
A Robust Hybrid Deep Convolutional Neural Network for COVID-19 Disease Identification from Chest X-ray Images

 , ,
, ,  and
and 
Abstract
:1. Introduction
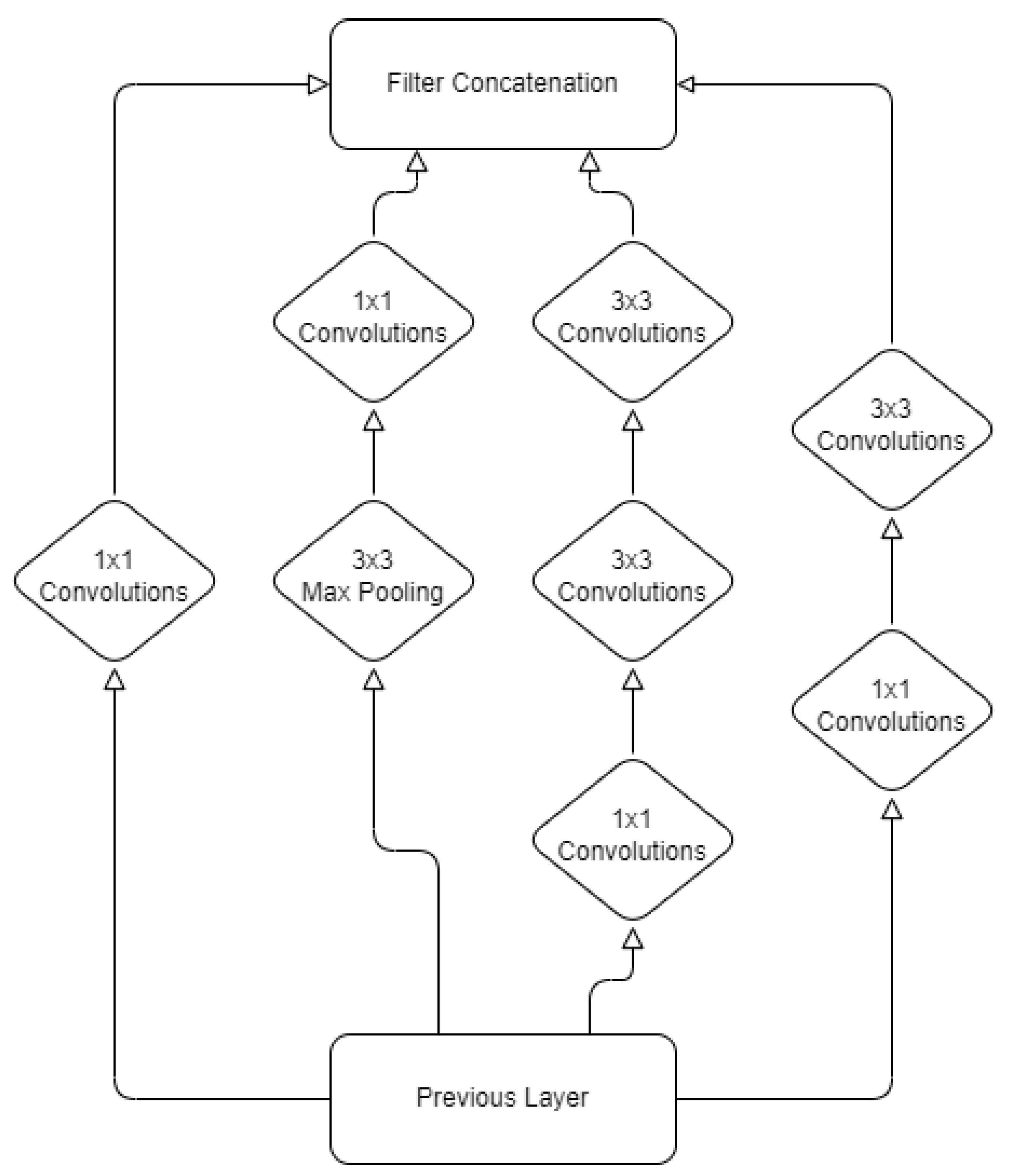
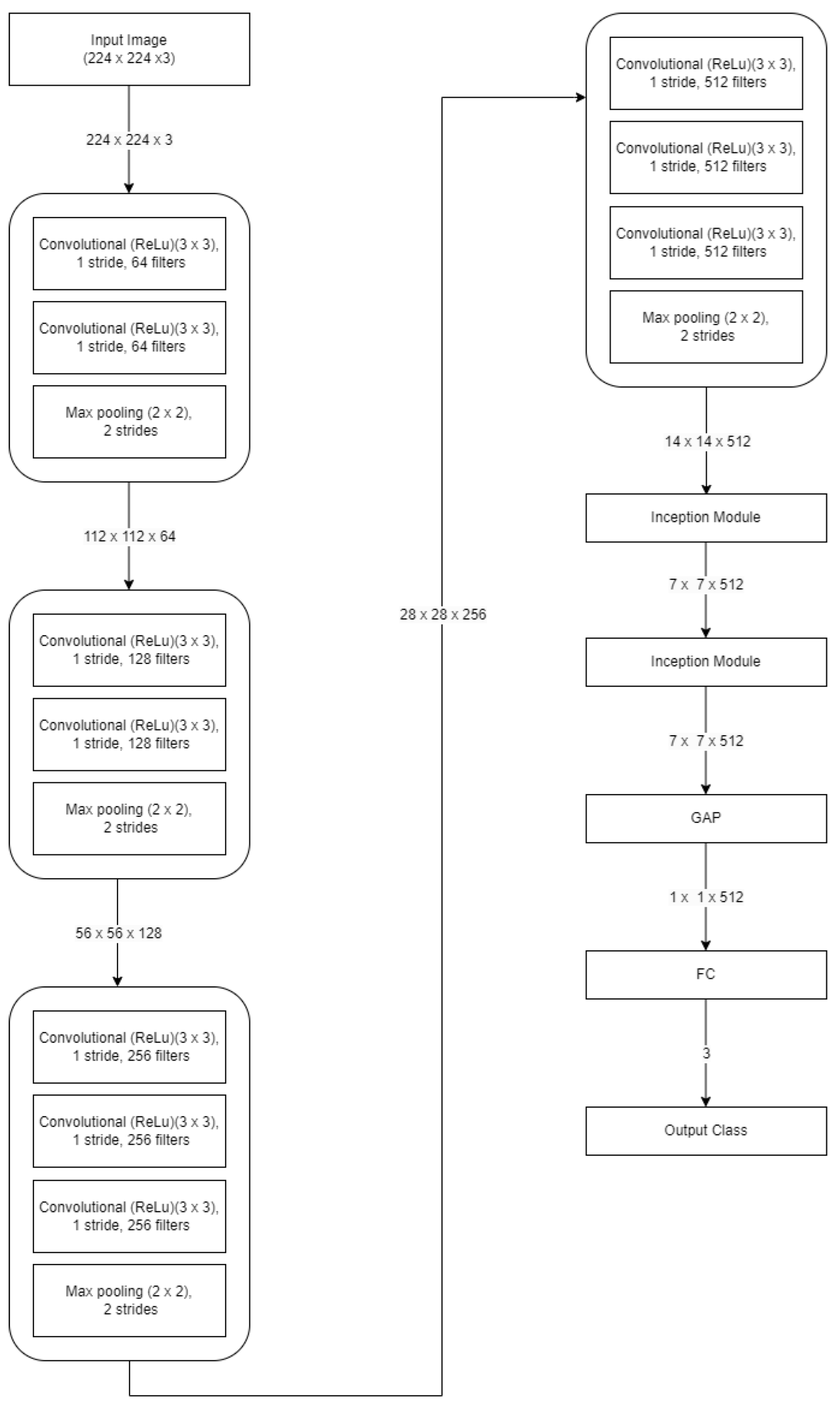
- The identification of pneumonia is performed using a hybrid DCNN mechanism. The modified VGG19 model includes two inception blocks to take advantage of simultaneous feature extraction capabilities. The hybrid DCNN is equipped with powerful feature extraction capabilities.
- We conducted exhaustive high-level simulations to assess the effectiveness of the presented hybrid DCNN. The proposed hybrid DCNN mechanism findings were compared to those obtained from the most current and advanced networks.
