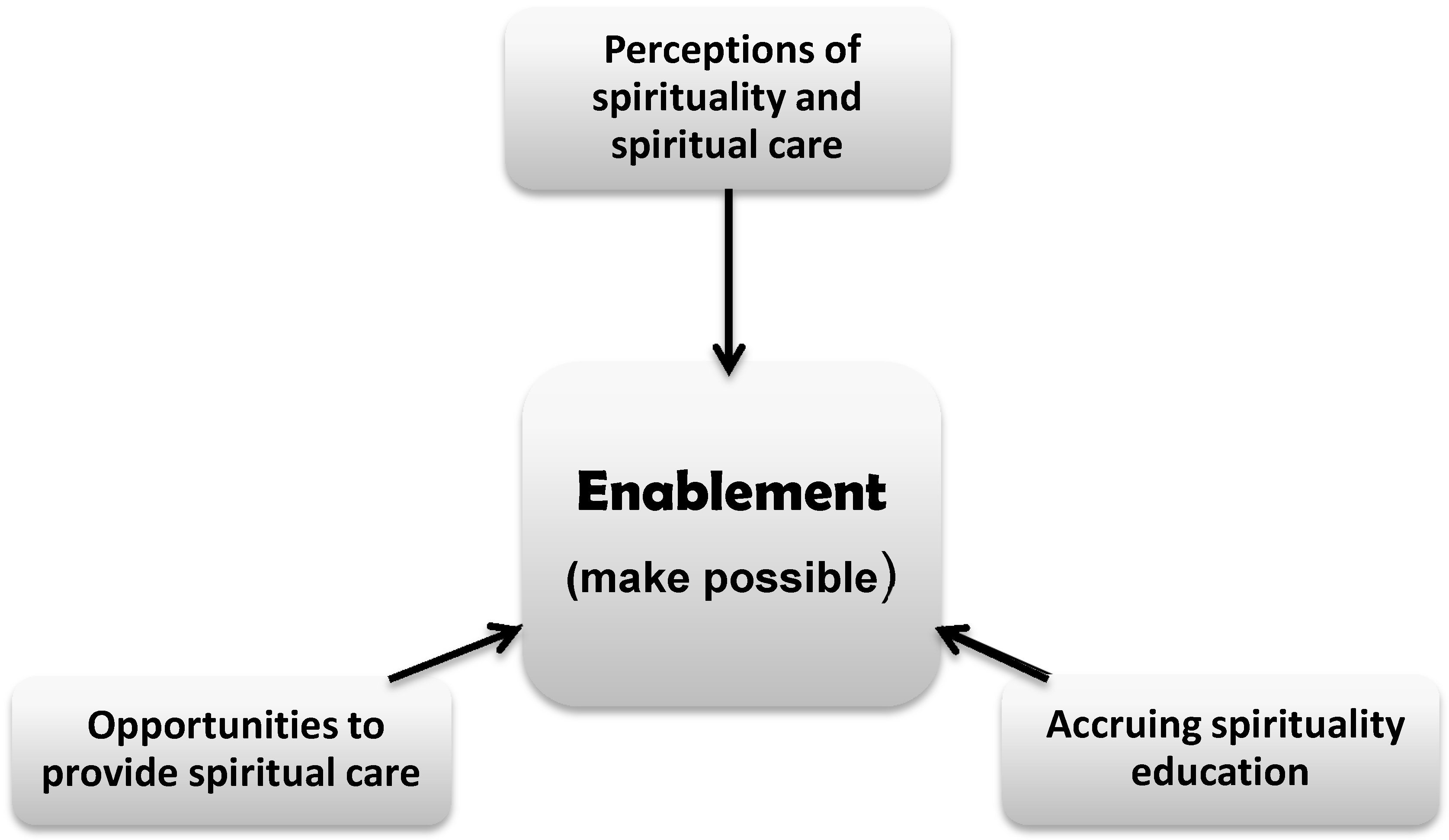
3.1. The Substantive Theory
3.2. Perceptions of Spirituality and Spiritual Care
I kind of believe that spirituality is not a particular religion, I say it’s more your own personal beliefs ….(P9)
Here, efforts were being made to explain spirituality. Moreover, perceiving spiritual care opportunities was enlightening.I think spirituality is something that everybody feels or has, it’s linked with who you are—your soul and your belief systems ….(P11)
On reflection, participants could identify spiritual care in their everyday nursing practice. Accordingly, ‘Fundamental Spiritual Care’ in the form of respect, dignity, and compassion was important.We do touch their spiritual life … nursing is already a spiritual job. Nursing patients you are already touching their spiritual life … treating your patient with dignity, compassion, and respect is also another way of showing spiritual care ….(P13)
3.3. Accruing Spirituality Education
We had a very good, very informative lecture … I thought, wow! this is something really important, something that we need to cover … I don’t think it was covered enough by any means … I went out thinking I really would like to follow-up and read some more … get a better understanding of it, something that I would like to look into further.(P2)
Any spiritual care that I think I’ve picked up has all been … seeing other nurses and healthcare professionals you know go about this … or from personal experiences from family and friends.(P6)
Nevertheless, participants acknowledged that the small amount of formal spirituality input received together with relevant life experience, innate resources, and any experiential learning, all contributed to their education in this area. However, they also recognised that knowledge and understanding of spirituality and spiritual care was an on-going process.Perhaps it’s an innate thing—being able to respond to peoples’ spiritual needs and listening and that kind of thing.(P7)
3.4. Opportunities to Provide Spiritual Care
Getting somebody in that is from their religion … you can just sit and listen to them really, it’s accepting … you are there to support them … to me, holding someone’s hand as they die, to me is as spiritual as it can get really … as they are passing over into you know, their other life….(P4)
All three main categories relating to “Enablement” (see Figure 3) will now be explained.I think just touching her hands and holding her hand when I went and spoke to her helped her ….(P7)
3.5. Perceptions of Spirituality and Spiritual Care and ‘Enablement’
3.6. Accruing Spirituality Education and ‘Enablement’
3.7. Opportunities to Provide Spiritual Care and ‘Enablement’
4. Discussion
5. Limitations of the Investigation
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Barnum, Barbara Stevens. 2011. Spirituality in Nursing: The Challenges of Complexity, 3rd ed. New York: Springer Publishing Company. [Google Scholar]
- Barss, Karen Scott. 2012. Building Bridges: An Interpretive Phenomenological Analysis of Nurse Educatiors’ Clinical Experience Using the T.R.U.S.T. Model of Inclusive Spiritual Care. International Journal of Niursing Education Scholarship 9: 1–15. [Google Scholar]
- Bradshaw, Ann. 1994. Lighting the Lamp: The Spiritual Dimension of Nursing Care. London: Scutari Press. [Google Scholar]
