

Public Health Impact and Health System Preparedness within a Changing Climate in Bangladesh: A Scoping Review
Abstract
:1. Introduction
2. Methods
2.1. Identifying the Research Question
2.2. Identifying Relevant Studies
2.3. Study Selection
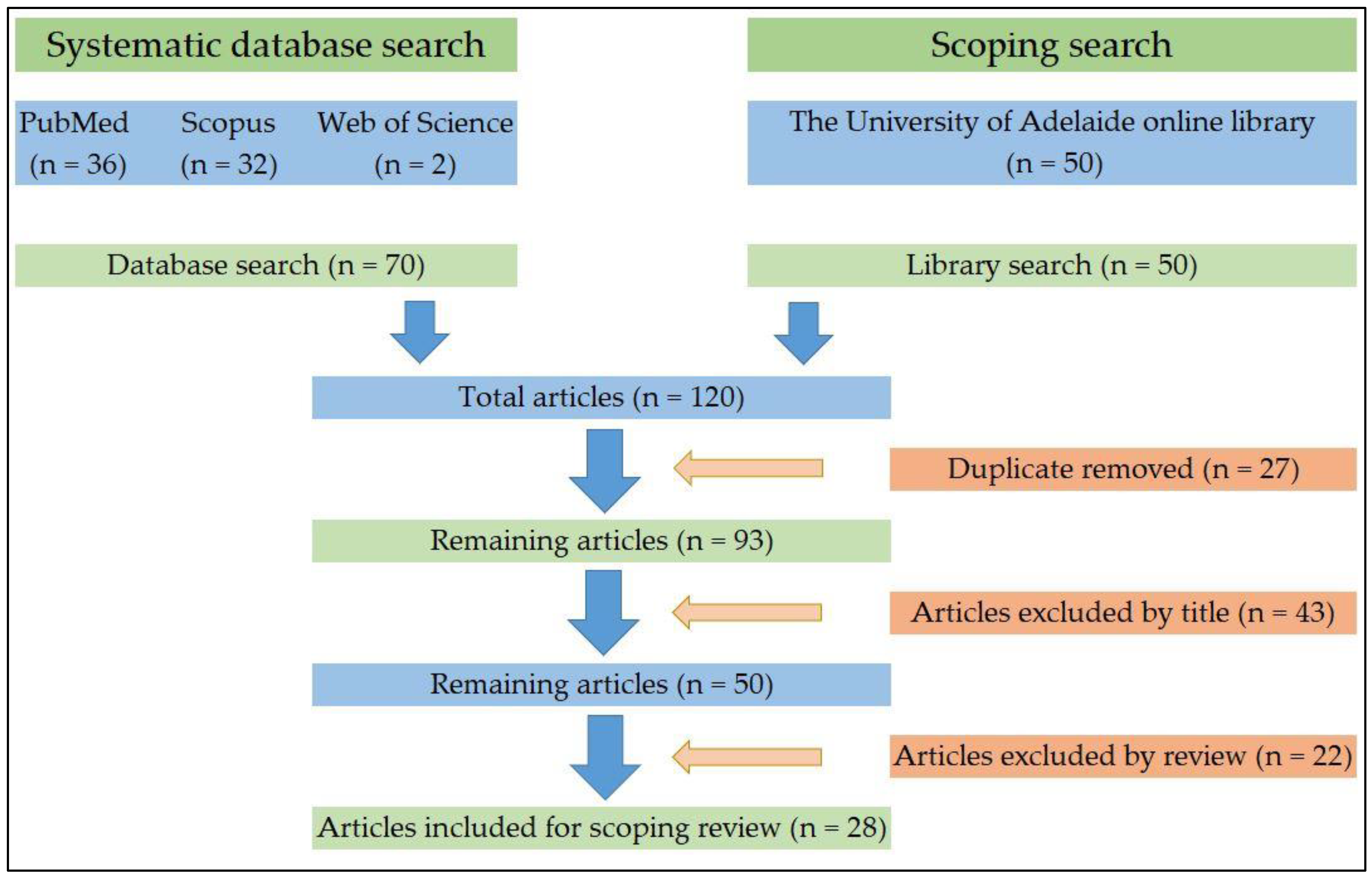
2.3.1. Search Result
2.3.2. Summary of the Results
2.4. Charting the Data
2.5. Collating, Summarizing and Reporting the Results
3. Results
3.1. Health Gains and Achievements
3.2. Bangladesh’s Pluralistic Health System
3.3. Health Policy and Governance Structure
3.4. Bangladesh’s Intrinsic Vulnerability to Climate Change
3.5. Climate Change Impact on Public Health
3.6. Climate Change Preparedness/Health Adaptation in Bangladesh
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| “Health Adaptation” | “Climate Change and Health” | “Health System in Bangladesh” |
|---|---|---|
| “Health adaptation” OR “Policies and practice” OR “Adaptation planning” OR “Policy” OR “Guideline” OR “National Health Policy” OR “Health Policy” OR “Operational Plans” OR “Action plan” OR “Public Policy +” OR “Strategy” OR “Government policy” OR “Strategic plan” OR “Action” OR “Policy reformation” OR “Health policy evaluation” OR “Health sector adaptation” OR “Health sector resilience” OR “Health sector preparedness” OR “health system adaptation” OR “action plan” | “Climate change and health” OR “Global Warming and health” OR “Sea Level Rise and health” OR “Climate change and Adolescent Health” OR “Climate change and Child Health” OR “Climate change and Global Health” OR “Climate change and Infant Health” OR “Climate change and Mental Health” OR “Climate change and Occupational Health” OR “Climate change and One Health” OR “Climate change and Population Health” OR “Climate change and Rural Health” OR “Climate change and Suburban Health” OR “Climate change and Urban Health” OR “Climate change and coastal health” OR “Climate change and Public Health” OR “Climate change and Reproductive Health” OR “Climate change and Social Determinants of Health” OR “Climate change and Men’s health” OR “Climate change and Women’s Health” OR “Climate change and Maternal Health” OR “Climate change and mental health” | “Bangladesh health sector” OR “Health in Bangladesh” OR “Bangladesh health sector” OR “Health system in Bangladesh” OR “Health policy Bangladesh” OR “National Health policy Bangladesh” OR “Climate Change Strategy and Action Plan Bangladesh” OR “National Adaptation Plan for Action Bangladesh” OR “Health, Population and Nutrition Sector Programme Bangladesh” OR “4th Health, Population and Nutrition Sector Programme” OR “4th HPNSP” |
| 1,926,890 | 9003 | 3693 |
| Initial hits | 44 results | |
| Final hits (after applying other filters) | 36 results | |
Appendix B
| S/n | Author—Article Title—Article Reference | Reason for Exclusion |
|---|---|---|
| 1 | Ahasan N. Climate change: Impact on health. Journal of Medicine. 2010;11(1):1–2. | Editorial |
| 2 | Alam N, Chowdhury HR, Ahmed A, Rahman M, Streatfield PK. Distribution of cause of death in rural Bangladesh during 2003–2010: evidence from two rural areas within Matlab Health and Demographic Surveillance site. Glob Health Action. 2014;7:25510. | Not useful to research topic |
| 3 | Alam N, Chowdhury HR, Das SC, Ashraf A, Streatfield PK. Causes of death in two rural demographic surveillance sites in Bangladesh, 2004–2010: automated coding of verbal autopsies using InterVA-4. Glob Health Action. 2014;7:25511. | Not useful to research topic |
| 4 | Alam N, Lindeboom W, Begum D, Streatfield PK. The association of weather and mortality in Bangladesh from 1983–2009. Glob Health Action. 2012;5:53–60. | More updated article available in the same topic |
| 5 | Bodrud-Doza M, Shammi M, Bahlman L, Islam A, Rahman MM. Psychosocial and Socio-Economic Crisis in Bangladesh Due to COVID-19 Pandemic: A Perception-Based Assessment. Front Public Health. 2020;8:341. | Article came from same/same type study—more relevant one included |
| 6 | Chatterjee S. Rights, risks and resilience: The 3Rs approach to child-centred climate change adaptation in Asian cities. Responding to Climate Change in Asian Cities: Governance for a More Resilient Urban Future2016. p. 33–55. | Not useful to research topic |
| 7 | Chowdhury MA, Hasan MK, Hasan MR, Younos TB. Climate change impacts and adaptations on health of Internally Displaced People (IDP): An exploratory study on coastal areas of Bangladesh. Heliyon. 2020;6(9). | Not useful to research topic |
| 8 | Das S, Kumar B, Kawsar LA. Disaggregated level child morbidity in Bangladesh: An application of small area estimation method. PLoS ONE. 2020;15(5). | Article came from same/same type study—more relevant one included |
| 9 | Haque MA, Yamamoto SS, Malik AA, Sauerborn R. Households’ perception of climate change and human health risks: a community perspective. Environ Health. 2012;11:1. | Article came from same/same type study—more relevant one included |
| 10 | Haque U, Hashizume M, Kolivras KN, Overgaard HJ, Das B, Yamamoto T. Reduced death rates from cyclones in Bangladesh: what more needs to be done? Bull World Health Organ. 2012;90(2):150–6. | Not useful to research topic |
| 11 | Huda MN. Understanding indigenous people’s perception on climate change and climatic hazards: a case study of Chakma indigenous communities in Rangamati Sadar Upazila of Rangamati District, Bangladesh. Natural Hazards. 2013;65(3):2147–59. | Not useful to research topic |
| 12 | Kabir A, Islam MZ, Ahmed A, Rahman MS, Rahman S. Health and drinking water supply vulnerabilities to climate variability in coastal and drought-prone areas of Bangladesh. International Journal of Climate Change: Impacts and Responses. 2019;11(2):41–56. | Not accessible |