2. Related Work
3. Materials and Methods
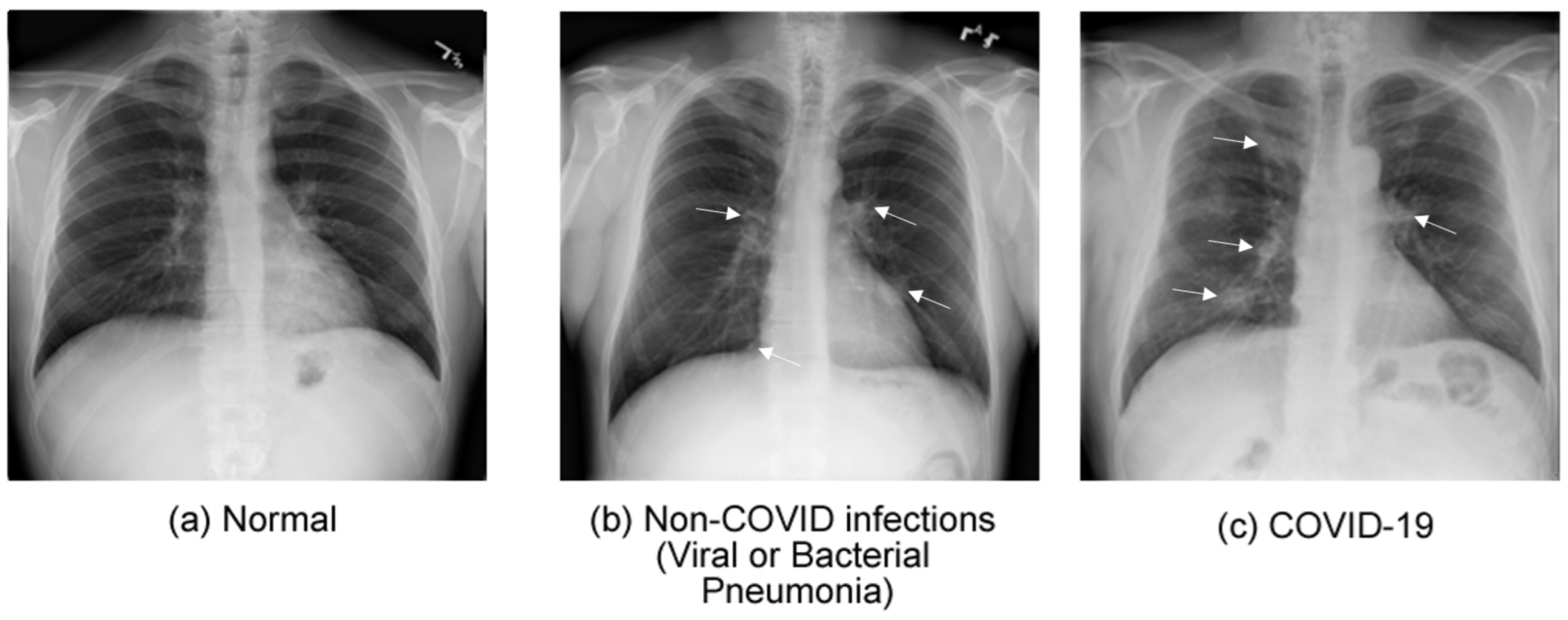
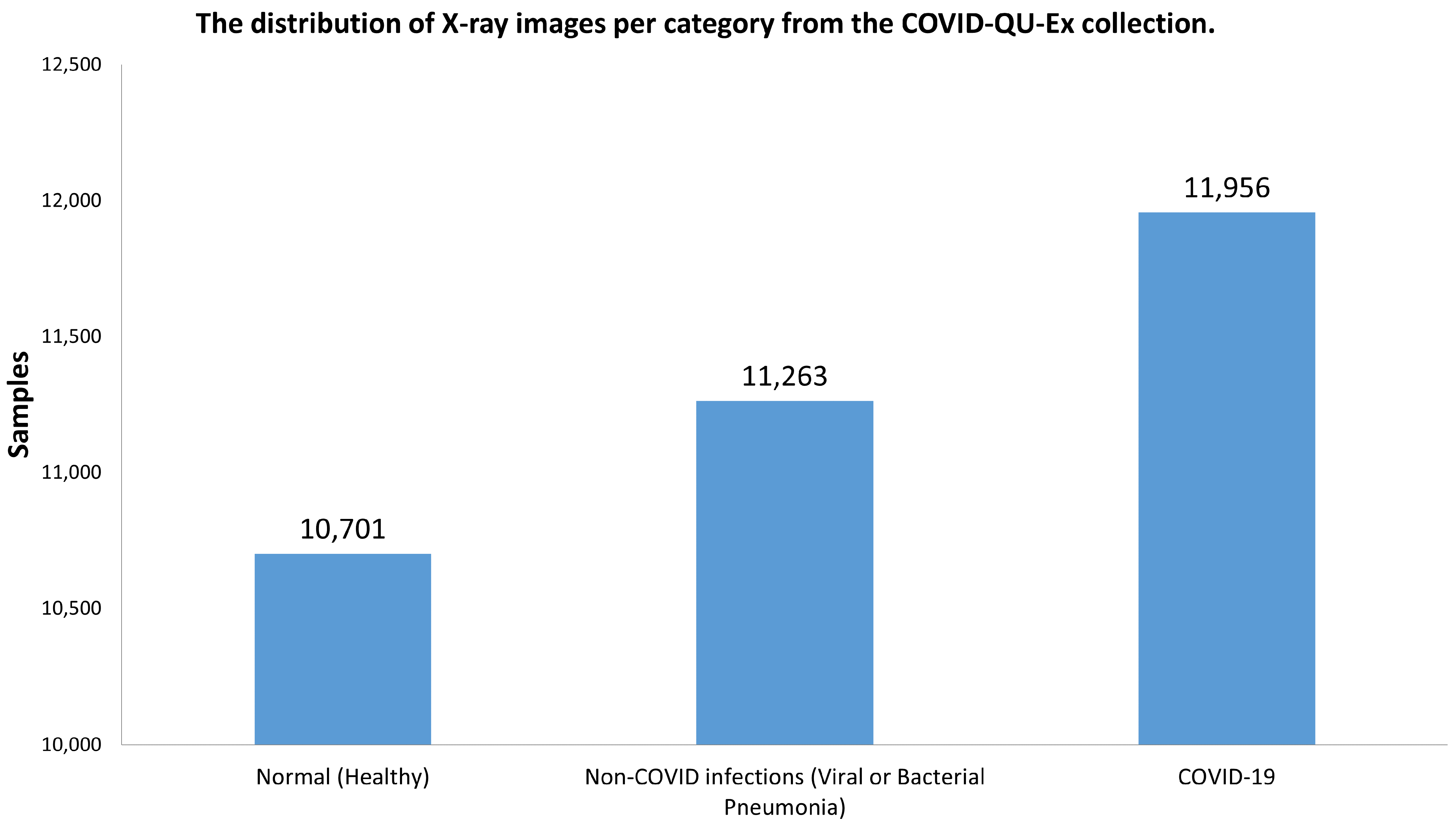
3.1. Dataset Collection
3.2. Split Collection
3.3. Hybrid DCNN for Diagnosing Pneumonia and COVID-19 Disease
3.4. Implementation Description
3.5. Performance Measures
4. Experimental Results
5. Conclusions and Future Work
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ARDS | Acute Respiratory Distress Syndrome |
| CAD | Computer-Aided Diagnostic |
| COPD | Chronic Obstructive Pulmonary Disease |
| CT | Computed Tomography |
| CXR | Chest X-Ray |
| DCNN | Deep Convolutional Neural Network |
| DL | Deep Learning |
| GPU | Graphics processing unit |
| ML | Machine Learning |
| MRI | Magnetic Resonance Imaging |
| ReLU | Rectified linear unit |
| SONs | Service-Oriented Networks |
| VGG | Visual geometry group |
References
- Lerner, D.K.; Garvey, K.L.; Arrighi-Allisan, A.E.; Filimonov, A.; Filip, P.; Shah, J.; Tweel, B.; Del Signore, A.; Schaberg, M.; Colley, P.; et al. Clinical features of parosmia associated with COVID-19 infection. Laryngoscope 2022, 132, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Mollarasouli, F.; Zare-Shehneh, N.; Ghaedi, M. A review on corona virus disease 2019 (COVID-19): Current progress, clinical features and bioanalytical diagnostic methods. Microchim. Acta 2022, 189, 103. [Google Scholar] [CrossRef]
- Watanabe, A.; So, M.; Mitaka, H.; Ishisaka, Y.; Takagi, H.; Inokuchi, R.; Iwagami, M.; Kuno, T. Clinical features and mortality of COVID-19-associated mucormycosis: A systematic review and meta-analysis. Mycopathologia 2022, 187, 271–289. [Google Scholar] [CrossRef]
- Irmici, G.; Cè, M.; Caloro, E.; Khenkina, N.; Della Pepa, G.; Ascenti, V.; Martinenghi, C.; Papa, S.; Oliva, G.; Cellina, M. Chest X-ray in Emergency Radiology: What Artificial Intelligence Applications Are Available? Diagnostics 2023, 13, 216. [Google Scholar] [CrossRef] [PubMed]