- Byrne, Marjory. 2002. Spirituality in Palliative Care: What Language Do We Need? International Journal of Palliative Nursing 8: 67–74. [Google Scholar] [CrossRef] [PubMed]
- Caldeira, Sílvia, Amélia Simões Figueiredo, Ana Paula da Conceição, Célia Ermel, João Mendes, Erika Chaves, Emília Campos de Carvalho, and Margarida Vieira. 2016. Spirituality in the undergraduate curricula of nursing schools in Portugal and São Paulo-Brazil. Religions 7: 134. [Google Scholar] [CrossRef]
- Callister, Lynn A. Clark, Elaine Bond, Gerry Matsumura, and Sandra Mangum. 2004. Threading Spirituality Throughout Nursing Education. Holistic Nursing Practice 18: 160–66. [Google Scholar] [CrossRef] [PubMed]
- Carroll, Barbara. 2001. A Phenomenological Exploration of the Nature of Spirituality and Spiritual Care. Mortality 6: 81–98. [Google Scholar] [CrossRef]
- Chan, Moon Fai. 2009. Factors Affecting Nursing Staff in Practising Spiritual Care. Journal of Clinical Nursing 19: 2128–36. [Google Scholar] [CrossRef] [PubMed]
- Charmaz, Kathy. 2006. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis. London: Sage Publications Ltd. [Google Scholar]
- Charmaz, Kathy. 2009. Shifting the Grounds: Constructivist Grounded Theory Methods. In Developing Grounded Theory: The Second Generation. Edited by Janice M. Morse, Phyllis Noerager Stern, Juliet Corbin, Barbara Bowers, Kathy Charmaz and Adele E. Clarke. Walnut Creek: Left Coast Press Inc. [Google Scholar]
- Charmaz, Kathy. 2014. Constructing Grounded Theory, 2nd ed. London: Sage Publications Ltd. [Google Scholar]
- Clarke, Adele E. 2005. Situational Analysis: Grounded Theory after the Postmodern Turn. Thousand Oaks: Sage Publications. [Google Scholar]
- Clarke, Janice. 2013. Spiritual Care in Everyday Nursing Practice: A New Approach. Basingstoke: Palgrave Macmillan. [Google Scholar]
- Cone, Pamela Meryl Heneise, and Tove Giske. 2013. Teaching Spiritual Care—A Grounded Theory Study among Undergraduate Nursing Educators. Journal of Clinical Nursing 22: 1951–60. [Google Scholar] [CrossRef] [PubMed]
- Corbin, Juliet, and Anselm L. Strauss. 2008. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. London: Sage Publications Ltd. [Google Scholar]
- De Chesney, Mary, ed. 2015. Nursing Research Using Grounded Theory: Qualitative Designs and Methods in Nursing. New York: Springer Publishing Company. [Google Scholar]
- Denscombe, M. 2014. The Good Research Guide: For Small-scale Social Research Projects, 5th ed. Maidenhead: Open University Press. [Google Scholar]
- Dey, Ian. 1999. Grounding Grounded Theory: Guidelines for Qualitative Inquiry. London: Academic Press. [Google Scholar]
- Dey, Ian. 2007. Grounding Categories. In The Sage Handbook of Grounded Theory. Edited by Antony Bryant and Kathy Charmaz. London: Sage Publications Ltd. [Google Scholar]
- Du Plessis, Emmerentia, Magdalene P. Koen, and Petra Bester. 2013. Exploring Home Visits in a Faith Community as a Service-Learning Opportunity. Nurse Education Today 33: 766–71. [Google Scholar] [CrossRef] [PubMed]
- Gibson, Barry, and Jan Hartman. 2014. Rediscovering Grounded Theory. London: Sage Publications Ltd. [Google Scholar]