| 13 | Kabir MI, Rahman MB, Smith W, Lusha MA, Milton AH. Climate change and health in Bangladesh: a baseline cross-sectional survey. Glob Health Action. 2016;9:29609. | Article came from same/same type study—more relevant one included |
| 14 | Khan AE, Xun WW, Ahsan H, Vineis P. Climate Change, Sea-Level Rise, & Health Impacts in Bangladesh. Environment: science and policy for sustainable development. 2011;53(5):18–33. | More updated article available in the same topic |
| 15 | Lindeboom W, Alam N, Begum D, Streatfield PK. The association of meteorological factors and mortality in rural Bangladesh, 1983–2009. Glob Health Action. 2012;5:61–73. | Not useful to research topic |
| 16 | Mobarak Hossain Khan M, KrÄMer A, Khandoker A, PrÜFer-KrÄMer L, Islam A. Trends in sociodemographic and health-related indicators in Bangladesh, 1993―2007: will inequities persist? Bulletin of the World Health Organization. 2011;89(8):583–92. | Not useful to research topic |
| 17 | Nayna Schwerdtle P, Stockemer J, Bowen KJ, Sauerborn R, McMichael C, Danquah I. A Meta-Synthesis of Policy Recommendations Regarding Human Mobility in the Context of Climate Change. International journal of environmental research and public health. 2020;17(24):9342. | Article came from same/same type study—more relevant one included |
| 18 | Rahman MM, Ahmad S. Health, livelihood and well-being in the coastal delta of Bangladesh. Ecosystem Services for Well-Being in Deltas: Integrated Assessment for Policy Analysis2018. p. 131–45. | Not useful to research topic |
| 19 | Rasul CH, Mostafa KG, Baruri NN, Ballav SK, Roy PK. Comparative study of climate related target diseasesin the coastal and plain area of Southern Bangladesh. Malaysian Journal of Public Health Medicine. 2015;15(2):24–31. | Not useful to research topic |
| 20 | Scheelbeek PFD, Chowdhury MAH, Haines A, Alam DS, Hoque MA, Butler AP, et al. Drinking Water Salinity and Raised Blood Pressure: Evidence from a Cohort Study in Coastal Bangladesh. Environ Health Perspect. 2017;125(5):057007. | Not useful to research topic |
| 21 | Schwerdtle PN, Stockemer J, Bowen KJ, Sauerborn R, McMichael C, Danquah I. A meta-synthesis of policy recommendations regarding human mobility in the context of climate change. International Journal of Environmental Research and Public Health. 2020;17(24):1–30. | Article came from same/same type study—more relevant one included |
| 22 | Shahid S. Probable Impacts of Climate Change on Public Health in Bangladesh. Asia-Pacific journal of public health. 2010;22(3):310–9. | More updated article available in the same topic |
Appendix C
| s/n | Operational Plans (OPs) | Is Climate Change Mentioned in the OP? | If Mentioned, Is There Any Specific Project and Programs on CC Included? | Is There Any Budget Allocated for the Project or Porgram? | Is There Any Indicator to Monitor Progress? | Is the Project or Program Being Integrated with Other Project or Porgrams in the Respective OP? | Score/Level of Integration |
|---|---|---|---|---|---|---|---|
| 1 | Sector-wide Program Management and Monitoring (SWPMM) | ✓ | ✓ | ✓ | ✓ | ✓ | 5/Fully integrated |
| 2 | Planning, Monitoring and Research (PMR) | ✓ | ✓ | ✓ | ✓ | ✓ | 5/Fully integrated |
| 3 | Planning, Monitoring andEvaluation (PME) | ✓ | 1/Mentioned | ||||
| 4 | Health Economics and Financing (HEF) | X | |||||
| 5 | Strengthening Drug Administration and Management (SDAM) | ✓ | 1/Mentioned | ||||
| 6 | Health Information System and E-Health (HIS and E-Health) | ✓ | ✓ | ✓ | ✓ | 4/Almost integrated | |
| 7 | Management Information System (MIS) | X | |||||
| 8 | Procurement, Storage and Supplies Management-HS (PSSM-HS) | ✓ | 1/Mentioned | ||||
| 9 | Procurement, Storage and Supplies Management FP (PSSM-FP) | X | |||||
| 10 | Human Resources Development (HRD) | X | |||||
| 11 | Medical Education and Health Manpower Development (ME and HMD) | X | |||||
| 12 | Nursing and Midwifery Education Services (NMES) | X | |||||
| 13 | Training, Research, and Development (TRD) | ✓ | ✓ | ✓ | ✓ | ✓ | 5/Fully integrated |
| 14 | Physical Facilities Development (PFD) | X | |||||
| 15 | Improved Financial Management (IFM) | X | |||||
| 16 | Maternal, Neonatal, Child and Adolscent Health (MNCAH) | ✓ | 1/Mentioned | ||||
| 17 | Maternal, Child, Reproductive and Adolscent Health (MCRAH) | X | |||||
| 18 | National Nutrition Services (NNS) | ✓ | ✓ | 2/Tried integration | |||
| 19 | Communicable Disease Control (CDC) | ✓ | ✓ | ✓ | ✓ | ✓ | 5/Fully integrated |
| 20 | Tuberculosis-Leprosy and AIDS STD Program (TBL and ASP) | ✓ | ✓ | ✓ | ✓ | ✓ | 5/Fully integrated |
| 21 | Non-communicable Disease Control (NCDC) | ✓ | ✓ | ✓ | ✓ | ✓ | 5/Fully integrated |
| 22 | National Eye Care (NEC) | X | |||||
| 23 | Community Based Healthcare (CBHC) | ✓ | ✓ | ✓ | ✓ | 4/Almost integrated | |
| 24 | Hospital Services Management (HSM) | X | |||||
| 25 | Clinical Contraception Services Delivery Program (CCSDP) | X | |||||
| 26 | Family Planning Field Services Delivery (FP-FSD) | ✓ | 1/Mentioned | ||||
| 27 | Lifestyle and Health Education and Promotion (LHEP) | ✓ | ✓ | ✓ | ✓ | ✓ | 5/Fully integrated |
| 28 | Information, Education and Communication (IEC) | X | |||||
| 29 | Alternate Medical Care (AMC) | X |
References
- IPCC. Summary for Policymakers. In Climate Change 2021: The Physical Science Basis. Contribution of Working Group I to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change; Masson-Delmotte, V., Zhai, P., Pirani, A., Connors, S.L., Péan, C., Berger, S., Caud, N., Chen, Y., Goldfarb, L., Gomis, M.I., et al., Eds.; IPCC: Geneva, Switzerland; Available online: https://www.ipcc.ch/report/ar6/wg1/downloads/report/IPCC_AR6_WGI_SPM.pdf (accessed on 25 May 2021).