- Taleghani, N.; Taghipour, F. Diagnosis of COVID-19 for controlling the pandemic: A review of the state-of-the-art. Biosens. Bioelectron. 2021, 174, 112830. [Google Scholar] [CrossRef]
- Ravi, V.; Narasimhan, H.; Pham, T.D. A cost-sensitive deep learning-based meta-classifier for pediatric pneumonia classification using chest X-rays. Expert Syst. 2022, 39, e12966. [Google Scholar] [CrossRef]
- Rajaraman, S.; Guo, P.; Xue, Z.; Antani, S.K. A Deep Modality-Specific Ensemble for Improving Pneumonia Detection in Chest X-rays. Diagnostics 2022, 12, 1442. [Google Scholar] [CrossRef]
- Hasan, M.M.; Islam, M.U.; Sadeq, M.J.; Fung, W.K.; Uddin, J. Review on the Evaluation and Development of Artificial Intelligence for COVID-19 Containment. Sensors 2023, 23, 527. [Google Scholar] [CrossRef]
- Soomro, T.A.; Zheng, L.; Afifi, A.J.; Ali, A.; Yin, M.; Gao, J. Artificial intelligence (AI) for medical imaging to combat coronavirus disease (COVID-19): A detailed review with direction for future research. Artif. Intell. Rev. 2022, 55, 1409–1439. [Google Scholar] [CrossRef]
- Pfaff, E.R.; Girvin, A.T.; Bennett, T.D.; Bhatia, A.; Brooks, I.M.; Deer, R.R.; Dekermanjian, J.P.; Jolley, S.E.; Kahn, M.G.; Kostka, K.; et al. Identifying who has long COVID in the USA: A machine learning approach using N3C data. Lancet Digit. Health 2022, 4, e532–e541. [Google Scholar] [CrossRef]
- Ahsan, M.M.; Luna, S.A.; Siddique, Z. Machine-learning-based disease diagnosis: A comprehensive review. Healthcare 2022, 10, 541. [Google Scholar] [CrossRef] [PubMed]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar] [CrossRef]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Conti, V.; Militello, C.; Rundo, L.; Vitabile, S. A novel bio-inspired approach for high-performance management in service-oriented networks. IEEE Trans. Emerg. Top. Comput. 2020, 9, 1709–1722. [Google Scholar] [CrossRef]