- Giske, Tove, and Pamela Meryl Heneise Cone. 2012. Opening up to Learning Spiritual Care of Patients: A Grounded Theory Study of Nursing Students. Journal of Clinical Nursing 21: 2006–15. [Google Scholar] [CrossRef] [PubMed]
- Glaser, Barney G. 1978. Theoretical Sensitivity: Advances in the Methodology of Grounded Theory. San Francisco: Sociology Press. [Google Scholar]
- Glaser, Barney G., and Judith Holton. 2004. Remodeling Grounded Theory. Forum: Qualitative Social Research 5. [Google Scholar] [CrossRef]
- Glaser, Barney G., and Anselm L. Strauss. 1967. The Discovery of Grounded Theory: Strategies for Qualitative Research. New Brunswick: Aldine Transaction. [Google Scholar]
- Golberg, Bernice. 1998. Connection: An Exploration of Spirituality in Nursing Care. Journal of Advanced Nursing 27: 836–42. [Google Scholar] [CrossRef] [PubMed]
- Greenstreet, Wendy M. 1999. Teaching Spirituality in Nursing: A Literature Review. Nurse Education Today 19: 649–58. [Google Scholar] [CrossRef] [PubMed]
- Healthcare Quality Improvement Partnership. 2016. End of Life Care Audit—Dying in Hospital National Report for England 2016. London: Royal College of Physcians. [Google Scholar]
- Henderson, Virginia. 1966. Nature of Nursing. New York: Macmillan. [Google Scholar]
- ICN. 2012. The ICN Code of Ethics for Nurses. Geneva: International Council of Nurses. [Google Scholar]
- Ivtzan, Itai, Christine P. L. Chan, Hannah E. Gardner, and Kiran Prashar. 2013. Linking Religion and Spirituality with Psychological Well-Being: Examining Self-Actualisation, Meaning in Life, and Personal Growth Initiative. Journal of Religion and Health 52: 915–29. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J. O., H. S. Jo, and S. H. Kim. 2016. Effect of the Spiritual Care Module Education Program for Nurses. The Journal of Korean Academic Society of Nursing Education 22: 51–62. [Google Scholar] [CrossRef]
- Krentzman, A. R. 2013. Why Is Spirituality Important? In Taking Charge of Your Health & Wellbeing. Minneapolis: Center for Spirituality & Healing. [Google Scholar]
- Lewinson, Lesline P., Wilfred McSherry, and Peter Kevern. 2015. Spirituality in Pre-Registration Nurse Education and Practice: A Review of the Literature. Nurse Education Today 35: 806–14. [Google Scholar] [CrossRef] [PubMed]
- Linda, Ntombizodwa S., Hester C. Klopper, and Deliwe R. Phetlhu. 2015. Students’ voices on spiritual care at a higher education institution in the Western Cape. Curationis 32: 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcsherry, Wilfred, and Steve Jamieson. 2011. An online survey of nurses’ perceptions of spirituality and spiritual care. Journal of Clinical Nursing 20: 1757–67. [Google Scholar] [CrossRef] [PubMed]
- Mcsherry, Wilfred, and L. Ross. 2015. Heed The Evidence on Place of Spiritual Needs in Health Care. Nursing Standard 29: 33. [Google Scholar] [CrossRef] [PubMed]
- Mcsherry, Wilfred, Mark Gretton, Peter Draper, and Roger Watson. 2008. The Ethical Basis of Teaching Spirituality and Spiritual Care: A Survey of Student Nurses’ Perceptions. Nurse Education Today 28: 1002–8. [Google Scholar] [CrossRef] [PubMed]
- Mooney, Bróna, and Fiona Timmins. 2007. Spirituality as a universal concept: Student experience of learning about spirituality through the medium of art. Nurse Education in Practice 7: 275–84. [Google Scholar] [CrossRef] [PubMed]