- Labonté, R.; Mohindra, K.; Schrecker, T. The growing impact of globalization for health and public health practice. Annu. Rev. Public Health 2011, 32, 263–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Quantitative Risk Assessment of the Effects of Climate Change on Selected Causes of Death, 2030s and 2050s; 9241507691; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Caminade, C.; McIntyre, K.M.; Jones, A.E. Impact of recent and future climate change on vector-borne diseases. Ann. N. Y. Acad. Sci. 2019, 1436, 157–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovats, R.; Edwards, S.; Hajat, S.; Armstrong, B.; Ebi, K.; Menne, B. The effect of temperature on food poisoning: A time-series analysis of salmonellosis in ten European countries. Epidemiol. Infect. 2004, 132, 443–453. [Google Scholar] [CrossRef]
- Curriero, F.C.; Patz, J.A.; Rose, J.B.; Lele, S. The association between extreme precipitation and waterborne disease outbreaks in the United States, 1948–1994. Am. J. Public Health 2001, 91, 1194–1199. [Google Scholar] [CrossRef]
- Mora, C.; McKenzie, T.; Gaw, I.M.; Dean, J.M.; von Hammerstein, H.; Knudson, T.A.; Setter, R.O.; Smith, C.Z.; Webster, K.M.; Patz, J.A. Over half of known human pathogenic diseases can be aggravated by climate change. Nat. Clim. Chang. 2022, 12, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Keenan, H.T.; Marshall, S.W.; Nocera, M.A.; Runyan, D.K. Increased incidence of inflicted traumatic brain injury in children after a natural disaster. Am. J. Prev. Med. 2004, 26, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Kahn, M.E. The death toll from natural disasters: The role of income, geography, and institutions. Rev. Econ. Stat. 2005, 87, 271–284. [Google Scholar] [CrossRef]
- McMichael, A.J. Globalization, climate change, and human health. N. Engl. J. Med. 2013, 368, 1335–1343. [Google Scholar] [CrossRef] [Green Version]
- Watts, N.; Amann, M.; Ayeb-Karlsson, S.; Belesova, K.; Bouley, T.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Chambers, J. The Lancet Countdown on health and climate change: From 25 years of inaction to a global transformation for public health. Lancet 2018, 391, 581–630. [Google Scholar] [CrossRef]
- WHO. Protecting Health from Climate Change: Connecting Science, Policy and People; 9241598883; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Eckstein, D.; Künzel, V.; Schäfer, L.; Winges, M. Global Climate Risk Index 2020; Germanwatch: Bonn, Germany, 2019. [Google Scholar]
- World Health Organization. Bangladesh Health System Review; WHO Regional Office for the Western Pacific: Geneva, Switzerland, 2015. [Google Scholar]
- MoHFW. National Health Policy 2011; Ministry of Health and Family Welfare (MoHFW), Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2011. Available online: http://www.mohfw.gov.bd/index.php?searchword=health+policy&ordering=&searchphrase=all&Itemid=1&option=com_search&lang=en (accessed on 1 June 2021).
- Ganesh, C.; Smith, J.A. Climate change, public health, and policy: A California case study. Am. J. Public Health 2018, 108, S114–S119. [Google Scholar] [CrossRef]
- Rahman, M.M.; Ahmad, S.; Mahmud, A.S.; Hassan-uz-Zaman, M.; Nahian, M.A.; Ahmed, A.; Nahar, Q.; Streatfield, P.K. Health consequences of climate change in Bangladesh: An overview of the evidence, knowledge gaps and challenges. Wiley Interdiscip. Rev. Clim. Chang. 2019, 10, e601. [Google Scholar] [CrossRef]
- Sucharew, H.; Macaluso, M. Progress notes: Methods for research evidence synthesis: The scoping review approach. J. Hosp. Med. 2019, 14, 416–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. JBI Evid. Implement. 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. JMLA 2018, 106, 420. [Google Scholar] [CrossRef] [PubMed]
- Team, T.E. EndNote; EndNote X9; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- Tracy, S.J. Qualitative quality: Eight “big-tent” criteria for excellent qualitative research. Qual. Inq. 2010, 16, 837–851. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, F.R.; Ibrahim, Q.S.U.; Bari, M.S.; Alam, M.J.; Dunachie, S.J.; Rodriguez-Morales, A.J.; Patwary, M.I. The association between temperature, rainfall and humidity with common climate-sensitive infectious diseases in Bangladesh. PLoS ONE 2018, 13, e0199579. [Google Scholar] [CrossRef]
- Das, S.; Chandra, H.; Saha, U.R. District level estimates and mapping of prevalence of diarrhoea among under-five children in Bangladesh by combining survey and census data. PloS ONE 2019, 14, e0211062. [Google Scholar] [CrossRef]
- Dewan, A.; Hashizume, M.; Rahman, M.M.; Abdullah, A.Y.M.; Corner, R.J.; Shogib, M.R.I.; Hossain, M.F. Environmental change and kala-azar with particular reference to Bangladesh. In Kala Azar in South Asia; Springer: Berlin/Heidelberg, Germany, 2016; pp. 223–247. [Google Scholar]
- Elahi, K.M. Climate change and health impacts in Bangladesh. In Climate Change and Human Health Scenario in South and Southeast Asia; Springer: Berlin/Heidelberg, Germany, 2016; pp. 207–219. [Google Scholar]
- Haque, M.A.; Budi, A.; Malik, A.A.; Yamamoto, S.S.; Louis, V.R.; Sauerborn, R. Health coping strategies of the people vulnerable to climate change in a resource-poor rural setting in Bangladesh. BMC Public Health 2013, 13, 565. [Google Scholar] [CrossRef] [Green Version]
- Haque, M.A.; Louis, V.R.; Phalkey, R.; Sauerborn, R. Use of traditional medicines to cope with climate-sensitive diseases in a resource poor setting in Bangladesh. BMC Public Health 2014, 14, 202. [Google Scholar] [CrossRef]
- Haque, M.R.; Parr, N.; Muhidin, S. Parents’ healthcare-seeking behavior for their children among the climate-related displaced population of rural Bangladesh. Soc. Sci. Med. 2019, 226, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Huda, M.M.; Chowdhury, R.; Ghosh, D.; Dash, A.P.; Bhattacharya, S.K.; Mondal, D. Visceral leishmaniasis-associated mortality in Bangladesh: A retrospective cross-sectional study. BMJ Open 2014, 4, e005408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabir, M.I.; Rahman, M.B.; Smith, W.; Lusha, M.A.F.; Azim, S.; Milton, A.H. Knowledge and perception about climate change and human health: Findings from a baseline survey among vulnerable communities in Bangladesh. BMC Public Health 2016, 16, 266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.M.H.; Gruebner, O.; Krämer, A. Is area affected by flood or stagnant water independently associated with poorer health outcomes in urban slums of Dhaka and adjacent rural areas? Nat. Hazards 2014, 70, 549–565. [Google Scholar] [CrossRef]
- Koehlmoos, T.P.; Anwar, S.; Cravioto, A. Global health: Chronic diseases and other emergent issues in global health. Infect. Dis. Clin. 2011, 25, 623–638. [Google Scholar] [CrossRef] [PubMed]
- Mamun, M.A.; Sakib, N.; Gozal, D.; Bhuiyan, A.I.; Hossain, S.; Bodrud-Doza, M.; Al Mamun, F.; Hosen, I.; Safiq, M.B.; Abdullah, A.H. The COVID-19 pandemic and serious psychological consequences in Bangladesh: A population-based nationwide study. J. Affect. Disord. 2021, 279, 462–472. [Google Scholar] [CrossRef]