- Han, X.; Hu, Z.; Wang, S.; Zhang, Y. A Survey on Deep Learning in COVID-19 Diagnosis. J. Imaging 2022, 9, 1. [Google Scholar] [CrossRef]
- Ayadi, M.; Ksibi, A.; Al-Rasheed, A.; Soufiene, B.O. COVID-AleXception: A Deep Learning Model Based on a Deep Feature Concatenation Approach for the Detection of COVID-19 from Chest X-ray Images. Healthcare 2022, 10, 2072. [Google Scholar] [CrossRef] [PubMed]
- Hafeez, U.; Umer, M.; Hameed, A.; Mustafa, H.; Sohaib, A.; Nappi, M.; Madni, H.A. A CNN based coronavirus disease prediction system for chest X-rays. J. Ambient. Intell. Humaniz. Comput. 2022, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.L.; Liao, Y.C. A lightweight CNN-based network on COVID-19 detection using X-ray and CT images. Comput. Biol. Med. 2022, 146, 105604. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.I.; Shah, J.L.; Bhat, M.M. CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest X-ray images. Comput. Methods Programs Biomed. 2020, 196, 105581. [Google Scholar] [CrossRef] [PubMed]
- Ghose, P.; Uddin, M.A.; Acharjee, U.K.; Sharmin, S. Deep viewing for the identification of covid-19 infection status from chest X-ray image using cnn based architecture. Intell. Syst. Appl. 2022, 16, 200130. [Google Scholar] [CrossRef]
- Ibrokhimov, B.; Kang, J.Y. Deep Learning Model for COVID-19-Infected Pneumonia Diagnosis Using Chest Radiography Images. BioMedInformatics 2022, 2, 654–670. [Google Scholar] [CrossRef]
- Khan, I.U.; Aslam, N. A deep-learning-based framework for automated diagnosis of COVID-19 using X-ray images. Information 2020, 11, 419. [Google Scholar] [CrossRef]
- Kaya, Y.; Gürsoy, E. A MobileNet-based CNN model with a novel fine-tuning mechanism for COVID-19 infection detection. Soft Comput. 2023, 27, 5521–5535. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.R.; Nayak, D.R.; Sinha, U.; Arora, V.; Pachori, R.B. An Efficient Deep Learning Method for Detection of COVID-19 Infection Using Chest X-ray Images. Diagnostics 2023, 13, 131. [Google Scholar] [CrossRef] [PubMed]