- Morse, Janice M., Juliet M. Corbin, Phyllis Noerager Stern, Barbara Bowers, and Adele E. Clarke, eds. 2009. Developing Grounded Theory: The Second Generation. Walnut Creek: Left Coast Press Inc. [Google Scholar]
- Narayanasamy, A. 2010. Recognising Spiritual Needs. In Spiritual Assessment in Healthcare Practice. Edited by Wilfred McSherry and Linda Ross. Keswick: M & K Publishing. [Google Scholar]
- Nardi, D., and L. Rooda. 2011. Spirituality-Based Nursing Practice by Nursing Students: An Exploratory Study. Journal of professional Nursing 27: 255–63. [Google Scholar] [CrossRef] [PubMed]
- NMC. 2010. Standards for Pre-Registration Nursing Education. London: NMC. [Google Scholar]
- Olson, J. K., P. Paul, L. Douglass, M. B. Clark, J. Simington, and N. Goddard. 2003. Addressing the Spiritual Dimension in Canadian Undergraduate Nursing Education. Canadian Journal of Nursing Research 35: 95–107. [Google Scholar]
- Orem, Dorothea E. 1985. Nursing: Concepts of Practice. New York: Mcgraw Hill. [Google Scholar]
- Paley, John. 2008. Spirituality and Nursing: A Reductionist Approach. Nursing Philosophy 9: 3–18. [Google Scholar] [CrossRef] [PubMed]
- Parahoo, Kadar. 2006. Nursing Research: Principles, Process and Issues, 2nd ed. Palgrave Macmillian: Basingstoke. [Google Scholar]
- Parahoo, Kadar. 2014. Nursing Research: Principles, Process and Issues, 3rd ed. Palgrave Macmillan: Basingstoke. [Google Scholar]
- Pike, Joanne. 2011. Spirituality in Nursing: A Systematic Review of the Literature from 2006–2010. British Journal of Nursing 20: 743–49. [Google Scholar] [CrossRef] [PubMed]
- Puchalski, Christina M., Beverly Lunsford, Mary H. Harris, and Rabbi Tamara Miller. 2006. Interdisciplinary spiritual care for seriously ill and dying patients: A collaborative model. Cancer Journal 12: 398–416. [Google Scholar] [CrossRef]
- RCN. 2011. Spirituality in Nursing Care: A Pocket Guide. Edited by R. C. O. Nursing. London: RCN. [Google Scholar]
- Ross, Linda A., Tove Giske, Wilfred McSherry, Aru Narayanasamy, Carmel Downes, Paul Jarvis, and Annemiek Schep-Akkerman. 2014. Student Nurses Perceptions of Spirituality and Competence in Delivery Spiritual Care: A European Pilot Study. Nurse Education Today 34: 697–702. [Google Scholar] [CrossRef] [PubMed]
- Ross, Linda, Tove Giske, René van Leeuwen, Donia Baldacchino, Wilfred McSherry, Aru Narayanasamy, Paul Jarvis, and Annemiek Schep-Akkerman. 2016. Factors Contributing to Student Nurses‘/Midwives’ Perceived Competency in Spiritual Care. Nurse Education Today 36: 445–51. [Google Scholar] [CrossRef] [PubMed]
- Stoll, R. I. 1989. The essence of spirituality. In CARSON. Edited by V. B. Spiritual Dimensions of Nursing Practice. Philadelphia: W. B. Saunders Company. [Google Scholar]
- Swinton, John. 2001. Spirituality and Mental Health Care: Rediscovering a ‘Forgotten’ Dimension. London: Jessica Kingsley. [Google Scholar]
- Swinton, John, and Stephen Pattison. 2010. Moving beyond clarity: Towards a thin, vague, and useful understanding of spirituality in nursing care. Nursing Philosophy 11: 226–37. [Google Scholar] [CrossRef] [PubMed]
- Thomas, Jacki. 2015. Hospice Chaplains: Talking About Spiritual Care and Avoiding the Modern Day ‘Inquisition’. Journal for the Study of Spirituality 5: 60–69. [Google Scholar] [CrossRef]