- Nahar, N.; Blomstedt, Y.; Wu, B.; Kandarina, I.; Trisnantoro, L.; Kinsman, J. Increasing the provision of mental health care for vulnerable, disaster-affected people in Bangladesh. BMC Public Health 2014, 14, 708. [Google Scholar] [CrossRef] [Green Version]
- Adams, A.M.; Ahmed, T.; El Arifeen, S.; Evans, T.G.; Huda, T.; Reichenbach, L. Innovation for universal health coverage in Bangladesh: A call to action. Lancet 2013, 382, 2104–2111. [Google Scholar] [CrossRef]
- Fahim, S.M.; Bhuayan, T.A.; Hassan, M.Z.; Abid Zafr, A.H.; Begum, F.; Rahman, M.M.; Alam, S. Financing health care in B angladesh: Policy responses and challenges towards achieving universal health coverage. Int. J. Health Plan. Manag. 2019, 34, e11–e20. [Google Scholar] [CrossRef] [Green Version]
- Haque, M. Hits and misses of bangladesh national health policy 2011. J. Pharm. Bioallied Sci. 2020, 12, 83–93. [Google Scholar] [CrossRef]
- Huq, S.; Chow, J.; Fenton, A.; Stott, C.; Taub, J.; Wright, H. (Eds.) Confronting Climate Change in Bangladesh: Policy Strategies for Adaptation and Resilience; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar] [CrossRef]
- Shafique, S.; Bhattacharyya, D.S.; Anwar, I.; Adams, A. Right to health and social justice in Bangladesh: Ethical dilemmas and obligations of state and non-state actors to ensure health for urban poor. BMC Med. Ethics 2018, 19, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasobant, S.; Saha, S.; Puwar, T.; Saxena, D. Toward the development of an integrated climate-sensitive disease surveillance in southeast asian countries: A situational analysis. Indian J. Community Med. Off. Publ. Indian Assoc. Prev. Soc. Med. 2020, 45, 270–273. [Google Scholar]
- Biswas, T.; Haider, M.M.; Gupta, R.D.; Uddin, J. Assessing the readiness of health facilities for diabetes and cardiovascular services in Bangladesh: A cross-sectional survey. BMJ Open 2018, 8, e022817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahaman, M.A.; Rahman, M.M.; Rahman, S.H. Pathways of Climate-Resilient Health Systems in Bangladesh. In Confronting Climate Change in Bangladesh. The Anthropocene: Politik—Economics—Society—Science; Huq, S., Chow, J., Fenton, A., Stott, C., Taub, J., Wright, H., Eds.; Springer: Cham, Switzerland, 2019; Volume 28. [Google Scholar] [CrossRef]
- Rahman, M.M.; Bodrud-Doza, M.; Shammi, M.; Islam, A.R.M.T.; Khan, A.S.M. COVID-19 pandemic, dengue epidemic, and climate change vulnerability in Bangladesh: Scenario assessment for strategic management and policy implications. Environ. Res. 2021, 192, 110303. [Google Scholar] [CrossRef]
- Streatfield, P.K.; Karar, Z.A. Population challenges for Bangladesh in the coming decades. J. Health Popul. Nutr. 2008, 26, 261–272. [Google Scholar] [CrossRef] [Green Version]
- Helldén, D.; Andersson, C.; Nilsson, M.; Ebi, K.L.; Friberg, P.; Alfvén, T. Climate change and child health: A scoping review and an expanded conceptual framework. Lancet Planet. Health 2021, 5, e164–e175. [Google Scholar] [CrossRef]
- Hunter, L.M.; Koning, S.; Fussell, E.; King, B.; Rishworth, A.; Merdjanoff, A.; Muttarak, R.; Riosmena, F.; Simon, D.H.; Skop, E. Scales and sensitivities in climate vulnerability, displacement, and health. Popul. Environ. 2021, 43, 61–81. [Google Scholar] [CrossRef]
- Hayward, G.; Ayeb-Karlsson, S. ‘Seeing with Empty Eyes’: A systems approach to understand climate change and mental health in Bangladesh. Clim. Chang. 2021, 165, 29. [Google Scholar] [CrossRef]
- Schwerdtle, P.N.; McMichael, C.; Mank, I.; Sauerborn, R.; Danquah, I.; Bowen, K.J. Health and migration in the context of a changing climate: A systematic literature assessment. Environ. Res. Lett. 2020, 15, 103006. [Google Scholar] [CrossRef]
- BBS. Preliminary Report on Household Income and Expenditure Survey (HIES) 2016; Bangladesh Bureau of Statistics (BBS): Dhaka, Bangladesh, 2017. [Google Scholar]
- BBS. Report on Bangladesh Sample Vital Statistics 2017; Bangladesh Bureau of Statistics (BBS): Dhaka, Bangladesh, 2018. [Google Scholar]
- GED. Millennium Development Goals Bangladesh Progress Report 2015; General Economics Division (GED): Dhaka, Bangladesh, 2015. [Google Scholar]
- Chowdhury, A.M.R.; Bhuiya, A.; Chowdhury, M.E.; Rasheed, S.; Hussain, Z.; Chen, L.C. The Bangladesh paradox: Exceptional health achievement despite economic poverty. Lancet 2013, 382, 1734–1745. [Google Scholar] [CrossRef]
- Islam, A.; Biswas, T. Health system in Bangladesh: Challenges and opportunities. Am. J. Health Res. 2014, 2, 366–374. [Google Scholar] [CrossRef]
- NIPORT; ACPR; ICF International. Bangladesh Health Facility Survey 2014; National Institute of Population Research and Training (NIPORT), Associates for Community and Population Research (ACPR), and ICF International: Dhaka, Bangladesh, 2016. [Google Scholar]
- Uddin, M.J.; Koehlmoos, T.L.; Ashraf, A.; Khan, A.; Saha, N.C.; Hossain, M. Health needs and health-care-seeking behaviour of street-dwellers in Dhaka, Bangladesh. Health Policy Plan. 2009, 24, 385–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, A. Urbanisation in Bangladesh Proves a Double-Edged Sword for Women. Available online: https://www.theguardian.com/global-development/2012/nov/05/urbanisation-bangladesh-women (accessed on 13 December 2020).
- Kelly, A. Bangladesh’s Urbanisation Creating a Healthcare Black Hole. Available online: https://www.theguardian.com/global-development/2012/sep/18/bangladesh-urbanisation-healthcare-black-hole (accessed on 13 December 2020).
- Ahmed, S.M.; Tomson, G.; Petzold, M.; Kabir, Z.N. Socioeconomic status overrides age and gender in determining health-seeking behaviour in rural Bangladesh. Bull. World Health Organ. 2005, 83, 109–117. [Google Scholar] [PubMed]
- Alam, N.; Chowdhury, H.R.; Bhuiyan, M.A.; Streatfield, P.K. Causes of death of adults and elderly and healthcare-seeking before death in rural Bangladesh. J. Health Popul. Nutr. 2010, 28, 520. [Google Scholar] [CrossRef] [Green Version]
- Ashaduzzaman, A.S.M.; Rahman, M.M.; Shamsur Rahman, M. Poor people’s access to health services in Bangladesh: Focusing on the issues of inequality. In Proceedings of the Network of Asia-Pacific Schools and Institutes of Public Administration and Governance (NAPSIPAG) Annual Conference, Beijing, China, 5–7 December 2005. [Google Scholar]
- Ahmed, S.M.; Evans, T.G.; Standing, H.; Mahmud, S. Harnessing pluralism for better health in Bangladesh. Lancet 2013, 382, 1746–1755. [Google Scholar] [CrossRef]
- Bloom, G.; Standing, H.; Lucas, H.; Bhuiya, A.; Oladepo, O.; Peters, D.H. Making health markets work better for poor people: The case of informal providers. Health Policy Plan. 2011, 26, i45–i52. [Google Scholar] [CrossRef]
- BBS. Report on the Survey of Private Healthcare Institutions 2019; Bangladesh Bureau of Statistics: Dhaka, Bangladesh, 2021. [Google Scholar]
- WHO. Health Policy. Available online: https://www.euro.who.int/en/health-topics/health-policy/health-policy (accessed on 30 August 2021).