- Sanida, T.; Sideris, A.; Tsiktsiris, D.; Dasygenis, M. Lightweight neural network for COVID-19 detection from chest X-ray images implemented on an embedded system. Technologies 2022, 10, 37. [Google Scholar] [CrossRef]
- Sanida, T.; Sideris, A.; Chatzisavvas, A.; Dossis, M.; Dasygenis, M. Radiography Images with Transfer Learning on Embedded System. In Proceedings of the 2022 7th South-East Europe Design Automation, Computer Engineering, Computer Networks and Social Media Conference (SEEDA-CECNSM), Ioannina, Greece, 23–25 September 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 1–4. [Google Scholar] [CrossRef]
- Tahir, A.M.; Chowdhury, M.E.; Khandakar, A.; Rahman, T.; Qiblawey, Y.; Khurshid, U.; Kiranyaz, S.; Ibtehaz, N.; Rahman, M.S.; Al-Maadeed, S.; et al. COVID-19 infection localization and severity grading from chest X-ray images. Comput. Biol. Med. 2021, 139, 105002. [Google Scholar] [CrossRef]
- Yasin, R.; Gouda, W. Chest X-ray findings monitoring COVID-19 disease course and severity. Egypt. J. Radiol. Nucl. Med. 2020, 51, 193. [Google Scholar] [CrossRef]
- Rousan, L.A.; Elobeid, E.; Karrar, M.; Khader, Y. Chest X-ray findings and temporal lung changes in patients with COVID-19 pneumonia. BMC Pulm. Med. 2020, 20, 245. [Google Scholar] [CrossRef]
- Sanida, M.V.; Sanida, T.; Sideris, A.; Dasygenis, M. An Efficient Hybrid CNN Classification Model for Tomato Crop Disease. Technologies 2023, 11, 10. [Google Scholar] [CrossRef]
- Mohanty, S.P.; Hughes, D.P.; Salathé, M. Using deep learning for image-based plant disease detection. Front. Plant Sci. 2016, 7, 1419. [Google Scholar] [CrossRef]
- Sanida, T.; Tsiktsiris, D.; Sideris, A.; Dasygenis, M. A heterogeneous implementation for plant disease identification using deep learning. Multimed. Tools Appl. 2022, 81, 15041–15059. [Google Scholar] [CrossRef]