- Tiew, Lay Hwa, and Debra K. Creedy. 2012. Development and Preliminary Validation of a Composite Spiritual Care-Giving Scale. International Journal of Nursing Studies 49: 682–90. [Google Scholar] [CrossRef] [PubMed]
- Tiew, Lay Hwa, Debra K. Creedy, and M. F. Chan. 2013. Student nurses’ perspectives of spirituality and spiritual care. Nurse Education Today 33: 574–79. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, R., and B. Cusveller. 2004. Nursing competences for spiritual care. Journal of Advanced Nursing 48: 234–46. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, René, Lucas J. Tiesinga, Berrie Middel, Doeke Post, and Henk Jochemsen. 2008. The effectiveness of an educational programme for nursing students on developing competence in the provision of spiritual care. Journal of Clinical Nursing 17: 2768–81. [Google Scholar] [CrossRef] [PubMed]
- Visser, Anja, Bert Garssen, and Ad Vingerhoets. 2010. Spirituality and Well-Being in Cancer Patients: A Review. Psychooncology 19: 565–72. [Google Scholar] [CrossRef] [PubMed]
- Wallace, Meredith, Suzanne Campbell, Sheila C. Grossman, Joyce M. Shea, Jean W. Lange, and Theresa T. Quell. 2008. Integrating Spirituality into Undergraduate Nursing Curricula. International Journal of Nursing Education Scholarship 5: 1–13. [Google Scholar] [CrossRef] [PubMed]
- Watson, J. 1988. Nursing: Human Science and Human Care, the Theory of Nursing. New York: National League of Nursing Press. [Google Scholar]
- Watson, J. 1997. The theory of Human Caring: retrospective and prospective. Nursing Science Quarterly 10: 49–52. [Google Scholar] [CrossRef] [PubMed]
- Watson, J. 2012. Human Caring Science: A Theory of Nursing, 2nd ed. Sudbury: Jones & Bartlett Learning. [Google Scholar]
- Weathers, Elizabeth, Geraldine McCarthy, and Alice Coffey. 2015. Concept Analysis of Spirituality: An Evolutionary Approach. Nursing Forum 51: 79–96. [Google Scholar] [CrossRef] [PubMed]
- WHO. 2002. Whoqol—Srpb Field-Test Instrument. Available online: http://www.who.int/mental_health/media/en/622.pdf (accessed on 9 June 2014).
- Wright, S., and J. Neuberger. 2012. Why Spirituality Is Essential For Nurses. Nursing Standard 26: 19–21. [Google Scholar] [CrossRef] [PubMed]
- Young, Caroline, and Cyndie Koopsen. 2005. Spirituality, Health, and Healing. Boston: Jones and Bartlett Publishers International. [Google Scholar]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewinson, L.P.; McSherry, W.; Kevern, P. “Enablement”—Spirituality Engagement in Pre-Registration Nurse Education and Practice: A Grounded Theory Investigation. Religions 2018, 9, 356. https://doi.org/10.3390/rel9110356
Lewinson LP, McSherry W, Kevern P. “Enablement”—Spirituality Engagement in Pre-Registration Nurse Education and Practice: A Grounded Theory Investigation. Religions. 2018; 9(11):356. https://doi.org/10.3390/rel9110356
Chicago/Turabian StyleLewinson, Lesline P., Wilfred McSherry, and Peter Kevern. 2018. "“Enablement”—Spirituality Engagement in Pre-Registration Nurse Education and Practice: A Grounded Theory Investigation" Religions 9, no. 11: 356. https://doi.org/10.3390/rel9110356
APA StyleLewinson, L. P., McSherry, W., & Kevern, P. (2018). “Enablement”—Spirituality Engagement in Pre-Registration Nurse Education and Practice: A Grounded Theory Investigation. Religions, 9(11), 356. https://doi.org/10.3390/rel9110356