- McMichael, C.; Waters, E.; Volmink, J. Evidence-based public health: What does it offer developing countries? J. Public Health 2005, 27, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Rajan, D.; Barroy, H.; Stenberg, K.; Schmets, G.; Kadandale, S. Strategizing National Health in the 21st Century: A Handbook; World Health Organazation: Geneva, Switzerland, 2016. [Google Scholar]
- PMMU. Program Implementation Report 2017; Programme Management and Monitoring Unit (PMMU), Planning Wing, Ministry of Health and Family Welfare: Dhaka, Bangladesh, 2017. [Google Scholar]
- Francis, A.; Maguire, R. Protection of Refugees and Displaced Persons in the Asia Pacific Region; Routledge: London, UK, 2016. [Google Scholar]
- DoE. Climate Change and Vulnerability of Bangladesh; Climate Change Cell (CCC), Department of Environment (DoE): Dhaka, Bangladesh, 2009. [Google Scholar]
- MoEFCC. Bangladesh Climate Change Strategy and Action Plan; Minsitry of Environment, Forest and Climate Change (MoEFCC), Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2009. Available online: http://cmsdata.iucn.org/downloads/bangladesh_climate_change_strategy_and_action_plan_2009.pdf (accessed on 7 June 2021).
- MFA. Climate Change Profile: Bangladesh; Ministry of Foreign Affairs of the Netherlands: The Hague, The Netherlands, 2018; Available online: www.government.nl/foreign-policy-evaluations (accessed on 5 October 2021).
- MoEFCC. National Adaptation Plan of Bangladesh (2030–2050). Dhaka: Minsitry of Environment, Forest and Climate Change (MoEFCC), Government of the People’s Republic of Bangladesh. Available online: https://www4.unfccc.int/sites/SubmissionsStaging/Documents/202211020942---National%20Adaptation%20Plan%20of%20Bangladesh%20(2023-2050).pdf (accessed on 25 October 2022).
- Karmalkar, A.; McSweeney, C.; New, M.; Lizcano, G. UNDP Climate Change Country Profiles: Bangladesh. 2012. Available online: http://country-profiles.geog.ox.ac.uk (accessed on 19 September 2021).
- Khatun, F.; Islam, A.N. Policy Agenda for Addressing Climate Change in Bangladesh: Copenhagen and Beyond; Centre for Policy Dialogue: Dhaka, Bangladesh, 2010. [Google Scholar]
- Dasgupta, S.; Huq, M.; Khan, Z.H.; Ahmed, M.M.Z.; Mukherjee, N.; Khan, M.F.; Pandey, K. Cyclones in a changing climate: The case of Bangladesh. Clim. Dev. 2014, 6, 96–110. [Google Scholar] [CrossRef]
- Immerzeel, W.; Pellicciotti, F.; Bierkens, M. Rising river flows throughout the twenty-first century in two Himalayan glacierized watersheds. Nat. Geosci. 2013, 6, 742–745. [Google Scholar] [CrossRef]
- Wright, H.; Kristjanson, P.M.; Bhatta, G.D. Understanding Adaptive Capacity: Sustainable Livelihoods and Food Security in Coastal Bangladesh; CCAFS Working Paper No. 32; CGIAR Research Program on Climate Change, Agriculture and Food Security (CCAFS): Copenhagen, Denmark, 2012. [Google Scholar]
- Nahian, M.A.; Islam, T.G.; Bala, S.K. Women in a changing climate—An analysis of gender dimension of vulnerability in coastal Bangladesh. In Proceedings of the 4th International Conference on Water & Flood Management (ICWFM-2013), Dhaka, Bangladesh, 9–11 March 2013. [Google Scholar]
- Martin, M.; Billah, M.; Siddiqui, T.; Black, R.; Kniveton, D. Policy Analysis: Climate Change and Migration Bangladesh; Refugee and Migratory Movements Research Unit (RMMRU): Dhaka, Bangladesh, 2013. [Google Scholar]
- Kulp, S.A.; Strauss, B.H. New elevation data triple estimates of global vulnerability to sea-level rise and coastal flooding. Nat. Commun. 2019, 10, 4844. [Google Scholar] [CrossRef] [Green Version]
- Philipsborn, R.; Ahmed, S.M.; Brosi, B.J.; Levy, K. Climatic drivers of diarrheagenic Escherichia coli incidence: A systematic review and meta-analysis. J. Infect. Dis. 2016, 214, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dey, N.; Alam, M.; Sajjan, A.; Bhuiyan, M.; Ghose, L.; Ibaraki, Y.; Karim, F. Assessing environmental and health impact of drought in the Northwest Bangladesh. J. Environ. Sci. Nat. Resour. 2011, 4, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Yunus, M.; Islam, M.S.; Emch, M. Influence of climate extremes and land use on fecal contamination of shallow tubewells in Bangladesh. Environ. Sci. Technol. 2016, 50, 2669–2676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, B.S.; Harris, J.B.; Khan, A.I.; Larocque, R.C.; Sack, D.A.; Malek, M.A.; Faruque, A.S.; Qadri, F.; Calderwood, S.B.; Luby, S.P. Diarrheal epidemics in Dhaka, Bangladesh, during three consecutive floods: 1988, 1998, and 2004. Am. J. Trop. Med. Hyg. 2006, 74, 1067. [Google Scholar] [CrossRef] [Green Version]
- Akanda, A.S.; Jutla, A.S.; Alam, M.; De Magny, G.C.; Siddique, A.K.; Sack, R.B.; Huq, A.; Colwell, R.R.; Islam, S. Hydroclimatic influences on seasonal and spatial cholera transmission cycles: Implications for public health intervention in the Bengal Delta. Water Resour. Res. 2011, 47. [Google Scholar] [CrossRef]
- Hashizume, M.; Faruque, A.S.; Wagatsuma, Y.; Hayashi, T.; Armstrong, B. Cholera in Bangladesh: Climatic components of seasonal variation. Epidemiology 2010, 21, 706–710. [Google Scholar] [CrossRef] [Green Version]
- Pascual, M.; Chaves, L.; Cash, B.; Rodó, X.; Yunus, M. Predicting endemic cholera: The role of climate variability and disease dynamics. Clim. Res. 2008, 36, 131–140. [Google Scholar] [CrossRef]
- Rita, R. Cholera and climate: A demonstrated relationship. Trans. Am. Clin. Climatol. Assoc. 2009, 120, 119. [Google Scholar]
- Lara, R.J.; Neogi, S.B.; Islam, M.S.; Mahmud, Z.H.; Yamasaki, S.; Nair, G.B. Influence of catastrophic climatic events and human waste on Vibrio distribution in the Karnaphuli estuary, Bangladesh. EcoHealth 2009, 6, 279–286. [Google Scholar] [CrossRef]
- Escobar, L.E.; Ryan, S.J.; Stewart-Ibarra, A.M.; Finkelstein, J.L.; King, C.A.; Qiao, H.; Polhemus, M.E. A global map of suitability for coastal Vibrio cholerae under current and future climate conditions. Acta Trop. 2015, 149, 202–211. [Google Scholar] [CrossRef]
- Dewan, A.M.; Corner, R.; Hashizume, M.; Ongee, E.T. Typhoid fever and its association with environmental factors in the Dhaka metropolitan area of Bangladesh: A spatial and time-series approach. PLoS Negl. Trop. Dis. 2013, 7, e1998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lafferty, K.D.; Mordecai, E.A. The rise and fall of infectious disease in a warmer world. F1000Research 2016, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banu, S.; Guo, Y.; Hu, W.; Dale, P.; Mackenzie, J.S.; Mengersen, K.; Tong, S. Impacts of El Niño southern oscillation and Indian Ocean dipole on dengue incidence in Bangladesh. Sci. Rep. 2015, 5, 16105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, H.L.; Haque, U.; Roy, S.; Islam, N.; Clements, A.C. Characterizing the spatial and temporal variation of malaria incidence in Bangladesh, 2007. Malar. J. 2012, 11, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MoHFW. Malaria National Strategic Plan 2015–2020; National Malaria Control Programme (NMCP), Communicable Disease Control Division, Directorate General of Health Services, Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2015.