- Tharwat, A. Classification assessment methods. Appl. Comput. Inform. 2020, 17, 168–192. [Google Scholar] [CrossRef]
- Delgado, R.; Tibau, X.A. Why Cohen’s Kappa should be avoided as performance measure in classification. PLoS ONE 2019, 14, e0222916. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 248–255. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Best Method | Accuracy (%) |
|---|---|---|
| [17] | COVID-AleXception | 98.68 |
| [18] | Custom CNN | 89.855 |
| [19] | Lightweight CNN | 98.33 |
| [20] | CoroNet | 89.60 |
| [21] | Custom CNN | 98.50 |
| [22] | VGG19 | 96.60 |
| [23] | VGG16 | 99.33 |
| [24] | MobileNetV2 | 97.61 |
| [25] | LW-CORONet | 98.67 |
| [26] | MobileNetV2 | 95.80 |
| Category | Number of Images | Training Images | Validation Images | Test Images |
|---|---|---|---|---|
| Normal (Healthy) | 10,701 | 6849 | 1712 | 2140 |
| Non-COVID infections (Viral or Bacterial Pneumonia) | 11,263 | 7208 | 1802 | 2253 |
| COVID-19 | 11,956 | 7658 | 1903 | 2395 |
| Total | 33,920 | 21,715 | 5417 | 6788 |
| Name of Parameter | Value for Training |
|---|---|
| Optimizer | Adam |
| Number of epochs | 30 |
| Learning rate | 0.0001 |
| Mini batch size | 32 |
| Loss function | Cross-entropy |
| Network | Accuracy (%) | Precision (%) | Recall (%) | F1-Score (%) | AUC (%) | Kappa-Score (%) |
|---|---|---|---|---|---|---|
| Hybrid DCNN | 99.25 (0.0254) | 99.23 (0.0270) | 99.25 (0.0295) | 99.24 (0.0307) | 99.43 (0.0354) | 99.10 (0.0386) |
| VGG19 with one inception module | 98.59 (0.0427) | 98.55 (0.0454) | 98.59 (0.0458) | 98.56 (0.0507) | 98.94 (0.0492) | 98.45 (0.0471) |
| VGG19 | 98.17 (0.0474) | 98.13 (0.0432) | 98.18 (0.0481) | 98.15 (0.0507) | 98.63 (0.0531) | 97.84 (0.0516) |
| VGG16 | 97.33 (0.0706) | 97.31 (0.0732) | 97.28 (0.0713) | 97.30 (0.0634) | 97.97 (0.0642) | 96.61 (0.0770) |
| ResNet50 | 96.45 (0.0552) | 96.41 (0.0507) | 96.41 (0.0587) | 96.40 (0.0602) | 97.32 (0.0580) | 95.17 (0.0524) |
| Network | Categories | Precision | Recall | F1-Score |