- Caminade, C.; Kovats, S.; Rocklov, J.; Tompkins, A.M.; Morse, A.P.; Colón-González, F.J.; Stenlund, H.; Martens, P.; Lloyd, S.J. Impact of climate change on global malaria distribution. Proc. Natl. Acad. Sci. USA 2014, 111, 3286–3291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamun, M.A.; Misti, J.M.; Griffiths, M.D.; Gozal, D. The dengue epidemic in Bangladesh: Risk factors and actionable items. Lancet 2019, 394, 2149–2150. [Google Scholar] [CrossRef] [Green Version]
- Paul, K.K.; Macadam, I.; Green, D.; Regan, D.G.; Gray, R.T. Dengue transmission risk in a changing climate: Bangladesh could experience a longer dengue fever season in the future. bioRxiv 2021. [Google Scholar] [CrossRef]
- Alvar, J.; Vélez, I.D.; Bern, C.; Herrero, M.; Desjeux, P.; Cano, J.; Jannin, J.; Boer, M.D.; Team, W.L.C. Leishmaniasis worldwide and global estimates of its incidence. PLoS ONE 2012, 7, e35671. [Google Scholar] [CrossRef] [PubMed]
- Rahman, R.; Bangali, M.; Kabir, H.; Naher, F.; Mahboob, S. Kala-azar situation in Bangladesh. In Natinal Guideline and Training Module for Kala-azar Elimination in Bangladesh; Directorate General of Health Services, Ministry of Health and Family Welfare: Dhaka, Bangladesh, 2008. [Google Scholar]
- Bern, C.; Chowdhury, R. The epidemiology of visceral leishmaniasis in Bangladesh: Prospects for improved control. Indian J. Med. Res. 2006, 123, 275–288. [Google Scholar]
- Hossain, M.; Noiri, E.; Moji, K. Climate change and kala-azar. In Kala Azar in South Asia; Springer: Berlin/Heidelberg, Germany, 2011; pp. 127–137. [Google Scholar]
- Kendall, E.A.; LaRocque, R.C.; Bui, D.M.; Galloway, R.; Ari, M.D.; Goswami, D.; Breiman, R.F.; Luby, S.; Brooks, W.A. Leptospirosis as a cause of fever in urban Bangladesh. Am. J. Trop. Med. Hyg. 2010, 82, 1127–1130. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.Z.; Islam, M.; Hossain, M.; Rahman, M.; Islam, A.; Siddika, A.; Hossain, M.; Sultana, S.; Rahman, M.; Klena, J. Genetic diversity of Nipah virus in Bangladesh. Int. J. Infect. Dis. 2021, 102, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Daszak, P.; Zambrana-Torrelio, C.; Bogich, T.L.; Fernandez, M.; Epstein, J.H.; Murray, K.A.; Hamilton, H. Interdisciplinary approaches to understanding disease emergence: The past, present, and future drivers of Nipah virus emergence. Proc. Natl. Acad. Sci. USA 2013, 110, 3681–3688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.; Honda, Y.; Liu, Q.; Olwoch, J.; Revich, B.; Sauerborn, R.; Aranda, C. Human health: Impacts, adaptation, and co-benefits. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK, 2014; pp. 709–754. [Google Scholar]
- Cerveny, R.S.; Bessemoulin, P.; Burt, C.C.; Cooper, M.A.; Cunjie, Z.; Dewan, A.; Finch, J.; Holle, R.L.; Kalkstein, L.; Kruger, A. WMO assessment of weather and climate mortality extremes: Lightning, tropical cyclones, tornadoes, and hail. Weather Clim. Soc. 2017, 9, 487–497. [Google Scholar] [CrossRef]
- Kabir, H.; Hossen, N. Impacts of flood and its possible solution in Bangladesh. Disaster Adv. 2019, 12, 48–57. [Google Scholar]
- Shultz, J.M.; Russell, J.; Espinel, Z. Epidemiology of tropical cyclones: The dynamics of disaster, disease, and development. Epidemiol. Rev. 2005, 27, 21–35. [Google Scholar] [CrossRef] [Green Version]
- Kovats, S.; Akhtar, R. Climate, climate change and human health in Asian cities. Environ. Urban. 2008, 20, 165–175. [Google Scholar] [CrossRef]
- Burkart, K.; Breitner, S.; Schneider, A.; Khan, M.M.H.; Krämer, A.; Endlicher, W. An analysis of heat effects in different subpopulations of Bangladesh. Int. J. Biometeorol. 2014, 58, 227–237. [Google Scholar] [CrossRef]
- Sultana, N. Analysis of landslide-induced fatalities and injuries in Bangladesh: 2000–2018. Cogent Soc. Sci. 2020, 6, 1737402. [Google Scholar] [CrossRef]
- Sarker, A.A.; Rashid, A.M. Landslide and flashflood in Bangladesh. In Disaster Risk Reduction Approaches in Bangladesh; Springer: Berlin/Heidelberg, Germany, 2013; pp. 165–189. [Google Scholar]
- HCTT. Flash Flood: Humanitarian Response Plan 2022; Humanitarian Coordinator Task Team (HCTT) in Collaboration with the Bangladesh Ministry of Disaster Management and Relief (MoDMR): Dhaka, Bangladesh, 2022. [Google Scholar]
- France-Presse, A. Cyclone Sitrang: 24 dead as Bangladesh seeks to restore power to millions. The Guardian, 26 October 2022. [Google Scholar]
- Nahian, M.A.; Ahmed, A.; Lázár, A.N.; Hutton, C.W.; Salehin, M.; Streatfield, P.K.; Chadwick, O.; Renaud, F. Drinking water salinity associated health crisis in coastal Bangladesh. Elem. Sci. Anthr. 2018, 6, 2. [Google Scholar] [CrossRef]
- Cissé, G.; McLeman, R.; Adams, H.; Aldunce, P.; Bowen, K.; Campbell-Lendrum, D.; Clayton, S.; Ebi, K.; Hess, J.; Huang, C. Health, Wellbeing, and the Changing Structure of Communities; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2022; pp. 1041–1170. [Google Scholar]
- Khan, A.E.; Scheelbeek, P.F.D.; Shilpi, A.B.; Chan, Q.; Mojumder, S.K.; Rahman, A.; Haines, A.; Vineis, P. Salinity in drinking water and the risk of (pre) eclampsia and gestational hypertension in coastal Bangladesh: A case-control study. PLoS ONE 2014, 9, e108715. [Google Scholar] [CrossRef] [Green Version]
- Clarke, D.; Williams, S.; Jahiruddin, M.; Parks, K.; Salehin, M. Projections of on-farm salinity in coastal Bangladesh. Environ. Sci. Process. Impacts 2015, 17, 1127–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payo, A.; Lázár, A.N.; Clarke, D.; Nicholls, R.J.; Bricheno, L.; Mashfiqus, S.; Haque, A. Modeling daily soil salinity dynamics in response to agricultural and environmental changes in coastal Bangladesh. Earth’s Future 2017, 5, 495–514. [Google Scholar] [CrossRef]
- Rabbani, G.; Rahman, A.; Mainuddin, K. Salinity-induced loss and damage to farming households in coastal Bangladesh. Int. J. Glob. Warm. 2013, 5, 400–415. [Google Scholar] [CrossRef]
- DoE. Air Quality Status and Trends: 2013–2015; Department of Environment: Dhaka, Bangladesh, 2016. Available online: http://www.doe.gov.bd/ (accessed on 25 February 2022).
- WHO. Ambient Air Pollution: A Global Assessment of Exposure and Burden of Disease; 9241511354; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Orru, H.; Ebi, K.; Forsberg, B. The interplay of climate change and air pollution on health. Curr. Environ. Health Rep. 2017, 4, 504–513. [Google Scholar] [CrossRef]
- Fuller, R.; Landrigan, P.J.; Balakrishnan, K.; Bathan, G.; Bose-O’Reilly, S.; Brauer, M.; Caravanos, J.; Chiles, T.; Cohen, A.; Corra, L. Pollution and health: A progress update. Lancet Planet. Health 2022, 6, e535–e547. [Google Scholar] [CrossRef]
- Nahian, M.A.; Ahmad, T.; Jahan, I.; Chakraborty, N.; Nahar, Q.; Streatfield, P.K. Air Pollution and Pregnancy Outcomes in Dhaka, Bangladesh. J. Clim. Change Health, 2022, in press. [CrossRef]
- UNEP. Air Pollution and Climate Change: Two Sides of the Same Coin. Available online: https://www.unep.org/news-and-stories/story/air-pollution-and-climate-change-two-sides-same-coin (accessed on 7 September 2022).
- Dadvand, P.; Ostro, B.; Figueras, F.; Foraster, M.; Basagaña, X.; Valentín, A.; Martinez, D.; Beelen, R.; Cirach, M.; Hoek, G. Residential proximity to major roads and term low birth weight: The roles of air pollution, heat, noise, and road-adjacent trees. Epidemiology 2014, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Ayers, J.M.; Huq, S.; Faisal, A.M.; Hussain, S.T. Mainstreaming climate change adaptation into development: A case study of Bangladesh. Wiley Interdiscip. Rev. Clim. Chang. 2014, 5, 37–51. [Google Scholar] [CrossRef]
- Neumayer, E.; Plümper, T. The gendered nature of natural disasters: The impact of catastrophic events on the gender gap in life expectancy, 1981–2002. Ann. Assoc. Am. Geogr. 2007, 97, 551–566. [Google Scholar] [CrossRef] [Green Version]
- Neelormi, S.; Adri, N.; Ahmed, A.U. Gender Perspectives of Increased Socio-Economic Risks of Waterlogging in Bangladesh Due to Climate Change; International Ocean Institute: St. Petersburg, FL, USA, 2008. [Google Scholar]
- BBC Bangla. Why Is there an Abnormal Rate of Hysterectomy in Coastal Areas? (In Bangla: উপকূলীয় অঞ্চলে নারীদের অস্বাভাবিক হারে জরায়ু অপসারণের ঘটনা কেন ঘটছে? 2022. Available online: https://www.youtube.com/watch?v=BhUKQslgqf8 (accessed on 10 August 2022).
- Papri, J. For women on Bangladesh’s coast, rising seas pose a reproductive health dilemma. Mongabay, 1 October 2022. [Google Scholar]
- Reiner, R.C.; Stoddard, S.T.; Forshey, B.M.; King, A.A.; Ellis, A.M.; Lloyd, A.L.; Long, K.C.; Rocha, C.; Vilcarromero, S.; Astete, H. Time-varying, serotype-specific force of infection of dengue virus. Proc. Natl. Acad. Sci. USA 2014, 111, E2694–E2702. [Google Scholar] [CrossRef] [Green Version]
- Githeko, A.K.; Lindsay, S.W.; Confalonieri, U.E.; Patz, J.A. Climate change and vector-borne diseases: A regional analysis. Bull. World Health Organ. 2000, 78, 1136–1147. [Google Scholar] [PubMed]
- Wu, X.; Lu, Y.; Zhou, S.; Chen, L.; Xu, B. Impact of climate change on human infectious diseases: Empirical evidence and human adaptation. Environ. Int. 2016, 86, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.A.; Galagan, S.R.; Prue, C.S.; Khyang, J.; Ahmed, S.; Ram, M.; Alam, M.S.; Haq, M.Z.; Akter, J.; Glass, G. Asymptomatic Plasmodium falciparum malaria in pregnant women in the Chittagong Hill Districts of Bangladesh. PLoS ONE 2014, 9, e98442. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.B.; Khan, J.R.; Parvez, M. Residential district multi-hazard risk is associated with childhood undernutrition: Evidence from Bangladesh. Int. J. Environ. Health Res. 2022, 32, 2005–2016. [Google Scholar] [CrossRef] [PubMed]
- Son, J.-Y.; Lee, J.-T.; Bell, M.L. Is ambient temperature associated with risk of infant mortality? A multi-city study in Korea. Environ. Res. 2017, 158, 748–752. [Google Scholar] [CrossRef]
- Babalola, O.; Razzaque, A.; Bishai, D. Temperature extremes and infant mortality in Bangladesh: Hotter months, lower mortality. PLoS ONE 2018, 13, e0189252. [Google Scholar] [CrossRef] [Green Version]
- Hashizume, M.; Wagatsuma, Y.; Hayashi, T.; Saha, S.K.; Streatfield, K.; Yunus, M. The effect of temperature on mortality in rural Bangladesh—A population-based time-series study. Int. J. Epidemiol. 2009, 38, 1689–1697. [Google Scholar] [CrossRef] [Green Version]
- Khalaj, B.; Lloyd, G.; Sheppeard, V.; Dear, K. The health impacts of heat waves in five regions of New South Wales, Australia: A case-only analysis. Int. Arch. Occup. Environ. Health 2010, 83, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Huang, C.; Hu, W.; Turner, L.R.; Su, H.; Tong, S. Extreme temperatures and emergency department admissions for childhood asthma in Brisbane, Australia. Occup. Environ. Med. 2013, 70, 730–735. [Google Scholar] [CrossRef]
- Xu, Z.; Sheffield, P.E.; Su, H.; Wang, X.; Bi, Y.; Tong, S. The impact of heat waves on children’s health: A systematic review. Int. J. Biometeorol. 2014, 58, 239–247. [Google Scholar] [CrossRef]
- Mrema, S.; Shamte, A.; Selemani, M.; Masanja, H. The influence of weather on mortality in rural Tanzania: A time-series analysis 1999–2010. Glob. Health Action 2012, 5, 19068. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Mashreky, S.R.; Chowdhury, S.; Giashuddin, M.; Uhaa, I.; Shafinaz, S.; Hossain, M.; Linnan, M.; Rahman, F. Analysis of the childhood fatal drowning situation in Bangladesh: Exploring prevention measures for low-income countries. Inj. Prev. 2009, 15, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.Z.K.; Rahman, A.; Rahman, M.A.; Renzaho, A.M. Impact of droughts on child mortality: A case study in Southern African countries. Nat. Hazards 2021, 108, 2211–2224. [Google Scholar] [CrossRef]
- Cooper, M.; Brown, M.E.; Azzarri, C.; Meinzen-Dick, R. Hunger, nutrition, and precipitation: Evidence from Ghana and Bangladesh. Popul. Environ. 2019, 41, 151–208. [Google Scholar] [CrossRef] [Green Version]
- Asmall, T.; Abrams, A.; Röösli, M.; Cissé, G.; Carden, K.; Dalvie, M.A. The adverse health effects associated with drought in Africa. Sci. Total Environ. 2021, 793, 148500. [Google Scholar] [CrossRef]
- Kabir, A.; Islam, M.Z.; Ahmed, A.; Rahman, M.S.; Rahman, S. Health and Drinking Water Supply Vulnerabilities to Climate Variability in Coastal and Drought-Prone Areas of Bangladesh. Int. J. Clim. Chang. Impacts Responses 2019, 11, 41–56. [Google Scholar] [CrossRef]
- Kamruzzaman, A.; Jahan, M.S.; Rahman, M.R.; Khatun, M.M. Impact of climate change on the outbreak of infectious diseases among children in Bangladesh. Am. J. Public Health Res. 2015, 3, 1–7. [Google Scholar] [CrossRef]
- Wang, B.; Wang, S.; Li, L.; Xu, S.; Li, C.; Li, S.; Wang, J.; He, H.; Niu, J.; Zhang, K. The association between drought and outpatient visits for respiratory diseases in four northwest cities of China. Clim. Chang. 2021, 167, 2. [Google Scholar] [CrossRef]
- Dean, J.G.; Stain, H.J. Mental health impact for adolescents living with prolonged drought. Aust. J. Rural Health 2010, 18, 32–37. [Google Scholar] [CrossRef]
- Landrigan, P.J. Children as a vulnerable population. Int. J. Occup. Med. Environ. Health 2004, 17, 175–178. [Google Scholar] [CrossRef]
- Sarkar, P.K.; Sarker, N.K.; Tayab, M.A. Hand, foot and mouth disease (hfmd): An update. Bangladesh J. Child Health 2016, 40, 115–119. [Google Scholar] [CrossRef]
- Mallett, L.H.; Etzel, R.A. Flooding: What is the impact on pregnancy and child health? Disasters 2018, 42, 432–458. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Hashizume, M.; Kolivras, K.N.; Overgaard, H.J.; Das, B.; Yamamoto, T. Reduced death rates from cyclones in Bangladesh: What more needs to be done? Bull. World Health Organ. 2012, 90, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkett, M. In search of refuge: Pacific Islands, climate-induced migration, and the legal frontier. Asia Pac. Issues 2011, 98, 1–8. [Google Scholar]
- Niazi, T. Ground Zero of Climate Change: Coastal and Island Nations of the Asia-Pacific. Asia-Pac. J. | Jpn. Focus Vol. 2015, 13, 1–7. [Google Scholar]
- Wali, N.; Chen, W.; Rawal, L.B.; Amanullah, A.; Renzaho, A.M. Integrating human rights approaches into public health practices and policies to address health needs amongst Rohingya refugees in Bangladesh: A systematic review and meta-ethnographic analysis. Arch. Public Health 2018, 76, 59. [Google Scholar] [CrossRef] [Green Version]
- Mantoo, S.A. Bihari refugees stranded in bangladesh since 1971. J. South Asian Stud. 2013, 1, 123–129. [Google Scholar]
- Rigaud, K.K.; De Sherbinin, A.; Jones, B.; Bergmann, J.; Clement, V.; Ober, K.; Schewe, J.; Adamo, S.; McCusker, B.; Heuser, S. Groundswell: Preparing for Internal Climate Migration; World Bank: Washinton DC, USA, 2018. [Google Scholar]
- Zall Kusek, J.; Rist, R.C. Ten Steps to a Results-Based Monitoring and Evaluation System: A Handbook for Development Practitioners; World Bank: Washington, DC, USA, 2004. [Google Scholar]
- Navi, M.; Hansen, A.; Nitschke, M.; Hanson-Easey, S.; Pisaniello, D. Developing health-related indicators of climate change: Australian stakeholder perspectives. Int. J. Environ. Res. Public Health 2017, 14, 552. [Google Scholar] [CrossRef]
- DGHS. Bangladesh Health-National Adaptation Plan (HNAP). 2018. Available online: https://www.who.int/publications/m/item/hnap-bangladesh (accessed on 10 October 2020).