|---|---|---|---|---|
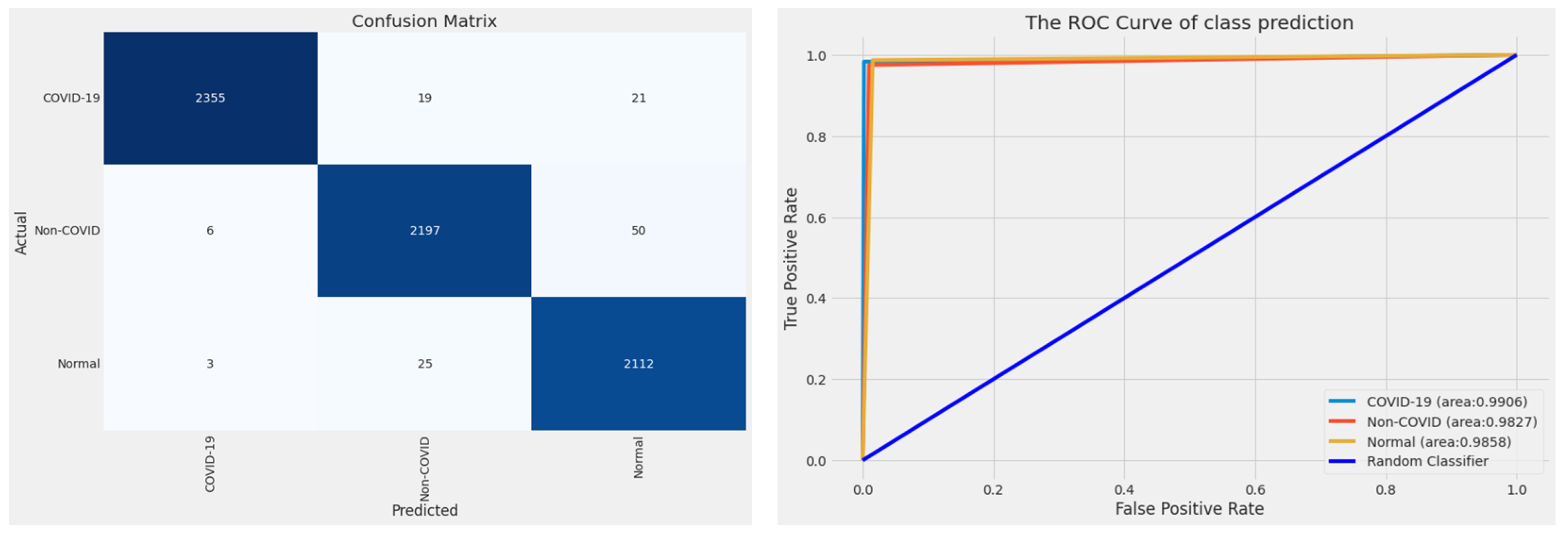
| Hybrid DCNN | COVID-19 | 0.9983 | 0.9933 | 0.9958 |
| Non-COVID | 0.9902 | 0.9916 | 0.9909 | |
| Normal | 0.9884 | 0.9925 | 0.9904 | |
| VGG19 with one inception module | COVID-19 | 0.9972 | 0.9901 | 0.9948 |
| Non-COVID | 0.9901 | 0.9734 | 0.9819 | |
| Normal | 0.9668 | 0.9919 | 0.9802 | |
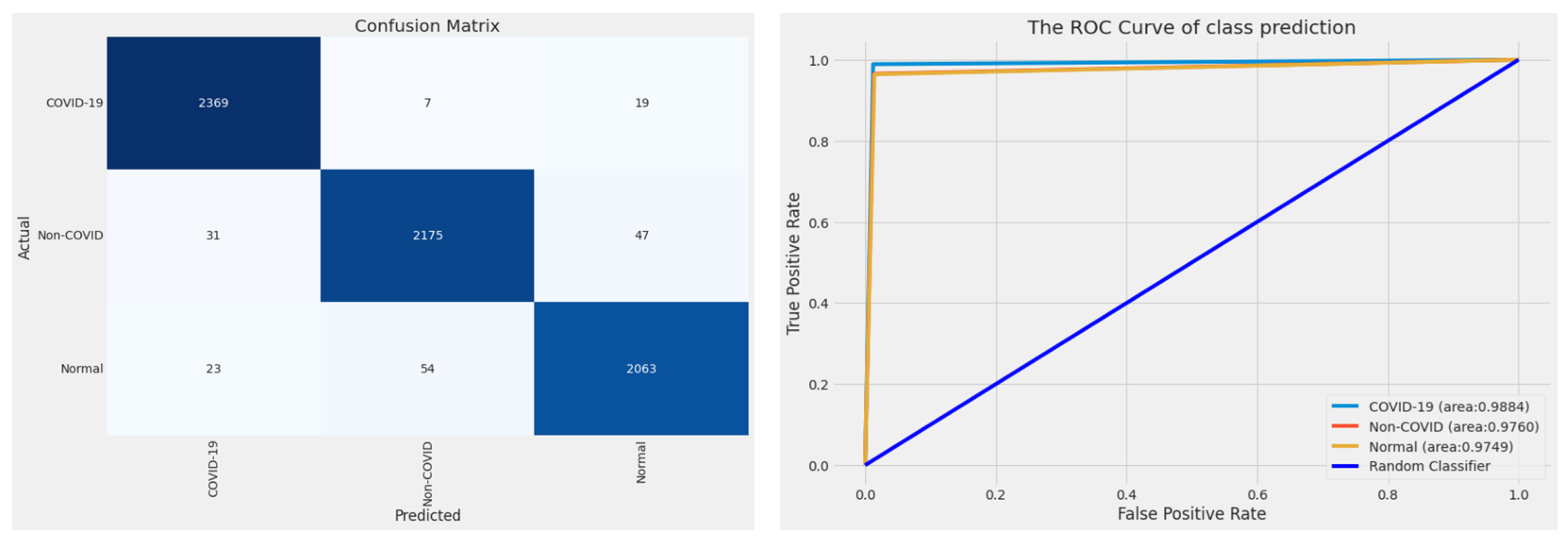
| VGG19 | COVID-19 | 0.9962 | 0.9833 | 0.9897 |
| Non-COVID | 0.9804 | 0.9751 | 0.9777 | |
| Normal | 0.9675 | 0.9869 | 0.9771 | |
| VGG16 | COVID-19 | 0.9777 | 0.9891 | 0.9834 |
| Non-COVID | 0.9727 | 0.9654 | 0.9690 | |
| Normal | 0.9690 | 0.9640 | 0.9665 | |
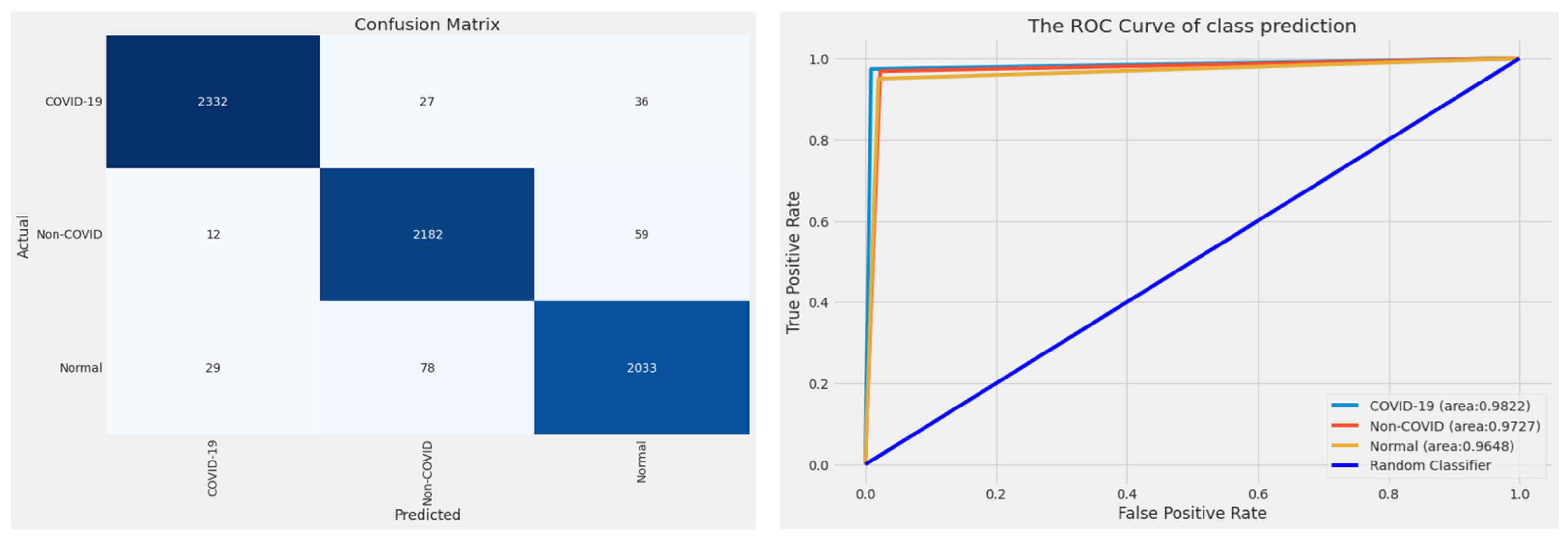
| ResNet50 | COVID-19 | 0.9827 | 0.9737 | 0.9782 |
| Non-COVID | 0.9541 | 0.9685 | 0.9612 | |
| Normal | 0.9554 | 0.9500 | 0.9527 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanida, T.; Tabakis, I.-M.; Sanida, M.V.; Sideris, A.; Dasygenis, M. A Robust Hybrid Deep Convolutional Neural Network for COVID-19 Disease Identification from Chest X-ray Images. Information 2023, 14, 310. https://doi.org/10.3390/info14060310
Sanida T, Tabakis I-M, Sanida MV, Sideris A, Dasygenis M. A Robust Hybrid Deep Convolutional Neural Network for COVID-19 Disease Identification from Chest X-ray Images. Information. 2023; 14(6):310. https://doi.org/10.3390/info14060310
Chicago/Turabian StyleSanida, Theodora, Irene-Maria Tabakis, Maria Vasiliki Sanida, Argyrios Sideris, and Minas Dasygenis. 2023. "A Robust Hybrid Deep Convolutional Neural Network for COVID-19 Disease Identification from Chest X-ray Images" Information 14, no. 6: 310. https://doi.org/10.3390/info14060310
APA StyleSanida, T., Tabakis, I. -M., Sanida, M. V., Sideris, A., & Dasygenis, M. (2023). A Robust Hybrid Deep Convolutional Neural Network for COVID-19 Disease Identification from Chest X-ray Images. Information, 14(6), 310. https://doi.org/10.3390/info14060310