- WHO. Operational Framework for Building Climate Resilient Health Systems; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]


| First Author; Year | Title | Thematic Topics/Areas | Reference No. |
|---|---|---|---|
| Chowdhury et al., 2018 | The association between temperature, rainfall and humidity with common climate-sensitive infectious diseases in Bangladesh. | Impact of climate change on population health—Evidence base | [24] |
| Das et al., 2019 | District level estimates and mapping of prevalence of diarrhoea among under-five children in Bangladesh by combining survey and census data. | [25] | |
| Dewan et al., 2006 | Environmental change and kala azar with particular reference to Bangladesh. | [26] | |
| Elahi, 2016 | Climate Change and Health Impacts in Bangladesh. | [27] | |
| Haque et al., 2016 | Health coping strategies of the people vulnerable to climate change in a resource-poor rural setting in Bangladesh. | [28] | |
| Haque et al., 2014 | Use of traditional medicines to cope with climate-sensitive diseases in a resource poor setting in Bangladesh. | [29] | |
| Haque et al., 2019 | Parents’ healthcare-seeking behavior for their children among the climate-related displaced population of rural Bangladesh | [30] | |
| Huda et al., 2014 | Visceral leishmaniasis-associated mortality in Bangladesh: a retrospective cross-sectional study. | [31] | |
| Kabir et al., 2016 | Knowledge and perception about climate change and human health: findings from a baseline survey among vulnerable communities in Bangladesh. | [32] | |
| Khan, et al., 2014 | Is area affected by flood or stagnant water independently associated with poorer health outcomes in urban slums of Dhaka and adjacent rural areas? | [33] | |
| Koehlmoos et al., 2011 | Global health: chronic diseases and other emergent issues in global health. | [34] | |
| Mamun et al., 2021 | The COVID-19 pandemic and serious psychological consequences in Bangladesh: A population-based nationwide study. | [35] | |
| Nahar et al., 2014 | Increasing the provision of mental healthcare for vulnerable, disaster-affected people in Bangladesh. | [36] | |
| Adams et al., 2013 | Innovation for universal health coverage in Bangladesh: a call to action. | Health policy-oriented articles and book chapters | [37] |
| Fahim et al., 2019 | Financing healthcare in Bangladesh: Policy responses and challenges towards achieving universal health coverage. | [38] | |
| Murshid et al., 2020 | Hits and misses of Bangladesh national health policy 2011. | [39] | |
| Huq et al., 2019 | Confronting climate change in Bangladesh: policy strategies for adaptation and resilience. | [40] | |
| Shafique et al., 2018 | Right to health and social justice in Bangladesh: Ethical dilemmas and obligations of state and non-state actors to ensure health for urban poor. | [41] | |
| Yasobant et al., 2020 | Toward the Development of an Integrated Climate-Sensitive Disease Surveillance in Southeast Asian Countries: A Situational Analysis. | [42] | |
| Biswas et al., 2018 | Assessing the readiness of health facilities for diabetes and cardiovascular services in Bangladesh: a cross-sectional survey. | Health system readiness/preparedness-related articles | [43] |
| Rahaman et al., 2019 | Pathways of Climate-Resilient Health Systems in Bangladesh. | [44] | |
| Rahman et al., 2021 | COVID-19 pandemic, dengue epidemic, and climate change vulnerability in Bangladesh: Scenario assessment for strategic management and policy implications. | [45] | |
| Streatfield et al., 2008 | Population challenges for Bangladesh in the coming decades. | [46] | |
| Helldén et al., 2021 | Climate change and child health: a scoping review and an expanded conceptual framework. | Scoping/critical review | [47] |
| Hunter et al., 2021 | Scales and sensitivities in climate vulnerability, displacement, and health. | [48] | |
| Rahman et al., 2019 | Health consequences of climate change in Bangladesh: An overview of the evidence, knowledge gaps and challenges. | [17] | |
| Hayward et al., 2021 | “Seeing with Empty Eyes”: a systems approach to understand climate change and mental health in Bangladesh. | Systematic review | [49] |
| Schwerdtle et al., 2020 | Health and migration in the context of a changing climate: A systematic literature assessment. | [50] |
| Question | Score | Combined Score | Level of CC Integration | Number of Ops | Name of Ops * |
|---|---|---|---|---|---|
| Is climate change mentioned in the OP? | 1 | 1 | Mentioned | 5 | PME, SDAM, PSSM-HS, MNCAH, FP-FSD |
| If mentioned, is there any specific project and programs on CC included? | 1 | 2 | Tried integration | 1 | NNS |
| Is there any budget allocated for the project or porgram? | 1 | 3 | Somehow integrated | - | |
| Is there any indicator to monitor progress? | 1 | 4 | Almost integrated | 2 | HIS and E-Health, CBHC |
| Is the project or program being integrated with other project or porgrams in the respective OP? | 1 | 5 | Fully integrated | 7 | SWPMM, PMR, TRD, CDC, TBL, and ASP, NCDC, LHEP |
| OPs without any mention of climate change | X | 14 | |||
| Total OPs | 29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nahian, M.A. Public Health Impact and Health System Preparedness within a Changing Climate in Bangladesh: A Scoping Review. Challenges 2023, 14, 4. https://doi.org/10.3390/challe14010004
Nahian MA. Public Health Impact and Health System Preparedness within a Changing Climate in Bangladesh: A Scoping Review. Challenges. 2023; 14(1):4. https://doi.org/10.3390/challe14010004
Chicago/Turabian StyleNahian, Mahin Al. 2023. "Public Health Impact and Health System Preparedness within a Changing Climate in Bangladesh: A Scoping Review" Challenges 14, no. 1: 4. https://doi.org/10.3390/challe14010004
APA StyleNahian, M. A. (2023). Public Health Impact and Health System Preparedness within a Changing Climate in Bangladesh: A Scoping Review. Challenges, 14(1), 4. https://doi.org/10.3390/challe14010004